
The Impact on the Clinical Prognosis of Low Serum Selenium Level in Patients with Severe Trauma: Systematic Review and Meta-Analysis

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.2.1. Population
2.2.2. Intervention and Comparison
2.2.3. Outcome Measures
2.2.4. Studies
2.3. Information Sources and Search
2.4. Study Selection
2.5. Data Collection Process and Quality Assessment
2.6. Data Synthesis
3. Results
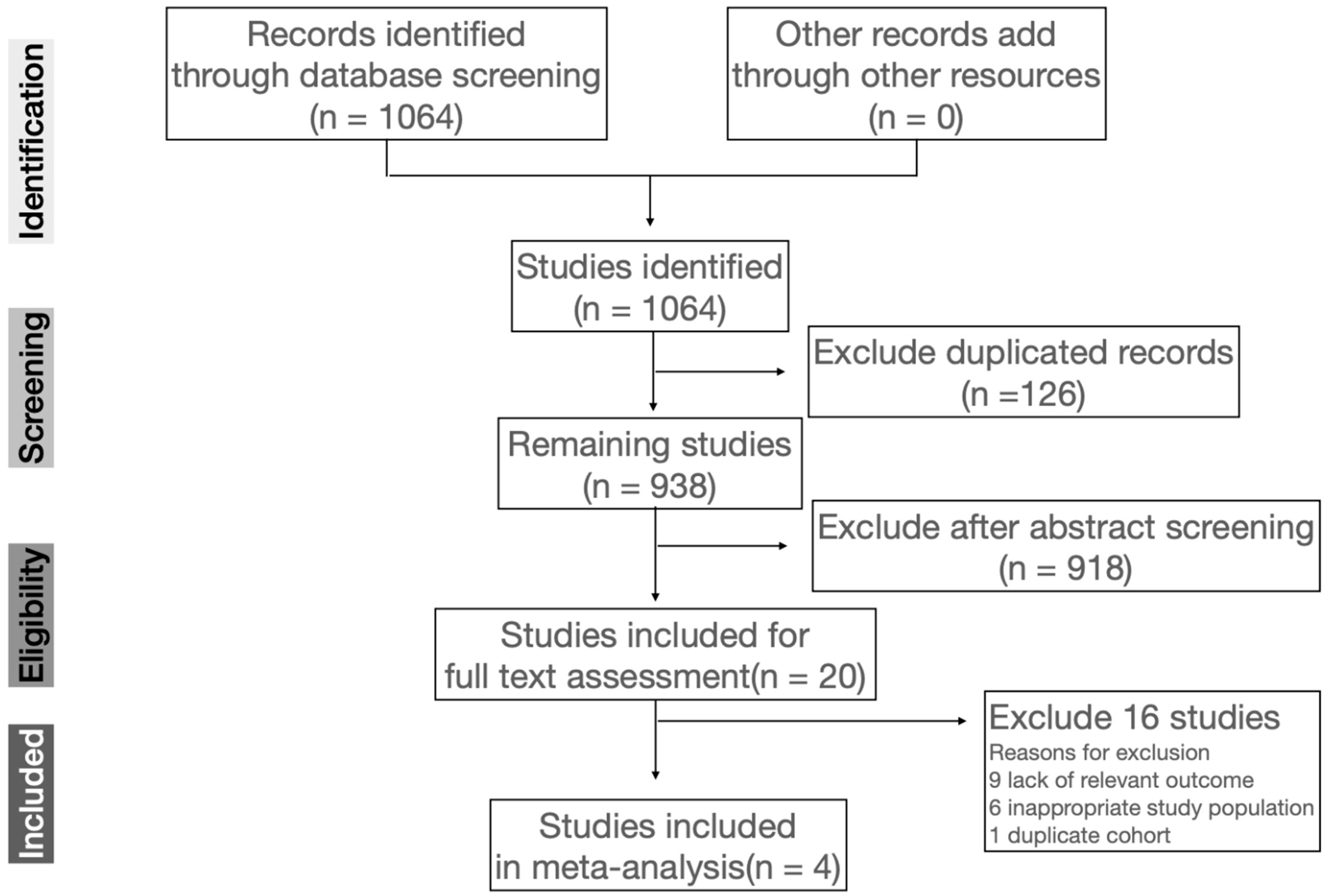
3.1. Study Selection
3.2. Study Characteristics
3.3. Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Labunskyy, V.M.; Hatfield, D.L.; Gladyshev, V.N. Selenoproteins: Molecular pathways and physiological roles. Physiol. Rev. 2014, 94, 739–777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avery, J.C.; Hoffmann, P.R. Selenium, Selenoproteins, and Immunity. Nutrients 2018, 10, 1203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kryukov, G.V.; Castellano, S.; Novoselov, S.V.; Lobanov, A.V.; Zehtab, O.; Guigo, R.; Gladyshev, V.N. Characterization of mammalian selenoproteomes. Science 2003, 300, 1439–1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, M.M.; Reymond, M.J.; Shenkin, A.; Rey, F.; Wardle, C.; Cayeux, C.; Schindler, C.; Chioléro, R.L. Influence of Selenium Supplements on the Post-Traumatic Alterations of the Thyroid Axis: A Placebo-Controlled Trial. Intensive Care Med. 2001, 27, 91–100. [Google Scholar] [CrossRef]
- Jang, J.Y.; Shim, H.; Lee, S.H.; Lee, J.G. Serum Selenium and Zinc Levels in Critically Ill Surgical Patients. J. Crit. Care 2014, 29, 317.e5–317.e8. [Google Scholar] [CrossRef]
- Angstwurm, M.W.A.; Engelmann, L.; Zimmermann, T.; Lehmann, C.; Spes, C.H.; Abel, P.; Strauss, R.; Meier-Hellmann, A.; Insel, R.; Radke, J.; et al. Selenium in Intensive Care (SIC): Results of a Prospective Randomized, Placebo-Controlled, Multiple-Center Study in Patients with Severe Systemic Inflammatory Response Syndrome, Sepsis, and Septic Shock. Crit. Care Med. 2007, 35, 118–126. [Google Scholar] [CrossRef]
- Gärtner, R.; Gasnier, B.C.H.; Dietrich, J.W.; Krebs, B.; Angstwurm, M.W.A. Selenium Supplementation in Patients with Autoimmune Thyroiditis Decreases Thyroid Peroxidase Antibodies Concentrations. J. Clin. Endocrinol. Metab. 2002, 87, 1687–1691. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.; Rose, A.H.; Hoffmann, P.R. The Role of Selenium in Inflammation and Immunity: From Molecular Mechanisms to Therapeutic Opportunities. Antioxid. Redox Signal. 2012, 16, 705–743. [Google Scholar] [CrossRef] [Green Version]
- Hollenbach, B.; Morgenthaler, N.G.; Struck, J.; Alonso, C.; Bergmann, A.; Köhrle, J.; Schomburg, L. New Assay for the Measurement of Selenoprotein P as a Sepsis Biomarker from Serum. J. Trace Elem. Med. Biol. 2008, 22, 24–32. [Google Scholar] [CrossRef]
- Demetriades, D.; Kimbrell, B.; Salim, A.; Velmahos, G.; Rhee, P.; Preston, C.; Gruzinski, G.; Chan, L. Trauma Deaths in a Mature Urban Trauma System: Is “Trimodal” Distribution a Valid Concept? J. Am. Coll. Surg. 2005, 201, 343–348. [Google Scholar] [CrossRef]
- Sobrino, J.; Shafi, S. Timing and Causes of Death after Injuries. Bayl. Univ. Med. Cent. Proc. 2013, 26, 120–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunst, M.; Ghaemmaghami, V.; Gruszecki, A.; Urban, J.; Frankel, H.; Shafi, S. Changing Epidemiology of Trauma Deaths Leads to a Bimodal Distribution. Bayl. Univ. Med. Cent. Proc. 2010, 23, 349–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciesla, D.J.; Moore, E.E.; Johnson, J.L.; Burch, J.M.; Cothren, C.C.; Sauaia, A. A 12-Year Prospective Study of Postinjury Multiple Organ Failure: Has Anything Changed? Arch. Surg. 2005, 140, 432–438; discussion 438–440. [Google Scholar] [CrossRef] [PubMed]
- Lefering, R.; Paffrath, T.; Bouamra, O.; Coats, T.J.; Woodford, M.; Jenks, T.; Wafaisade, A.; Nienaber, U.; Lecky, F. Epidemiology of in-Hospital Trauma Deaths. Eur. J. Trauma Emerg. Surg. 2012, 38, 3–9. [Google Scholar] [CrossRef]
- Guisasola, M.C.; Alonso, B.; Bravo, B.; Vaquero, J.; Chana, F. An Overview of Cytokines and Heat Shock Response in Polytraumatized Patients. Cell Stress Chaperones 2018, 23, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Braunstein, M.; Kusmenkov, T.; Zuck, C.; Angstwurm, M.; Becker, N.-P.; Böcker, W.; Schomburg, L.; Bogner-Flatz, V. Selenium and Selenoprotein P Deficiency Correlates with Complications and Adverse Outcome After Major Trauma. Shock 2020, 53, 63–70. [Google Scholar] [CrossRef]
- Klein, G.L.; Rodriguez, N.A.; Branski, L.K.; Herndon, D.N. Vitamin and Trace Element Homeostasis Following Severe Burn Injury. In Total Burn Care; WB Saunders: London, UK, 2012; pp. 321–324. [Google Scholar]
- Kurmis, R.; Greenwood, J.; Aromataris, E. Trace Element Supplementation Following Severe Burn Injury: A Systematic Review and Meta-Analysis. J. Burn Care Res. 2016, 37, 143–159. [Google Scholar] [CrossRef]
- Berger, M.M.; Cavadini, C.; Chiolero, R.; Dirren, H. Copper, Selenium, and Zinc Status and Balances after Major Trauma. J. Trauma 1996, 40, 103–109. [Google Scholar] [CrossRef]
- Mertens, K.; Lowes, D.A.; Webster, N.R.; Talib, J.; Hall, L.; Davies, M.J.; Beattie, J.H.; Galley, H.F. Low Zinc and Selenium Concentrations in Sepsis Are Associated with Oxidative Damage and Inflammation. Br. J. Anaesth. 2015, 114, 990–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, S.B.; Jung, Y.T.; Lee, J.G. Association of Initial Low Serum Selenium Level with Infectious Complications and 30-Day Mortality in Multiple Trauma Patients. Nutrients 2019, 11, 1844. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.; Shea, B.; Robertson, J.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analysis. Available online: https://scholar.archive.org/work/zuw33wskgzf4bceqgi7opslsre/access/wayback/http://www3.med.unipmn.it/dispense_ebm/2009-2010/Corso%20Perfezionamento%20EBM_Faggiano/NOS_oxford.pdf (accessed on 7 February 2022).
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019; ISBN 9781119536611. [Google Scholar]
- Berger, M.M.; Soguel, L.; Shenkin, A.; Revelly, J.-P.; Pinget, C.; Baines, M.; Chioléro, R.L. Influence of Early Antioxidant Supplements on Clinical Evolution and Organ Function in Critically Ill Cardiac Surgery, Major Trauma, and Subarachnoid Hemorrhage Patients. Crit. Care 2008, 12, R101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Zanten, A.R.H.; Sztark, F.; Kaisers, U.X.; Zielmann, S.; Felbinger, T.W.; Sablotzki, A.R.; De Waele, J.J.; Timsit, J.-F.; Honing, M.L.H.; Keh, D.; et al. High-Protein Enteral Nutrition Enriched with Immune-Modulating Nutrients vs Standard High-Protein Enteral Nutrition and Nosocomial Infections in the ICU: A Randomized Clinical Trial. JAMA 2014, 312, 514–524. [Google Scholar] [CrossRef] [PubMed]
- Bentzer, P.; Fjell, C.; Walley, K.R.; Boyd, J.; Russell, J.A. Plasma Cytokine Levels Predict Response to Corticosteroids in Septic Shock. Intensive Care Med. 2016, 42, 1970–1979. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.-F.; Hsu, C.-P.; Ouyang, C.-H.; Cheng, C.-T.; Wang, C.-C.; Liao, C.-H.; Wu, Y.-T.; Hsieh, C.-H. The Impact of Selenium Supplementation on Trauma Patients—Systematic Review and Meta-Analysis. Nutrients 2022, 14, 342. [Google Scholar] [CrossRef] [PubMed]
- Heyland, D.K. Selenium Supplementation in Critically Ill Patients: Can Too Much of a Good Thing Be a Bad Thing? Crit. Care 2007, 11, 153. [Google Scholar] [CrossRef] [Green Version]
- Collier, B.R.; Giladi, A.; Dossett, L.A.; Dyer, L.; Fleming, S.B.; Cotton, B.A. Impact of High-Dose Antioxidants on Outcomes in Acutely Injured Patients. JPEN J. Parenter. Enteral Nutr. 2008, 32, 384–388. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Terms | Filters/Limits |
|---|---|---|
| Pubmed | (trace element OR selenium) AND (trauma OR injury) | Clinical Trial, Randomized Controlled Trial, Humans, English, from 1990–2021 |
| Embase | (trace: ti, ab AND element: ti, ab OR selenium: ti, ab) AND (trauma: ti, ab OR injury: ti, ab) | [humans]/lim AND [english]/lim AND [clinical study]/lim AND [1990–2021]/py |
| Web of Science | ((TS = (trace element OR selenium)) OR (TI = (trace element OR selenium))) AND ((TS = (trauma OR injury)) OR TI = (trauma OR injury)) NOT ALL = (in vitro OR rabbit OR rat OR animal OR mice OR mouse OR pig OR porcine OR sheep OR lamb) AND (DT = (“ARTICLE” OR “MEETING ABSTRACT” OR “PROCEEDINGS PAPER” OR “EDITORIAL MATERIAL” OR “EARLY ACCESS”)) | From 1990–2021 |
| Study | Methods | Participants, Setting | Intervention | Outcome Measures | Newcastle Ottawa Scale |
|---|---|---|---|---|---|
| Berger et al. (2001) [4] | Study design: prospective RCT, DB Duration of follow-up: 20 days | Participants: Total n = 32 Intervention n = 20; placebo n = 12 23 males and 9 females Mean age: 42.43 ± 16.55 years Setting: SICU, Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland Inclusion criteria: Age 18–70; multiple injuries with ISS > 15; admission within first 24 h of injury | Intervention: 500 μg Se alone per day, or Se and 150 mg alpha-tocopherol, 2.6 mg Cu and 13 mg Zn per day Control: placebo | Mortality Incidence of complications and organ failure Hospital stays | 8/9 |
| Berger et al. (2008) [24] | Study design: prospective RCT, DB Duration of follow-up: 3 months after discharge | Participants: Total n = 66 Intervention n = 34; placebo n = 32 52 males and 14 females Mean age: 40 ± 19 years Setting: SICU, Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland Inclusion criteria: ISS > 9 | Intervention: selenium 270 μg IV, zinc 30 mg IV, vitamin C 1.1 g IV, vitamin B1 100 mg IV, vitamin E 6.4 mg IV and 300 mg PO with a double-loading dose on days 1 and 2, total for 5 days plus ICU standard vitamin profile as control group Control: ICU standard vitamin profile: 500 mg vitamin C/day for 5 days and 100 mg vitamin B1/day for 3 days | Mortality Hospital stays Kidney function Subsequent organ failure Infections and pneumonia | 8/9 |
| van Zanten et al. (2014) [25] | Study design: prospective RCT, DB Duration of follow-up: Six months after start study product | Participants: Total n = 109 Intervention n = 55; control n = 54 87 males and 22 females Mean age: 43 years Setting: ICU, multi-country, multi-center Inclusion criteria: age ≥ 18 years, mechanically ventilated ICU patients | Intervention: Tube feed formula enriched in glutamine, vitamin C and E, selenium, zinc and EPA and DHA, and low in carbohydrate content Control product: Isocaloric standard tube feed with the same amount of protein. | Incidence of nosocomial infections and organ failure Duration of ventilation, ICU and hospital stay Mortality | 9/9 |
| Choi et al. (2019) [21] | Study design: retrospective case control study Duration of follow-up: Until discharge | Participants: Total n = 135 Intervention n = 36; control n = 99 99 males and 36 females Mean age: 48.5 ± 18.8 years Setting: Trauma center, Yonsei University College of Medicine, Seoul, Korea Inclusion criteria: serum selenium levels were measured within 2 days of admission | Classification by Se level Case: >70 ng/mL Control: <70 ng/mL | Infection complications, Duration of ventilation, ICU and hospital stay Mortality | 4/9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, S.-Y.; Hsu, C.-P.; Ou Yang, C.-H.; Wang, C.-C.; Wu, Y.-T.; Fu, C.-Y.; Hsieh, C.-H.; Cheng, C.-T.; Lin, W.-C.; Huang, J.-F.; et al. The Impact on the Clinical Prognosis of Low Serum Selenium Level in Patients with Severe Trauma: Systematic Review and Meta-Analysis. Nutrients 2022, 14, 1295. https://doi.org/10.3390/nu14061295
Chan S-Y, Hsu C-P, Ou Yang C-H, Wang C-C, Wu Y-T, Fu C-Y, Hsieh C-H, Cheng C-T, Lin W-C, Huang J-F, et al. The Impact on the Clinical Prognosis of Low Serum Selenium Level in Patients with Severe Trauma: Systematic Review and Meta-Analysis. Nutrients. 2022; 14(6):1295. https://doi.org/10.3390/nu14061295
Chicago/Turabian StyleChan, Shang-Yu, Chih-Po Hsu, Chun-Hsiang Ou Yang, Chia-Cheng Wang, Yu-Tung Wu, Chih-Yuan Fu, Chi-Hsun Hsieh, Chi-Tung Cheng, Wei-Cheng Lin, Jen-Fu Huang, and et al. 2022. "The Impact on the Clinical Prognosis of Low Serum Selenium Level in Patients with Severe Trauma: Systematic Review and Meta-Analysis" Nutrients 14, no. 6: 1295. https://doi.org/10.3390/nu14061295
APA StyleChan, S.-Y., Hsu, C.-P., Ou Yang, C.-H., Wang, C.-C., Wu, Y.-T., Fu, C.-Y., Hsieh, C.-H., Cheng, C.-T., Lin, W.-C., Huang, J.-F., & Liao, C.-H. (2022). The Impact on the Clinical Prognosis of Low Serum Selenium Level in Patients with Severe Trauma: Systematic Review and Meta-Analysis. Nutrients, 14(6), 1295. https://doi.org/10.3390/nu14061295