
Global Burden of Vitamin A Deficiency in 204 Countries and Territories from 1990–2019

Abstract
1. Introduction
2. Materials and Methods
2.1. Overview and Definitions
2.2. Data Sources
2.3. Statistical Analysis
3. Results
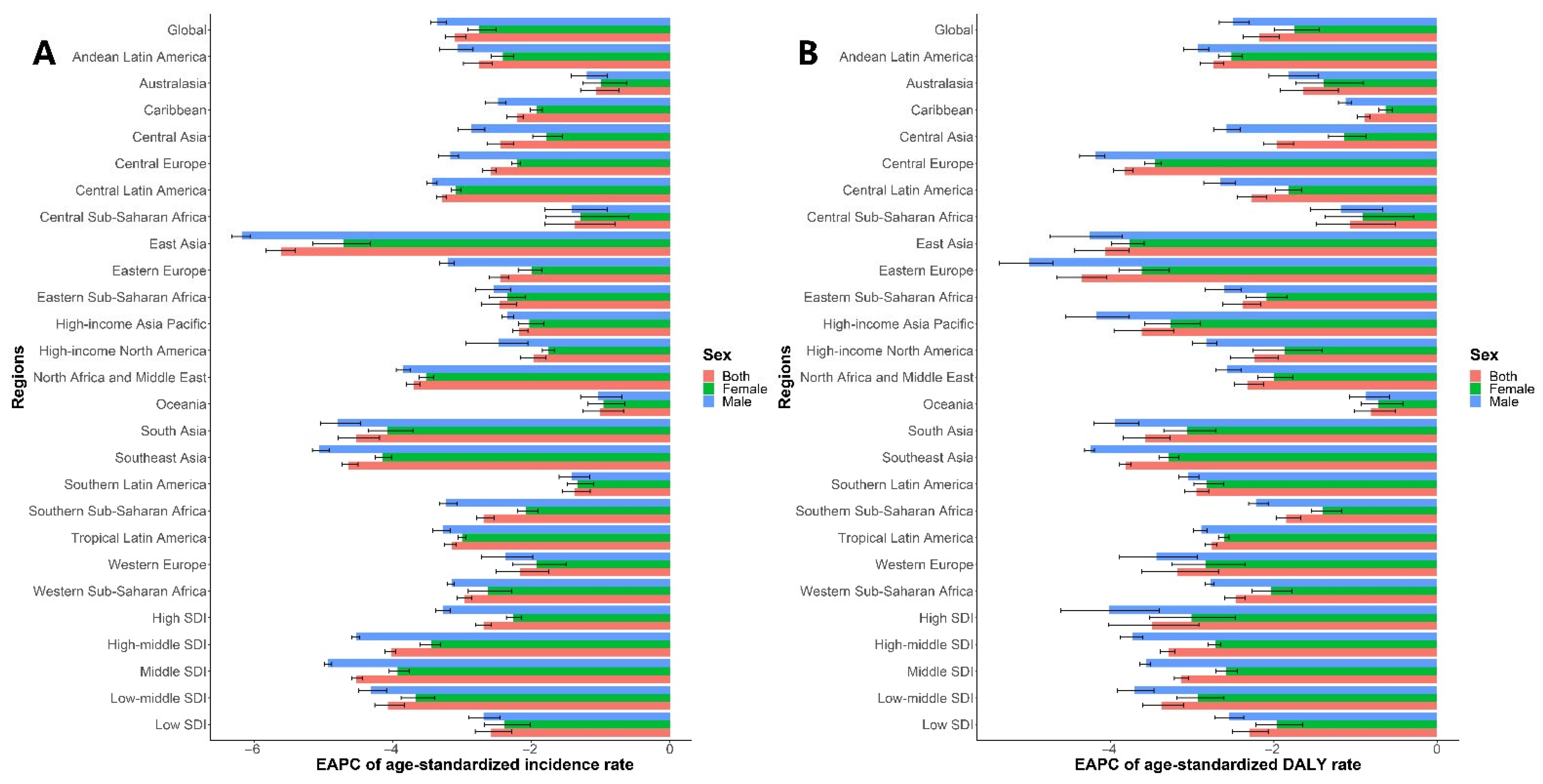
3.1. Analysis of Changes in VAD Incidence
3.2. Analysis of Changes in DALYs Due to VAD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Darnton-Hill, I. Public Health Aspects in the Prevention and Control of Vitamin Deficiencies. Curr. Dev. Nutr. 2019, 3, nzz075. [Google Scholar] [CrossRef]
- Xu, Y.; Shan, Y.; Lin, X.; Miao, Q.; Lou, L.; Wang, Y.; Ye, J. Global patterns in vision loss burden due to vitamin A deficiency from 1990 to 2017. Public Health Nutr. 2021, 24, 5786–5794. [Google Scholar] [CrossRef]
- Aibana, O.; Franke, M.F.; Huang, C.-C.; Galea, J.T.; Calderon, R.; Zhang, Z.; Becerra, M.C.; Smith, E.R.; Ronnenberg, A.G.; Contreras, C.; et al. Impact of Vitamin A and Carotenoids on the Risk of Tuberculosis Progression. Clin. Infect. Dis. 2017, 65, 900–909. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Liu, J.; Xiong, X.; Yang, T.; Hou, N.; Liang, X.; Chen, J.; Cheng, Q.; Li, T. Correlation between Nutrition and Symptoms: Nutritional Survey of Children with Autism Spectrum Disorder in Chongqing, China. Nutrients 2016, 8, 294. [Google Scholar] [CrossRef]
- Wołoszynowska-Fraser, M.U.; Kouchmeshky, A.; McCaffery, P. Vitamin A and Retinoic Acid in Cognition and Cognitive Disease. Annu. Rev. Nutr. 2020, 40, 247–272. [Google Scholar] [CrossRef] [PubMed]
- Mertens, E.; Peñalvo, J.L. The Burden of Malnutrition and Fatal COVID-19: A Global Burden of Disease Analysis. Front. Nutr. 2021, 7, 619850. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Prevalence of Vitamin A Deficiency in Populations at Risk 1995–2005: WHO Global Database on Vitamin A Deficiency; WHO: Geneva, Switzerland, 2009. Available online: https://www.who.int/publications/i/item/9789241598019 (accessed on 15 January 2022).
- Keats, E.C.; Neufeld, L.M.; Garrett, G.S.; Mbuya, M.N.N.; Bhutta, Z.A. Improved micronutrient status and health outcomes in low- and middle-income countries following large-scale fortification: Evidence from a systematic review and meta-analysis. Am. J. Clin. Nutr. 2019, 109, 1696–1708. [Google Scholar] [CrossRef]
- Alaofè, H.; Burney, J.; Naylor, R.; Taren, D. Prevalence of anaemia, deficiencies of iron and vitamin A and their determinants in rural women and young children: A cross-sectional study in Kalalé district of northern Benin. Public Health Nutr. 2017, 20, 1203–1213. [Google Scholar] [CrossRef] [PubMed]
- Sahile, Z.; Yilma, D.; Tezera, R.; Bezu, T.; Haileselassie, W.; Seifu, B.; Ali, J.H. Prevalence of Vitamin A Deficiency among Preschool Children in Ethiopia: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2020, 2020, 8032894. [Google Scholar] [CrossRef]
- Rajaeieh, G.; Takian, A.; Kalantari, N.; Mohammadi-Nasrabadi, F. Analysis for policy to overcome barriers to reducing the prevalence of vitamin a deficiency among children (15–23 months) in Iran. BMC Public Health 2021, 21, 1234. [Google Scholar] [CrossRef]
- Bahreynian, M.; Qorbani, M.; Naderimagham, S.; Nejatinamini, S.; Jafari, A.A.-; Sharifi, F.; Saqib, F.; Khajavi, A.; Mansourian, M.; Ahmadishokouh, A.A.; et al. Burden of disease attributable to vitamin A deficiency in Iranian population aged less than five years: Findings from the global burden of disease study 2010. J. Diabetes Metab. Disord. 2017, 16, 32. [Google Scholar] [CrossRef] [PubMed]
- Hassen, H.Y.; Ali, J.H.; Gebreyesus, S.H.; Endris, B.S.; Temesgen, A.M. National incidence, prevalence and disability-adjusted life years (DALYs) of common micronutrient deficiencies in Ethiopia from 1990 to 2017: Estimates from the global burden of diseases study. Glob. Health Action 2020, 13, 1776507. [Google Scholar] [CrossRef] [PubMed]
- Boyers, L.N.; Karimkhani, C.; Hilton, J.; Richheimer, W.; Dellavalle, R.P. Global Burden of Eye and Vision Disease as Reflected in theCochrane Database of Systematic Reviews. JAMA Ophthalmol. 2015, 133, 25–31. [Google Scholar] [CrossRef]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222, Erratum in Lancet 2020, 396, 1562. [Google Scholar] [CrossRef]
- Liu, X.; Jiang, J.; Yu, C.; Wang, Y.; Sun, Y.; Tang, J.; Chen, T.; Bi, Y.; Liu, Y.; Zhang, Z.-J. Secular trends in incidence and mortality of bladder cancer in China, 1990–2017: A joinpoint and age-period-cohort analysis. Cancer Epidemiol. 2019, 61, 95–103. [Google Scholar] [CrossRef]
- Masters, W.A.; Rosenblum, N.Z.; Alemu, R.G. Agricultural Transformation, Nutrition Transition and Food Policy in Africa: Preston Curves Reveal New Stylised Facts. J. Dev. Stud. 2018, 54, 788–802. [Google Scholar] [CrossRef]
- Imdad, A.; Mayo-Wilson, E.; Herzer, K.; Bhutta, Z.A. Vitamin A supplementation for preventing morbidity and mortality in children from six months to five years of age. Cochrane Database Syst. Rev. 2017, 3, CD008524. [Google Scholar] [CrossRef]
- Strunz, E.C.; Suchdev, P.S.; Addiss, D.G. Soil-Transmitted Helminthiasis and Vitamin A Deficiency: Two Problems, One Policy. Trends Parasitol. 2016, 32, 10–18. [Google Scholar] [CrossRef]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451, Erratum in Lancet 2013, 382, 396. [Google Scholar] [CrossRef]
- Stevens, G.A.; Bennett, J.E.; Hennocq, Q.; Lu, Y.; De-Regil, L.M.; Rogers, L.; Danaei, G.; Li, G.; White, R.A.; Flaxman, S.R.; et al. Trends and mortality effects of vitamin A deficiency in children in 138 low-income and middle-income countries between 1991 and 2013: A pooled analysis of population-based surveys. Lancet Glob. Health 2015, 3, e528–e536. [Google Scholar] [CrossRef]
- Wu, D.C.N.; Horton, S.; Saleh, N.; Mosha, T.C.; Yusuph, N. Impact of behaviour change communication interventions on sales of fortified sunflower oil in Tanzania: A spatial–temporal analysis and association study. Matern. Child Nutr. 2019, 15, e12873. [Google Scholar] [CrossRef]
- Yang, C.; Chen, J.; Liu, Z.; Yun, C.; Piao, J.; Yang, X. Prevalence and influence factors of vitamin A deficiency of Chinese pregnant women. Nutr. J. 2015, 15, 12. [Google Scholar] [CrossRef]
- Bassey, C.; Crooks, H.; Paterson, K.; Ball, R.; Howell, K.; Humphries-Cuff, I.; Gaffigan, K.; Rao, N.; Whitty, J.A.; Hooper, L. Impact of home food production on nutritional blindness, stunting, wasting, underweight and mortality in children: A systematic review and meta-analysis of controlled trials. Crit. Rev. Food Sci. Nutr. 2020, 1–14. [Google Scholar] [CrossRef]
- WHO. Medical Product Alert N°1/2021: Falsified Vitamin A [Internet]; WHO: Geneva, Switzerland, 2021. Available online: https://www.who.int/news/item/10-03-2021-medical-product-alert-n-1-2021-falsified-vitamin-a (accessed on 15 January 2022).
- Low, J.W.; Mwanga, R.O.; Andrade, M.; Carey, E.; Ball, A.-M. Tackling vitamin A deficiency with biofortified sweetpotato in sub-Saharan Africa. Glob. Food Secur. 2017, 14, 23–30. [Google Scholar] [CrossRef]
- Lewandowski, K.; Zhang, X.; Hayes, M.; Ferruzzi, M.; Paton, C. Design and Nutrient Analysis of a Carotenoid-Rich Food Product to Address Vitamin A and Protein Deficiency. Foods 2021, 10, 1019. [Google Scholar] [CrossRef] [PubMed]
- Laurie, S.M.; Faber, M.; Claasen, N. Incorporating orange-fleshed sweet potato into the food system as a strategy for improved nutrition: The context of South Africa. Food Res. Int. 2018, 104, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Siwela, M.; Pillay, K.; Govender, L.; Lottering, S.; Mudau, F.N.; Modi, A.T.; Mabhaudhi, T. Biofortified Crops for Combating Hidden Hunger in South Africa: Availability, Acceptability, Micronutrient Retention and Bioavailability. Foods 2020, 9, 815. [Google Scholar] [CrossRef]
- Ekpa, O.; Fogliano, V.; Linnemann, A. Carotenoid stability and aroma retention during the post-harvest storage of biofortified maize. J. Sci. Food Agric. 2021, 101, 4042–4049. [Google Scholar] [CrossRef] [PubMed]
- Ghouchi-Eskandar, N.; Simovic, S.; Prestidge, C.A. Solid-state nanoparticle coated emulsions for encapsulation and improving the chemical stability of all-trans-retinol. Int. J. Pharm. 2012, 423, 384–391. [Google Scholar] [CrossRef]
- GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef]
- Yamamura, C.M.; Sullivan, K.M.; Van Der Haar, F.; Auerbach, S.B.; Iohp, K.K. Risk factors for vitamin A deficiency among preschool aged children in Pohnpei, Federated States of Micronesia. J. Trop. Pediatr. 2004, 50, 16–19. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Paul, J.-Y.; Harding, R.; Tushemereirwe, W.; Dale, J. Banana21: From Gene Discovery to Deregulated Golden Bananas. Front. Plant Sci. 2018, 9, 558. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; West, K.P., Jr.; Black, R.E. The Epidemiology of Global Micronutrient Deficiencies. Ann. Nutr. Metab. 2015, 66 (Suppl. S2), 22–33. [Google Scholar] [CrossRef] [PubMed]
- Sivakumar, B.; Reddy, V. Absorption of labelled vitamin A in children during infection. Br. J. Nutr. 1972, 27, 299–304. [Google Scholar] [CrossRef]
- Jevnikar, K.; Šuštar, M.; Kozjek, N.R.; Štrucl, A.M.; Markelj, Š.; Hawlina, M.; Fakin, A. Disruption of the outer segments of the photoreceptors on OCT as a feature of vitamin A deficiency. Retin. Cases Brief Rep. 2020. [Google Scholar] [CrossRef]
- GBD 2017 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922, Erratum in Lancet 2019, 393, e44. [Google Scholar] [CrossRef]
- Martínez-Torres, J.; Meneses-Echavéz, J.F.; Ramírez-Vélez, R. Prevalence and demographic factors associated with vitamin A deficiency in Colombian children aged 12–59 months. Endocrinol. Nutr. 2014, 61, 460–466. [Google Scholar] [CrossRef]
- Disalvo, L.; Biochemista, A.V.; Biochemista, N.M.; Biochemista, A.M.; Fasano, M.V.; González, H.F. Vitamin A deficiency and associated factors in preschoolers from the outskirts of La Plata, Buenos Aires. Arch. Argent. Pediatr. 2019, 117, 19–25. [Google Scholar] [CrossRef]
- Beydoun, H.A.; Shroff, M.R.; Mohan, R.; Beydoun, M.A. Associations of serum vitamin A and carotenoid levels with markers of prostate cancer detection among US men. Cancer Causes Control 2011, 22, 1483–1495. [Google Scholar] [CrossRef]
- Jensen, K.J.; Ndure, J.; Plebanski, M.; Flanagan, K.L. Heterologous and sex differential effects of administering vitamin A supplementation with vaccines. Trans. R. Soc. Trop. Med. Hyg. 2014, 109, 36–45. [Google Scholar] [CrossRef]
- Kennedy, E.; Binder, G.; Humphries-Waa, K.; Tidhar, T.; Cini, K.; Comrie-Thomson, L.; Vaughan, C.; Francis, K.; Scott, N.; Wulan, N.; et al. Gender inequalities in health and wellbeing across the first two decades of life: An analysis of 40 low-income and middle-income countries in the Asia-Pacific region. Lancet Glob. Health 2020, 8, e1473–e1488. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| 1990 | 2019 | 1990–2019 | ||||
|---|---|---|---|---|---|---|
| Age-Standardized Incidence Rate (per 100,000) | Age-Standardized Incidence Rate (per 100,000) | Change in Number No. (%) | EAPC | |||
| No. (95% UI) | Male/Female Ratio | No. (95% UI) | Male/Female Ratio | No. (95% CI) | ||
| Overall | 17,323.23 (16,526.51, 18,138.92) | 1.57 | 6955.65 (6645.87, 7294.23) | 1.31 | −59.85% | −3.11 (−3.24, −2.94) |
| Sex | ||||||
| Male | 21,073.77 (19,711.46, 22,557.32) | NA | 7886.24 (7367.67, 8489.75) | NA | −62.58% | −3.36 (−3.45, −3.23) |
| Female | 13,456.51 (12,848.51, 14,141.38) | NA | 5999.11 (5719.02, 6307.27) | NA | −55.42% | −2.75 (−2.92, −2.51) |
| Sociodemographic index | ||||||
| Low | 40,460.46 (39,202.05, 41,687.35) | 1.57 | 19,156.10 (18,357.37, 19,950.88) | 1.46 | −52.65% | −2.58 (−2.81, −2.28) |
| Low-middle | 29,005.62 (27,110.79, 30,890.15) | 1.62 | 8877.03 (8202.49, 9642.84) | 1.36 | −69.40% | −4.07 (−4.26, −3.83) |
| Middle | 14,790.69 (13,836.85, 15,869.70) | 1.61 | 3805.06 (3559.91, 4080.13) | 1.18 | −74.27% | −4.53 (−4.59, −4.44) |
| High-middle | 8176.35 (7576.08, 8905.80) | 1.35 | 2575.67 (2431.78, 2737.05) | 0.96 | −68.50% | −4.02 (−4.11, −3.96) |
| High | 1338.23 (1268.38, 1413.80) | 0.80 | 586.69 (550.35, 625.85) | 0.60 | −56.16% | −2.69 (−2.80, −2.58) |
| Region | ||||||
| Andean Latin America | 12,877.69 (11,631.86, 14,260.37) | 1.18 | 5904.69 (5259.36, 6633.17) | 1.03 | −54.15% | −2.75 (−2.98, −2.56) |
| Australasia | 237.41 (210.38, 270.03) | 0.59 | 148.85 (131.41, 168.77) | 0.59 | −37.30% | −1.07 (−1.29, −0.74) |
| Caribbean | 11,146.70 (10,301.07, 11,991.62) | 1.19 | 6289.74 (5659.18, 6996.38) | 1.05 | −43.57% | −2.21 (−2.35, −2.12) |
| Central Asia | 8840.26 (8009.36, 9737.17) | 1.96 | 4272.03 (3883.12, 4669.62) | 1.48 | −51.68% | −2.45 (−2.64, −2.25) |
| Central Europe | 15,274.02 (14,477.09, 16,139.86) | 0.71 | 7477.38 (7089.51, 7916.52) | 0.57 | −51.05% | −2.59 (−2.70, −2.51) |
| Central Latin America | 14,629.63 (13,257.67, 16,046.77) | 1.56 | 5717.55 (5096.11, 6419.49) | 1.43 | −60.92% | −3.29 (−3.37, −3.23) |
| Central Sub-Saharan Africa | 43,280.37 (39,834.15, 46,536.67) | 1.80 | 25,905.22 (23,288.44, 28,883.03) | 1.79 | −40.15% | −1.37 (−1.80, −0.79) |
| East Asia | 11,210.77 (9382.33, 13,316.53) | 1.99 | 2183.64 (1847.06, 2605.03) | 1.18 | −80.52% | −5.61 (−5.83, −5.41) |
| Eastern Europe | 1071.28 (979.53, 1179.11) | 0.77 | 530.88 (481.60, 587.02) | 0.56 | −50.44% | −2.45 (−2.61, −2.33) |
| Eastern Sub-Saharan Africa | 46,770.60 (45,268.61, 48,255.91) | 1.32 | 23,500.02 (22,337.24, 24,765.11) | 1.27 | −49.75% | −2.46 (−2.72, −2.21) |
| High-income Asia Pacific | 1376.91 (1194.36, 1589.88) | 0.82 | 683.87 (599.04, 779.97) | 0.80 | −50.33% | −2.18 (−2.27, −2.05) |
| High-income North America | 811.05 (703.77, 924.89) | 0.39 | 485.64 (408.06, 574.05) | 0.36 | −40.12% | −1.97 (−2.16, −1.79) |
| North Africa and Middle East | 15,427.65 (14,749.24, 16,089.90) | 1.37 | 5249.91 (4905.88, 5602.53) | 1.26 | −65.97% | −3.70 (−3.80, −3.60) |
| Oceania | 19,889.72 (18,034.35, 21,935.52) | 1.42 | 13,011.64 (11,381.72, 14,879.79) | 1.36 | −34.58% | −1.01 (−1.25, −0.67) |
| South Asia | 27,177.40 (24,364.57, 30,028.67) | 1.69 | 7189.30 (6181.29, 8388.98) | 1.37 | −73.55% | −4.53 (−4.79, −4.19) |
| Southeast Asia | 21,792.80 (20,300.59, 23,360.26) | 1.32 | 5175.32 (4667.95, 5733.85) | 1.01 | −76.25% | −4.64 (−4.73, −4.50) |
| Southern Latin America | 10,805.24 (9611.36, 12,213.65) | 1.44 | 6672.80 (5811.84, 7650.26) | 1.40 | −38.24% | −1.38 (−1.55, −1.15) |
| Southern Sub-Saharan Africa | 18,153.70 (16,488.62, 20,003.67) | 1.38 | 7834.62 (7001.01, 8690.17) | 1.03 | −56.84% | −2.69 (−2.79, −2.54) |
| Tropical Latin America | 24,605.66 (22,010.20, 27,545.33) | 1.27 | 10,005.39 (8592.70, 11,600.54) | 1.21 | −59.34% | −3.15 (−3.25, −3.08) |
| Western Europe | 1408.59 (1320.28, 1508.58) | 1.17 | 683.24 (637.29, 735.61) | 1.08 | −51.49% | −2.16 (−2.51, −1.75) |
| Western Sub-Saharan Africa | 36,703.57 (35,417.46, 38,048.52) | 1.93 | 15,570.91 (14,825.25, 16,315.94) | 1.73 | −57.58% | −2.97 (−3.07, −2.86) |
| 1990 | 2019 | 1990–2019 | ||||
|---|---|---|---|---|---|---|
| Age-Standardized DALY Rate (per 100,000) | Age-Standardized DALY Rate (per 100,000) | Change in Number No. (%) | EAPC | |||
| No. (95% UI) | Male/Female Ratio | No. (95% UI) | Male/Female Ratio | No. (95% CI) | ||
| Overall | 31.95 (22.11, 45.30) | 1.42 | 16.91 (11.53, 23.47) | 1.17 | −47.07% | −2.18 (−2.38, −1.93) |
| Sex | ||||||
| Male | 37.29 (25.60, 53.04) | NA | 18.20 (12.41, 25.16) | NA | −51.20% | −2.50 (−2.67, −2.30) |
| Female | 26.30 (17.83, 37.37) | NA | 15.54 (10.55, 21.80) | NA | −40.91% | −1.75 (−1.99, −1.44) |
| Sociodemographic index | ||||||
| Low | 73.54 (50.66, 102.90) | 1.44 | 38.02 (26.12, 52.78) | 1.24 | −48.29% | −2.30 (−2.51, −2.07) |
| Low-middle | 50.95 (35.19, 72.27) | 1.42 | 19.32 (12.93, 27.45) | 1.16 | −62.07% | −3.38 (−3.61, −3.11) |
| Middle | 21.53 (14.48, 30.75) | 1.37 | 8.61 (5.75, 12.42) | 1.06 | −60.03% | −3.14 (−3.22, −3.05) |
| High-middle | 9.28 (6.17, 13.25) | 1.40 | 3.74 (2.49, 5.43) | 1.08 | −59.68% | −3.29 (−3.39, −3.21) |
| High | 0.91 (0.58, 1.35) | 1.00 | 0.29 (0.18, 0.44) | 0.77 | −67.90% | −3.49 (−4.03, −2.92) |
| Region | ||||||
| Andean Latin America | 19.29 (12.72, 27.67) | 1.23 | 9.14 (5.99, 13.34) | 1.10 | −52.61% | −2.74 (−2.90, −2.62) |
| Australasia | 0.10 (0.05, 0.19) | 1.31 | 0.05 (0.03, 0.09) | 1.24 | −50.11% | −1.64 (−1.92, −1.21) |
| Caribbean | 16.71 (10.96, 24.06) | 1.18 | 12.76 (8.29, 19.05) | 1.05 | −23.69% | −0.89 (−0.98, −0.82) |
| Central Asia | 13.52 (8.72, 19.67) | 1.54 | 7.59 (5.02, 11.02) | 1.08 | −43.84% | −1.96 (−2.13, −1.76) |
| Central Europe | 10.14 (6.45, 15.08) | 1.03 | 3.55 (2.22, 5.43) | 0.86 | −64.97% | −3.83 (−3.97, −3.73) |
| Central Latin America | 14.99 (9.90, 21.27) | 1.23 | 7.63 (5.06, 10.97) | 0.94 | −49.08% | −2.27 (−2.45, −2.09) |
| Central Sub-Saharan Africa | 73.73 (48.76, 103.15) | 1.42 | 49.08 (32.59, 69.88) | 1.37 | −33.43% | −1.07 (−1.48, −0.51) |
| East Asia | 10.80 (6.95, 15.80) | 1.70 | 3.75 (2.40, 5.64) | 1.52 | −65.26% | −4.07 (−4.44, −3.78) |
| Eastern Europe | 0.35 (0.22, 0.55) | 1.28 | 0.11 (0.06, 0.18) | 0.92 | −70.18% | −4.36 (−4.66, −4.05) |
| Eastern Sub-Saharan Africa | 69.27 (47.83, 97.67) | 1.27 | 35.90 (24.49, 50.85) | 1.13 | −48.18% | −2.38 (−2.63, −2.16) |
| High-income Asia Pacific | 1.14 (0.64, 1.84) | 0.70 | 0.35 (0.19, 0.60) | 0.55 | −69.02% | −3.62 (−3.96, −3.23) |
| High-income North America | 0.29 (0.16, 0.49) | 0.61 | 0.15 (0.08, 0.27) | 0.55 | −49.15% | −2.24 (−2.53, −1.95) |
| North Africa and Middle East | 20.07 (13.53, 28.81) | 1.32 | 10.17 (6.74, 14.32) | 1.17 | −49.35% | −2.32 (−2.48, −2.13) |
| Oceania | 26.96 (17.73, 39.26) | 1.30 | 18.30 (11.19, 27.04) | 1.24 | −32.11% | −0.81 (−1.01, −0.51) |
| South Asia | 55.94 (38.43, 79.56) | 1.44 | 20.24 (13.41, 29.10) | 1.12 | −63.81% | −3.58 (−3.85, −3.27) |
| Southeast Asia | 38.43 (26.06, 56.15) | 1.31 | 12.68 (8.35, 18.34) | 1.03 | −67.01% | −3.82 (−3.89, −3.75) |
| Southern Latin America | 10.14 (6.05, 15.65) | 1.44 | 4.24 (2.37, 7.09) | 1.36 | −58.18% | −2.95 (−3.09, −2.80) |
| Southern Sub-Saharan Africa | 29.88 (19.56, 42.74) | 1.34 | 16.42 (11.00, 23.58) | 1.10 | −45.07% | −1.85 (−1.97, −1.67) |
| Tropical Latin America | 22.99 (14.52, 34.01) | 1.06 | 10.17 (6.22, 15.05) | 1.00 | −55.77% | −2.76 (−2.84, −2.70) |
| Western Europe | 0.82 (0.51, 1.26) | 1.32 | 0.29 (0.17, 0.47) | 1.15 | −64.79% | −3.18 (−3.62, −2.68) |
| Western Sub-Saharan Africa | 74.45 (50.41, 104.17) | 1.64 | 37.04 (25.35, 51.76) | 1.35 | −50.24% | −2.47 (−2.60, −2.35) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, T.; Liu, S.; Zhang, R.; Zhao, Z.; Yu, H.; Pu, L.; Wang, L.; Han, L. Global Burden of Vitamin A Deficiency in 204 Countries and Territories from 1990–2019. Nutrients 2022, 14, 950. https://doi.org/10.3390/nu14050950
Zhao T, Liu S, Zhang R, Zhao Z, Yu H, Pu L, Wang L, Han L. Global Burden of Vitamin A Deficiency in 204 Countries and Territories from 1990–2019. Nutrients. 2022; 14(5):950. https://doi.org/10.3390/nu14050950
Chicago/Turabian StyleZhao, Tian, Shiwei Liu, Ruijie Zhang, Zhenping Zhao, Hu Yu, Liyuan Pu, Li Wang, and Liyuan Han. 2022. "Global Burden of Vitamin A Deficiency in 204 Countries and Territories from 1990–2019" Nutrients 14, no. 5: 950. https://doi.org/10.3390/nu14050950
APA StyleZhao, T., Liu, S., Zhang, R., Zhao, Z., Yu, H., Pu, L., Wang, L., & Han, L. (2022). Global Burden of Vitamin A Deficiency in 204 Countries and Territories from 1990–2019. Nutrients, 14(5), 950. https://doi.org/10.3390/nu14050950