
Risk of Drop-Out from Follow-Up Evaluations for Celiac Disease: Is It Similar for All Patients?

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Setting
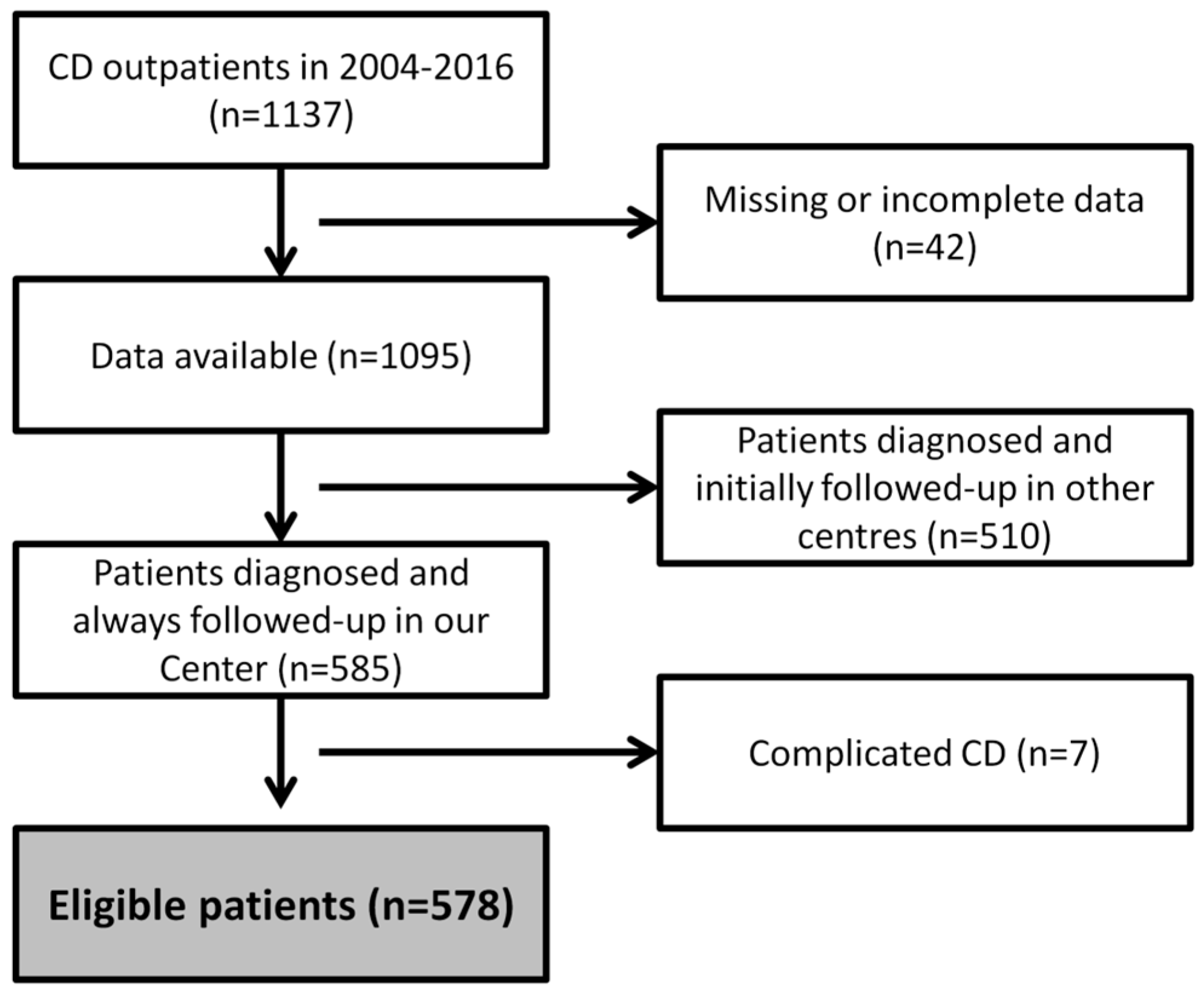
2.2. Inclusion and Exclusion Criteria
2.3. Evaluations
2.4. Compliance with the GFD
2.5. Compliance with Follow-Up Procedures and Drop-Out Definition
2.6. Ethics
2.7. Statistical Analysis
3. Results
3.1. Study Population: Baseline Characteristics
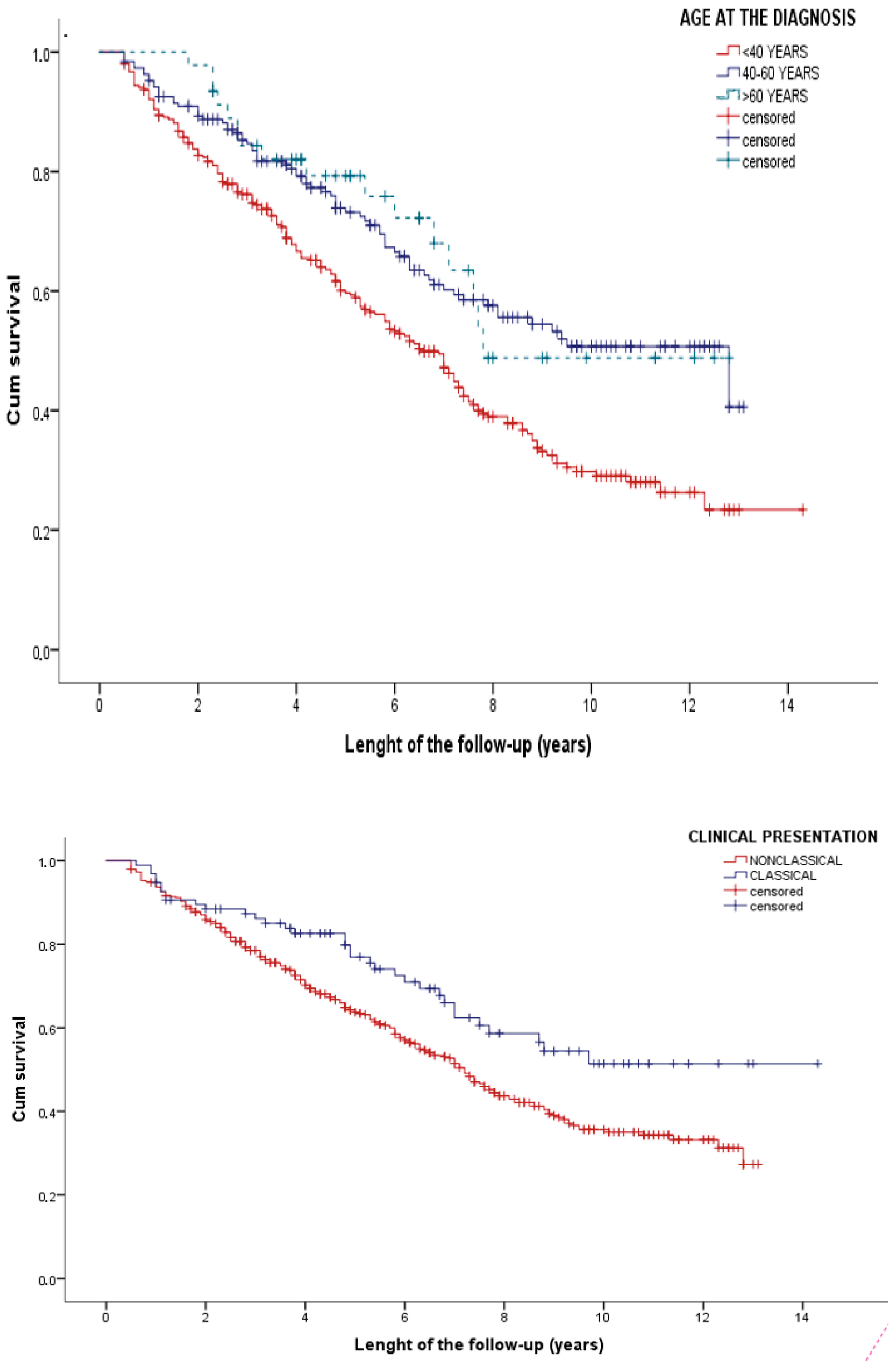
3.2. Risk of Early Drop-Out
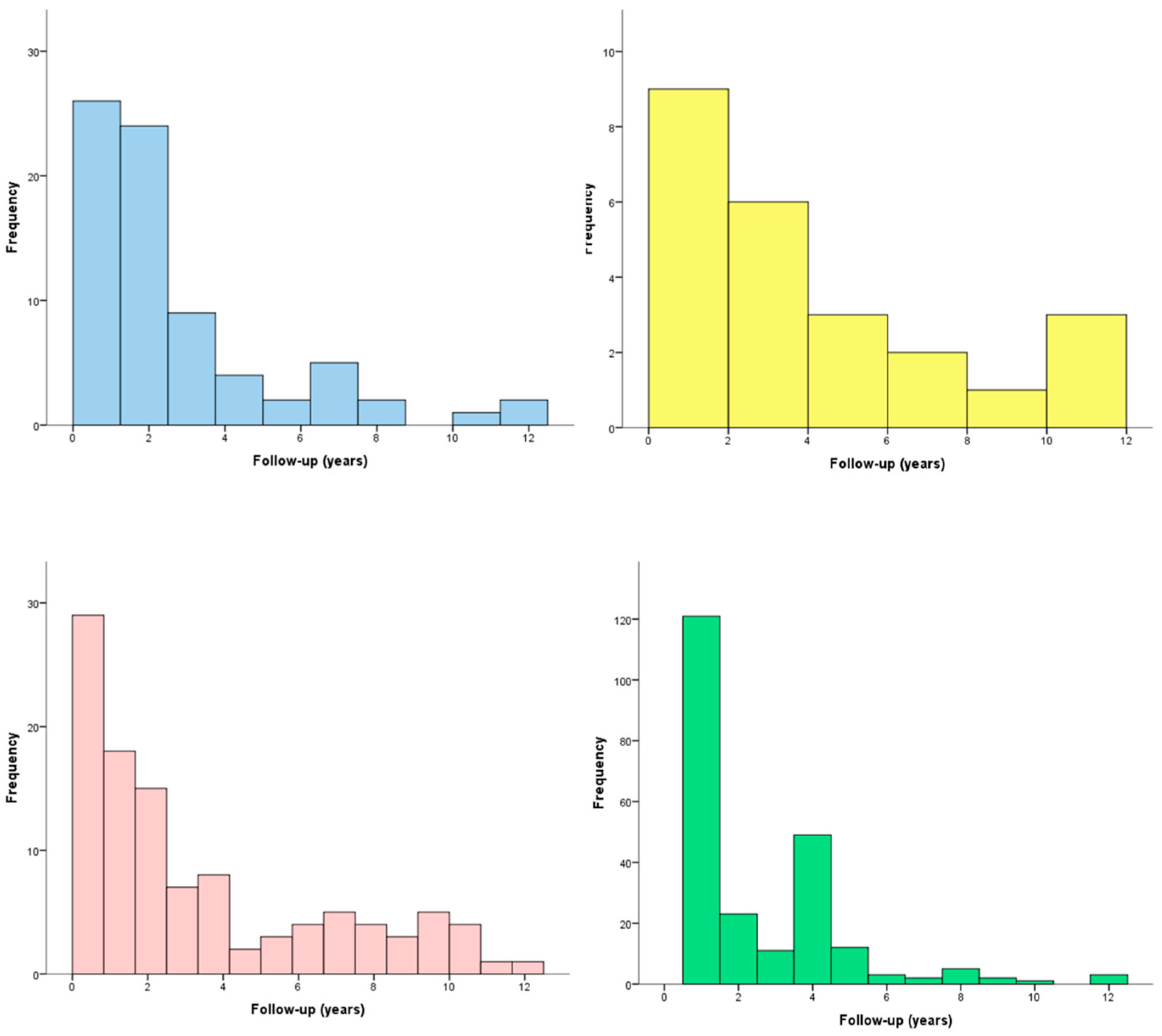
3.3. Follow-Up
3.4. Risk of Late Drop-Out
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef]
- Volta, U.; Fabbri, A.; Parisi, C.; Piscaglia, M.; Caio, G.; Tovoli, F.; Fiorini, E. Old and new serological tests for celiac disease screening. Expert Rev. Gastroenterol. Hepatol. 2010, 4, 31–35. [Google Scholar] [CrossRef]
- Haines, M.L.; Anderson, R.P.; Gibson, P.R. Systematic review: The evidence base for long-term management of coeliac disease. Aliment. Pharmacol. Ther. 2008, 28, 1042–1066. [Google Scholar] [CrossRef]
- Tovoli, F.; Granito, A.; Negrini, G.; Guidetti, E.; Faggiano, C.; Bolondi, L. Long term effects of gluten-free diet in non-celiac wheat sensitivity. Clin. Nutr. 2019, 38, 357–363. [Google Scholar] [CrossRef]
- Lee, A.; Newman, J.M. Celiac diet: Its impact on quality of life. J. Am. Diet. Assoc. 2003, 103, 1533–1535. [Google Scholar] [CrossRef]
- Martínez, M.I.; Alegre, A.; Garcia-Ibanez, J.; Cauli, O. Quality of Life in People with Coeliac Disease: Psychological and Socio- Economic Aspects. Endocr. Metab. Immune Disord.-Drug Targets 2019, 19, 116–120. [Google Scholar] [CrossRef]
- Tovoli, F.; Negrini, G.; Farì, R.; Guidetti, E.; Faggiano, C.; Napoli, L.; Bolondi, L.; Granito, A. Increased risk of nonalcoholic fatty liver disease in patients with coeliac disease on a gluten-free diet: Beyond traditional metabolic factors. Aliment. Pharmacol. Ther. 2018, 48, 538–546. [Google Scholar] [CrossRef]
- Tortora, R.; Capone, P.; De Stefano, G.; Imperatore, N.; Gerbino, N.; Donetto, S.; Monaco, V.; Caporaso, N.; Rispo, A. Metabolic syndrome in patients with coeliac disease on a gluten-free diet. Aliment. Pharmacol. Ther. 2015, 41, 352–359. [Google Scholar] [CrossRef] [Green Version]
- Imperatore, N.; Tortora, R.; Testa, A.; Gerbino, N.; Caporaso, N.; Rispo, A. Proton pump inhibitors as risk factor for metabolic syndrome and hepatic steatosis in coeliac disease patients on gluten-free diet. J. Gastroenterol. 2018, 53, 507–516. [Google Scholar] [CrossRef]
- Reilly, N.R.; Lebwohl, B.; Hultcrantz, R.; Green, P.H.R.; Ludvigsson, J.F. Increased risk of non-alcoholic fatty liver disease after diagnosis of celiac disease. J. Hepatol. 2015, 62, 1405–1411. [Google Scholar] [CrossRef] [Green Version]
- Rubio-Tapia, A.; Hill, I.D.; Kelly, C.P.; Calderwood, A.H.; Murray, J.A. ACG Clinical Guidelines: Diagnosis and Management of Celiac Disease. Am. J. Gastroenterol. 2013, 108, 656–676. [Google Scholar] [CrossRef] [Green Version]
- Husby, S.; Murray, J.A.; Katzka, D.A. AGA Clinical Practice Update on Diagnosis and Monitoring of Celiac Disease—Changing Utility of Serology and Histologic Measures: Expert Review. Gastroenterology 2019, 156, 885–889. [Google Scholar] [CrossRef]
- Hill, I.D.; Fasano, A.; Guandalini, S.; Hoffenberg, E.; Levy, J.; Reilly, N.; Verma, R. NASPGHAN Clinical Report on the Diagnosis and Treatment of Gluten-related Disorders. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 156–165. [Google Scholar] [CrossRef]
- Al-Toma, A.; Volta, U.; Auricchio, R.; Castillejo, G.; Sanders, D.S.; Cellier, C.; Mulder, C.J.; Lundin, K.E.A. European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United Eur. Gastroenterol. J. 2019, 7, 583–613. [Google Scholar] [CrossRef]
- Protocollo Diagnosi e Follow-Up Celiachia [Internet]. AIC—Associazione Italiana Celiachia. Available online: https://www.celiachia.it/celiachia/diagnosi/protocollo-diagnosi-e-follow-up-celiachia/ (accessed on 28 September 2020).
- Raiteri, A.; Granito, A.; Giamperoli, A.; Catenaro, T.; Negrini, G.; Tovoli, F. Current guidelines for the management of celiac disease: A systematic review with comparative analysis. World J. Gastroenterol. 2022, 28, 154–176. [Google Scholar] [CrossRef]
- Biagi, F.; Schiepatti, A.; Maiorano, G.; Fraternale, G.; Agazzi, S.; Zingone, F.; Ciacci, C.; Volta, U.; Caio, G.; Tortora, R.; et al. Risk of complications in coeliac patients depends on age at diagnosis and type of clinical presentation. Dig. Liver Dis. 2018, 50, 549–552. [Google Scholar] [CrossRef]
- Biagi, F.; Corazza, G.R. Do different patients with coeliac disease have different mortality rates? Gut 2014, 64, 1187–1188. [Google Scholar] [CrossRef]
- Kinos, S.; Kurppa, K.; Ukkola, A.; Collin, P.; Lähdeaho, M.-L.; Huhtala, H.; Kekkonen, L.; Mäki, M.; Kaukinen, K. Burden of Illness in Screen-detected Children with Celiac Disease and Their Families. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 412–416. [Google Scholar] [CrossRef]
- Kivelä, L.; Kaukinen, K.; Huhtala, H.; Lähdeaho, M.-L.; Mäki, M.; Kurppa, K. At-Risk Screened Children with Celiac Disease are Comparable in Disease Severity and Dietary Adherence to Those Found because of Clinical Suspicion: A Large Cohort Study. J. Pediatr. 2017, 183, 115–121.e2. [Google Scholar] [CrossRef] [Green Version]
- Kurppa, K.; Lauronen, O.; Collin, P.; Ukkola, A.; Laurila, K.; Huhtala, H.; Mäki, M.; Kaukinen, K. Factors Associated with Dietary Adherence in Celiac Disease: A Nationwide Study. Digestion 2012, 86, 309–314. [Google Scholar] [CrossRef]
- Vilppula, A.; Kaukinen, K.; Luostarinen, L.; Krekelä, I.; Patrikainen, H.; Valve, R.; Luostarinen, M.; Laurila, K.; Mäki, M.; Collin, P. Clinical benefit of gluten-free diet in screen-detected older celiac disease patients. BMC Gastroenterol. 2011, 11, 136. [Google Scholar] [CrossRef] [Green Version]
- Capuozzo, M.; Ottaiano, A.; Nava, E.; Cascone, S.; Cinque, C.; Iaffaioli, R.V.; Scognamiglio, C.; Palumbo, E.; Capuozzo, M. Epidemiology and Economic Impact of Celiac Disease in the South Vesuvian Area of Naples: A Survey. Front. Public Health 2013, 1, 18. [Google Scholar] [CrossRef] [Green Version]
- Silvester, J.A.; Graff, L.A.; Rigaux, L.; Walker, J.R.; Duerksen, D.R. Symptomatic suspected gluten exposure is common among patients with coeliac disease on a gluten-free diet. Aliment. Pharmacol. Ther. 2016, 44, 612–619. [Google Scholar] [CrossRef] [Green Version]
- Biagi, F.; Bianchi, P.I.; Marchese, A.; Trotta, L.; Vattiato, C.; Balduzzi, D.; Brusco, G.; Andrealli, A.; Cisarò, F.; Astegiano, M.; et al. A score that verifies adherence to a gluten-free diet: A cross-sectional, multicentre validation in real clinical life. Br. J. Nutr. 2012, 108, 1884–1888. [Google Scholar] [CrossRef]
- Pekki, H.; Kaukinen, K.; Ilus, T.; Mäki, M.; Huhtala, H.; Laurila, K.; Kurppa, K. Long-term follow-up in adults with coeliac disease: Predictors and effect on health outcomes. Dig. Liver Dis. 2018, 50, 1189–1194. [Google Scholar] [CrossRef] [Green Version]
- Pekki, H.; Kurppa, K.; Mäki, M.; Huhtala, H.; Laurila, K.; Ilus, T.; Kaukinen, K. Performing routine follow-up biopsy 1 year after diagnosis does not affect long-term outcomes in coeliac disease. Aliment. Pharmacol. Ther. 2017, 45, 1459–1468. [Google Scholar] [CrossRef] [Green Version]
- Bebb, J.R.; Lawson, A.; Knight, T.; Long, R.G. Long-term follow-up of coeliac disease—What do coeliac patients want? Aliment. Pharmacol. Ther. 2006, 23, 827–831. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | |
|---|---|
| Female sex | 453 (78.4) |
| Age at diagnosis | |
| 40 years | 327 (56.6) |
| 40–59 years | 200 (34.6) |
| ≥60 years | 51 (8.8) |
| Family history of CD | 109 (18.9) |
| Symptomatic CD | 471 (81.5) |
| Classical presentation | 107 (18.5) |
| Iron-deficiency anemia | 275 (47.6) |
| Variable | |
|---|---|
| GFD adherence | 468 (87.0) |
| IBS-like symptoms (total) | 80 (14.9) |
| * IBS-mixed-like symptoms | 44 (8.2) |
| * IBS-diarrhea-like symptoms | 9 (1.7) |
| * IBS-constipation-like symptoms | 27 (5.0) |
| GERD-like symptoms | 24 (4.5) |
| Metabolic alterations (at least one) | 109 (20.3) |
| * Weight gain > 10 kg | 55 (10.2) |
| * Hypercholesterolemia | 59 (11.0) |
| * Metabolic syndrome | 25 (4.6) |
| Osteoporosis | 238 (44.2) |
| Univariable Analyses | Multivariable Analyses | |||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p | Hazard Ratio | 95% CI | p | |
| 0.994 | 0.738–1.339 | 0.880 | Female sex | |||
| Age at diagnosis | ||||||
| - | Reference | - | <40 years | - | Reference | - |
| 0.583 | 0.444–0.765 | <0.001 | 40–59 years | 0.600 | 0.455–0.790 | <0.001 |
| 0.556 | 0.333–0.927 | 0.024 | ≥60 years | 0.598 | 0.357–0.997 | 0.048 |
| 0.900 | 0.659–1.230 | 0.510 | Family history of CD | |||
| 1.235 | 0.906–1.683 | 0.181 | Symptomatic CD | |||
| 0.648 | 0.456–0.920 | 0.015 | Classical presentation | 0.641 | 0.446–0.920 | 0.016 |
| 1.019 | 0.803–1.292 | 0.880 | Iron deficiency | |||
| 0.761 | 0.597–0.970 | 0.027 | Osteoporosis * | 0.846 | 0.659–1.086 | 0.190 |
| 1.317 | 0.944–1.836 | 0.105 | GFD compliance * | |||
| 1.356 | 0.934–1.968 | 0.190 | IBS-like symptoms * | |||
| 0.966 | 0.397–2.349 | 0.939 | GERD-like symptoms * | |||
| 0.865 | 0.579–1.291 | 0.477 | Metabolic alterations * | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tovoli, F.; Faggiano, C.; Raiteri, A.; Giamperoli, A.; Catenaro, T.; Sansone, V.; Pallotta, D.P.; Granito, A. Risk of Drop-Out from Follow-Up Evaluations for Celiac Disease: Is It Similar for All Patients? Nutrients 2022, 14, 1223. https://doi.org/10.3390/nu14061223
Tovoli F, Faggiano C, Raiteri A, Giamperoli A, Catenaro T, Sansone V, Pallotta DP, Granito A. Risk of Drop-Out from Follow-Up Evaluations for Celiac Disease: Is It Similar for All Patients? Nutrients. 2022; 14(6):1223. https://doi.org/10.3390/nu14061223
Chicago/Turabian StyleTovoli, Francesco, Chiara Faggiano, Alberto Raiteri, Alice Giamperoli, Teresa Catenaro, Vito Sansone, Dante Pio Pallotta, and Alessandro Granito. 2022. "Risk of Drop-Out from Follow-Up Evaluations for Celiac Disease: Is It Similar for All Patients?" Nutrients 14, no. 6: 1223. https://doi.org/10.3390/nu14061223
APA StyleTovoli, F., Faggiano, C., Raiteri, A., Giamperoli, A., Catenaro, T., Sansone, V., Pallotta, D. P., & Granito, A. (2022). Risk of Drop-Out from Follow-Up Evaluations for Celiac Disease: Is It Similar for All Patients? Nutrients, 14(6), 1223. https://doi.org/10.3390/nu14061223