
Usability of myfood24 Healthcare and Mathematical Diet Optimisation in Clinical Populations: A Pilot Feasibility Randomised Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
1.1. Improved Health and Recovery through Technology-Supported Dietary Behaviour Change
1.2. myfood24 Healthcare Technology
1.3. Study Objectives
2. Materials and Methods
2.1. Automated Feedback
2.2. Patient Involvement
2.3. Economic Analysis
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics and Feedback
3.2. Health Care Professional Use and Feedback on myfood24
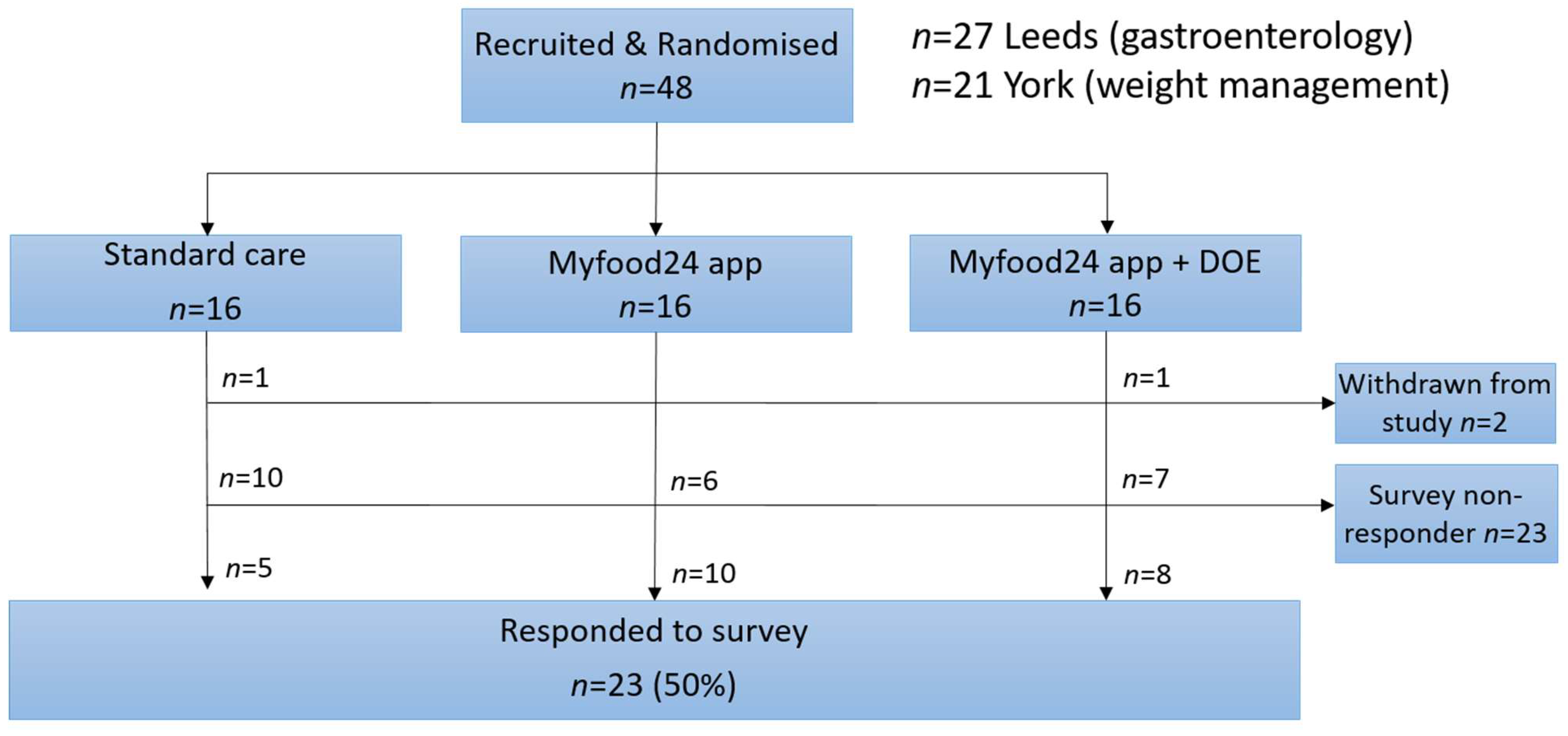
3.3. Process Evaluation
3.4. Health Economic Estimates
4. Discussion
4.1. Strengths/Limitations
4.2. Next Steps
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN guideline: Clinical nutrition in surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fakih El Khoury, C.; Karavetian, M.; Halfens, R.J.G.; Crutzen, R.; Khoja, L.; Schols, J. The Effects of Dietary Mobile Apps on Nutritional Outcomes in Adults with Chronic Diseases: A Systematic Review and Meta-Analysis. J. Acad. Nutr. Diet. 2019, 119, 626–651. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.; Beeken, R.J.; Wardle, J. Health behaviour advice to cancer patients: The perspective of social network members. Br. J. Cancer 2013, 108, 831–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandt, C.J.; Clemensen, J.; Nielsen, J.B.; Søndergaard, J. Drivers for successful long-term lifestyle change, the role of e-health: A qualitative interview study. BMJ Open 2018, 8, e017466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.C.; Lee, M.S.; Cheng, H.L.; Chou, H.Y.; Chan, L.C. More Frequent Nutrition Counseling Limits Weight Loss and Improves Energy Intake During Oncology Management: A Longitudinal Inpatient Study in Taiwan. Nutr. Cancer 2019, 71, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Lis, C.G.; Gupta, D.; Lammersfeld, C.A.; Markman, M.; Vashi, P.G. Role of nutritional status in predicting quality of life outcomes in cancer--a systematic review of the epidemiological literature. Nutr. J. 2012, 11, 27. [Google Scholar] [CrossRef] [Green Version]
- Villinger, K.; Wahl, D.R.; Boeing, H.; Schupp, H.T.; Renner, B. The effectiveness of app-based mobile interventions on nutrition behaviours and nutrition-related health outcomes: A systematic review and meta-analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2019, 20, 1465–1484. [Google Scholar] [CrossRef] [Green Version]
- Franco, R.Z.; Fallaize, R.; Lovegrove, J.A.; Hwang, F. Popular Nutrition-Related Mobile Apps: A Feature Assessment. JMIR mHealth uHealth 2016, 4, e85. [Google Scholar] [CrossRef]
- Ferrara, G.; Kim, J.; Lin, S.; Hua, J.; Seto, E. A Focused Review of Smartphone Diet-Tracking Apps: Usability, Functionality, Coherence With Behavior Change Theory, and Comparative Validity of Nutrient Intake and Energy Estimates. JMIR mHealth uHealth 2019, 7, e9232. [Google Scholar] [CrossRef]
- Eldridge, A.L.; Piernas, C.; Illner, A.K.; Gibney, M.J.; Gurinović, M.A.; de Vries, J.H.M.; Cade, J.E. Evaluation of New Technology-Based Tools for Dietary Intake Assessment-An ILSI Europe Dietary Intake and Exposure Task Force Evaluation. Nutrients 2018, 11, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cade, J.E. Measuring diet in the 21st century: Use of new technologies. Proc. Nutr. Soc. 2017, 76, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Cade, J.E.; Allman-Farinelli, M. The Most Popular Smartphone Apps for Weight Loss: A Quality Assessment. JMIR mHealth uHealth 2015, 3, e104. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Lieffers, J.; Bauman, A.; Hanning, R.; Allman-Farinelli, M. Designing Health Apps to Support Dietetic Professional Practice and Their Patients: Qualitative Results From an International Survey. JMIR mHealth uHealth 2017, 5, e40. [Google Scholar] [CrossRef] [PubMed]
- Wark, P.A.; Hardie, L.J.; Frost, G.S.; Alwan, N.A.; Carter, M.; Elliott, P.; Ford, H.E.; Hancock, N.; Morris, M.A.; Mulla, U.Z.; et al. Validity of an online 24-h recall tool (myfood24) for dietary assessment in population studies: Comparison with biomarkers and standard interviews. BMC Med. 2018, 16, 136. [Google Scholar] [CrossRef]
- Carter, M.C.; Albar, S.A.; Morris, M.A.; Mulla, U.Z.; Hancock, N.; Evans, C.E.; Alwan, N.A.; Greenwood, D.C.; Hardie, L.J.; Frost, G.S.; et al. Development of a UK Online 24-h Dietary Assessment Tool: myfood24. Nutrients 2015, 7, 4016–4032. [Google Scholar] [CrossRef] [Green Version]
- Gianfrancesco, C.; Darwin, Z.; McGowan, L.; Smith, D.M.; Haddrill, R.; Carter, M.; Scott, E.M.; Alwan, N.A.; Morris, M.A.; Albar, S.A.; et al. Exploring the Feasibility of Use of An Online Dietary Assessment Tool (myfood24) in Women with Gestational Diabetes. Nutrients 2018, 10, 1147. [Google Scholar] [CrossRef] [Green Version]
- Public Health England. Government Dietary Recommendations. Government Recommendations for Energy and Nutrients for Males and Females Aged 1–18 Years and 19+ Years; PHE: London, UK, 2016.
- Gazan, R.; Brouzes, C.M.C.; Vieux, F.; Maillot, M.; Lluch, A.; Darmon, N. Mathematical Optimization to Explore Tomorrow’s Sustainable Diets: A Narrative Review. Adv. Nutr. 2018, 9, 602–616. [Google Scholar] [CrossRef]
- Boyle, M. Mobile Internet Statistics. Available online: https://www.finder.com/uk/mobile-internet-statistics (accessed on 5 April 2022).
- Lieffers, J.R.; Hanning, R.M. Dietary assessment and self-monitoring with nutrition applications for mobile devices. Can. J. Diet. Pract. Res. 2012, 73, e253–e260. [Google Scholar] [CrossRef]
- Campbell, J.; Porter, J. Dietary mobile apps and their effect on nutritional indicators in chronic renal disease: A systematic review. Nephrology (Carlton) 2015, 20, 744–751. [Google Scholar] [CrossRef] [Green Version]
- Carter, M.C.; Burley, V.J.; Nykjaer, C.; Cade, J.E. Adherence to a smartphone application for weight loss compared to website and paper diary: Pilot randomized controlled trial. J. Med. Internet Res. 2013, 15, e32. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.L.; Hopkins, C.M.; Brooks, T.L.; Bennett, G.G. Comparing Self-Monitoring Strategies for Weight Loss in a Smartphone App: Randomized Controlled Trial. JMIR mHealth uHealth 2019, 7, e12209. [Google Scholar] [CrossRef] [PubMed]
- Dounavi, K.; Tsoumani, O. Mobile Health Applications in Weight Management: A Systematic Literature Review. Am. J. Prev. Med. 2019, 56, 894–903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner-McGrievy, G.M.; Dunn, C.G.; Wilcox, S.; Boutte, A.K.; Hutto, B.; Hoover, A.; Muth, E. Defining Adherence to Mobile Dietary Self-Monitoring and Assessing Tracking Over Time: Tracking at Least Two Eating Occasions per Day Is Best Marker of Adherence within Two Different Mobile Health Randomized Weight Loss Interventions. J. Acad. Nutr. Diet. 2019, 119, 1516–1524. [Google Scholar] [CrossRef] [PubMed]
- Wellard-Cole, L.; Potter, M.; Jung, J.J.; Chen, J.; Kay, J.; Allman-Farinelli, M. A Tool to Measure Young Adults’ Food Intake: Design and Development of an Australian Database of Foods for the Eat and Track Smartphone App. JMIR mHealth uHealth 2018, 6, e12136. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.C.; Burley, V.J.; Cade, J.E. Weight Loss Associated With Different Patterns of Self-Monitoring Using the Mobile Phone App My Meal Mate. JMIR mHealth uHealth 2017, 5, e8. [Google Scholar] [CrossRef]
- Omlin, A.; Blum, D.; Wierecky, J.; Haile, S.R.; Ottery, F.D.; Strasser, F. Nutrition impact symptoms in advanced cancer patients: Frequency and specific interventions, a case-control study. J. Cachexia Sarcopenia Muscle 2013, 4, 55–61. [Google Scholar] [CrossRef]
- Public Health England. National Diet and Nutrition Survey: Diet, Nutrition and Physical Activity in 2020. A Follow Up Study during COVID-19; Public Health England: London, UK, 2021.
- Public Health England and the Food Standards Agency. National Diet and Nutrition Survey Rolling Programme Years 9 to 11 (2016/2017 to 2018/2019); Public Health Englad: London, UK, 2020.
- Schuetz, P.; Fehr, R.; Baechli, V.; Geiser, M.; Deiss, M.; Gomes, F.; Kutz, A.; Tribolet, P.; Bregenzer, T.; Braun, N.; et al. Individualised nutritional support in medical inpatients at nutritional risk: A randomised clinical trial. Lancet 2019, 393, 2312–2321. [Google Scholar] [CrossRef]
- Chen, J.; Gemming, L.; Hanning, R.; Allman-Farinelli, M. Smartphone apps and the nutrition care process: Current perspectives and future considerations. Patient Educ. Couns. 2018, 101, 750–757. [Google Scholar] [CrossRef]
- Chen, J.; Lieffers, J.; Bauman, A.; Hanning, R.; Allman-Farinelli, M. The use of smartphone health apps and other mobile health (mHealth) technologies in dietetic practice: A three country study. J. Hum. Nutr. Diet. 2017, 30, 439–452. [Google Scholar] [CrossRef]
- British Dietetic Association. Model and Process for Nutrition and Dietetic Practice; The British Dietetic Association: Birmingham, UK, 2020. [Google Scholar]
- Crowley, J.; Ball, L.; Hiddink, G.J. Nutrition in medical education: A systematic review. Lancet Planet Health 2019, 3, e379–e389. [Google Scholar] [CrossRef]
- Macaninch, E.; Buckner, L.; Amin, P.; Broadley, I.; Crocombe, D.; Herath, D.; Jaffee, A.; Carter, H.; Golubic, R.; Rajput-Ray, M.; et al. Time for nutrition in medical education. BMJ Nutr. Prev. Health 2020, 3, 40–48. [Google Scholar] [CrossRef] [PubMed]
- AfN Inter-Professional Working Group on Medical Nutrition Education. UK Undergraduate Curriculum in Nutrition for Medical Doctors; Association for Nutrition: London, UK, 2021. [Google Scholar]
- NHS. Better Health. Healthier Families. Food Scanner App. Available online: https://www.nhs.uk/healthier-families/ (accessed on 31 January 2022).
- Adams, S.H.; Anthony, J.C.; Carvajal, R.; Chae, L.; Khoo, C.S.H.; Latulippe, M.E.; Matusheski, N.V.; McClung, H.L.; Rozga, M.; Schmid, C.H.; et al. Perspective: Guiding Principles for the Implementation of Personalized Nutrition Approaches That Benefit Health and Function. Adv. Nutr. 2020, 11, 25–34. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Tier 3 Weight Management Patients | Gastroenterology Surgery Patients | All | |
|---|---|---|---|
| Number recruited | 21 | 27 | 48 |
| Age, years | 46 (11) | 55 (13) | 51 (13) |
| BMI, kg/m2 | 49.0 (7.8) | 25.8 (7.0) | 35.9 (13.7) |
| Sex | |||
| Male | 3 (14) | 8 (30) | 11 (23) |
| Female | 18 (86) | 19 (70) | 37 (77) |
| Ethnicity 1,2 | |||
| White | 11 | 10 | 21 |
| Black | 0 | 0 | 0 |
| Asian | 0 | 1 | 1 |
| Highest educational achievement 1 | |||
| Undergraduate, postgraduate, higher degree, or teaching qualification | 3 | 8 | 11 |
| AS or A-level/City and Guilds Technical or trade certificate | 3 | 1 | 4 |
| NVQ/GNVQ/CSE/O-level/GCSE | 5 | 2 | 7 |
| Occupation 1 | |||
| Managerial and Professional | 3 | 4 | 7 |
| Intermediate occupations | 0 | 2 | 2 |
| Semi-routine and Routine | 3 | 0 | 3 |
| Retired | 2 | 5 | 7 |
| Unemployed/non-paid work | 3 | 0 | 3 |
| Usual eating pattern 1 | |||
| Non-vegetarian | 9 | 9 | 18 |
| Vegetarian | 2 | 1 | 3 |
| Vegan | 0 | 0 | 0 |
| Other diet pattern | 0 | 1 | 1 |
| Tier 3 Weight Management Patients | Gastroenterology Surgery Patients | All | |
|---|---|---|---|
| Questionnaire: Respondents/allocated, n | 12/21 | 11/25 | 23/46 |
| Received dietary guidance or advice from HCP in the last 12 months | |||
| Yes, ongoing | 9 | 3 | 12 |
| Yes, once | 2 | 2 | 4 |
| No, but would like advice | 1 | 5 | 6 |
| No, did not want advice | 0 | 1 | 1 |
| Dietary advice given by | |||
| Hospital doctor | 2 | 1 | 3 |
| Hospital nurse | 2 | 0 | 2 |
| GP | 1 | 0 | 1 |
| Practice nurse | 0 | 0 | 0 |
| Dietician | 10 | 5 | 15 |
| Private nutritionist | 0 | 0 | 0 |
| Other | 1 | 1 | 2 |
| Never received advice | 0 | 4 | 4 |
| Conditions requiring dietary support | |||
| Obesity | 12 | 0 | 12 |
| Bowel cancer | 0 | 1 | 1 |
| Other cancer | 0 | 0 | 0 |
| Irritable bowel syndrome | 1 | 1 | 2 |
| Malnutrition | 0 | 2 | 2 |
| Other conditions | 2 | 9 | 11 |
| Medical conditions or symptoms affecting diet | |||
| Yes | 4 | 9 | 13 |
| No | 6 | 2 | 8 |
| Not sure | 1 | 0 | 1 |
| Have kept a paper or electronic food diary | 11 | 10 | 21 |
| Have kept a food record using computer, laptop, tablet, or smartphone app | 6 | 3 | 9 |
| Self-rated internet ability (score 1–5) 1 | Mean 2.4 (1.2) | Mean 1.8 (0.9) | 2.2 (1.2) |
| Internet use frequency | |||
| Daily | 10 | 10 | 20 |
| 2–6 times a week | 1 | 0 | 1 |
| Less than once per week | 0 | 1 | 1 |
| Less than once per month | 0 | 0 | 0 |
| Self-rated confidence in using technology in general (score 1–10) 2 | Mean 7.6 (2.5) | Mean 9.0 (1.3) | 8.2 (2.4) |
| Tier 3 Weight Management Patients | Gastroenterology Surgery Patients | All | ||
|---|---|---|---|---|
| N allocated (groups 2 + 3) | 14 | 16 | 30 | |
| Used app to record diet | 14 | 11 | 25 | |
| Daily recorded nutrient intake | ||||
| Energy, kcal | 1060 (513) | 1209 (675) | 1148 (617) | |
| Total fat | g/day | 35.8 (22.9) | 51.1 (33.3) | 44.8 (30.4) |
| % energy | 29 | 37 | 34 | |
| Saturated fat | g/day | 15.0 (10.8) | 21.3 (21.3) | 18.7 (18.0) |
| % energy | 13 | 15 | 14 | |
| Carbohydrate | g/day | 133.1 (64.4) | 141.9 (76.6) | 138.3 (71.9) |
| % energy | 52 | 50 | 51 | |
| Total sugar | g/day | 61.2 (40.4) | 59.5 (37.2) | 60.2 (38.5) |
| % energy | 25 | 22 | 23 | |
| Protein | g/day | 50.3 (26.3) | 42.5 (26.9) | 45.7 (26.9) |
| % energy | 20 | 13 | 16 | |
| Fibre (AOAC) 1 | g/day | 15.4 (7.4) | 9.7 (6.4) | 12.0 (7.4) |
| Salt | g/day | 3.9 (3.0) | 4.0 (5.2) | 4.0 (4.5) |
| Tier 3 Weight Management Patients | Gastroenterology Surgery Patients | All | |
|---|---|---|---|
| N allocated to app (groups 2 + 3) | 14 | 18 | 32 |
| Used app to record diet at least once | 14 | 11 | 25 |
| Number of food diaries submitted | |||
| Mean (SD) | 10.3 (13.7) | 18.9 (20.3) | 14.0 (17.5) |
| Median (IQR) | 5 (3–13) | 8 (2–40) | 6 (2.5–17) |
| Range | 1–55 | 1–58 | 1–58 |
| Used app + completed survey 1 | 9 | 7 | 16 |
| Device used to access app | |||
| Personal computer or Laptop | 0 | 0 | 0 |
| Smartphone | 8 | 6 | 14 |
| Tablet | 0 | 1 | 1 |
| Time to complete 24-hour diary, minutes Mean (SD) | 16 (11) | 13 (9) | 15 (10) |
| ‘Did your symptoms/conditions improve as a result of using myfood24?’ | |||
| Yes | 2 | 1 | 3 |
| No | 5 | 5 | 10 |
| Not sure | 2 | 1 | 3 |
| ‘Did you find all consumed food items when using myfood24?’ | |||
| Yes | 2 | 2 | 4 |
| No | 6 | 5 | 11 |
| ‘Did you discuss diet, as recorded in myfood24, with HCP?’ | |||
| Yes | 6 | 1 | 7 |
| Had a consultation but was not given dietary advice | 0 | 0 | 0 |
| No consultation since using myfood24 | 3 | 6 | 9 |
| ‘If not, will you use myfood24 feedback to ask for dietary advice at next appointment?’ | |||
| Yes | 3 | 3 | 6 |
| No | 2 | 3 | 5 |
| ‘Does myfood24 gives you confidence to stick to dietary advice from HCP?’ | |||
| Yes | 2 | 2 | 4 |
| No | 1 | 3 | 4 |
| Not sure | 6 | 2 | 8 |
| ‘Could myfood24 help manage conditions/symptoms in the future?’ | |||
| Yes | 3 | 1 | 4 |
| No | 1 | 3 | 4 |
| Not sure | 5 | 3 | 8 |
| Likelihood of using myfood24 again (scale 1–10) 2 | 5.6 (3.5) | 4.6 (3.5) | 5.1 (3.4) |
| Ease of use (scale 1–3) 3 | |||
| I thought the time taken to complete myfood24 was reasonable | 2.4 (0.9) | 2.3 (1.0) | 2.4 (0.9) |
| I thought the instructions and wording used on myfood24 was clear and easy to understand | 2.4 (0.9) | 2.1 (0.9) | 2.3 (0.9) |
| I liked the design and layout of myfood24 | 2.4 (0.9) | 2.1 (0.9) | 2.3 (0.9) |
| Finding the right food and drink items was simple and efficient | 1.3 (0.7) | 1.6 (0.8) | 1.4 (0.7) |
| I found the selection of a portion size straightforward | 2.3 (1.0) | 2.3 (1.0) | 2.3 (0.9) |
| I found the possibility to add a home-cooked recipe straightforward | 1.8 (1.0) | 1.6 (0.9) | 1.7 (0.9) |
| If I made a mistake, I found it easy to correct | 2.4 (0.9) | 2.6 (0.8) | 2.5 (0.8) |
| The feedback graphs were easy to understand | 2.3 (1.0) | 2.8 (0.4) | 2.5 (0.8) |
| System usability score 4 (Score 0–100) | 54 (17) | 65 (26) | 59 (21) |
| Score components 5 (Score 0–4 with 2 being middle) | |||
| I think that I would like to use myfood24 frequently | 2.0 (1.6) | 2.3 (1.6) | 2.1 (1.5) |
| I found myfood24 unnecessarily complex (it was complicated to use) | 1.9 (1.4) | 1.3 (1.4) | 1.6 (1.4) |
| I thought myfood24 was easy to use | 2.3 (1.2) | 2.7 (1.3) | 2.5 (1.2) |
| I think that I would need the support of a technical person to use myfood24 | 1.9 (1.1) | 1.4 (1.4) | 1.7 (1.2) |
| I found that the various functions in myfood24 were well-integrated (everything worked together smoothly) | 2.0 (1.2) | 2.1 (1.8) | 2.1 (1.4) |
| I thought there was too much inconsistency in myfood24 | 1.9 (1.4) | 1.9 (1.7) | 1.9 (1.5) |
| I think most people would learn to use myfood24 very quickly | 2.2 (1.1) | 3.1 (0.7) | 2.6 (1.0) |
| I found myfood24 very cumbersome to use | 1.1 (0.9) | 1.9 (1.9) | 1.4 (1.4) |
| I felt very confident in using myfood24 | 1.9 (1.2) | 3.1 (1.5) | 2.4 (1.4) |
| I needed to learn a lot of things before I could get going with myfood24 | 1.9 (1.4) | 0.9 (1.6 | 1.4 (1.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Threapleton, D.E.; Beer, S.L.; Foley, D.J.; Gibson, L.E.; Trevillion, S.; Burke, D.; Wheatstone, P.; Gath, J.; Hex, N.; Setters, J.; et al. Usability of myfood24 Healthcare and Mathematical Diet Optimisation in Clinical Populations: A Pilot Feasibility Randomised Controlled Trial. Nutrients 2022, 14, 1768. https://doi.org/10.3390/nu14091768
Threapleton DE, Beer SL, Foley DJ, Gibson LE, Trevillion S, Burke D, Wheatstone P, Gath J, Hex N, Setters J, et al. Usability of myfood24 Healthcare and Mathematical Diet Optimisation in Clinical Populations: A Pilot Feasibility Randomised Controlled Trial. Nutrients. 2022; 14(9):1768. https://doi.org/10.3390/nu14091768
Chicago/Turabian StyleThreapleton, Diane E., Sarah L. Beer, Dustin J. Foley, Lauren E. Gibson, Sarah Trevillion, Dermot Burke, Pete Wheatstone, Jacqui Gath, Nick Hex, Jo Setters, and et al. 2022. "Usability of myfood24 Healthcare and Mathematical Diet Optimisation in Clinical Populations: A Pilot Feasibility Randomised Controlled Trial" Nutrients 14, no. 9: 1768. https://doi.org/10.3390/nu14091768
APA StyleThreapleton, D. E., Beer, S. L., Foley, D. J., Gibson, L. E., Trevillion, S., Burke, D., Wheatstone, P., Gath, J., Hex, N., Setters, J., Greenwood, D. C., & Cade, J. E. (2022). Usability of myfood24 Healthcare and Mathematical Diet Optimisation in Clinical Populations: A Pilot Feasibility Randomised Controlled Trial. Nutrients, 14(9), 1768. https://doi.org/10.3390/nu14091768