Evaluating Dietary Patterns in Women from Southern Italy and Western Mexico

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Populations
2.2. Dietary Assessment
2.3. Dietary Pattern Analysis
2.4. Anthropometric Assessment
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Italian and Mexican Women
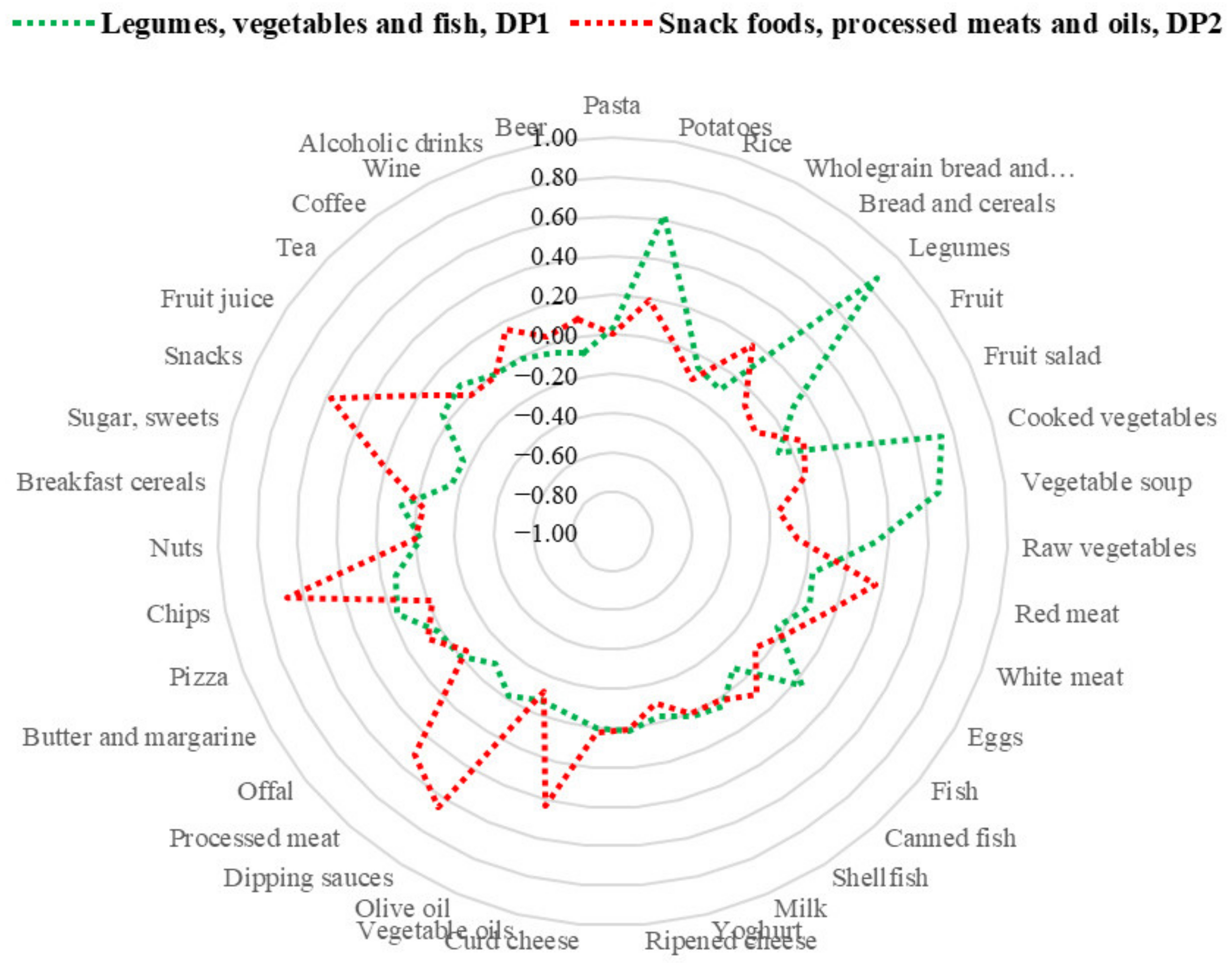
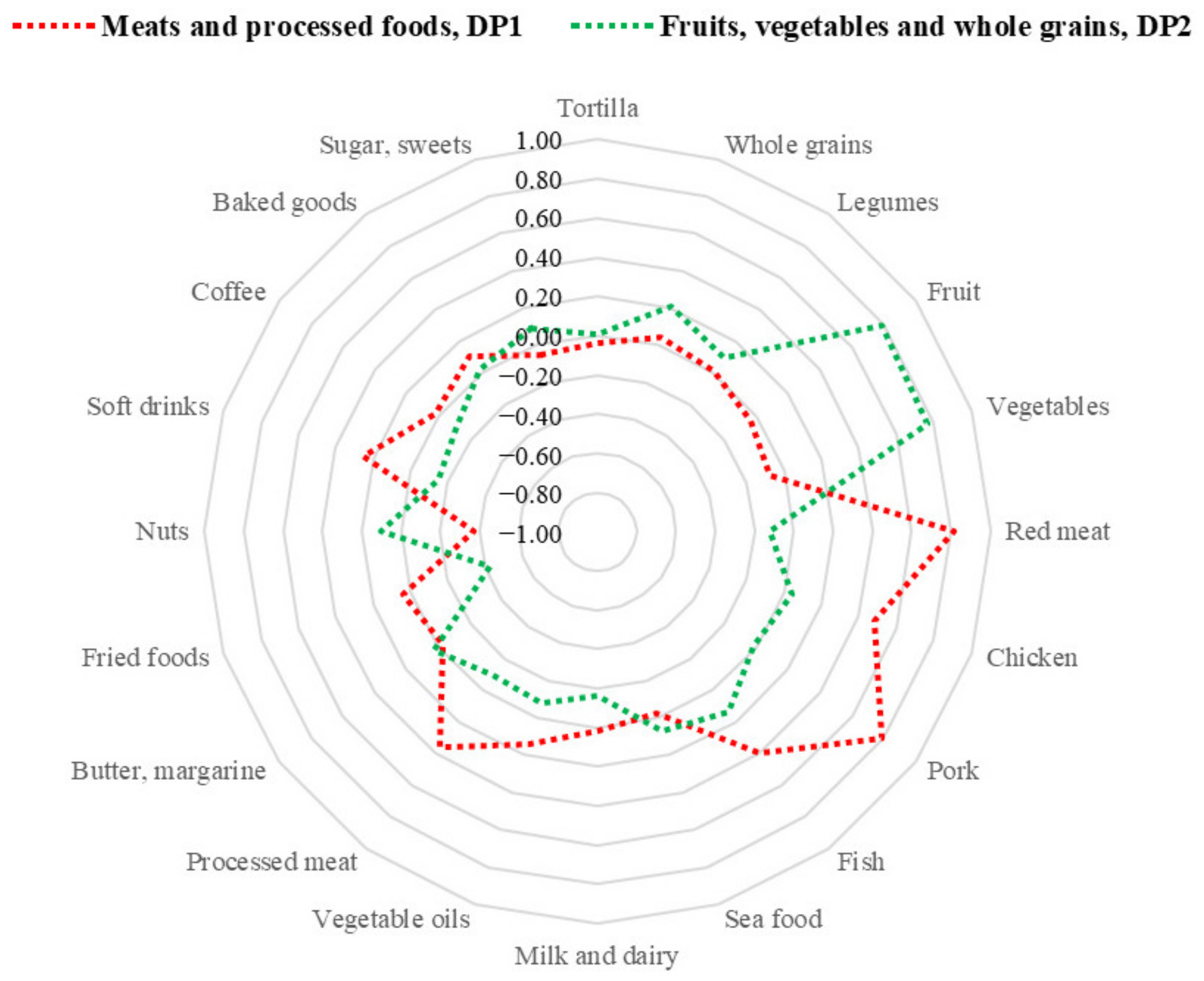
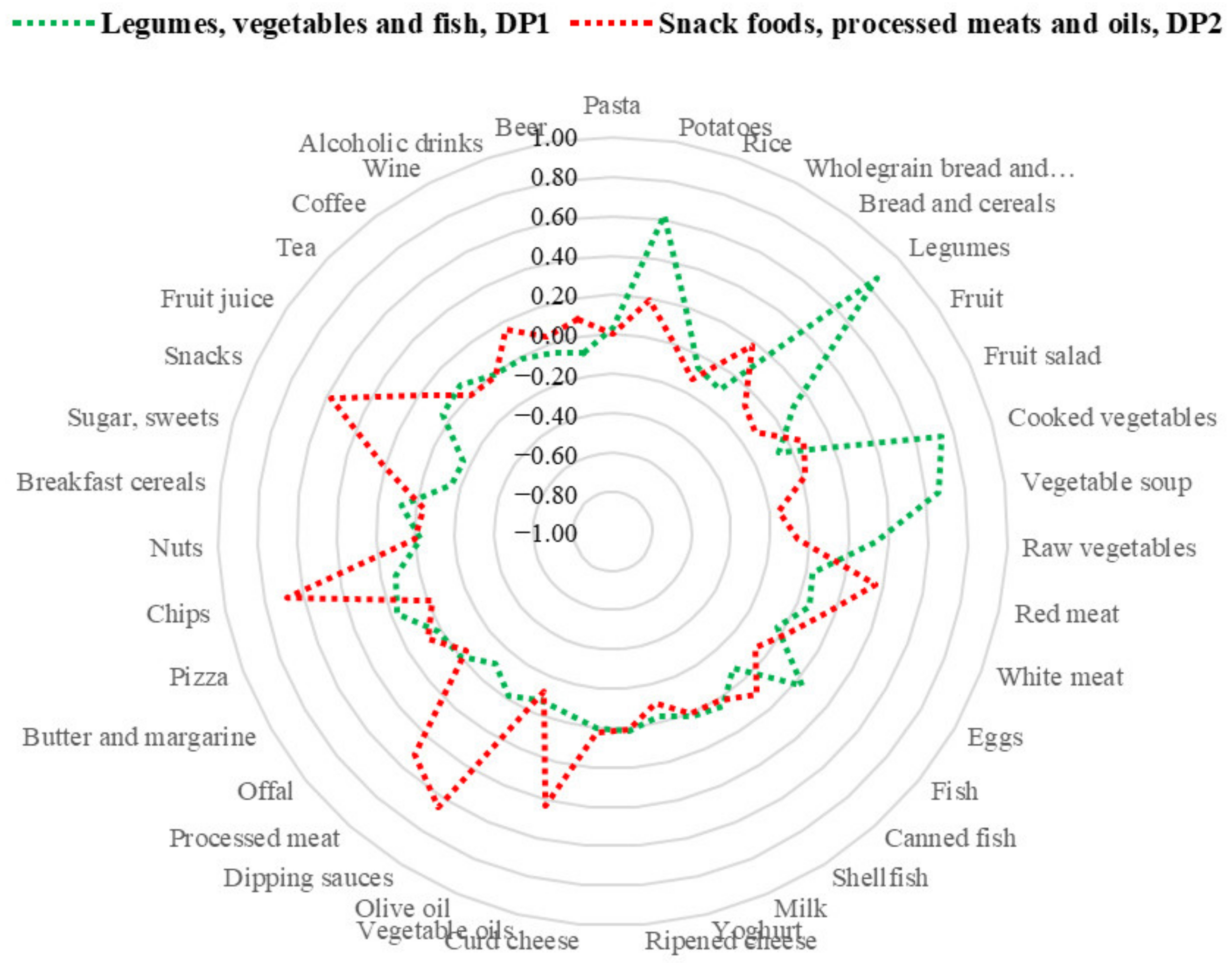
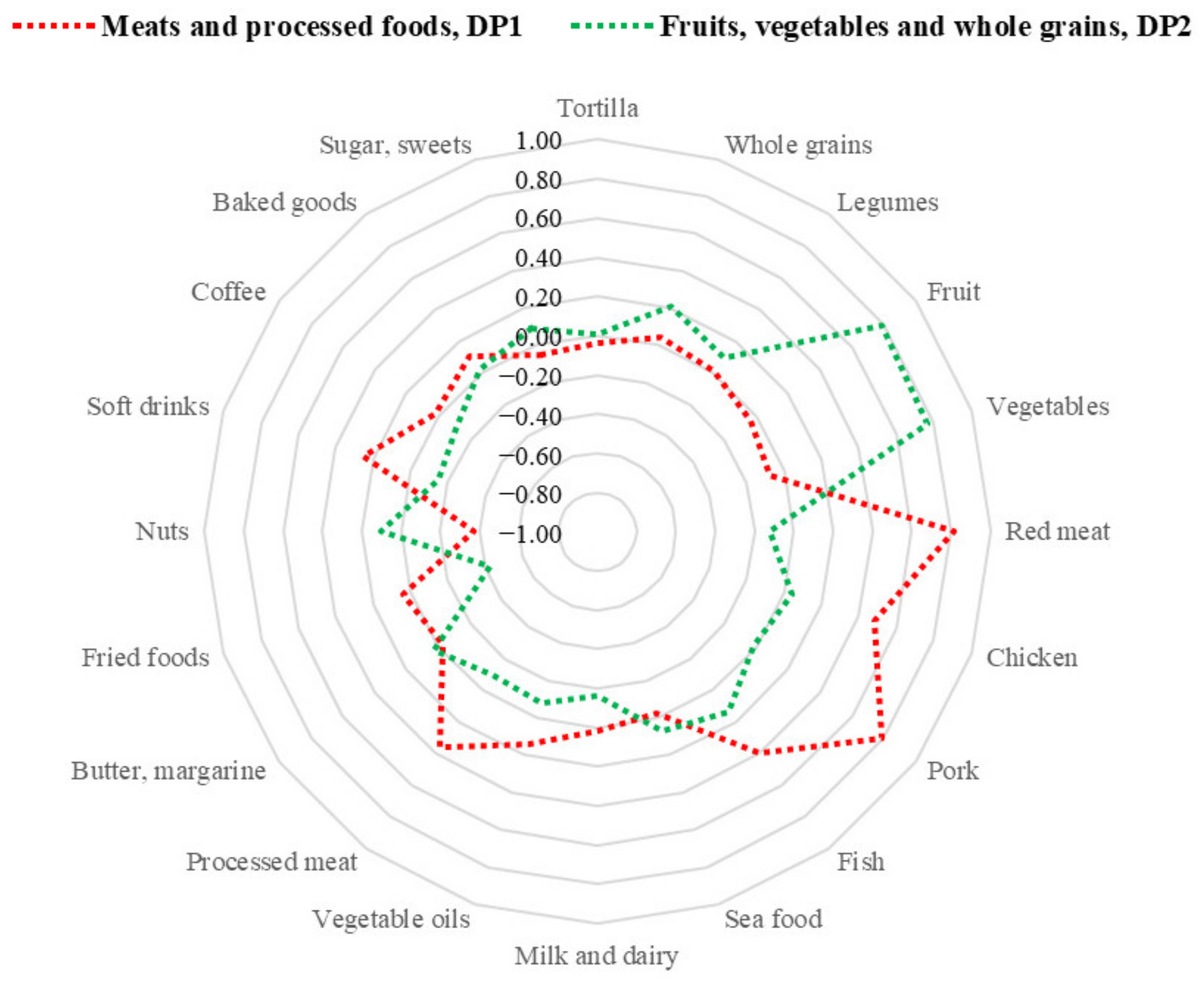
3.2. Dietary Patterns in Italian and Mexican Women
3.3. Characteristics of Italian and Mexican Women in Relation to Adherence to Dietary Patterns
3.4. Nutritional Content according to Adherence to Italian and Mexican Dietary Patterns
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karanikolos, M.; Adany, R.; McKee, M. The Epidemiological Transition in Eastern and Western Europe: A Historic Natural Experiment. Eur. J. Public Health 2017, 27, 4–8. [Google Scholar] [CrossRef] [PubMed]
- UNESCO. Available online: https://ich.unesco.org/en/decisions (accessed on 21 April 2021).
- UNESCO. Available online: https://ich.unesco.org/en/lists (accessed on 22 April 2021).
- Donini, L.M.; Serra-Majem, L.; Bulló, M.; Gil, Á.; Salas-Salvadó, J. The Mediterranean Diet: Culture, Health and Science. Br. J. Nutr. 2015, 113 (Suppl. 2), S1–S3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lăcătușu, C.-M.; Grigorescu, E.-D.; Floria, M.; Onofriescu, A.; Mihai, B.-M. The Mediterranean Diet: From an Environment-Driven Food Culture to an Emerging Medical Prescription. Int. J. Environ. Res. Public. Health 2019, 16, 942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burlingame, B.A.; Dernini, S.; Food and Agriculture Organization of the United Nations; Biodiversity International (Eds.) Sustainable Diets and Biodiversity: Directions and Solutions for Policy, Research and Action; FAO: Rome, Italy, 2012; ISBN 978-92-5-107311-7. [Google Scholar]
- Cussó Segura, X.; Garrabou Segura, R. La transición nutricional en la España contemporánea: Las variaciones en el consumo de pan, patatas y legumbres (1850–2000). Investigaciones Historia Económica 2007, 3, 69–100. [Google Scholar] [CrossRef]
- De Molina, M.G.; Soto, D.; Aguilera, E.; Infante, J. Crecimiento Agrario en España y Cambios en la Oferta Alimentaria, 1900–1933; Fundacion Instituto de Historia Social: Valencia, Spain, 2014; pp. 157–183. [Google Scholar]
- Medina-Albaladejo, F.J.; Calatayud, S. Children’s Diet during the Early Stages of the Nutritional Transition. The Foundlings in the Hospital of Valencia (Spain), 1852–1931. Int. J. Environ. Res. Public. Health 2021, 18, 11999. [Google Scholar] [CrossRef]
- Valerino-Perea, S.; Lara-Castor, L.; Armstrong, M.E.G.; Papadaki, A. Definition of the Traditional Mexican Diet and Its Role in Health: A Systematic Review. Nutrients 2019, 11, 2803. [Google Scholar] [CrossRef] [Green Version]
- Román, S.; Ojeda-Granados, C.; Panduro, A. Genética y evolución de la alimentación de la población en México. Rev. Endocrinol. Nutr. 2013, 21, 42–51. [Google Scholar]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean Diet and Health Status: Meta-Analysis. BMJ 2008, 337, a1344. [Google Scholar] [CrossRef] [Green Version]
- Vitale, M.; Giosuè, A.; Vaccaro, O.; Riccardi, G. Recent Trends in Dietary Habits of the Italian Population: Potential Impact on Health and the Environment. Nutrients 2021, 13, 476. [Google Scholar] [CrossRef]
- D’Errico, M.; Pavlova, M.; Spandonaro, F. The Economic Burden of Obesity in Italy: A Cost-of-Illness Study. Eur. J. Health Econ. 2021, 23, 177–192. [Google Scholar] [CrossRef]
- Barquera, S.; Rivera, J.A. Obesity in Mexico: Rapid Epidemiological Transition and Food Industry Interference in Health Policies. Lancet Diabetes Endocrinol. 2020, 8, 746–747. [Google Scholar] [CrossRef]
- Barquera, S.; Campos, I.; Rivera, J.A. Mexico Attempts to Tackle Obesity: The Process, Results, Push Backs and Future Challenges. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2013, 14 (Suppl. 2), 69–78. [Google Scholar] [CrossRef] [Green Version]
- Buscemi, S.; Corleo, D.; Galvano, F.; De Lorenzo, A. Chapter 26—The Mediterranean Diet and Its Individual Components: Linking with Obesity in Italy. In The Mediterranean Diet, 2nd ed.; Preedy, V.R., Watson, R.R., Eds.; Academic Press: New York, NY, USA, 2020; pp. 285–292. ISBN 978-0-12-818649-7. [Google Scholar]
- Bach, A.; Serra-Majem, L.; Carrasco, J.L.; Roman, B.; Ngo, J.; Bertomeu, I.; Obrador, B. The Use of Indexes Evaluating the Adherence to the Mediterranean Diet in Epidemiological Studies: A Review. Public Health Nutr. 2006, 9, 132–146. [Google Scholar] [CrossRef]
- Valerino-Perea, S.; Armstrong, M.E.G.; Papadaki, A. Development of an Index to Assess Adherence to the Traditional Mexican Diet Using a Modified Delphi Method. Public Health Nutr. 2021, 24, 4387–4396. [Google Scholar] [CrossRef]
- Waxman, A. World Health Assembly. WHO Global Strategy on Diet, Physical Activity and Health. Food Nutr. Bull. 2004, 25, 292–302. [Google Scholar] [CrossRef]
- Barchitta, M.; Maugeri, A.; Quattrocchi, A.; Agrifoglio, O.; Scalisi, A.; Agodi, A. The Association of Dietary Patterns with High-Risk Human Papillomavirus Infection and Cervical Cancer: A Cross-Sectional Study in Italy. Nutrients 2018, 10, 469. [Google Scholar] [CrossRef] [Green Version]
- Maugeri, A.; Barchitta, M.; Fiore, V.; Rosta, G.; Favara, G.; La Mastra, C.; La Rosa, M.C.; Magnano San Lio, R.; Agodi, A. Determinants of Adherence to the Mediterranean Diet: Findings from a Cross-Sectional Study in Women from Southern Italy. Int. J. Environ. Res. Public. Health 2019, 16, 2963. [Google Scholar] [CrossRef] [Green Version]
- Ojeda-Granados, C.; Panduro, A.; Gonzalez-Aldaco, K.; Rivera-Iñiguez, I.; Campos-Medina, L.; Roman, S. Adherence to a Fish-Rich Dietary Pattern Is Associated with Chronic Hepatitis C Patients Showing Low Viral Load: Implications for Nutritional Management. Nutrients 2021, 13, 3337. [Google Scholar] [CrossRef]
- USDA. USDA National Nutrient Database for Standard Reference, Release 24; USDA Nutrient Data Laboratory: Beltsville, MD, USA, 2011.
- Pérez Lizaur, A.B.; Palacios González, B.; Castro Becerra, A.L.; Flores Galicia, I. Sistema Mexicano de Alimentos Equivalentes, 4th ed.; Cuadernos de Nutrición (Fomento de Nutrición y Salud, A.C.): Mexico City, Mexico, 2011; ISBN 978-607-00-7928-3. [Google Scholar]
- Denova-Gutiérrez, E.; Ramírez-Silva, I.; Rodríguez-Ramírez, S.; Jiménez-Aguilar, A.; Shamah-Levy, T.; Rivera-Dommarco, J.A. Validity of a Food Frequency Questionnaire to Assess Food Intake in Mexican Adolescent and Adult Population. Salud Pública México 2016, 58, 617–628. [Google Scholar] [CrossRef]
- Dernini, S.; Berry, E.M.; Serra-Majem, L.; Vecchia, C.L.; Capone, R.; Medina, F.X.; Aranceta-Bartrina, J.; Belahsen, R.; Burlingame, B.; Calabrese, G.; et al. Med Diet 4.0: The Mediterranean Diet with Four Sustainable Benefits. Public Health Nutr. 2017, 20, 1322–1330. [Google Scholar] [CrossRef]
- Castellanos-Gutiérrez, A.; Sánchez-Pimienta, T.G.; Batis, C.; Willett, W.; Rivera, J.A. Toward a Healthy and Sustainable Diet in Mexico: Where Are We and How Can We Move Forward? Am. J. Clin. Nutr. 2021, 113, 1177–1184. [Google Scholar] [CrossRef] [PubMed]
- Denoth, F.; Scalese, M.; Siciliano, V.; Di Renzo, L.; De Lorenzo, A.; Molinaro, S. Clustering Eating Habits: Frequent Consumption of Different Dietary Patterns among the Italian General Population in the Association with Obesity, Physical Activity, Sociocultural Characteristics and Psychological Factors. Eat. Weight Disord. EWD 2016, 21, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Flores, M.; Macias, N.; Rivera, M.; Lozada, A.; Barquera, S.; Rivera-Dommarco, J.; Tucker, K.L. Dietary Patterns in Mexican Adults Are Associated with Risk of Being Overweight or Obese. J. Nutr. 2010, 140, 1869–1873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno-Altamirano, L.; Hernández-Montoya, D.; Soto-Estrada, G.; García-García, J.J.; Silberman, M.; Capraro, S.; Panico, S. Changes in Mediterranean Dietary Patterns in Italy from 1961 to 2011. Mediterr. J. Nutr. Metab. 2016, 9, 171–181. [Google Scholar] [CrossRef]
- Rivera, J.A.; Barquera, S.; Campirano, F.; Campos, I.; Safdie, M.; Tovar, V. Epidemiological and Nutritional Transition in Mexico: Rapid Increase of Non-Communicable Chronic Diseases and Obesity. Public Health Nutr. 2002, 5, 113–122. [Google Scholar] [CrossRef]
- Maugeri, A.; Barchitta, M.; Favara, G.; La Rosa, M.C.; La Mastra, C.; Magnano San Lio, R.; Agodi, A. Maternal Dietary Patterns Are Associated with Pre-Pregnancy Body Mass Index and Gestational Weight Gain: Results from the “Mamma & Bambino” Cohort. Nutrients 2019, 11, 1308. [Google Scholar] [CrossRef] [Green Version]
- Barchitta, M.; Maugeri, A.; Magnano San Lio, R.; Favara, G.; La Rosa, M.C.; La Mastra, C.; Quattrocchi, A.; Agodi, A. Dietary Patterns Are Associated with Leukocyte LINE-1 Methylation in Women: A Cross-Sectional Study in Southern Italy. Nutrients 2019, 11, 1843. [Google Scholar] [CrossRef] [Green Version]
- Moreno-Altamirano, L.; García-García, J.J.; Salvatore, P.; Soto-Estrada, G.; Hernández-Montoya, D. Metabolic Syndrome: Changes in Mediterranean and Mesoamerican Diet Due to Socioeconomic Factors in Mexico and Italy. Mediterr. J. Nutr. Metab. 2017, 10, 49–59. [Google Scholar] [CrossRef]
- Pérez-Tepayo, S.; Rodríguez-Ramírez, S.; Unar-Munguía, M.; Shamah-Levy, T. Trends in the Dietary Patterns of Mexican Adults by Sociodemographic Characteristics. Nutr. J. 2020, 19, 51. [Google Scholar] [CrossRef]
- Moreno-Altamirano, L.; Sapienza, E. Food Patterns, Diabetes and Overweight/Obesity and Some Socio-Economic Indicators in the Italy Regions. J. Nutr. Food Sci. 2018, 8, 1000679. [Google Scholar]
- Medicine, I. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; The National Academies Press: Washington, DC, USA, 2005; ISBN 978-0-309-08525-0. [Google Scholar]
- Vitale, M.; Masulli, M.; Calabrese, I.; Rivellese, A.A.; Bonora, E.; Signorini, S.; Perriello, G.; Squatrito, S.; Buzzetti, R.; Sartore, G.; et al. Impact of a Mediterranean Dietary Pattern and Its Components on Cardiovascular Risk Factors, Glucose Control, and Body Weight in People with Type 2 Diabetes: A Real-Life Study. Nutrients 2018, 10, 1067. [Google Scholar] [CrossRef] [Green Version]
- Barchitta, M.; Maugeri, A.; Magnano San Lio, R.; Favara, G.; La Mastra, C.; La Rosa, M.C.; Agodi, A. Dietary Folate Intake and Folic Acid Supplements among Pregnant Women from Southern Italy: Evidence from the “Mamma & Bambino” Cohort. Int. J. Environ. Res. Public. Health 2020, 17, 638. [Google Scholar] [CrossRef] [Green Version]
- Guéant-Rodriguez, R.-M.; Guéant, J.-L.; Debard, R.; Thirion, S.; Hong, L.X.; Bronowicki, J.-P.; Namour, F.; Chabi, N.W.; Sanni, A.; Anello, G.; et al. Prevalence of Methylenetetrahydrofolate Reductase 677T and 1298C Alleles and Folate Status: A Comparative Study in Mexican, West African, and European Populations. Am. J. Clin. Nutr. 2006, 83, 701–707. [Google Scholar] [CrossRef] [Green Version]
- Girelli, D.; Martinelli, N.; Pizzolo, F.; Friso, S.; Olivieri, O.; Stranieri, C.; Trabetti, E.; Faccini, G.; Tinazzi, E.; Pignatti, P.F.; et al. The Interaction between MTHFR 677 C→T Genotype and Folate Status Is a Determinant of Coronary Atherosclerosis Risk. J. Nutr. 2003, 133, 1281–1285. [Google Scholar] [CrossRef] [Green Version]
- Ibarra-Lopez, J.J.; Duarte, P.; Antonio-Vejar, V.; Calderon-Aranda, E.S.; Huerta-Beristain, G.; Flores-Alfaro, E.; Moreno-Godinez, M.E. Maternal C677T MTHFR Polymorphism and Environmental Factors Are Associated with Cleft Lip and Palate in a Mexican Population. J. Investig. Med. Off. Publ. Am. Fed. Clin. Res. 2013, 61, 1030–1035. [Google Scholar] [CrossRef]
- Baldini, M.; Pasqui, F.; Bordoni, A.; Maranesi, M. Is the Mediterranean Lifestyle Still a Reality? Evaluation of Food Consumption and Energy Expenditure in Italian and Spanish University Students. Public Health Nutr. 2009, 12, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Grosso, G.; Marventano, S.; Buscemi, S.; Scuderi, A.; Matalone, M.; Platania, A.; Giorgianni, G.; Rametta, S.; Nolfo, F.; Galvano, F.; et al. Factors Associated with Adherence to the Mediterranean Diet among Adolescents Living in Sicily, Southern Italy. Nutrients 2013, 5, 4908–4923. [Google Scholar] [CrossRef] [Green Version]
- Betancourt-Nuñez, A.; Márquez-Sandoval, F.; González-Zapata, L.I.; Babio, N.; Vizmanos, B. Unhealthy Dietary Patterns among Healthcare Professionals and Students in Mexico. BMC Public Health 2018, 18, 1246. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | Italian Women (n = 811) | Age Tertile | p-Value | ||
|---|---|---|---|---|---|
| 18–33 Years | 34–46 Years | 47–72 Years | |||
| Age, years | 40.0 (19) | 28.0 (6.0) | 40.0 (6) | 54.0 (11) | <0.001 |
| Weight, kg | 60.0 (15.0) | 57.0 (15.0) | 60.0 (15.0) | 63.0 (13.0) | <0.001 |
| BMI, kg/m2 | 22.9 (5.2) | 21.2 (5.0) | 22.9 (4.8) | 24.2 (5.1) | <0.001 |
| Underweight, n (%) | 56 (7.0) | 36 (13.7) | 16 (5.6) | 4 (1.6) | <0.001 |
| Normal weight, n (%) | 490 (60.9) | 168 (64.1) | 186 (64.8) | 136 (53.1) | |
| Overweight, n (%) | 175 (21.7) | 37 (14.1) | 56 (19.5) | 82 (32.0) | |
| Obesity, n (%) | 84 (10.4) | 21 (8.1) | 29 (10.1) | 34 (13.3) | |
| Characteristic | Mexican Women (n = 215) | Age Tertile | p-Value | ||
|---|---|---|---|---|---|
| 18–31 Years | 32–45 Years | 46–72 Years | |||
| Age, years | 40.0 (21) | 23.0 (7.0) | 40.0 (5) | 53.0 (11) | <0.001 |
| Weight, kg | 72.0 (21.0) | 66.0 (23.0) a | 76.5 (20.0) | 74.0 (19.8) | 0.005 |
| Body fat, % | 36.8 (10.5) | 32.7 (12.5) b | 38.3 (7.0) | 38.3 (9.5) | <0.001 |
| BMI, kg/m2 | 29.4 (8.8) | 25.5 (8.9) c | 30.2 (6.5) | 31.0 (8.1) | <0.001 |
| Normal weight, n (%) | 53 (24.7) | 34 (49.3) | 10 (14.3) | 9 (11.8) | <0.001 |
| Overweight, n (%) | 60 (27.9) | 17 (24.6) | 21 (30.0) | 22 (28.9) | |
| Obesity, n (%) | 102 (47.4) | 18 (26.1) | 39 (55.7) | 45 (59.3) | |
| Characteristic | Adherence to Dietary Patterns | p-Value | ||||
|---|---|---|---|---|---|---|
| Exclusively “Snack Foods, Processed Meats, and Oils, DP2” (n = 85) | Preferably “Snack Foods, Processed Meats, and Oils, DP2” (n = 178) | No Preference (n = 285) | Preferably “Legumes, Vegetables, and Fish, DP1” (n = 178) | Exclusively “Legumes, Vegetables, and Fish, DP1” (n = 85) | ||
| Age, years | 38.0 (14.0) a | 37.0 (17.0) b | 40.0 (20.0) | 42.0 (21.0) | 42.0 (18.0) | 0.001 |
| Weight, kg | 58.0 (11.8) | 60.0 (15.8) | 60.0 (16.0) | 62.0 (13.5) | 62.5 (15.0) | 0.065 |
| BMI, kg/m2 | 22.1 (5.5) | 22.6 (4.9) | 23.1 (6.2) | 23.0 (5.0) | 23.1 (6.2) | 0.273 |
| Underweight, n (%) | 8 (14.3) | 16 (28.6) | 20 (35.7) | 8 (14.3) | 4 (4.8) | 0.933 |
| Normal weight, n (%) | 51 (10.4) | 105 (21.4) | 171 (34.9) | 113 (23.1) | 50 (10.2) | |
| Overweight, n (%) | 18 (10.3) | 38 (21.7) | 62 (35.4) | 36 (20.6) | 21 (12.0) | |
| Obesity, n (%) | 84 (10.4) | 176 (21.9) | 285 (35.4) | 176 (21.9) | 84 (10.4) | |
| Characteristic | Adherence to Dietary Patterns | p-Value | ||||
|---|---|---|---|---|---|---|
| Exclusively “Meats and Processed Foods, DP1” (n = 26) | Preferably “Meats and Processed Foods, DP1” (n = 40) | No Preference (n = 80) | Preferably “Fruits, Vegetables, and Whole Grains, DP2” (n = 46) | Exclusively “Fruits, Vegetables, and Whole Grains, DP2” (n = 23) | ||
| Age, years | 41.0 (21.0) | 37.5 (22.0) a | 41.0 (21.0) | 40.0 (21.0) | 45.0 (29.0) | 0.109 |
| Weight, kg | 77.0 (31.3) | 75.1 (17.8) | 72.5 (21.3) | 71.5 (18.8) | 68.0 (15.0) | 0.363 |
| Body fat, % | 38.5 (16.9) | 38.0 (8.8) | 37.5 (9.7) | 34.8 (9.4) | 35.6 (8.8) | 0.186 |
| BMI, kg/m2 | 32.1 (12.6) | 29.5 (7.9) | 29.9 (9.5) | 28.7 (7.5) | 26.7 (6.8) | 0.461 |
| Normal weight, n (%) | 8 (15.4) | 8 (15.4) | 16 (30.8) | 12 (23.1) | 8 (15.4) | 0.396 |
| Overweight, n (%) | 3 (5.0) | 12 (20.0) | 21 (35.0) | 16 (26.7) | 8 (13.3) | |
| Obesity, n (%) | 15 (15.5) | 20 (20.6) | 37 (38.1) | 18 (18.6) | 7 (7.2) | |
| Nutrients | Adherence to Italian Dietary Patterns | p-Value | ||||
|---|---|---|---|---|---|---|
| Exclusively “Snack Foods, Processed Meats, and Oils, DP2” (n = 85) | Preferably “Snack Foods, Processed Meats, and Oils, DP2” (n = 178) | No Preference (n = 285) | Preferably “Legumes, Vegetables, and Fish, DP1” (n = 178) | Exclusively “Legumes, Vegetables, and Fish, DP1” (n = 85) | ||
| Total energy, kcal | 2015.4 (634.0) | 1878.9 (639.0) | 1916.2 (805.2) | 1940.8 (661.1) | 1942.1 (548.6) | 0.719 |
| SFAs, % | 25.4 (10.2) | 23.7 (13.2) | 23.0 (11.7) | 23.7 (10.6) | 22.6 (8.9) | 0.161 |
| MUFAs, % | 44.9 (19.8) | 43.4 (23.9) | 43.9 (23.1) | 45.1 (22.5) | 39.8 (22.2) | 0.675 |
| PUFAs, % | 14.5 (6.5) | 13.5 (6.2) | 12.8 (5.3) | 12.7 (4.5) a | 12.4 (5.0) a | 0.001 |
| Folates, µg/d DFEs | 184.7 (99.0) | 230.1 (112.0) | 264.7 (153.2) | 319.3 (172.5) b | 404.6 (146.1) b | <0.001 |
| Vitamin A, µg/d | 762.9 (471.6) | 889.7 (558.3) | 1057.8 (849.1) | 1276.3 (911.6) c | 1675.0 (944.0) c | <0.001 |
| Vitamin C, mg/d | 95.2 (96.8) | 88.7 (98.3) | 109.5 (122.3) | 132.6 (139.9) d | 149.3 (161.3) d | <0.001 |
| Vitamin D, µg/d | 3.8 (3.9) | 3.8 (3.3) | 4.3 (5.5) | 4.9 (5.6) e | 7.4 (5.5) f | <0.001 |
| Thiamin, mg/d | 1.4 (0.6) | 1.4 (0.6) | 1.5 (0.7) | 1.5 (0.6) | 1.5 (0.5) | 0.054 |
| Pyridoxine, mg/d | 1.9 (0.7) | 1.9 (0.9) | 1.9 (1.0) | 2.0 (1.0) g | 2.3 (0.8) h | <0.001 |
| Calcium, mg/d | 743.9 (385.1) | 816.1 (444.6) | 825.6 (503.2) | 872.3 (384.5) i | 930.9 (416.9) i | 0.007 |
| Iron, mg/d | 11.2 (4.8) | 12.0 (5.9) | 12.8 (7.7) | 13.8 (6.9) j | 14.6 (6.5) j | <0.001 |
| Magnesium, mg/d | 262.7 (97.0) | 284.0 (99.0) | 296.4 (137.7) | 307.8 (122.0) k | 346.3 (98.5) l | <0.001 |
| Zinc, mg/d | 8.8 (3.7) | 8.6 (3.6) | 8.7 (4.5) | 8.9 (3.4) | 9.5 (3.0) m | 0.039 |
| Nutrients | Adherence to Mexican Dietary Patterns | p-Value | ||||
|---|---|---|---|---|---|---|
| Exclusively “Meats and Processed Foods, DP1” (n = 26) | Preferably “Meats and Processed Foods, DP1” (n = 40) | No Preference (n = 80) | Preferably “Fruits, Vegetables, and Whole Grains, DP2” (n = 46) | Exclusively “Fruits, Vegetables, and Whole Grains, DP2” (n = 23) | ||
| Total energy, kcal | 1866.5 (1001.5) | 1804.5 (635.5) | 1896.5 (806.5) | 1754.0 (555.5) | 1717.0 (518.0) | 0.731 |
| Protein, % | 17.5 (9.0) | 16.0 (4.3) | 17.0 (6.0) | 17.0 (4.3) | 17.0 (7.0) | 0.828 |
| Total fat, % | 36.0 (12.3) | 33.0 (11.0) | 34.0 (12.8) | 30.0 (14.5) | 31.0 (20.0) | 0.371 |
| SFAs, % | 10.0 (6.0) | 10.0 (5.3) | 10.0 (6.0) | 9.0 (5.5) | 6.0 (6.0) a | 0.013 |
| MUFAs, % | 11.0 (7.3) | 10.0 (5.5) | 10.0 (6.8) | 9.5 (6.3) | 9.0 (11.0) | 0.980 |
| PUFAs, % | 5.0 (4.8) | 4.0 (3.0) | 4.0 (2.0) | 5.0 (4.0) | 4.0 (5.0) | 0.894 |
| Cholesterol, mg | 308.5 (299.8) | 245.0 (195.8) | 211.0 (836.0) | 207.5 (148.3) | 260.0 (249.0) | 0.557 |
| Carbohydrates, % | 49.0 (9.8) | 52.0 (11.3) | 51.5 (15.0) | 53.5 (12.5) | 54.0 (13.0) | 0.407 |
| Fiber, g/d | 15.5 (15.3) | 18.0 (15.0) | 18.0 (18.0) | 19.0 (18.0) | 20.0 (17.0) | 0.408 |
| Folates, µg/d DFEs | 114.9 (113.6) | 85.2 (70.4) | 148.1 (133.3) | 177.0 (149.8) b | 238.9 (248.8) b | <0.001 |
| Vitamin A, µg/d | 585.0 (1374.0) | 364.5 (910.0) | 733.0 (1349.0) | 665.0 (1082.0) | 840.0 (1602.0) | 0.087 |
| Vitamin C, mg/d | 41.2 (117.1) | 38.6 (97.5) | 55.2 (100.2) | 94.0 (109.7) c | 158.8 (232.5) c | 0.002 |
| Vitamin E, mg/d | 2.2 (3.2) | 1.4 (1.8) | 2.2 (3.4) | 2.1 (2.6) | 2.4 (2.0) | 0.363 |
| Thiamin, mg/d | 1.1 (0.7) | 0.9 (0.7) | 1.2 (0.9) | 1.2 (0.6) | 1.1 (0.8) | 0.038 |
| Riboflavin, mg/d | 1.2 (0.7) | 1.0 (0.7) | 1.3 (1.0) | 1.4 (0.9) | 1.2 (0.8) | 0.181 |
| Niacin, mg/d | 18.5 (17.5) | 11.2 (11.7) | 14.5 (12.9) | 15.8 (12.4) | 15.6 (9.3) | 0.424 |
| Pyridoxine, mg/d | 1.1 (0.9) | 1.1 (1.1) | 1.1 (0.9) | 1.6 (0.9) d | 1.4 (1.4) | 0.006 |
| Cobalamin, µg/d | 2.5 (4.4) | 2.4 (1.8) | 2.4 (2.2) | 2.3 (3.1) | 1.7 (1.9) | 0.531 |
| Pantothenic acid, mg/d | 1.8 (1.2) | 1.7 (1.5) | 2.1 (1.6) | 2.0 (1.6) | 2.4 (1.9) | 0.487 |
| Calcium, mg/d | 959.5 (732.0) | 889.5 (501.0) | 938.0 (543.0) | 869.5 (460.0) | 932.0 (764.0) | 0.646 |
| Iron, mg/d | 11.3 (10.2) | 12.3 (6.3) | 14.2 (9.9) | 13.9 (10.6) | 13.6 (7.0) | 0.442 |
| Sodium, g/d | 1.9 (2.0) | 2.0 (1.1) | 2.1 (1.7) | 1.7 (1.3) | 1.5 (1.4) | 0.146 |
| Potassium, mg/d | 1576.5 (990.0) | 1707.5 (869.0) | 1966.0 (1199.0) | 2351.0 (1207.0) e | 2352.0 (1580.0) f | 0.003 |
| Selenium, µg/d | 41.0 (45.0) | 36.0 (27.0) | 45.0 (41.0) | 37.5 (39.0) | 41.0 (33.0) | 0.286 |
| Phosphorus, mg/d | 583.0 (473.0) | 620.0 (412.0) | 737.0 (451.0) | 705.0 (485.0) | 690.0 (641.0) | 0.781 |
| Magnesium, mg/d | 171.5 (285.0) | 185.5 (233.0) | 224.0 (273.0) | 258.5 (186.0) | 244.0 (182.0) | 0.377 |
| Zinc, mg/d | 6.2 (6.9) | 6.2 (5.7) | 6.5 (4.2) | 6.4 (5.2) | 5.9 (3.6) | 0.615 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ojeda-Granados, C.; Barchitta, M.; La Rosa, M.C.; La Mastra, C.; Roman, S.; Panduro, A.; Agodi, A.; Maugeri, A. Evaluating Dietary Patterns in Women from Southern Italy and Western Mexico. Nutrients 2022, 14, 1603. https://doi.org/10.3390/nu14081603
Ojeda-Granados C, Barchitta M, La Rosa MC, La Mastra C, Roman S, Panduro A, Agodi A, Maugeri A. Evaluating Dietary Patterns in Women from Southern Italy and Western Mexico. Nutrients. 2022; 14(8):1603. https://doi.org/10.3390/nu14081603
Chicago/Turabian StyleOjeda-Granados, Claudia, Martina Barchitta, Maria Clara La Rosa, Claudia La Mastra, Sonia Roman, Arturo Panduro, Antonella Agodi, and Andrea Maugeri. 2022. "Evaluating Dietary Patterns in Women from Southern Italy and Western Mexico" Nutrients 14, no. 8: 1603. https://doi.org/10.3390/nu14081603
APA StyleOjeda-Granados, C., Barchitta, M., La Rosa, M. C., La Mastra, C., Roman, S., Panduro, A., Agodi, A., & Maugeri, A. (2022). Evaluating Dietary Patterns in Women from Southern Italy and Western Mexico. Nutrients, 14(8), 1603. https://doi.org/10.3390/nu14081603