
Calcium, Magnesium, and Zinc Supplementation during Pregnancy: The Additive Value of Micronutrients on Maternal Immune Response after SARS-CoV-2 Infection

 ,
,  , , , ,
, , , ,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
2.2. Inclusion Criteria and Study Variables
2.3. Statistical Analysis
3. Results
3.1. Background Analysis
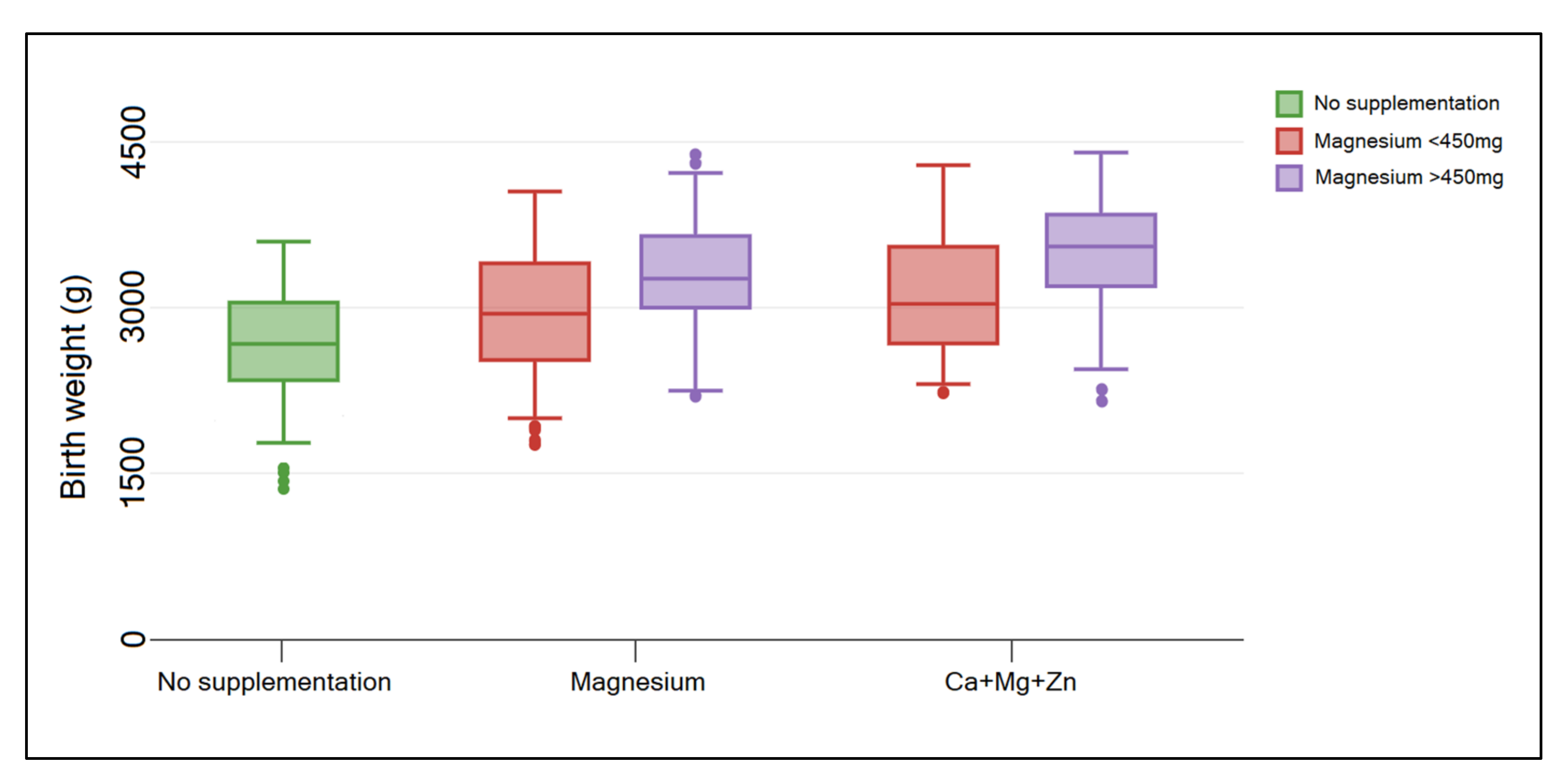
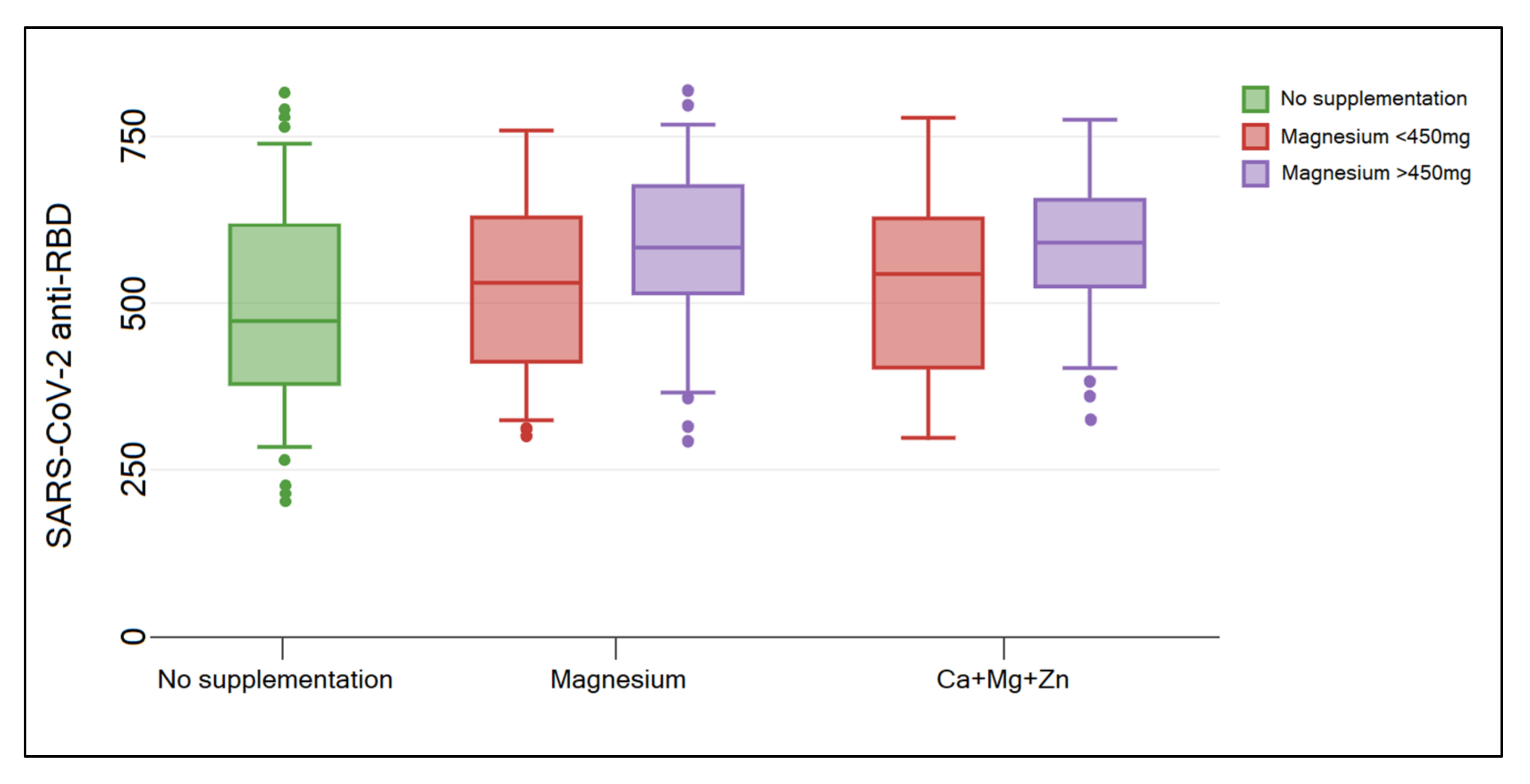
3.2. Analysis of Magnesium Supplementation Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mostafa, A.; Kandeil, A.; Shehata, M.; El Shesheny, R.; Samy, A.M.; Kayali, G.; Ali, M.A. Middle East Respiratory Syndrome Coronavirus (MERS-CoV): State of the Science. Microorganisms 2020, 8, 991. [Google Scholar] [CrossRef] [PubMed]
- Karmouty-Quintana, H.; Thandavarayan, R.A.; Keller, S.P.; Sahay, S.; Pandit, L.M.; Akkanti, B. Emerging Mechanisms of Pulmonary Vasoconstriction in SARS-CoV-2-Induced Acute Respiratory Distress Syndrome (ARDS) and Potential Therapeutic Targets. Int. J. Mol. Sci. 2020, 21, 8081. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Liang, W.H.; Zhao, Y.; Liang, H.R.; Chen, Z.S.; Li, Y.M.; Liu, X.Q.; Chen, R.C.; Tang, C.L.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabaan, A.A.; Al-Ahmed, S.H.; Muhammad, J.; Khan, A.; Sule, A.A.; Tirupathi, R.; Mutair, A.A.; Alhumaid, S.; Al-Omari, A.; Dhawan, M.; et al. Role of Inflammatory Cytokines in COVID-19 Patients: A Review on Molecular Mechanisms, Immune Functions, Immunopathology and Immunomodulatory Drugs to Counter Cytokine Storm. Vaccines 2021, 9, 436. [Google Scholar] [CrossRef]
- Kudlay, D.; Kofiadi, I.; Khaitov, M. Peculiarities of the T Cell Immune Response in COVID-19. Vaccines 2022, 10, 242. [Google Scholar] [CrossRef]
- Zanza, C.; Romenskaya, T.; Manetti, A.C.; Franceschi, F.; La Russa, R.; Bertozzi, G.; Maiese, A.; Savioli, G.; Volonnino, G.; Longhitano, Y. Cytokine Storm in COVID-19: Immunopathogenesis and Therapy. Medicina 2022, 58, 144. [Google Scholar] [CrossRef]
- Skirrow, H.; Barnett, S.; Bell, S.; Riaposova, L.; Mounier-Jack, S.; Kampmann, B.; Holder, B. Women’s views on accepting COVID-19 vaccination during and after pregnancy, and for their babies: A multi-methods study in the UK. BMC Pregnancy Childbirth 2022, 22, 33. [Google Scholar] [CrossRef]
- Alsaffar, W.A.; Alwesaibi, A.A.; Alhaddad, M.J.; Alsenan, Z.K.; Alsheef, H.J.; Alramadan, S.H.; Aljassas, H.A.; Alsaghirat, M.A.; Alzahrani, H.J. The Effectiveness of COVID-19 Vaccines in Improving the Outcomes of Hospitalized COVID-19 Patients. Cureus 2022, 14, e21485. [Google Scholar] [CrossRef]
- Citu, I.M.; Citu, C.; Gorun, F.; Sas, I.; Tomescu, L.; Neamtu, R.; Motoc, A.; Gorun, O.M.; Burlea, B.; Bratosin, F.; et al. Immunogenicity Following Administration of BNT162b2 and Ad26.COV2.S COVID-19 Vaccines in the Pregnant Population during the Third Trimester. Viruses 2022, 14, 307. [Google Scholar] [CrossRef]
- Wen, W.; Chen, C.; Tang, J.; Wang, C.; Zhou, M.; Cheng, Y.; Zhou, X.; Wu, Q.; Zhang, X.; Feng, Z.; et al. Efficacy and safety of three new oral antiviral treatment (molnupiravir, fluvoxamine and Paxlovid) for COVID-19: A meta-analysis. Ann. Med. 2022, 54, 516–523. [Google Scholar] [CrossRef]
- Vimercati, A.; De Nola, R.; Trerotoli, P.; Metta, M.E.; Cazzato, G.; Resta, L.; Malvasi, A.; Lepera, A.; Ricci, I.; Capozza, M.; et al. COVID-19 Infection in Pregnancy: Obstetrical Risk Factors and Neonatal Outcomes—A Monocentric, Single-Cohort Study. Vaccines 2022, 10, 166. [Google Scholar] [CrossRef] [PubMed]
- Gorun, F.; Motoi, S.; Malita, D.; Navolan, D.B.; Nemescu, D.; Olariu, T.R.; Craina, M.; Vilibic-Cavlek, T.; Ciohat, I.; Boda, D.; et al. Cytomegalovirus seroprevalence in pregnant women in the western region of Romania: A large-scale study. Exp. Ther. Med. 2020, 20, 2439–2443. [Google Scholar] [CrossRef] [PubMed]
- Álvarez Bartolomé, A.; Abdallah Kassab, N.A.; Cruz Melguizo, S.; de la Cruz Conty, M.L.; Forcen Acebal, L.; Abascal Saiz, A.; Pintado Recarte, P.; Martinez Varea, A.; Cerrillos Gonzalez, L.; García Fernández, J.; et al. Critical Care in SARS-CoV-2 Infected Pregnant Women: A Prospective Multicenter Study. Biomedicines 2022, 10, 475. [Google Scholar] [CrossRef] [PubMed]
- Cruz Melguizo, S.; de la Cruz Conty, M.L.; Carmona Payán, P.; Abascal-Saiz, A.; Pintando Recarte, P.; González Rodríguez, L.; Cuenca Marín, C.; Martínez Varea, A.; Oreja Cuesta, A.B.; Rodríguez, P.P.; et al. Pregnancy Outcomes and SARS-CoV-2 Infection: The Spanish Obstetric Emergency Group Study. Viruses 2021, 13, 853. [Google Scholar] [CrossRef]
- Celewicz, A.; Celewicz, M.; Michalczyk, M.; Woźniakowska-Gondek, P.; Krejczy, K.; Misiek, M.; Rzepka, R. Pregnancy as a Risk Factor of Severe COVID-19. J. Clin. Med. 2021, 10, 5458. [Google Scholar] [CrossRef]
- Sinopoli, A.; Isonne, C.; Santoro, M.M.; Baccolini, V. The effects of orally administered lactoferrin in the prevention and management of viral infections: A systematic review. Rev. Med. Virol. 2022, 32, e2261. [Google Scholar] [CrossRef]
- Junaid, K.; Ejaz, H.; Abdalla, A.E.; Abosalif, K.O.A.; Ullah, M.I.; Yasmeen, H.; Younas, S.; Hamam, S.S.M.; Rehman, A. Effective Immune Functions of Micronutrients against SARS-CoV-2. Nutrients 2020, 12, 2992. [Google Scholar] [CrossRef]
- Dobrescu, A.; Copaescu, C.; Zmeu, B.; Duta, C.; Bedreag, O.H.; Stoica, L.; Tarta, C.; Rogobete, A.F.; Lazar, F. Ghrelin levels and hunger sensation after laparoscopic sleeve gastrectomy compared with laparoscopic greater curvature plication in obese patients. Clin. Lab. 2020, 66, 847–853. [Google Scholar] [CrossRef]
- Iddir, M.; Brito, A.; Dingeo, G.; Fernandez Del Campo, S.S.; Samouda, H.; La Frano, M.R.; Bohn, T. Strengthening the Immune System and Reducing Inflammation and Oxidative Stress through Diet and Nutrition: Considerations during the COVID-19 Crisis. Nutrients 2020, 12, 1562. [Google Scholar] [CrossRef]
- Marcos, A. Editorial: A Review of Micronutrients and the Immune System—Working in Harmony to Reduce the Risk of Infection. Nutrients 2021, 13, 4180. [Google Scholar] [CrossRef]
- Wessels, I.; Maywald, M.; Rink, L. Zinc as a Gatekeeper of Immune Function. Nutrients 2017, 9, 1286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yalcin Bahat, P.; Aldikactioglu Talmac, M.; Bestel, A.; Topbas Selcuki, N.F.; Aydın, Z.; Polat, İ. Micronutrients in COVID-19 Positive Pregnancies. Cureus 2020, 12, e10609. [Google Scholar] [CrossRef] [PubMed]
- Schwalfenberg, G.K.; Genuis, S.J. The Importance of Magnesium in Clinical Healthcare. Scientifica 2017, 2017, 4179326. [Google Scholar] [CrossRef]
- Stewart, T.; Lambourne, J.; Thorp-Jones, D.; Thomas, D.W. Implementation of early management of iron deficiency in pregnancy during the SARS-CoV-2 pandemic. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 258, 60–62. [Google Scholar] [CrossRef] [PubMed]
- Uta, M.; Neamtu, R.; Bernad, E.; Mocanu, A.G.; Gluhovschi, A.; Popescu, A.; Dahma, G.; Dumitru, C.; Stelea, L.; Citu, C.; et al. The Influence of Nutritional Supplementation for Iron Deficiency Anemia on Pregnancies Associated with SARS-CoV-2 Infection. Nutrients 2022, 14, 836. [Google Scholar] [CrossRef]
- Toprak, O.; Kurt, H.; Sarı, Y.; Şarkış, C.; Us, H.; Kırık, A. Magnesium Replacement Improves the Metabolic Profile in Obese and Pre-Diabetic Patients with Mild-to-Moderate Chronic Kidney Disease: A 3-Month, Randomised, Double-Blind, Placebo-Controlled Study. Kidney Blood Press. Res. 2017, 42, 33–42. [Google Scholar] [CrossRef]
- Trapani, V.; Rosanoff, A.; Baniasadi, S.; Barbagallo, M.; Castiglioni, S.; Guerrero-Romero, F.; Iotti, S.; Mazur, A.; Micke, O.; Pourdowlat, G.; et al. The relevance of magnesium homeostasis in COVID-19. Eur. J. Nutr. 2021, 61, 625–636. [Google Scholar] [CrossRef]
- Kawano, Y.; Matsuoka, H.; Takishita, S.; Omae, T. Effects of Magnesium Supplementation in Hypertensive Patients. Hypertension 1998, 32, 260–265. [Google Scholar] [CrossRef] [Green Version]
- Chaffee, B.W.; King, J.C. Effect of zinc supplementation on pregnancy and infant outcomes: A systematic review. Paediatr. Perinat. Epidemiol. 2012, 26 (Suppl. 1), 118–137. [Google Scholar] [CrossRef] [Green Version]
- Ota, E.; Mori, R.; Middleton, P.; Tobe-Gai, R.; Mahomed, K.; Miyazaki, C.; Bhutta, Z.A. Zinc supplementation for improving pregnancy and infant outcome. Cochrane Database Syst. Rev. 2015, 2015, CD000230. [Google Scholar] [CrossRef]
- Rude, R.K. Magnesium. In Modern Nutrition in Health and Disease, 11th ed.; Ross, A.C., Caballero, B., Cousins, R.J., Tucker, K.L., Ziegler, T.R., Eds.; Lippincott Williams & Wilkins: Baltimore, MA, USA, 2012; pp. 159–175. [Google Scholar]
- Gupta, A.; Khenduja, P.; Pandey, R.M.; Sati, H.C.; Sofi, N.Y.; Kapil, U. Dietary Intake of Minerals, Vitamins, and Trace Elements Among Geriatric Population in India. Biol. Trace Element Res. 2017, 180, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Killilea, D.W.; Maier, J.A.M. A connection between magnesium deficiency and aging: New insights from cellular studies. Magnes. Res. 2008, 21, 77–82. [Google Scholar] [PubMed]
- Fanni, D.; Gerosa, C.; Nurchi, V.M.; Manchia, M.; Saba, L.; Coghe, F.; Crisponi, G.; Gibo, Y.; Van Eyken, P.; Fanos, V.; et al. The Role of Magnesium in Pregnancy and in Fetal Programming of Adult Diseases. Biol. Trace Elem. Res. 2021, 199, 3647–3657. [Google Scholar] [CrossRef] [PubMed]
- Nasser, R.; Naffaa, M.E.; Mashiach, T.; Azzam, Z.S.; Braun, E. The association between serum magnesium levels and community-acquired pneumonia 30-day mortality. BMC Infect. Dis. 2018, 18, 698. [Google Scholar] [CrossRef]
- Ghelani, D.; Alesi, S.; Mousa, A. Vitamin D and COVID-19: An Overview of Recent Evidence. Int. J. Mol. Sci. 2021, 22, 10559. [Google Scholar] [CrossRef]
- O’Driscoll, M.; Ribeiro Dos Santos, G.; Wang, L.; Cummings, D.A.T.; Azman, A.S.; Paireau, J.; Fontanet, A.; Cauchemez, S.; Salje, H. Age-specific mortality and immunity patterns of SARS-CoV-2. Nature 2020, 590, 140–145. [Google Scholar] [CrossRef]
- Acharya, D.; Lee, K.; Lee, D.S.; Lee, Y.S.; Moon, S.-S. Mortality Rate and Predictors of Mortality in Hospitalized COVID-19 Patients with Diabetes. Healthcare 2020, 8, 338. [Google Scholar] [CrossRef]
- Palaiodimos, L.; Ali, R.; Teo, H.O.; Parthasarathy, S.; Karamanis, D.; Chamorro-Pareja, N.; Kokkinidis, D.G.; Kaur, S.; Kladas, M.; Sperling, J.; et al. Obesity, Inflammation, and Mortality in COVID-19: An Observational Study from the Public Health Care System of New York City. J. Clin. Med. 2022, 11, 622. [Google Scholar] [CrossRef]
- Propper, R.E. Smell/Taste alteration in COVID-19 may reflect zinc deficiency. J. Clin. Biochem. Nutr. 2021, 68, 3. [Google Scholar] [CrossRef]
- Shittu, M.O.; Afolami, O.I. Improving the efficacy of Chloroquine and Hydroxychloroquine against SARS-CoV-2 may require Zinc additives—A better synergy for future COVID-19 clinical trials. Infez. Med. 2020, 28, 192–197. [Google Scholar] [PubMed]
- Skalny, A.V.; Rink, L.; Ajsuvakova, O.P.; Aschner, M.; Gritsenko, V.A.; Alekseenko, S.I.; Svistunov, A.A.; Petrakis, D.; Spandidos, D.A.; Aaseth, J.; et al. Zinc and respiratory tract infections: Perspectives for COVID-19 (Review). Int. J. Mol. Med. 2020, 46, 17–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.-W.; Lee, M.-C.; Lin, B.-R.; Lu, Y.-P.; Hsu, Y.-J.; Chuang, C.-Y.; Huang, T.-T.; Chen, Y.-K. The Effect of Azithromycin Plus Zinc Sulfate on ACE2 Expression through IκBα of Human Respiratory Cells in SARS-CoV-2: In Vitro Study. COVID 2021, 1, 263–275. [Google Scholar] [CrossRef]
- Nawsherwan, N.; Khan, S.; Zeb, F.; Shoaib, M.; Nabi, G.; Haq, I.U.; Xu, K.; Li, H. Selected Micronutrients: An Option to Boost Immunity against COVID-19 and Prevent Adverse Pregnancy Outcomes in Pregnant Women: A Narrative Review. Iran. J. Public Health 2020, 49, 2032–2043. [Google Scholar] [CrossRef] [PubMed]
- Erol, S.A.; Polat, N.; Akdas, S.; Ayral, P.A.; Anuk, A.T.; Tokalioglu, E.O.; Ayhan, G.; Kesikli, B.; Ceylan, M.N.; Tanacan, A.; et al. Maternal selenium status plays a crucial role on clinical outcomes of pregnant women with COVID-19 infection. J. Med. Virol. 2021, 93, 5438–5445. [Google Scholar] [CrossRef] [PubMed]
- Alejo, J.L.; Mitchell, J.; Chang, A.; Chiang, T.P.Y.; Massie, A.B.; Segev, D.L.; Makary, M.A. Prevalence and Durability of SARS-CoV-2 Antibodies Among Unvaccinated US Adults by History of COVID-19. JAMA 2022, 327, 1085–1087. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables * | No Supplementation (n = 313) | Mg Supplementation (n = 61) | Ca+Mg+Zn Supplementation (n = 74) | p-Value |
|---|---|---|---|---|
| Age | 0.298 | |||
| <25 | 34 (10.9%) | 9 (14.8%) | 13 (17.6%) | |
| 25–34 | 221 (70.6%) | 40 (65.6%) | 43 (58.1%) | |
| >34 | 58 (18.5%) | 12 (19.7%) | 18 (24.3%) | |
| Gravidity | <0.001 | |||
| 1 | 129 (41.2%) | 38 (62.3%) | 46 (62.2%) | |
| 2 | 94 (30.0%) | 14 (23.0%) | 22 (29.7%) | |
| ≥3 | 90 (28.8%) | 9 (14.8%) | 6 (8.1%) | |
| Parity | <0.001 | |||
| 1 | 137 (43.8%) | 41 (67.2%) | 49 (66.2%) | |
| 2 | 102 (32.6%) | 16 (26.2%) | 20 (27.0%) | |
| ≥3 | 74 (23.6%) | 4 (6.6%) | 5 (6.8%) | |
| Area of residence | 0.006 | |||
| Urban | 139 (44.4%) | 38 (62.3%) | 44 (59.5%) | |
| Rural | 174 (55.6%) | 23 (37.7%) | 30 (40.5%) | |
| Occupation | 0.028 | |||
| No occupation | 62 (19.8%) | 8 (13.1%) | 11 (14.9%) | |
| Student | 54 (17.3%) | 17 (27.9%) | 24 (32.4%) | |
| Employed | 197 (62.9%) | 36 (59.0%) | 39 (52.7%) | |
| Level of education | 0.156 | |||
| Elementary | 38 (12.1%) | 4 (6.6%) | 7 (9.5%) | |
| Middle | 106 (33.9%) | 15 (24.6%) | 19 (25.7%) | |
| Higher | 169 (54.0%) | 42 (68.9%) | 48 (64.9%) | |
| Level of income | 0.042 | |||
| Low | 63 (20.1%) | 9 (14.8%) | 10 (13.5%) | |
| Medium | 195 (62.3%) | 34 (55.7%) | 41 (55.4%) | |
| High | 55 (17.6%) | 18 (29.5%) | 23 (31.1%) | |
| Civil status | 0.923 | |||
| Married | 283 (90.4%) | 57 (93.4%) | 66 (89.2%) | |
| Single | 12 (3.8%) | 2 (3.3%) | 3 (4.1%) | |
| Divorced/Widowed | 18 (5.8%) | 2 (3.3%) | 5 (6.8%) |
| Variables * | Mg Supplementation (n = 61) | Ca+Mg+Zn Supplementation (n = 74) | p-Value |
|---|---|---|---|
| Reason for supplementation | 0.594 | ||
| Self-medicated | 39 (63.9%) | 44 (59.5%) | |
| By recommendation | 22 (36.1%) | 30 (40.5%) | |
| Duration of supplementation | 0.266 | ||
| <9 months | 48 (78.7%) | 52 (70.3%) | |
| ≥9 months | 13 (21.3%) | 22 (29.7%) | |
| Other supplements used | |||
| Folate | 24 (39.3%) | 39 (52.7%) | 0.121 |
| Iron | 41 (67.2%) | 52 (70.3%) | 0.702 |
| Vitamin D | 18 (29.5%) | 24 (32.4%) | 0.714 |
| Probiotics | 14 (23.0%) | 21 (28.4%) | 0.473 |
| Consistency of intake | 0.852 | ||
| Daily | 39 (63.9%) | 45 (60.8%) | |
| At least 5 times a week | 18 (29.5%) | 25 (33.8%) | |
| Less than 5 times a week | 4 (6.6%) | 4 (5.4%) | |
| Form of magnesium | 0.967 | ||
| Mg(OH)2 | 6 (9.8%) | 6 (8.5%) | |
| MgO | 13 (21.3%) | 16 (22.5%) | |
| MgCl2 | 7 (11.5%) | 5 (7.0%) | |
| Lactate | 6 (9.8%) | 8 (11.3%) | |
| Citrate | 21 (34.4%) | 26 (36.6%) | |
| Aspartate | 8 (13.1%) | 10 (14.1%) | |
| Magnesium dose | 0.774 | ||
| <450 mg | 20 (32.8%) | 26 (35.1%) | |
| ≥450 mg | 41 (67.2%) | 48 (64.9%) |
| Variables * | No Supplementation (n = 313) | Magnesium Supplementation (n = 61) | Ca+Mg+Zn Supplementation (n = 74) | p-Value |
|---|---|---|---|---|
| Comorbidities | ||||
| Obesity, (BMI ≥ 30 kg/m2) | 65 (20.8%) | 11 (18.0%) | 14 (18.9%) | 0.859 |
| High blood pressure | 28 (8.9%) | 5 (8.2%) | 7 (9.5%) | 0.967 |
| Thromboembolic events | 7 (2.2%) | 0 (0.0%) | 1 (1.4%) | 0.460 |
| Others ** | 16 (5.1%) | 4 (6.6%) | 4 (5.4%) | 0.899 |
| COVID-19 severity | 0.868 | |||
| Mild | 229 (73.2%) | 47 (77.0%) | 53 (71.6%) | |
| Moderate | 70 (22.4%) | 12 (19.7%) | 19 (25.7%) | |
| Severe | 14 (4.5%) | 2 (3.3%) | 2 (2.7%) | |
| COVID-19 symptoms | ||||
| Fever | 246 (78.6%) | 45 (73.8%) | 53 (71.6%) | 0.369 |
| Anosmia/Ageusia | 179 (57.2%) | 27 (44.3%) | 31 (41.9%) | 0.020 |
| Cough | 215 (68.7%) | 39 (63.9%) | 42 (56.8%) | 0.139 |
| Fatigue | 272 (86.9%) | 46 (75.4%) | 54 (73.0%) | 0.003 |
| Dyspnea | 124 (39.6%) | 22 (36.1%) | 25 (33.8%) | 0.607 |
| Digestive symptoms | 88 (28.1%) | 11 (18.0%) | 12 (16.2%) | 0.043 |
| Others | 71 (22.7%) | 11 (18.0%) | 14 (18.9%) | 0.610 |
| Maternal complications | ||||
| Anemia | 98 (31.3%) | 17 (27.9%) | 19 (25.7%) | 0.592 |
| Gestational diabetes mellitus | 27 (8.6%) | 3 (4.9%) | 5 (6.8%) | 0.573 |
| Gestational hypertension | 25 (8.0%) | 2 (3.3%) | 2 (2.7%) | 0.138 |
| Oligohydramnios | 17 (5.4%) | 1 (1.6%) | 3 (4.1%) | 0.422 |
| Polyhydramnios | 15 (4.8%) | 2 (3.3%) | 1 (1.4%) | 0.379 |
| Abnormal presentation | 33 (10.5%) | 4 (6.6%) | 5 (6.8%) | 0.433 |
| PROM | 34 (10.9%) | 2 (3.3%) | 3 (4.1%) | 0.047 |
| Cesarean delivery | 76 (24.3%) | 12 (19.7%) | 15 (20.3%) | 0.611 |
| Neonatal complications | ||||
| Anemia | 62 (19.8%) | 9 (14.8%) | 12 (16.2%) | 0.555 |
| Puerperal infection | 21 (6.7%) | 2 (3.3%) | 2 (2.7%) | 0.281 |
| Premature birth | 45 (14.4%) | 4 (6.6%) | 4 (5.4%) | 0.038 |
| Malformations | 3 (1.0%) | 0 (0.0%) | 1 (1.4%) | 0.690 |
| NRDS | 16 (5.1%) | 2 (3.3%) | 2 (2.7%) | 0.592 |
| Birth weight | 0.037 | |||
| <1500 g | 13 (4.2%) | 1 (1.6%) | 1 (1.4%) | |
| 1500–2500 g | 41 (13.1%) | 3 (4.9%) | 3 (4.1%) | |
| >2500 g | 259 (82.7%) | 57 (93.4%) | 70 (94.6%) | |
| APGAR score | 0.033 | |||
| ≥9 | 238 (76.0%) | 54 (88.5%) | 66 (89.2%) | |
| 7–8 | 57 (18.2%) | 4 (6.6%) | 6 (8.1%) | |
| ≤6 | 18 (5.8%) | 3 (4.9%) | 2 (2.7%) | |
| Days since COVID-19 diagnosis | 0.898 | |||
| <90 days | 131 (41.9%) | 24 (39.3%) | 42 (43.2%) | |
| ≥90 days | 182 (58.1%) | 37 (60.7%) | 42 (56.8%) | |
| SARS-CoV-2 anti-RBD (U/mL) | 0.044 | |||
| <500 | 197 (62.9%) | 30 (49.2%) | 38 (51.4%) | |
| ≥500 | 116 (37.1%) | 31 (50.8%) | 36 (48.6%) |
| No Supplementation (OR–95% CI) | p-Value | Magnesium Supplementation (OR–95% CI) | p-Value | |
|---|---|---|---|---|
| Age | ||||
| <25 ^ | 0.91 (0.72–1.10) | 0.572 | 0.84 (0.60–1.13) | 0.662 |
| 25–34 | 0.99 (0.76–1.24) | 0.384 | 0.92 (0.84–1.27) | 0.513 |
| >34 | 1.12 (1.01–1.38) | 0.047 | 1.04 (0.82–1.21) | 0.296 |
| Obesity | ||||
| No ^ | 0.94 (0.63–1.48) | 0.316 | 0.88 (0.36–1.44) | 0.581 |
| Yes | 1.56 (1.28–2.34) | 0.011 | 1.42 (1.05–1.93) | 0.040 |
| Duration of supplementation | ||||
| <9 months | 1.18 (0.78–1.69) | 0.427 | 1.04 (0.75–1.28) | 0.338 |
| ≥9 months ^ | 1.01 (0.83–1.26) | 0.290 | 0.92 (0.81–1.05) | 0.194 |
| Vitamin D supplementation | ||||
| No | 1.17 (0.91–1.32) | 0.522 | 1.01 (0.88–1.39) | 0.194 |
| Yes ^ | 0.85 (0.36–1.16) | 0.314 | 0.76 (0.62–0.92) | 0.086 |
| COVID-19 severity | ||||
| Mild ^ | 1.33 (1.02–0.78) | 0.071 | 1.24 (1.09–1.76) | 0.142 |
| Moderate | 1.13 (0.93–1.42) | 0.461 | 1.05 (0.83–1.41) | 0.510 |
| Severe | 0.86 (0.72–0.98) | 0.283 | 0.82 (0.69–1.05) | 0.308 |
| Days since COVID-19 clearance | ||||
| <90 days ^ | 1.10 (0.99–0.48) | 0.308 | 0.99 (0.72–0.98) | 0.416 |
| ≥90 days | 1.62 (1.24–2.15) | 0.001 | 1.27 (1.04–1.82) | 0.008 |
| Magnesium dose | ||||
| <450 mg ^ | - | - | 1.25 (1.08–1.66) | 0.003 |
| ≥450 mg | - | - | 0.98 (0.63–1.17) | 0.372 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Citu, I.M.; Citu, C.; Margan, M.-M.; Craina, M.; Neamtu, R.; Gorun, O.M.; Burlea, B.; Bratosin, F.; Rosca, O.; Grigoras, M.L.; et al. Calcium, Magnesium, and Zinc Supplementation during Pregnancy: The Additive Value of Micronutrients on Maternal Immune Response after SARS-CoV-2 Infection. Nutrients 2022, 14, 1445. https://doi.org/10.3390/nu14071445
Citu IM, Citu C, Margan M-M, Craina M, Neamtu R, Gorun OM, Burlea B, Bratosin F, Rosca O, Grigoras ML, et al. Calcium, Magnesium, and Zinc Supplementation during Pregnancy: The Additive Value of Micronutrients on Maternal Immune Response after SARS-CoV-2 Infection. Nutrients. 2022; 14(7):1445. https://doi.org/10.3390/nu14071445
Chicago/Turabian StyleCitu, Ioana Mihaela, Cosmin Citu, Madalin-Marius Margan, Marius Craina, Radu Neamtu, Oana Maria Gorun, Bogdan Burlea, Felix Bratosin, Ovidiu Rosca, Mirela Loredana Grigoras, and et al. 2022. "Calcium, Magnesium, and Zinc Supplementation during Pregnancy: The Additive Value of Micronutrients on Maternal Immune Response after SARS-CoV-2 Infection" Nutrients 14, no. 7: 1445. https://doi.org/10.3390/nu14071445
APA StyleCitu, I. M., Citu, C., Margan, M.-M., Craina, M., Neamtu, R., Gorun, O. M., Burlea, B., Bratosin, F., Rosca, O., Grigoras, M. L., Motoc, A., Malita, D., Neagoe, O., & Gorun, F. (2022). Calcium, Magnesium, and Zinc Supplementation during Pregnancy: The Additive Value of Micronutrients on Maternal Immune Response after SARS-CoV-2 Infection. Nutrients, 14(7), 1445. https://doi.org/10.3390/nu14071445