
The Relationship between Dietary Habits and Work Engagement among Female Finnish Municipal Employees

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Participants
2.2. Physical Examination
2.3. Work-Related Factors
2.4. Health Behavior and Other Measures
2.5. Psychosocial Measures
2.6. Food Frequency Questionnaire
2.7. Statistical Analyses
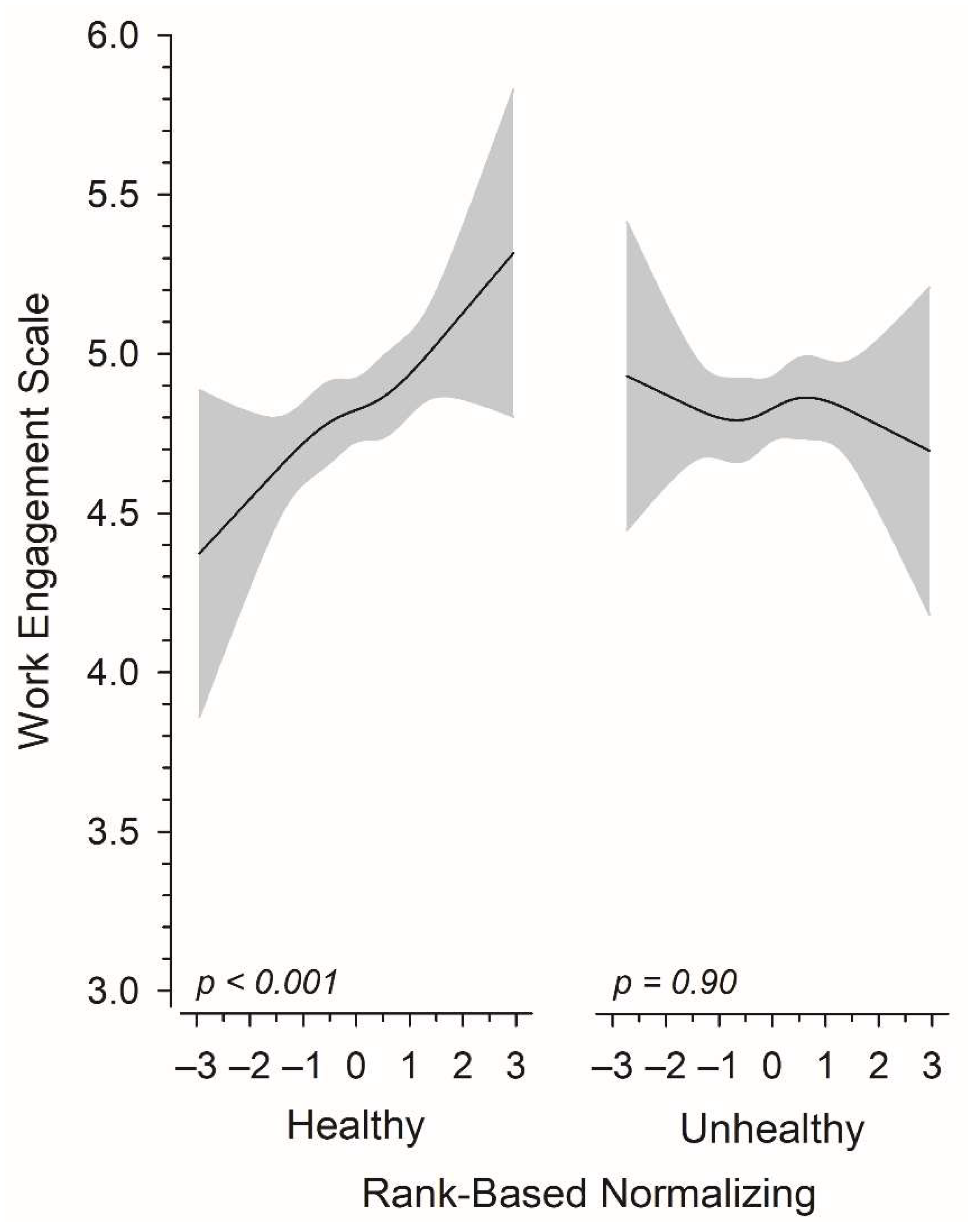
3. Results
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schaufeli, W.; Salanova, M.; González-romá, V.; Bakker, A. The Measurement of Engagement and Burnout: A Two Sample Confirmatory Factor Analytic Approach. J. Happiness Stud. 2002, 3, 71–92. [Google Scholar] [CrossRef]
- Shimazu, A.; Schaufeli, W.B.; Kamiyama, K.; Kawakami, N. Workaholism vs. Work Engagement: The Two Different Predictors of Future Well-being and Performance. Int. J. Behav. Med. 2015, 22, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Veromaa, V.; Kautiainen, H.; Korhonen, P.E. Physical and mental health factors associated with work engagement among Finnish female municipal employees: A cross-sectional study. BMJ Open 2017, 7, e017303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaufeli, W.B.; Taris, T.W.; Van Rhenen, W. Workaholism, burnout, and work engagement: Three of a kind or three different kinds of employee well-being? Appl. Psychol. 2008, 57, 173–203. [Google Scholar] [CrossRef] [Green Version]
- Imamura, K.; Kawakami, N.; Inoue, A.; Shimazu, A.; Tsutsumi, A.; Takahashi, M.; Totsuzaki, T. Work engagement as a predictor of onset of major depressive episode (MDE) among workers, independent of psychological distress: A 3-year prospective cohort study. PLoS ONE 2016, 11, e0148157. [Google Scholar]
- Hakanen, J.J.; Rouvinen, P.; Ylhäinen, I. The impact of work engagement on future occupational rankings, wages, unemployment, and disability pensions—A register-based study of a representative sample of finnish employees. Sustainability 2021, 13, 1626. [Google Scholar] [CrossRef]
- Nishi, D.; Suzuki, Y.; Nishida, J.; Mishima, K.; Yamanouchi, Y. Personal lifestyle as a resource for work engagement. J. Occup. Health 2017, 59, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Amano, H.; Fukuda, Y.; Baden, M.Y.; Kawachi, I. Is work engagement associated with healthier dietary patterns? A cross-sectional study. J. Occup. Health 2020, 62, e12149. [Google Scholar] [PubMed]
- Martín-Peláez, S.; Fito, M.; Castaner, O. Mediterranean Diet Effects on Type 2 Diabetes Prevention, Disease Progression, and Related Mechanisms. A Review. Nutrients 2020, 12, 2236. [Google Scholar] [CrossRef]
- Mentella, M.C.; Scaldaferri, F.; Ricci, C.; Gasbarrini, A.; Miggiano, G.A.D. Cancer and Mediterranean Diet: A Review. Nutrients 2019, 11, 2059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galbete, C.; Kröger, J.; Jannasch, F.; Iqbal, K.; Schwingshackl, L.; Schwedhelm, C.; Weikert, C.; Boeing, H.; Schulze, M.B. Nordic diet, Mediterranean diet, and the risk of chronic diseases: The EPIC-Potsdam study. BMC Med. 2018, 16, 99. [Google Scholar] [CrossRef]
- Lankinen, M.; Uusitupa, M.; Schwab, U. Nordic Diet and Inflammation—A Review of Observational and Intervention Studies. Nutrients 2019, 6, 1369. [Google Scholar] [CrossRef] [Green Version]
- McGrattan, A.M.; McGuinness, B.; McKinley, M.C.; Kee, F.; Passmore, P.; Woodside, J.V.; McEvoy, C.T. Diet and Inflammation in Cognitive Ageing and Alzheimer’s Disease. Curr. Nutr. Rep. 2019, 8, 53–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, A.; Tovar, J.; Johansson, M.; Radeborg, K.; Björck, I. A diet based on multiple functional concepts improves cognitive performance in healthy subjects. Nutr. Metab. 2013, 10, 49. [Google Scholar] [CrossRef] [Green Version]
- Tolkien, K.; Bradburn, S.; Murgatroyd, C. An anti-inflammatory diet as a potential intervention for depressive disorders: A systematic review and meta-analysis. Clin. Nutr. 2019, 38, 2045–2052. [Google Scholar] [CrossRef] [Green Version]
- Penttinen, M.A.; Virtanen, J.; Laaksonen, M.; Erkkola, M.; Vepsäläinen, H.; Kautiainen, H.; Korhonen, P. The association between healthy diet and burnout symptoms among finnish municipal employees. Nutrients 2021, 13, 2393. [Google Scholar] [CrossRef]
- Hakanen, J. Työn Imun. Available online: https://www.wilmarschaufeli.nl/publications/Schaufeli/Test Manuals/Test_manual_UWES_Finnish.pdf (accessed on 1 March 2022).
- Schaufeli, W.B. The measurement of work engagement. Res. Methods Occup. Health Psychol. Meas. Des. Data Anal. 2012, 66, 138–154. [Google Scholar]
- Schaufeli, W.B.; Bakker, A.B. Utrecht Work Engagement Scale Preliminary Manual Version 1.1. Available online: https://www.wilmarschaufeli.nl/publications/Schaufeli/Test%20Manuals/Test_manual_UWES_English.pdf (accessed on 1 March 2022).
- Bush, K.; Kivlahan, D.R.; McDonell, M.B.; Fihn, S.D.; Bradley, K.A. The AUDIT alcohol consumption questions (AUDIT-C): An effective brief screening test for problem drinking. Arch. Intern. Med. 1998, 158, 1789–1795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuunanen, M.; Aalto, M.; Seppä, K. Binge drinking and its detection among middle-aged men using AUDIT, AUDIT-C and AUDIT-3. Drug Alcohol. Rev. 2007, 26, 295–299. [Google Scholar] [CrossRef]
- Bech, P.; Rasmussen, N.A.; Olsen, L.R.; Noerholm, V.; Abildgaard, W. The sensitivity and specificity of the Major Depression Inventory, using the Present State Examination as the index of diagnostic validity. J. Affect. Disord. 2001, 66, 159–164. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Korkalo, L.; Vepsäläinen, H.; Ray, C.; Skaffari, E.; Lehto, R.; Hauta-Alus, H.H.; Nissinen, K.; Meinilä, J.; Roos, E.; Erkkola, M. Parents’ reports of preschoolers’ diets: Relative validity of a food frequency questionnaire and dietary patterns. Nutrients 2019, 11, 159. [Google Scholar] [CrossRef] [Green Version]
- Määttä, S.; Vepsäläinen, H.; Lehto, R.; Erkkola, M.; Roos, E.; Ray, C. Reproducibility of Preschool Personnel and Guardian Reports on Energy Balance-Related Behaviors and Their Correlates in Finnish Preschool Children. Children 2018, 5, 144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.J.; Keage, H.A.D.; Murphy, K.J. A Mediterranean diet supplemented with dairy foods improves mood and processing speed in an Australian sample: Results from the MedDairy randomized controlled trial. Nutr. Neurosci. 2020, 23, 646–658. [Google Scholar] [CrossRef] [PubMed]
- Sandstrom, B.; Lyhne, N.; Pedersen, J.I.; Aro, A.; Thorsdottir, I.; Becker, W. Nordic Nutrition: Recommendations 2012; Nordic Council of Ministers: Copenhagen, Denmark, 2012; Volume 40, ISBN 9789289326704. [Google Scholar]
- Frank, E.; Harrell, J. Regression Modeling Strategies: With Applications to Linear Models, Logistic and Ordinal Regression, and Survival Analysis; Springer: Berlin/Heidelberg, Germany, 2001. [Google Scholar]
- Solomon, S.R.; Sawilowsky, S.S. Impact of rank-based normalizing transformations on the accuracy of test scores. J. Mod. Appl. Stat. Methods 2009, 8, 448–462. [Google Scholar] [CrossRef]
- Miller, A.H.; Maletic, V.; Raison, C.L. Inflammation and Its Discontents: The Role of Cytokines in the Pathophysiology of Major Depression. Biol. Psychiatry 2009, 65, 732–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libby, P. Inflammation in atherosclerosis. Nature 2002, 420, 868–874. [Google Scholar] [CrossRef]
- Neale, E.P.; Batterham, M.J.; Tapsell, L.C. Consumption of a healthy dietary pattern results in significant reductions in C-reactive protein levels in adults: A meta-analysis. Nutr. Res. 2016, 36, 391–401. [Google Scholar] [CrossRef]
- Miller, A.H.; Raison, C.L. The role of inflammation in depression: From evolutionary imperative to modern treatment target. Nat. Rev. Immunol. 2016, 16, 22–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bibbò, S.; Ianiro, G.; Giorgio, V.; Scaldaferri, F.; Masucci, L.; Gasbarrini, A.; Cammarota, G. The role of diet on gut microbiota composition. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 4742–4749. [Google Scholar] [PubMed]
- Sanada, K.; Nakajima, S.; Kurokawa, S.; Barceló-Soler, A.; Ikuse, D.; Hirata, A.; Yoshizawa, A.; Tomizawa, Y.; Salas-Valero, M.; Noda, Y.; et al. Gut microbiota and major depressive disorder: A systematic review and meta-analysis. J. Affect. Disord. 2020, 266, 1–13. [Google Scholar] [CrossRef]
- Carabotti, M.; Scirocco, A.; Maselli, M.A.; Severi, C. The gut-brain axis: Interactions between enteric microbiota, central and enteric nervous systems. Ann. Gastroenterol. 2015, 28, 203–209. [Google Scholar]
- Wang, J.; Geng, L. Effects of Socioeconomic Status on Physical and Psychological Health: Lifestyle as a Mediator. Int. J. Environ. Res. Public Health 2019, 16, 281. [Google Scholar] [CrossRef] [Green Version]
- Shih, T.H.; Fan, X. Comparing response rates in e-mail and paper surveys: A meta-analysis. Educ. Res. Rev. 2009, 4, 26–40. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Healthy Food Groups | Unhealthy Food Groups |
|---|---|
| Fat free milk and sour milk, low-fat cheese (fat <20%) | Red meat, sausages, red cold meat |
| Unflavoured nuts, seeds and almonds | Juices and beverages sweetened with sugar |
| Legumes (peas, lentils, beans) | Savoury bakery products such as pies and pastries, potato chips and nachos, popcorn, salty nuts |
| Fresh vegetables | Sweet bakery products (buns, pies, cookies, cakes), chocolate, sweets |
| Fresh fruits and berries | Alcohol |
| Whole grain pasta and rice, rye bread, rye crisp bread, breakfast cereal, muesli, porridge | High-fat dairy products: full fat milk and sour milk, full-fat cheese (fat >20%), butter, butter-oil spreads (fat >80%) |
| Fish and fish dishes | |
| Margarines and oils (cooking, bread spread, salad dressing) | |
| Cooked vegetables | |
| Eggs | |
| White meat |
| Categories of Healthy Food Items Consumed per Day * | p for Linearity | ||||
|---|---|---|---|---|---|
| I n = 126 | II n = 189 | III n = 189 | IV n = 126 | ||
| Sociodemographic factors | |||||
| Age, years, mean (SD) | 48 (10) | 47 (9) | 49 (10) | 52 (9) | 0.002 |
| Education years, mean (SD) | 13.7 (2.7) | 14.1 (2.6) | 14.0 (2.8) | 14.1 (2.7) | 0.52 |
| Cohabiting, n (%) | 94 (75) | 149 (79) | 156 (83) | 106 (84) | 0.036 |
| Financial satisfaction, n (%) | 78 (62) | 135 (71) | 144 (76) | 99 (79) | 0.002 |
| Working hours, hours/week, mean (SD) | 36.0 (10.9) | 36.0 (10.0) | 36.4 (5.9) | 37.0 (9.7) | 0.33 |
| Shift work, n (%) | 38 (30) | 61 (32) | 44 (23) | 29 (23) | 0.055 |
| Health behaviors | |||||
| PA, hours per week, mean (SD) | 2.0 (3.5) | 2.5 (2.2) | 2.8 (3.2) | 2.9 (2.2) | 0.004 |
| Good quality of sleep, n (%) | 87 (69) | 157 (83) | 139 (74) | 96 (76) | 0.68 |
| Daily breakfast, n (%) | 98 (78) | 173 (92) | 176 (93) | 115 (91) | <0.001 |
| AUDIT-C, mean (SD) | 3.0 (1.6) | 2.7 (1.6) | 2.7 (1.7) | 2.7 (1.5) | 0.11 |
| Current smoking, n (%) | 19 (15) | 15 (8) | 10 (5) | 8 (7) | 0.008 |
| Clinical factors | |||||
| Major Depression Inventory, mean (SD) | 6.5 (6.3) | 4.2 (4.9) | 6.1 (6.7) | 3.7 (4.1) | 0.018 |
| General Anxiety Scale, mean (SD) | 3.4 (3.3) | 2.7 (3.2) | 3.3 (3.7) | 2.1 (2.7) | 0.028 |
| Blood pressure, mmHg, mean (SD) | |||||
| Systolic | 129 (16) | 130 (17) | 132 (18) | 133 (18) | 0.029 |
| Diastolic | 85 (9) | 84 (11) | 85 (10) | 84 (11) | 0.95 |
| Height, cm, mean (SD) | 164 (6) | 165 (6) | 166 (6) | 165 (6) | 0.089 |
| Weight, kg, mean (SD) | 72.7 (15.7) | 74.2 (15.7) | 72.7 (13.2) | 71.7 (12.2) | 0.36 |
| Body mass index, kg/m2, mean (SD) | 26.9 (5.3) | 27.2 (5.2) | 26.6 (4.6) | 26.2 (4.3) | 0.11 |
| Waist, cm, mean (SD) | 90 (14) | 90 (13) | 88 (12) | 88 (12) | 0.081 |
| Total cholesterol, mmol/L, mean (SD) | 5.40 (0.99) | 5.22 (0.85) | 5.16 (0.94) | 5.36 (0.88) | 0.58 |
| LDL cholesterol, mmol/L, mean (SD) | 3.11 (0.78) | 2.98 (0.71) | 2.89 (0.77) | 3.03 (0.69) | 0.24 |
| HDL cholesterol, mmol/L, mean (SD) | 1.76 (0.42) | 1.76 (0.43) | 1.80 (0.45) | 1.84 (0.48) | 0.11 |
| Triglycerides, mmol/L, mean (SD) | 1.20 (0.57) | 1.09 (0.57) | 1.06 (0.56) | 1.08 (0.59) | 0.12 |
| Fasting glucose, mmol/L, mean (SD) | 5.60 (0.56) | 5.45 (0.46) | 5.51 (0.64) | 5.43 (0.50) | 0.041 |
| Antihypertensive medication, n (%) | 24 (19) | 28 (15) | 39 (21) | 19 (15) | 0.84 |
| Antilipidemic medication, n (%) | 3 (2) | 5 (3) | 12 (6) | 10 (8) | 0.011 |
| Categories of Healthy Food Items Consumed per Day * | p for Linearity | ||||
|---|---|---|---|---|---|
| I n = 126 Mean (SE) | II n = 189 Mean (SE) | III n = 189 Mean (SE) | IV n = 126 Mean (SE) | ||
| Total consumption of healthy food items | 6.02 (0.11) | 9.04 (0.06) | 12.50 (0.08) | 17.96 (0.26) | <0.001 |
| Fat-free milk and sour milk, low-fat cheese (fat <20%) | 0.46 (0.05) | 0.91 (0.06) | 1.70 (0.09) | 2.73 (0.17) | <0.001 |
| Unflavored nuts, seeds and almonds | 0.15 (0.02) | 0.28 (0.03) | 0.39 (0.03) | 0.72 (0.08) | <0.001 |
| Legumes | 0.05 (0.01) | 0.15 (0.02) | 0.23 (0.03) | 0.23 (0.03) | <0.001 |
| Fresh vegetables | 0.93 (0.04) | 1.28 (0.04) | 1.63 (0.06) | 2.26 (0.09) | <0.001 |
| Fruits and berries | 1.12 (0.05) | 1.57 (0.04) | 2.10 (0.07) | 2.90 (0.12) | <0.001 |
| Whole grain products | 1.35 (0.07) | 1.93 (0.06) | 2.54 (0.08) | 3.49 (0.14) | <0.001 |
| Fish and fish dishes | 0.23 (0.01) | 0.25 (0.01) | 0.31 (0.02) | 0.41 (0.03) | <0.001 |
| Margarine and oils | 0.75 (0.06) | 1.33 (0.06) | 2.01 (0.08) | 3.12 (0.13) | <0.001 |
| Cooked vegetables | 0.48 (0.03) | 0.69 (0.03) | 0.82 (0.04) | 1.07 (0.06) | <0.001 |
| Eggs | 0.24 (0.02) | 0.29 (0.02) | 0.37 (0.03) | 0.43 (0.04) | <0.001 |
| White meat | 0.25 (0.02) | 0.34 (0.02) | 0.43 (0.03) | 0.60 (0.06) | <0.001 |
| Total consumption of unhealthy food items | 3.93 (0.20) | 3.82 (0.14) | 3.92 (0.16) | 4.28 (0.24) | 0.057 |
| Red meat, sausages, red cold meat | 1.09 (0.07) | 1.15 (0.06) | 1.33 (0.06) | 1.39 (0.09) | <0.001 |
| Juices and beverages sweetened with sugar | 0.18 (0.04) | 0.12 (0.02) | 0.09 (0.02) | 0.07 (0.02) | 0.021 |
| Savory bakery products | 0.16 (0.02) | 0.15 (0.02) | 0.16 (0.02) | 0.19 (0.02) | 0.10 |
| Sweet bakery products | 0.87 (0.06) | 0.96 (0.05) | 1.02 (0.07) | 1.15 (0.09) | 0.003 |
| Alcohol | 0.16 (0.02) | 0.14 (0.01) | 0.15 (0.02) | 0.19 (0.03) | 0.32 |
| High-fat dairy products | 1.47 (0.12) | 1.30 (0.08) | 1.17 (0.09) | 1.29 (0.13) | 0.34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Virtanen, J.; Penttinen, M.A.; Laaksonen, M.; Erkkola, M.; Vepsäläinen, H.; Kautiainen, H.; Korhonen, P. The Relationship between Dietary Habits and Work Engagement among Female Finnish Municipal Employees. Nutrients 2022, 14, 1267. https://doi.org/10.3390/nu14061267
Virtanen J, Penttinen MA, Laaksonen M, Erkkola M, Vepsäläinen H, Kautiainen H, Korhonen P. The Relationship between Dietary Habits and Work Engagement among Female Finnish Municipal Employees. Nutrients. 2022; 14(6):1267. https://doi.org/10.3390/nu14061267
Chicago/Turabian StyleVirtanen, Jenni, Markus A. Penttinen, Marika Laaksonen, Maijaliisa Erkkola, Henna Vepsäläinen, Hannu Kautiainen, and Päivi Korhonen. 2022. "The Relationship between Dietary Habits and Work Engagement among Female Finnish Municipal Employees" Nutrients 14, no. 6: 1267. https://doi.org/10.3390/nu14061267
APA StyleVirtanen, J., Penttinen, M. A., Laaksonen, M., Erkkola, M., Vepsäläinen, H., Kautiainen, H., & Korhonen, P. (2022). The Relationship between Dietary Habits and Work Engagement among Female Finnish Municipal Employees. Nutrients, 14(6), 1267. https://doi.org/10.3390/nu14061267