
Pre-Pregnancy Body Mass Index and Risk of Macrosomia and Large for Gestational Age Births with Gestational Diabetes Mellitus as a Mediator: A Prospective Cohort Study in Central China

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
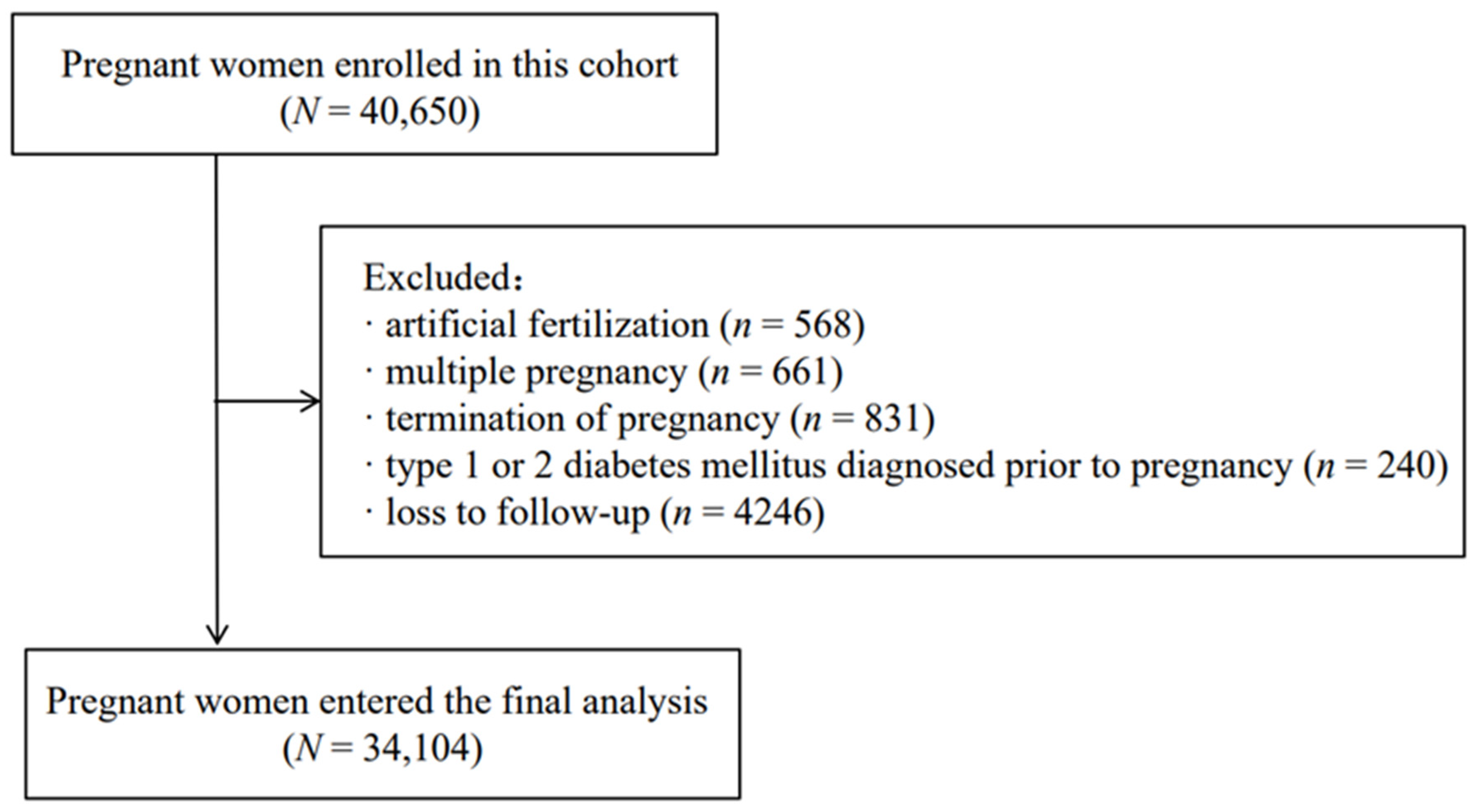
2.1. The Study Population
2.2. Information Collection
2.3. Outcome
2.4. Exposure
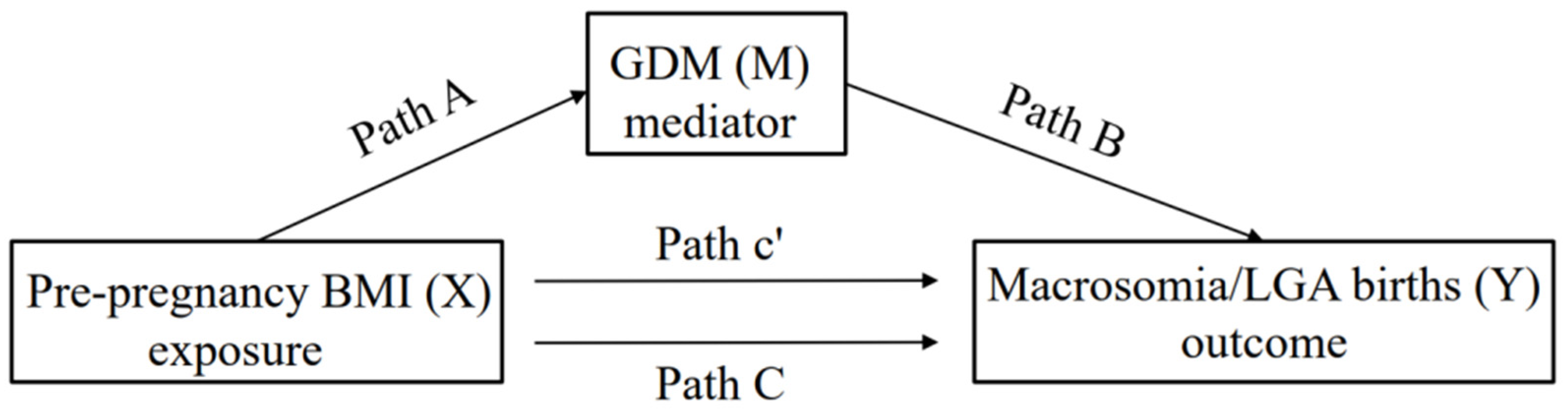
2.5. Mediator
2.6. Covariates
2.7. Statistical Analyses
3. Result
3.1. Characteristics of Participants
3.2. Prevalence of GDM, Macrosomia and LGA Births across Maternal Pre-Pregnancy BMI Status
3.3. Mediation Analysis
3.4. Assessment of Unmeasured Confounding
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Alfadhli, E.M. Gestational diabetes mellitus. Saudi Med. J. 2015, 36, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Sun, X.; Lu, L.; Liu, F.; Yuan, J. Prevalence of gestational diabetes mellitus in mainland China: A systematic review and meta-analysis. J. Diabetes Investig. 2018, 10, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Kc, K.; Shakya, S.; Zhang, H. Gestational diabetes mellitus and macrosomia: A literature review. Ann. Nutr. Metab. 2015, 66 (Suppl. 2), 14–20. [Google Scholar] [CrossRef] [PubMed]
- Landon, M.B.; Spong, C.Y.; Thom, E.; Carpenter, M.W.; Ramin, S.M.; Casey, B.; Wapner, R.J.; Varner, M.W.; Rouse, D.J.; Thorp, J.M., Jr.; et al. A multicenter, randomized trial of treatment for mild gestational diabetes. N. Engl. J. Med. 2009, 361, 1339–1348. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. ACOG Committee opinion no. 549: Obesity in pregnancy. Obstet. Gynecol. 2013, 121, 213–217. [Google Scholar]
- Wang, D.; Hong, Y.; Zhu, L.; Wang, X.; Lv, Q.; Zhou, Q.; Ruan, M.; Chen, C. Risk factors and outcomes of macrosomia in China: A multicentric survey based on birth data. J. Matern. Neonatal Med. 2017, 30, 623–627. [Google Scholar] [CrossRef]
- Vidarsdottir, H.; Geirsson, R.T.; Hardardottir, H.; Valdimarsdottir, U.; Dagbjartsson, A. Obstetric and neonatal risks among extremely macrosomic babies and their mothers. Am. J. Obstet. Gynecol. 2011, 204, 423.e1–423.e6. [Google Scholar] [CrossRef]
- Barber, E.L.; Lundsberg, L.S.; Belanger, K.; Pettker, C.M.; Funai, E.F.; Illuzzi, J.L. Indications Contributing to the Increasing Cesarean Delivery Rate. Obstet. Gynecol. 2011, 118, 29–38. [Google Scholar] [CrossRef]
- Li, G.; Kong, L.; Li, Z.; Zhang, L.; Fan, L.; Zou, L.; Chen, Y.; Ruan, Y.; Wang, X.; Zhang, W. Prevalence of Macrosomia and Its Risk Factors in China: A Multicentre Survey Based on Birth Data Involving 101 723 Singleton Term Infants. Paediatr. Périnat. Epidemiol. 2014, 28, 345–350. [Google Scholar] [CrossRef]
- Freeman, D.J. Effects of maternal obesity on fetal growth and body composition: Implications for programming and future health. Semin. Fetal Neonatal Med. 2010, 15, 113–118. [Google Scholar] [CrossRef]
- Cnattingius, S.; Villamor, E.; Lagerros, Y.T.; Wikström, A.-K.; Granath, F. High birth weight and obesity—A vicious circle across generations. Int. J. Obes. 2011, 36, 1320–1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, J. Weight and length at birth of infants of diabetic mothers. Eur. J. Endocrinol. 1954, 16, 330–342. [Google Scholar] [CrossRef] [PubMed]
- Ricart, W.; Lopez, J.; Mozas, J.; Pericot, A.; Sancho, M.A.; Gonzalez, N.; Balsells, M.; Luna, R.; Cortázar, A.; Navarro, P.; et al. Body mass index has a greater impact on pregnancy outcomes than gestational hyperglycaemia. Diabetology 2005, 48, 1736–1742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, E.A. Diagnosing gestational diabetes. Diabetologia 2011, 54, 480–486. [Google Scholar] [CrossRef] [Green Version]
- Torloni, M.R.; Betrán, A.P.; Horta, B.L.; Nakamura, M.U.; Atallah, A.N.; Moron, A.; Valente, O. Prepregnancy BMI and the risk of gestational diabetes: A systematic review of the literature with meta-analysis. Obes. Rev. 2009, 10, 194–203. [Google Scholar] [CrossRef]
- Li, G.; Wei, T.; Ni, W.; Zhang, A.; Zhang, J.; Xing, Y.; Xing, Q. Incidence and Risk Factors of Gestational Diabetes Mellitus: A Prospective Cohort Study in Qingdao, China. Front. Endocrinol. 2020, 11, 636. [Google Scholar] [CrossRef]
- Kondracki, A.J.; Valente, M.J.; Ibrahimou, B.; Bursac, Z. Risk of large for gestational age births at early, full and late term in relation to pre-pregnancy body mass index: Mediation by gestational diabetes status. Paediatr. Périnat. Epidemiol. 2021. [Google Scholar] [CrossRef]
- Ding, P.; VanderWeele, T.J. Sensitivity Analysis without Assumptions. Epidemiology 2016, 27, 368–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondracki, A.J. Low birthweight in term singletons mediates the association between maternal smoking intensity exposure status and immediate neonatal intensive care unit admission: The E-value assessment. BMC Pregnancy Childbirth 2020, 20, 341. [Google Scholar] [CrossRef]
- VanderWeele, T.J.; Ding, P. Sensitivity Analysis in Observational Research: Introducing the E-Value. Ann. Intern. Med. 2017, 167, 268–274. [Google Scholar] [CrossRef]
- Carey, J.C.; Klebanoff, M.A.; Hauth, J.C.; Hillier, S.L.; Thom, E.A.; Ernest, J.M.; Heine, R.P.; Nugent, R.P.; Fischer, M.L.; Leveno, K.J.; et al. Metronidazole to Prevent Preterm Delivery in Pregnant Women with Asymptomatic Bacterial Vaginosis. N. Engl. J. Med. 2000, 342, 534–540. [Google Scholar] [CrossRef]
- National Health Commission of the People’s Republic of China: Criteria of Weight for Adults. 2013. Available online: http://www.nhc.gov.cn/ewebeditor/uploadfile/2013/08/20130808135715967 (accessed on 1 February 2022).
- Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; Leiva, A.; Hod, M.; Kitzmiler, J.L.; et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Dai, R.-X.; He, X.-J.; Hu, C.-L. The Association between Advanced Maternal Age and Macrosomia: A Meta-Analysis. Child. Obes. 2019, 15, 149–155. [Google Scholar] [CrossRef]
- Al-Farsi, Y.M.; Brooks, D.R.; Werler, M.M.; Cabral, H.J.; Al-Shafaee, M.A.; Wallenburg, H.C. Effect of high parity on occurrence of some fetal growth indices: A cohort study. Int. J. Women’s Heal. 2012, 4, 289–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, A.K.; Rai, M.; Rehkopf, D.H.; Abrams, B. Educational attainment and obesity: A systematic review. Obes. Rev. 2013, 14, 989–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Uitert, E.M.; van der Elst-Otte, N.; Wilbers, J.J.; Exalto, N.; Willemsen, S.P.; Eilers, P.H.; Koning, A.H.; Steegers, E.A.; Steegers-Theunissen, R.P. Periconception maternal characteristics and embryonic growth trajectories: The Rotterdam Predict study. Hum. Reprod. 2013, 28, 3188–3196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of Gestational Weight Gain With Maternal and Infant Outcomes: A Systematic Review and Meta-analysis. JAMA 2017, 317, 2207–2225. [Google Scholar] [CrossRef]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.L.; Boyle, J.A.; Harrison, C.L.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; et al. Gestational weight gain across continents and ethnicity: Systematic review and meta-analysis of maternal and infant outcomes in more than one million women. BMC Med. 2018, 16, 153. [Google Scholar] [CrossRef]
- Valeri, L.; VanderWeele, T.J. Mediation analysis allowing for exposure–mediator interactions and causal interpretation: Theoretical assumptions and implementation with SAS and SPSS macros. Psychol. Methods 2013, 18, 137–150. [Google Scholar] [CrossRef] [Green Version]
- Böhnke, J.R. Explanation in causal inference: Methods for mediation and interaction. Q. J. Exp. Psychol. (Hove) 2016, 69, 1243–1244. [Google Scholar] [CrossRef]
- Ananth, C.V. Proportion mediated in a causal mediation analysis: How useful is this measure? BJOG Int. J. Obstet. Gynaecol. 2019, 126, 983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ananth, C.V.; VanderWeele, T.J. Placental Abruption and Perinatal Mortality with Preterm Delivery as a Mediator: Disentangling Direct and Indirect Effects. Am. J. Epidemiol. 2011, 174, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Trinquart, L.; Erlinger, A.L.; Petersen, J.M.; Fox, M.; Galea, S. Applying the E Value to Assess the Robustness of Epidemiologic Fields of Inquiry to Unmeasured Confounding. Am. J. Epidemiol. 2019, 188, 1174–1180. [Google Scholar] [CrossRef]
- Babu, G.R.; Deepa, R.; Lewis, M.G.; Lobo, E.; Krishnan, A.; Ana, Y.; Katon, J.G.; Enquobahrie, D.A.; Arah, O.A.; Kinra, S.; et al. Do Gestational Obesity and Gestational Diabetes Have an Independent Effect on Neonatal Adiposity? Results of Mediation Analysis from a Cohort Study in South India. Clin. Epidemiol. 2019, 11, 1067–1080. [Google Scholar] [CrossRef] [Green Version]
- Gibson, K.S.; Stetzer, B.; Catalano, P.M.; Myers, S.A. Comparison of 2- and 3-Dimensional Sonography for Estimation of Birth Weight and Neonatal Adiposity in the Setting of Suspected Fetal Macrosomia. J. Ultrasound Med. 2016, 35, 1123–1129. [Google Scholar] [CrossRef]
- Sovio, U.; Murphy, H.R.; Smith, G.C. Accelerated Fetal Growth Prior to Diagnosis of Gestational Diabetes Mellitus: A Prospective Cohort Study of Nulliparous Women. Diabetes Care 2016, 39, 982–987. [Google Scholar] [CrossRef] [Green Version]
- Brand, J.S.; West, J.; Tuffnell, D.; Bird, P.K.; Wright, J.; Tilling, K.; Lawlor, D.A. Gestational diabetes and ultrasound-assessed fetal growth in South Asian and White European women: Findings from a prospective pregnancy cohort. BMC Med. 2018, 16, 203. [Google Scholar] [CrossRef]
- Macaulay, S.; Munthali, R.J.; Dunger, D.B.; Norris, S.A. The effects of gestational diabetes mellitus on fetal growth and neonatal birth measures in an African cohort. Diabet. Med. 2018, 35, 1425–1433. [Google Scholar] [CrossRef]
- Kim, S.Y.; Sharma, A.J.; Sappenfield, W.; Wilson, H.G.; Salihu, H.M. Association of Maternal Body Mass Index, Excessive Weight Gain, and Gestational Diabetes Mellitus with Large-for-Gestational-Age Births. Obstet. Gynecol. 2014, 123, 737–744. [Google Scholar] [CrossRef]
- Li, M.; Hinkle, S.N.; Grantz, K.L.; Kim, S.; Grewal, J.; Grobman, W.A.; Skupski, D.W.; Newman, R.B.; Chien, E.K.; Sciscione, A.; et al. Glycaemic status during pregnancy and longitudinal measures of fetal growth in a multi-racial US population: A prospective cohort study. Lancet Diabetes Endocrinol. 2020, 8, 292–300. [Google Scholar] [CrossRef]
- Chiefari, E.; Quaresima, P.; Visconti, F.; Mirabelli, M.; Brunetti, A. Gestational diabetes and fetal overgrowth: Time to rethink screening guidelines. Lancet Diabetes Endocrinol. 2020, 8, 561–562. [Google Scholar] [CrossRef]
- Koivusalo, S.B.; Rönö, K.; Klemetti, M.M.; Roine, R.P.; Lindström, J.; Erkkola, M.; Kaaja, R.J.; Pöyhönen-Alho, M.; Tiitinen, A.; Huvinen, E.; et al. Gestational Diabetes Mellitus Can Be Prevented by Lifestyle Intervention: The Finnish Gestational Diabetes Prevention Study (RADIEL): A Randomized Controlled Trial. Diabetes Care 2016, 39, 24–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.; Tobias, D.K.; Chavarro, J.; Bao, W.; Wang, D.; Ley, S.; Hu, F.B. Adherence to healthy lifestyle and risk of gestational diabetes mellitus: Prospective cohort study. BMJ 2014, 349, g5450. [Google Scholar] [CrossRef] [Green Version]
- Grivell, R.M.; Yelland, L.N.; Deussen, A.R.; Crowther, C.A.; Dodd, J. Antenatal dietary and lifestyle advice for women who are overweight or obese and the effect on fetal growth and adiposity: The LIMIT randomised trial. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 233–243. [Google Scholar] [CrossRef]
- Goossens, G.H. The Metabolic Phenotype in Obesity: Fat Mass, Body Fat Distribution, and Adipose Tissue Function. Obes. Facts 2017, 10, 207–215. [Google Scholar] [CrossRef]
- Son, G.H.; Kwon, J.Y.; Kim, Y.H.; Park, Y.W. Maternal serum triglycerides as predictive factors for large-for-gestational age newborns in women with gestational diabetes mellitus. Acta Obstet. Gynecol. Scand. 2010, 89, 700–704. [Google Scholar] [CrossRef]
- Tsai, P.J.; Davis, J.; Bryant-Greenwood, G. Systemic and placental leptin and its receptors in pregnancies associated with obesity. Reprod. Sci. 2015, 22, 189–197. [Google Scholar] [CrossRef] [Green Version]
- Atègbo, J.-M.; Grissa, O.; Yessoufou, A.; Hichami, A.; Dramane, K.L.; Moutairou, K.; Miled, A.; Grissa, A.; Jerbi, M.; Tabka, Z.; et al. Modulation of Adipokines and Cytokines in Gestational Diabetes and Macrosomia. J. Clin. Endocrinol. Metab. 2006, 91, 4137–4143. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Maternal and Infant Characteristics | Total Births n (%) | GDM n (%) | Macrosomia n (%) | LGA n (%) |
|---|---|---|---|---|
| 34,104 | 5430 (15.9%) | 1374 (4.0%) | 3359 (9.9%) | |
| Pre-pregnancy BMI (kg/m2) | ||||
| Underweight (<18.5) | 4920 (14.4) | 448 (8.3) | 122 (8.9) | 315 (9.4) |
| Normal (18.5–23.9) | 23,925 (70.2) | 3696 (68.1) | 888 (64.6) | 2300 (68.5) |
| Overweight (24.0–27.9) | 4334 (12.7) | 1002 (18.5) | 230 (16.7) | 538 (16.0) |
| Obese (≥28.0) | 925 (2.7) | 284 (5.2) | 134 (9.8) | 206 (6.1) |
| Age at pregnancy onset | ||||
| <25 | 1769 (5.2) | 126 (2.3) | 78 (5.7) | 151 (4.5) |
| 25–29 | 11,873 (34.8) | 1412 (26.0) | 472 (34.4) | 1266 (37.7) |
| 30–34 | 12,803 (37.5) | 2168 (39.9) | 532 (38.7) | 1246 (37.1) |
| ≥35 | 7659 (22.5) | 1724 (31.7) | 292 (21.3) | 696 (20.7) |
| Education | ||||
| High school or less | 12,242 (35.9) | 1865 (34.3) | 470 (34.2) | 1109 (33.0) |
| Some college | 17,351 (50.9) | 2877 (53.0) | 722 (52.5) | 1820 (54.2) |
| Bachelor’s or higher | 4511 (13.2) | 688 (12.7) | 182 (13.2) | 430 (12.8) |
| Parity | ||||
| Primipara | 16,446 (48.2) | 2486 (45.8) | 653 (47.5) | 1707 (50.8) |
| Multipara | 17,658 (51.8) | 2944 (54.2) | 721 (52.5) | 1652 (49.2) |
| Infant sex | ||||
| Male | 17,953 (52.6) | 2743 (50.5) | 883 (64.3) | 2139 (63.7) |
| Female | 16,151 (47.4) | 2687 (49.5) | 491 (35.7) | 1220 (36.3) |
| Pre-Pregnancy BMI (kg/m2) | GDM % (95% CI) | Macrosomia % (95% CI) | LGA % (95% CI) |
|---|---|---|---|
| Total | 9.8 (9.5–10.2) | 4.0 (3.8–4.2) | 15.9 (15.5–16.3) |
| Underweight (<18.5) | 6.4 (5.7–7.1) | 2.5 (2.0–2.9) | 9.1 (8.3–9.9) |
| Normal (18.5–23.9) | 9.6 (9.2–10.0) | 3.7 (3.5–4.0) | 15.4 (15.0–15.9) |
| Overweight (24.0–27.9) | 12.4 (11.4–13.4) | 5.3 (4.6–6.0) | 23.1 (21.9–24.4) |
| Obese (≥28.0) | 22.3 (19.6–25.0) | 14.5 (12.2–16.8) | 30.7 (27.7–33.7) |
| Pre-Pregnancy BMI (kg/m2) | Total Effect | Natural Direct Effect | Natural Indirect Effect | Path A | Path B | Proportion Mediated |
|---|---|---|---|---|---|---|
| aRRTE (95% CI) | aRRNDE (95% CI) | aRRNIE (95% CI) | aRR (95% CI) | aRR (95% CI) | % | |
| Adjusted risk ratio of fetal macrosomia | ||||||
| Normal (18.5–23.9) | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) | - |
| Underweight (<18.5) | 0.56 (0.49–0.64) | 0.66 (0.54–0.79) | 0.86 (0.78–0.93) | 0.62 (0.56–0.69) | 1.39 (1.17–1.63) | 21.4 |
| Overweight (24.0–27.9) | 1.75 (1.56–1.96) | 1.40 (1.20–1.62) | 1.25 (1.16–1.36) | 1.60 (1.48–1.74) | 1.61 (1.39–1.85) | 46.7 |
| Obese (≥28.0) | 6.18 (5.26–7.26) | 4.10 (3.35–4.99) | 1.51 (1.31–1.76) | 2.34 (2.02–2.71) | 1.62 (1.39–1.88) | 40.3 |
| Adjusted risk ratio of LGA | ||||||
| Normal (18.5–23.9) | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) | - |
| Underweight (<18.5) | 0.57 (0.52–0.63) | 0.62 (0.55–0.70) | 0.92 (0.87–0.97) | 0.62 (0.56–0.69) | 1.19 (1.07–1.33) | 11.5 |
| Overweight (24.0–27.9) | 1.49 (1.37–1.62) | 1.34 (1.21–1.49) | 1.11 (1.05–1.17) | 1.60 (1.48–1.74) | 1.24 (1.12–1.37) | 30.2 |
| Obese (≥28.0) | 3.44 (3.02–3.92) | 2.63 (2.23–3.09) | 1.31 (1.19–1.46) | 2.34 (2.02–2.71) | 1.37 (1.23–1.52) | 33.3 |
| Pre-Pregnancy BMI (kg/m2) | Natural Direct Effect | Natural Indirect Effect | ||
|---|---|---|---|---|
| Adjusted Risk Ratio | Upper/Lower Confidence Limit | Adjusted Risk Ratio | Upper/Lower Confidence Limit | |
| Adjusted risk ratio of fetal macrosomia | ||||
| Underweight (<18.5) | 2.40 | Upper 1.85 | 1.60 | Upper 1.36 |
| Overweight (24.0–27.9) | 2.15 | Lower 1.69 | 1.81 | Lower 1.59 |
| Obese (≥28.0) | 7.67 | Lower 6.16 | 2.39 | Lower 1.95 |
| Adjusted risk ratio of LGA | ||||
| Underweight (<18.5) | 2.61 | Upper 2.21 | 1.39 | Upper 1.21 |
| Overweight (24.0–27.9) | 2.01 | Lower 1.71 | 1.46 | Lower 1.28 |
| Obese (≥28.0) | 4.70 | Lower 3.89 | 1.95 | Lower 1.67 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, X.; Shu, J.; Zhang, S.; Chen, L.; Diao, J.; Li, J.; Li, Y.; Wei, J.; Liu, Y.; Sun, M.; et al. Pre-Pregnancy Body Mass Index and Risk of Macrosomia and Large for Gestational Age Births with Gestational Diabetes Mellitus as a Mediator: A Prospective Cohort Study in Central China. Nutrients 2022, 14, 1072. https://doi.org/10.3390/nu14051072
Song X, Shu J, Zhang S, Chen L, Diao J, Li J, Li Y, Wei J, Liu Y, Sun M, et al. Pre-Pregnancy Body Mass Index and Risk of Macrosomia and Large for Gestational Age Births with Gestational Diabetes Mellitus as a Mediator: A Prospective Cohort Study in Central China. Nutrients. 2022; 14(5):1072. https://doi.org/10.3390/nu14051072
Chicago/Turabian StyleSong, Xinli, Jing Shu, Senmao Zhang, Letao Chen, Jingyi Diao, Jinqi Li, Yihuan Li, Jianhui Wei, Yiping Liu, Mengting Sun, and et al. 2022. "Pre-Pregnancy Body Mass Index and Risk of Macrosomia and Large for Gestational Age Births with Gestational Diabetes Mellitus as a Mediator: A Prospective Cohort Study in Central China" Nutrients 14, no. 5: 1072. https://doi.org/10.3390/nu14051072
APA StyleSong, X., Shu, J., Zhang, S., Chen, L., Diao, J., Li, J., Li, Y., Wei, J., Liu, Y., Sun, M., Wang, T., & Qin, J. (2022). Pre-Pregnancy Body Mass Index and Risk of Macrosomia and Large for Gestational Age Births with Gestational Diabetes Mellitus as a Mediator: A Prospective Cohort Study in Central China. Nutrients, 14(5), 1072. https://doi.org/10.3390/nu14051072