
Temporal Associations between Tri-Ponderal Mass Index and Blood Pressure in Chinese Children: A Cross-Lag Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Procedures
2.2. Study Measures
2.3. Statistical Analysis
3. Results
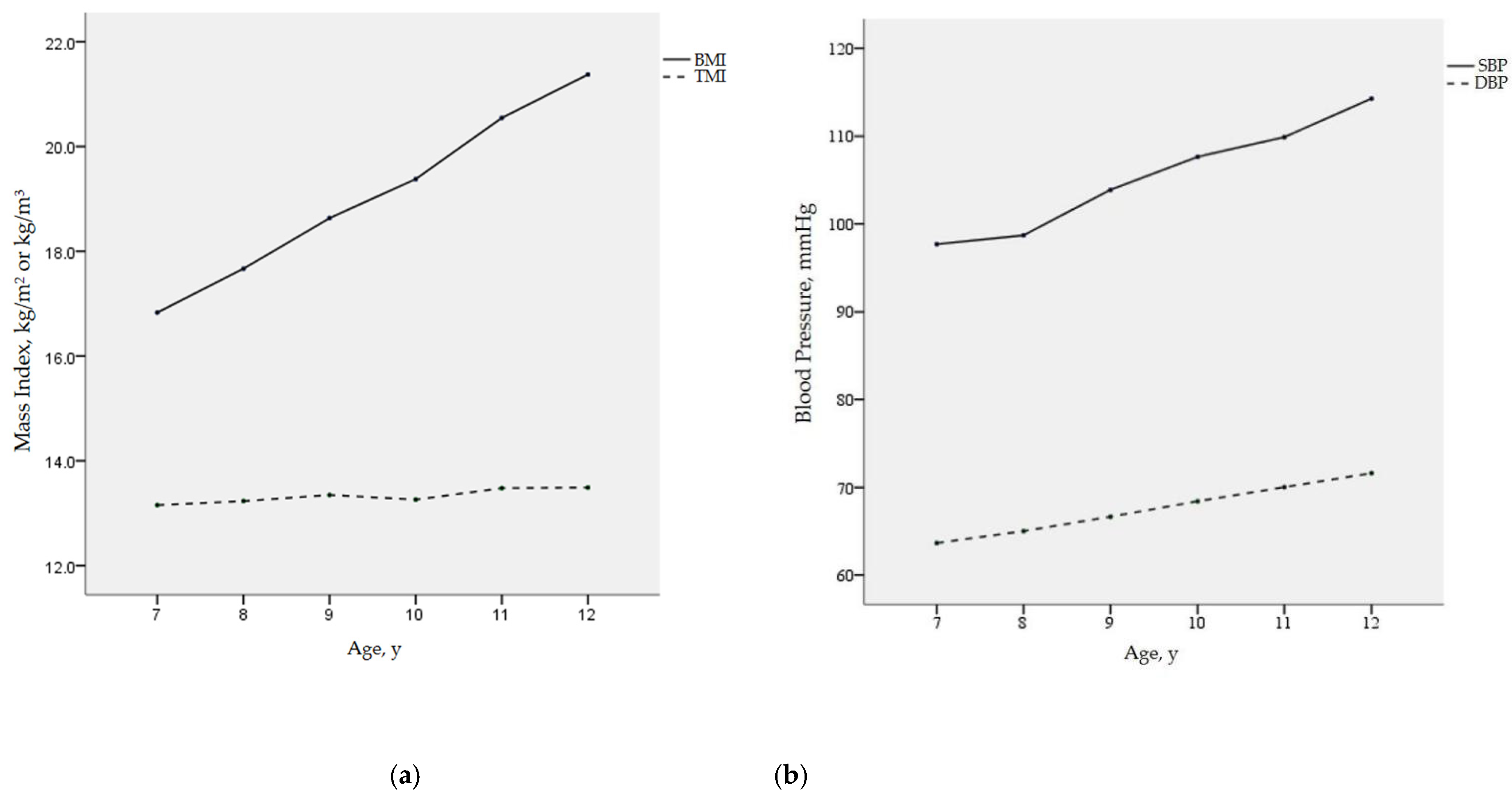
3.1. Stability of TMI and BMI with Age
3.2. Cross-Lagged Panel Analysis
3.2.1. Descriptive Statistics
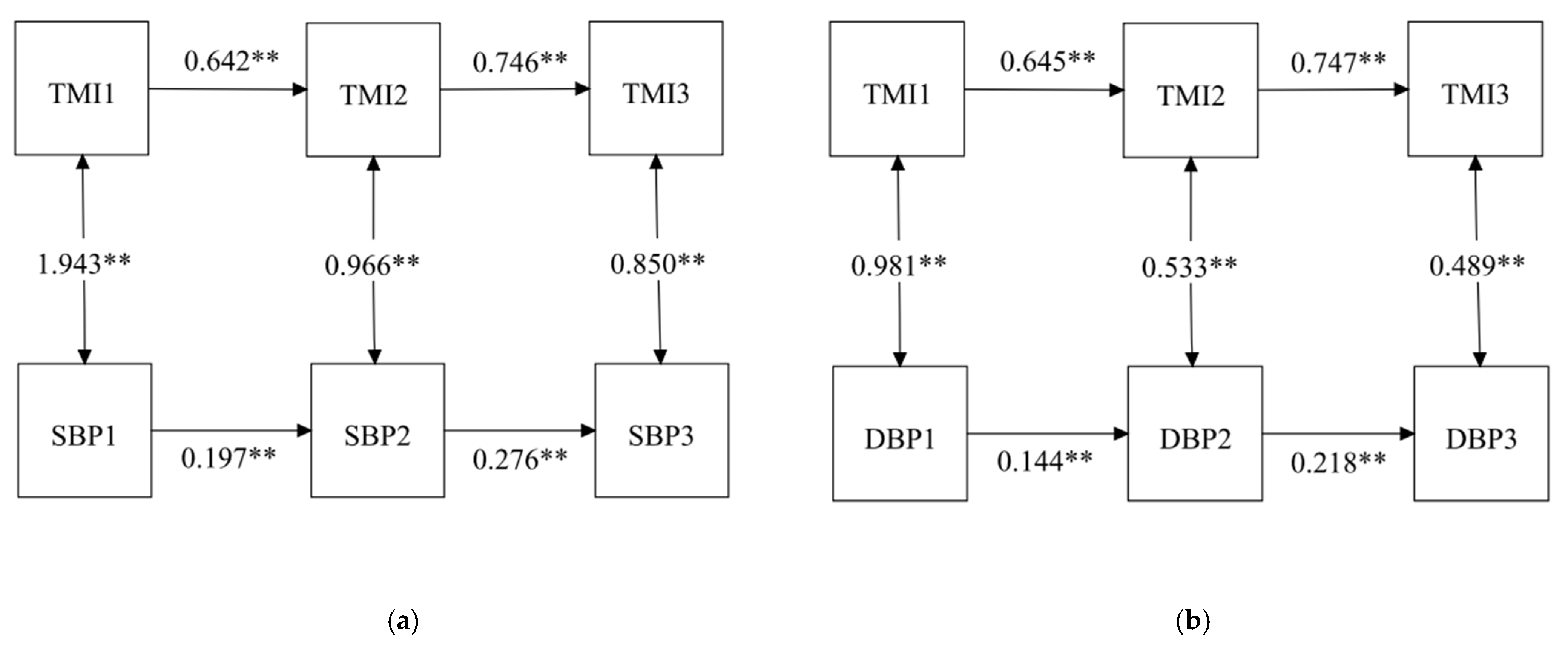
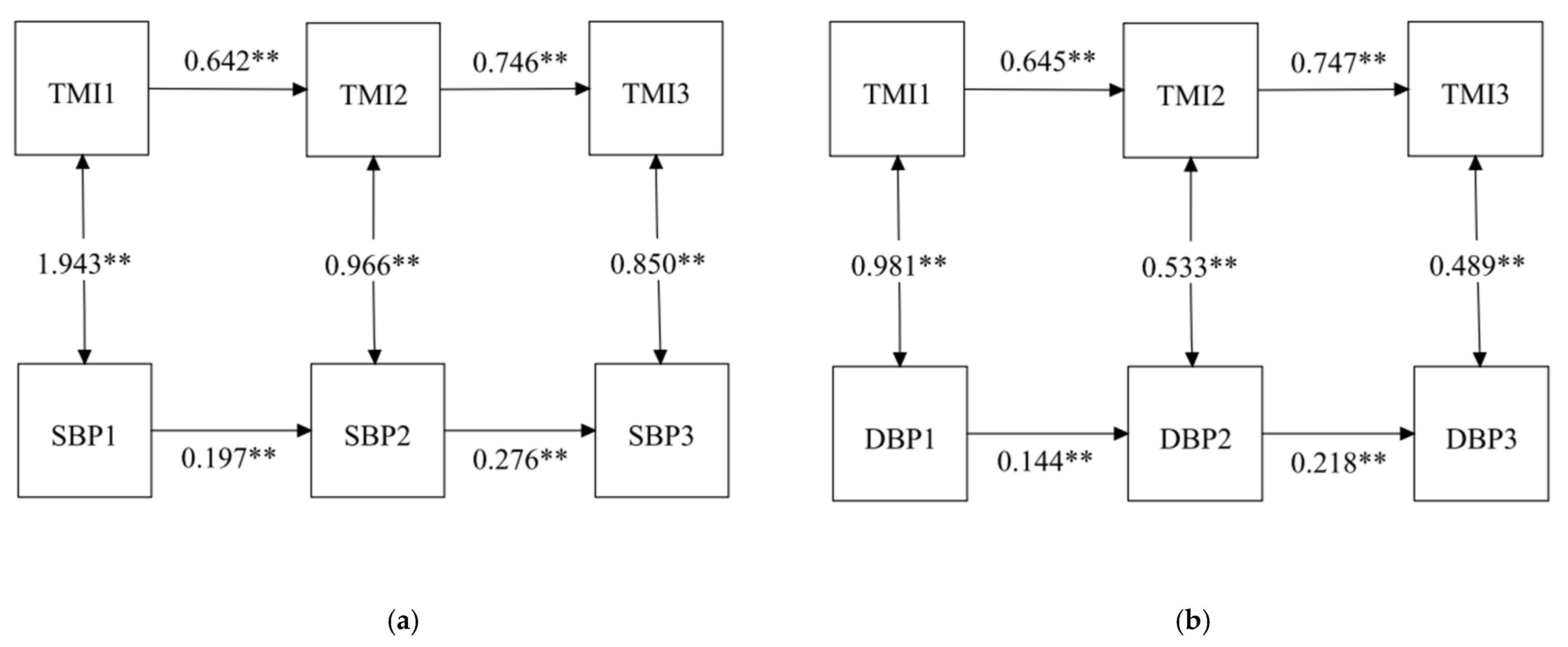
3.2.2. Stability Model
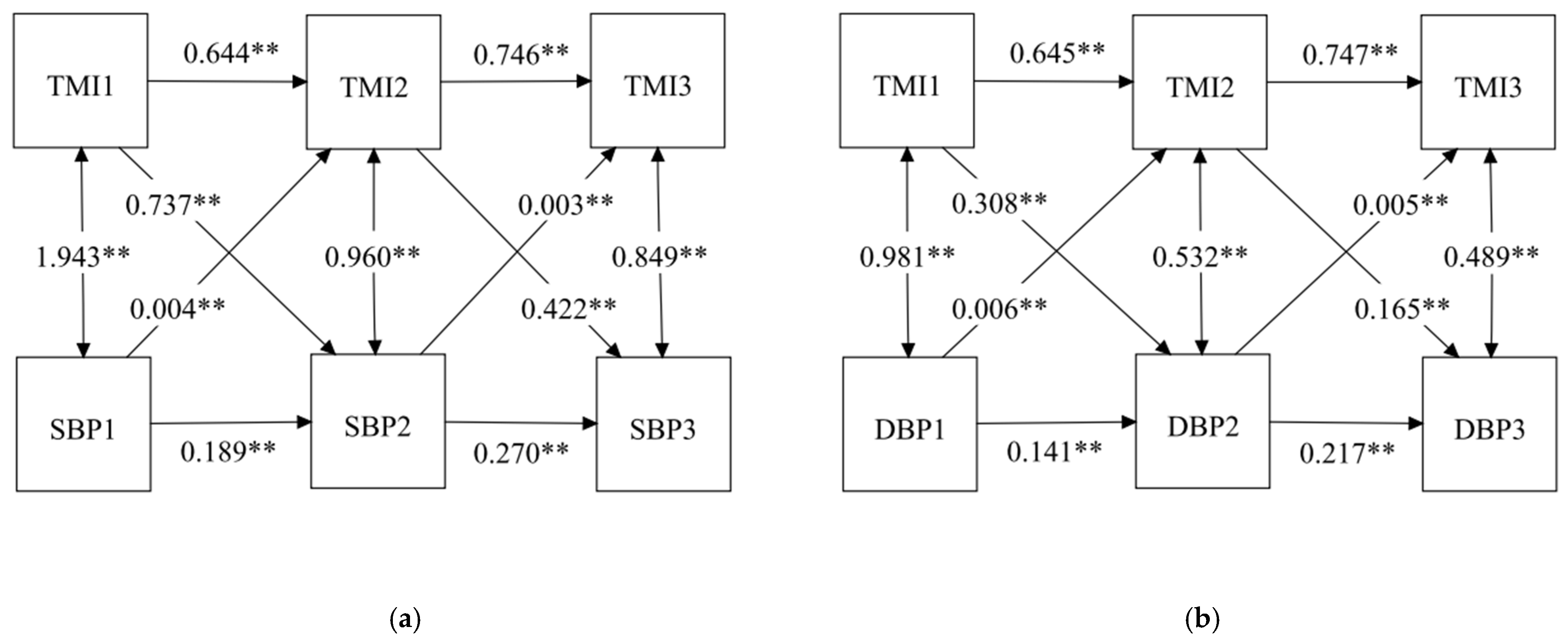
3.2.3. Cross-Lagged Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ashraf, M.; Irshad, M.; Parry, N.A. Pediatric hypertension: An updated review. Clin. Hypertens. 2020, 26, 22. [Google Scholar] [CrossRef] [PubMed]
- Rao, G. Diagnosis, Epidemiology, and Management of Hypertension in Children. Pediatrics 2016, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, Y.; Song, Y.; Zou, Z.; Ma, J.; Dong, B.; Prochaska, J.J. Updates to pediatric hypertension guidelines: Influence on classification of high blood pressure in children and adolescents. J Hypertens. 2019, 37, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Hanevold, C.D. White Coat Hypertension in Children and Adolescents. Hypertension 2019, 73, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Cha, S.D.; Patel, H.P.; Hains, D.S.; Mahan, J.D. The effects of hypertension on cognitive function in children and adolescents. Int. J. Pediatr. 2012, 2012, 891094. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.; Dana, T.; Bougatsos, C.; Blazina, I.; Norris, S.L. Screening for hypertension in children and adolescents to prevent cardiovascular disease. Pediatrics 2013, 131, 490–525. [Google Scholar] [CrossRef] [Green Version]
- Lona, G.; Endes, K.; Kochli, S.; Infanger, D.; Zahner, L.; Hanssen, H. Retinal Vessel Diameters and Blood Pressure Progression in Children. Hypertension 2020, 76, 450–457. [Google Scholar] [CrossRef]
- Wang, L.; Song, L.; Liu, B.; Zhang, L.; Wu, M.; Cao, Z.; Wang, Y. Trends and Status of the Prevalence of Elevated Blood Pressure in Children and Adolescents in China: A Systematic Review and Meta-analysis. Curr. Hypertens. Rep. 2019, 21, 88. [Google Scholar] [CrossRef]
- WHO. Obesity and Overweight. Fact Sheet. 2015. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 10 December 2021).
- Prentice, A.M.; Jebb, S.A. Beyond body mass index. Obes. Rev. 2001, 2, 141–147. [Google Scholar] [CrossRef]
- Cole, T.; Flegal, K.; Nicholls, D.; Jackson, A. Body mass index cut offs to define thinness in children and adolescents: International survey. BMJ Clin. Res. Ed. 2007, 335, 194. [Google Scholar] [CrossRef] [Green Version]
- Moselakgomo, V.K.; Van Staden, M. Diagnostic accuracy of tri-ponderal mass index and body mass index in estimating overweight and obesity in South African children. Afr. J. Prim. Health Care Fam. Med. 2019, 11, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Peterson, C.M.; Su, H.; Thomas, D.M.; Heo, M.; Golnabi, A.H.; Pietrobelli, A.; Heymsfield, S.B. Tri-Ponderal Mass Index vs. Body Mass Index in Estimating Body Fat During Adolescence. JAMA Pediatr. 2017, 171, 629–636. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, A.; Romano, L.; Di Renzo, L.; Gualtieri, P.; Salimei, C.; Carrano, E.; Rampello, T.; de Miranda, R.C. Triponderal mass index rather than body mass index: An indicator of high adiposity in Italian children and adolescents. Nutrition 2019, 60, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Qu, Y.; Niu, H.; Li, L.; Li, M.; Yan, S.; Li, M.; Jiang, S.; Ma, X.; Li, B.; Wu, H. Analysis of Dose-response Relationship between BMI and Hypertension in Northeastern China Using Restricted Cubic Spline Functions. Sci. Rep. 2019, 9, 18208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, Q.; Sun, L.; Zeng, Q. Trajectories of mid-life to elderly adulthood BMI and incident hypertension: The China Health and Nutrition Survey. BMJ Open 2021, 11, e047920. [Google Scholar] [CrossRef]
- Sabo, R.T.; Lu, Z.; Daniels, S.; Sun, S.S. Serial childhood BMI and associations with adult hypertension and obesity: The Fels Longitudinal Study. Obesity 2012, 20, 1741–1743. [Google Scholar] [CrossRef]
- Wang, X.; Dong, B.; Huang, S.; Ma, Y.; Zou, Z.; Ma, J.; Yang, Z.; Wang, Z. Body Mass Index Trajectory and Incident Hypertension: Results from a Longitudinal Cohort of Chinese Children and Adolescents, 2006–2016. Am. J. Public Health 2020, 110, 1689–1695. [Google Scholar] [CrossRef]
- Wang, J.; Zhu, Y.; Jing, J.; Chen, Y.; Mai, J.; Wong, S.H.; O’Reilly, J.; Ma, L. Relationship of BMI to the incidence of hypertension: A 4 years’ cohort study among children in Guangzhou, 2007–2011. BMC Public Health 2015, 15, 782. [Google Scholar] [CrossRef] [Green Version]
- Hu, J.; Chu, G.P.; Huang, F.F.; Zhou, Y.K.; Teng, C.G.; Yang, H.B.; Shen, H. Relation of body mass index (BMI) to the prevalence of hypertension in children: A 3years’ school-based prospective study in Suzhou, China. Int. J. Cardiol. 2016, 222, 270–274. [Google Scholar] [CrossRef]
- Lu, Y.; Luo, B.; Xie, J.; Zhang, X.; Zhu, H. Prevalence of hypertension and prehypertension and its association with anthropometrics among children: A cross-sectional survey in Tianjin, China. J. Hum. Hypertens. 2018, 32, 789–798. [Google Scholar] [CrossRef]
- Macdonald-Wallis, C.; Solomon-Moore, E.; Sebire, S.J.; Thompson, J.L.; Lawlor, D.A.; Jago, R. A longitudinal study of the associations of children’s body mass index and physical activity with blood pressure. PLoS ONE 2017, 12, e0188618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malavazos, A.E.; Capitanio, G.; Milani, V.; Ambrogi, F.; Matelloni, I.A.; Basilico, S.; Dubini, C.; Sironi, F.M.; Stella, E.; Castaldi, S.; et al. Tri-Ponderal Mass Index vs. body Mass Index in discriminating central obesity and hypertension in adolescents with overweight. Nutr. Metab. Cardiovasc. Dis. NMCD 2021, 31, 1613–1621. [Google Scholar] [CrossRef] [PubMed]
- Burns, R.A.; Crisp, D.A.; Burns, R.B. Re-examining the reciprocal effects model of self-concept, self-efficacy, and academic achievement in a comparison of the Cross-Lagged Panel and Random-Intercept Cross-Lagged Panel frameworks. Br. J. Educ. Psychol. 2020, 90, 77–91. [Google Scholar] [CrossRef] [PubMed]
- Hamaker, E.L.; Kuiper, R.M.; Grasman, R.P. A critique of the cross-lagged panel model. Psychol. Methods 2015, 20, 102–116. [Google Scholar] [CrossRef]
- Graham, J.W. Missing data analysis: Making it work in the real world. Annu. Rev. Psychol. 2009, 60, 549–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bentler, P. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- McDonald, R.P.; Ho, M.-H.R. Principles and practice in reporting structural equation analyses. Psychol. Methods 2002, 7, 64–82. [Google Scholar] [CrossRef]
- Oni, T.; Macia, E.; Gueye, L.; Duboz, P. Hypertension and Obesity in Dakar, Senegal. PLoS ONE 2016, 11, e0161544. [Google Scholar] [CrossRef] [Green Version]
- Gao, W.; Qiao, X.; Wang, Y.; Wan, L.; Wang, Z.; Wang, X.; Di, Z.; Liu, X. The Interactive Association of General Obesity and Central Obesity with Prevalent Hypertension in Rural Lanzhou, China. PLoS ONE 2016, 11, e0164409. [Google Scholar] [CrossRef]
- Matsuo, T.; Sairenchi, T.; Suzuki, K.; Tanaka, K.; Muto, T. Long-term stable obesity increases risk of hypertension. Int. J. Obes. 2011, 35, 1056–1062. [Google Scholar] [CrossRef] [Green Version]
- Kruger, R.; Kruger, H.S.; Monyeki, M.A.; Pienaar, A.E.; Roux, S.B.-L.; Gafane-Matemane, L.F.; Smith, W.; Mels, C.M.C.; Lammertyn, L.; Brits, J.S.; et al. A demographic approach to assess elevated blood pressure and obesity in prepubescent children: The ExAMIN Youth South Africa study. J. Hypertens. 2021, 39, 2190–2199. [Google Scholar] [CrossRef]
- Sanchez-Zamorano, L.M.; Salazar-Martinez, E.; Anaya-Ocampo, R.; Lazcano-Ponce, E. Body mass index associated with elevated blood pressure in Mexican school-aged adolescents. Prev. Med. 2009, 48, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Dong, B.; Ma, J.; Song, Y.; Zou, Z.; Arnold, L. Role of tri-ponderal mass index in cardio-metabolic risk assessment in children and adolescents: Compared with body mass index. Int. J. Obes. 2020, 44, 886–894. [Google Scholar] [CrossRef] [PubMed]
- Weihe, P.; Weihrauch-Bluher, S. Metabolic Syndrome in Children and Adolescents: Diagnostic Criteria, Therapeutic Options and Perspectives. Curr. Obes. Rep. 2019, 8, 472–479. [Google Scholar] [CrossRef]
- Ramirez-Velez, R.; Correa-Bautista, J.E.; Carrillo, H.A.; Gonzalez-Jimenez, E.; Schmidt-RioValle, J.; Correa-Rodriguez, M.; Garcia-Hermoso, A.; Gonzalez-Ruiz, K. Tri-Ponderal Mass Index vs. Fat Mass/Height(3) as a Screening Tool for Metabolic Syndrome Prediction in Colombian Children and Young People. Nutrients 2018, 10, 412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoshhali, M.; Heidari-Beni, M.; Qorbani, M.; Motlagh, M.E.; Ziaodini, H.; Heshmat, R.; Kelishadi, R. Tri-ponderal mass index and body mass index in prediction of pediatric metabolic syndrome: The CASPIAN-V study. Arch. Endocrinol. Metab. 2020, 64, 171–178. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Ma, J.; Huang, S.; Dong, B.; Dong, Y.; Yang, Z.; Hu, J.; Liang, W. Use of Tri-Ponderal Mass Index in Predicting Late Adolescent Overweight and Obesity in Children Aged 7-18. Front Nutr 2022, 9, 785863. [Google Scholar] [CrossRef]
- Wu, F.; Buscot, M.J.; Niinikoski, H.; Rovio, S.P.; Juonala, M.; Sabin, M.A.; Jula, A.; Ronnemaa, T.; Viikari, J.S.A.; Raitakari, O.T.; et al. Age-Specific Estimates and Comparisons of Youth Tri-Ponderal Mass Index and Body Mass Index in Predicting Adult Obesity-Related Outcomes. J. Pediatr. 2020, 218, 198–203.e6. [Google Scholar] [CrossRef]
- Lee, M.H.; Kang, D.R.; Kim, H.C.; Ahn, S.V.; Khaw, K.T.; Suh, I. A 24-year follow-up study of blood pressure tracking from childhood to adulthood in Korea: The Kangwha Study. Yonsei Med. J. 2014, 55, 360–366. [Google Scholar] [CrossRef] [Green Version]
- Kelly, R.K.; Thomson, R.; Smith, K.J.; Dwyer, T.; Venn, A.; Magnussen, C.G. Factors Affecting Tracking of Blood Pressure from Childhood to Adulthood: The Childhood Determinants of Adult Health Study. J. Pediatr. 2015, 167, 1422–1428.e2. [Google Scholar] [CrossRef] [Green Version]
- Sarganas, G.; Schaffrath Rosario, A.; Niessner, C.; Woll, A.; Neuhauser, H.K. Tracking of Blood Pressure in Children and Adolescents in Germany in the Context of Risk Factors for Hypertension. Int. J. Hypertens. 2018, 2018, 8429891. [Google Scholar] [CrossRef] [PubMed]
- Jonk, A.; Houben, A.; de Jongh, R.; Serné, E.; Schaper, N.; Stehouwer, C. Microvascular dysfunction in obesity: A potential mechanism in the pathogenesis of obesity-associated insulin resistance and hypertension. Physiology 2007, 22, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Vaneckova, I.; Maletinska, L.; Behuliak, M.; Nagelova, V.; Zicha, J.; Kunes, J. Obesity-related hypertension: Possible pathophysiological mechanisms. J. Endocrinol. 2014, 223, R63–R78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wirix, A.J.G.; Kaspers, P.J.; Nauta, J.; Chinapaw, M.J.M.; Kist-van Holthe, J.E. Pathophysiology of hypertension in obese children: A systematic review. Obes. Rev. 2015, 16, 831–842. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Total Participants | Males | Females | p | |
|---|---|---|---|---|
| N (%) | 132,159 | 64,226 (48.6) | 67,933 (51.4) | |
| Age | 9.33 ± 1.68 | 9.24 ± 1.67 | 9.43 ± 1.68 | <0.001 a |
| Urban, n (%) | 66,454 (50.3) | 32,256 (50.2) | 34,198 (50.3) | <0.001 b |
| Height (m) | 1.41 ± 0.12 | 1.41 ± 0.12 | 1.42 ± 0.12 | <0.001 a |
| Weight (kg) | 36.30 ± 9.48 | 36.40 ± 9.52 | 36.21 ± 9.44 | 0.001 a |
| TMI (kg/m3) | ||||
| Wave 1 | 12.72 ± 1.69 | 12.90 ± 1.71 | 12.55 ± 1.65 | <0.001 a |
| Wave 2 | 12.79 ± 1.79 | 12.88 ± 1.88 | 12.70 ± 1.69 | <0.001 a |
| Wave 3 | 12.93 ± 1.81 | 12.80 ± 1.92 | 13.07 ± 1.69 | <0.001 a |
| SBP (mmHg) | ||||
| Wave 1 | 102.08 ± 12.48 | 102.19 ± 12.46 | 101.97 ± 12.50 | 0.001 a |
| Wave 2 | 110.38 ± 12.25 | 111.06 ± 12.61 | 109.74 ± 11.88 | <0.001 a |
| Wave 3 | 115.04 ± 11.87 | 116.96 ± 12.32 | 113.22 ± 11.12 | <0.001 a |
| DBP (mmHg) | ||||
| Wave 1 | 65.32 ± 8.62 | 65.19 ± 8.54 | 65.45 ± 8.69 | <0.001 a |
| Wave 2 | 69.04 ± 8.72 | 68.80 ± 8.82 | 69.27 ± 8.62 | <0.001 a |
| Wave 3 | 72.02 ± 8.31 | 71.92 ± 8.53 | 72.12 ± 8.08 | <0.001 a |
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. TMI (Wave 1) | 12.72 | 1.69 | 1.000 | ||||||||
| 2. TMI (Wave 2) | 12.79 | 1.79 | 0.631 * | 1.000 | |||||||
| 3. TMI (Wave 3) | 12.93 | 1.81 | 0.555 * | 0.745 * | 1.000 | ||||||
| 4. SBP (Wave 1) | 102.08 | 12.48 | 0.013 * | 0.002 | 0.003 | 1.000 | |||||
| 5. SBP (Wave 2) | 110.38 | 12.25 | 0.044 * | 0.048 * | 0.039 * | 0.300 * | 1.000 | ||||
| 6. SBP (Wave 3) | 115.04 | 11.87 | 0.065 * | 0.051 * | 0.058 * | 0.229 * | 0.337 * | 1.000 | |||
| 7. DBP (Wave 1) | 65.32 | 8.61 | 0.012 * | 0.011 * | 0.007 * | 0.587 * | 0.195 * | 0.145 * | 1.000 | ||
| 8. DBP (Wave 2) | 69.04 | 8.72 | 0.026 * | 0.041 * | 0.052 * | 0.192 * | 0.585 * | 0.187 * | 0.174 * | 1.000 | |
| 9. DBP (Wave 3) | 72.02 | 8.31 | 0.025 * | 0.018 * | 0.048 * | 0.131 * | 0.241 * | 0.517 * | 0.123 * | 0.249 * | 1.000 |
| Variables | χ2 | df | CFI | TLI | RMSEA | SRMR | Comparison | ∆χ2 | ∆df | |
|---|---|---|---|---|---|---|---|---|---|---|
| SBP | Model 1 a | 9050.29 | 20 | 0.966 | 0.923 | 0.058 (0.057–0.059) | 0.032 | |||
| Model 2 b | 6954.08 | 18 | 0.974 | 0.934 | 0.054 (0.053–0.055) | 0.019 | M1–M2 | 2096.21 ** | 2 | |
| Model 3 c | 8723.44 | 18 | 0.967 | 0.917 | 0.060 (0.059–0.062) | 0.030 | M1–M3 | 326.85 ** | 2 | |
| Model 4 d | 6638.67 | 16 | 0.975 | 0.929 | 0.056 (0.055–0.057) | 0.018 | M1–M4 | 2411.62 ** | 4 | |
| DBP | Model 1 a | 6349.27 | 20 | 0.971 | 0.936 | 0.049 (0.048–0.050) | 0.022 | |||
| Model 2 b | 5717.17 | 18 | 0.974 | 0.936 | 0.049 (0.048–0.050) | 0.016 | M1–M2 | 632.10 ** | 2 | |
| Model 3 c | 6003.29 | 18 | 0.973 | 0.932 | 0.050 (0.049–0.051) | 0.020 | M1–M3 | 345.98 ** | 2 | |
| Model 4 d | 5374.45 | 16 | 0.976 | 0.932 | 0.050 (0.049–0.051) | 0.015 | M1–M4 | 974.82 ** | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, Y.; Zhang, F.; Wang, H.; Zhao, L.; Song, R.; Han, M.; Shen, X. Temporal Associations between Tri-Ponderal Mass Index and Blood Pressure in Chinese Children: A Cross-Lag Analysis. Nutrients 2022, 14, 1783. https://doi.org/10.3390/nu14091783
Cui Y, Zhang F, Wang H, Zhao L, Song R, Han M, Shen X. Temporal Associations between Tri-Ponderal Mass Index and Blood Pressure in Chinese Children: A Cross-Lag Analysis. Nutrients. 2022; 14(9):1783. https://doi.org/10.3390/nu14091783
Chicago/Turabian StyleCui, Yixin, Fan Zhang, Hao Wang, Longzhu Zhao, Ruihan Song, Miaomiao Han, and Xiaoli Shen. 2022. "Temporal Associations between Tri-Ponderal Mass Index and Blood Pressure in Chinese Children: A Cross-Lag Analysis" Nutrients 14, no. 9: 1783. https://doi.org/10.3390/nu14091783
APA StyleCui, Y., Zhang, F., Wang, H., Zhao, L., Song, R., Han, M., & Shen, X. (2022). Temporal Associations between Tri-Ponderal Mass Index and Blood Pressure in Chinese Children: A Cross-Lag Analysis. Nutrients, 14(9), 1783. https://doi.org/10.3390/nu14091783