
Early Nutritional Intervention to Promote Healthy Eating Habits in Pediatric Oncology: A Feasibility Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Framework and Ethics
2.2. Participants
2.3. Nutritional Intervention
2.4. Participants’ Socio-Demographic and Cancer-Related Characteristics
2.5. Assessment of Nutritional Status and Vitamin D
2.6. Evaluation of Study Feasibility
2.7. Assessment of Dietary Intakes
2.8. Data Analysis
3. Results
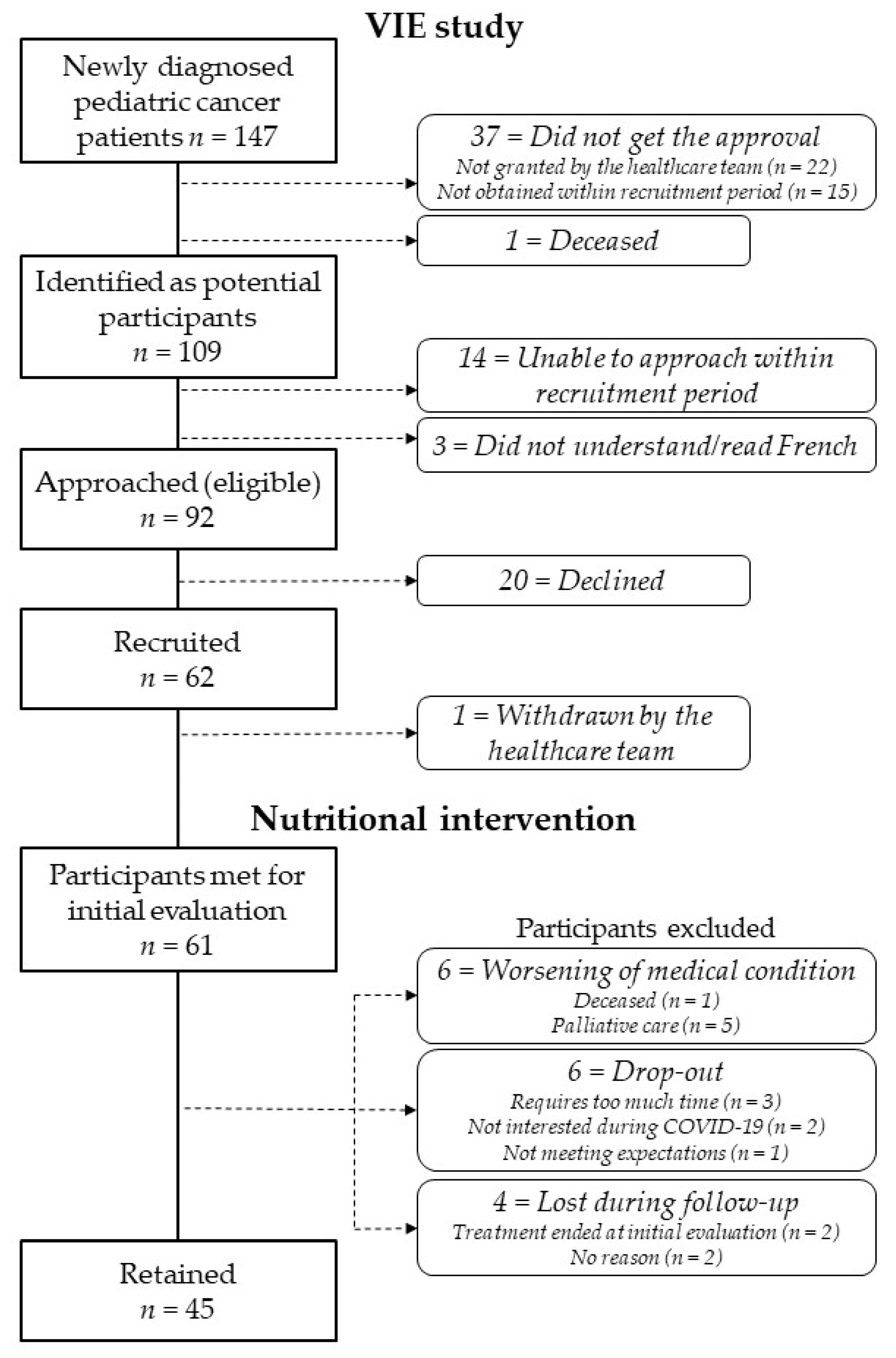
3.1. Recruitment and Description of the Cohort
3.2. Feasibility of the Intervention
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ellison, L.F.; Xie, L.; Sung, L. Trends in paediatric cancer survival in Canada, 1992 to 2017. Health Rep. 2021, 32, 3–15. [Google Scholar] [CrossRef]
- De, P.; Ellison, L.F.; Barr, R.D.; Semenciw, R.; Marrett, L.D.; Weir, H.K.; Dryer, D.; Grunfeld, E. Canadian adolescents and young adults with cancer: Opportunity to improve coordination and level of care. Can. Med. Assoc. 2011, 183, E187–E194. [Google Scholar] [CrossRef] [Green Version]
- Oeffinger, K.C.; Mertens, A.C.; Sklar, C.A.; Kawashima, T.; Hudson, M.M.; Meadows, A.T.; Friedman, D.L.; Marina, N.; Hobbie, W.; Kadan-Lottick, N.S.; et al. Chronic health conditions in adult survivors of childhood cancer. New Engl. J. Med. 2006, 355, 1572–1582. [Google Scholar] [CrossRef]
- Hudson, M.M.; Mulrooney, D.A.; Bowers, D.C.; Sklar, C.A.; Green, D.M.; Donaldson, S.S.; Oeffinger, K.C.; Neglia, J.P.; Meadows, A.T.; Robison, L.L. High-risk populations identified in Childhood Cancer Survivor Study investigations: Implications for risk-based surveillance. J. Clin. Oncol. 2009, 27, 2405–2414. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, K.E.; Derdak, J.; Bernstein, D.; Reynolds, J.C.; Avila, N.A.; Gerber, L.; Steinberg, S.M.; Chrousos, G.; Mackall, C.L.; Mansky, P.J. Metabolic syndrome traits in long-term survivors of pediatric sarcoma. Pediatr. Blood Cancer 2008, 50, 341–346. [Google Scholar] [CrossRef]
- Levy, E.; Samoilenko, M.; Morel, S.; England, J.; Amre, D.; Bertout, L.; Drouin, S.; Laverdière, C.; Krajinovic, M.; Sinnett, D.; et al. Cardiometabolic Risk Factors in Childhood, Adolescent and Young Adult Survivors of Acute Lymphoblastic Leukemia—A Petale Cohort. Sci. Rep. 2017, 7, 17684. [Google Scholar] [CrossRef] [Green Version]
- Faber, J.; Wingerter, A.; Neu, M.A.; Henninger, N.; Eckerle, S.; Münzel, T.; Lackner, K.J.; Beutel, M.E.; Blettner, M.; Rathmann, W.; et al. Burden of cardiovascular risk factors and cardiovascular disease in childhood cancer survivors: Data from the German CVSS-study. Eur. Heart J. 2018, 39, 1555–1562. [Google Scholar] [CrossRef]
- De Ferranti, S.D.; Steinberger, J.; Ameduri, R.; Baker, A.; Gooding, H.; Kelly, A.S.; Mietus-Snyder, M.; Mitsnefes, M.M.; Peterson, A.L.; St-Pierre, J.; et al. Cardiovascular Risk Reduction in High-Risk Pediatric Patients: A Scientific Statement From the American Heart Association. Circulation 2019, 139, e603–e634. [Google Scholar] [CrossRef] [PubMed]
- Children’s Oncology Group. Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers; Version 5.0; Children’s Oncology Group: Monrovia, CA, USA.
- Tonorezos, E.S.; Robien, K.; Eshelman-Kent, D.; Moskowitz, C.S.; Church, T.S.; Ross, R.; Oeffinger, K.C. Contribution of diet and physical activity to metabolic parameters among survivors of childhood leukemia. Cancer Causes Control 2013, 24, 313–321. [Google Scholar] [CrossRef] [Green Version]
- Landy, D.C.; Lipsitz, S.R.; Kurtz, J.M.; Hinkle, A.S.; Constine, L.S.; Adams, M.J.; Lipshultz, S.E.; Miller, T.L. Dietary quality, caloric intake, and adiposity of childhood cancer survivors and their siblings: An analysis from the cardiac risk factors in childhood cancer survivors study. Nutr. Cancer 2013, 65, 547–555. [Google Scholar] [CrossRef]
- Bérard, S.; Morel, S.; Teasdale, E.; Shivappa, N.; Hebert, J.R.; Laverdière, C.; Sinnett, D.; Levy, E.; Marcil, V. Diet Quality Is Associated with Cardiometabolic Outcomes in Survivors of Childhood Leukemia. Nutrients 2020, 12, 2137. [Google Scholar] [CrossRef] [PubMed]
- Robinson, D.L.; Loman, D.G.; Balakas, K.; Flowers, M. Nutritional screening and early intervention in children, adolescents, and young adults with cancer. J. Pediatr. Oncol. Nurs. 2012, 29, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Sacks, N.; Wallace, E.; Desai, S.; Prasad, V.K.; Henry, D.; Guzikowski, V.; Carney, L.N.; Wright, B.B.; Rheingold, S. Oncology, Hematopoietic Transplant, and Survivorship. In The A.S.P.E.N. Pediatric Nutrition Support Core Curriculum; Corkins, M.R., Ed.; American Society for Parenteral and Enteral Nutrition: Silver Spring, MD, USA, 2010; pp. 349–377. [Google Scholar]
- Co-Reyes, E.; Li, R.; Huh, W.; Chandra, J. Malnutrition and obesity in pediatric oncology patients: Causes, consequences, and interventions. Pediatr. Blood Cancer 2012, 59, 1160–1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, E.; Hopkins, M.; Arbuckle, L.; Williams, N.; Forsythe, L.; Bujkiewicz, S.; Pizer, B.; Estlin, E.; Picton, S. Nutritional problems in children treated for medulloblastoma: Implications for enteral nutrition support. Pediatr. Blood Cancer 2009, 53, 570–575. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, G.; Shemesh, E.; Frenkel, T.; Jacobson, J.M.; Toren, A. Abnormal body mass index at diagnosis in patients with Ewing sarcoma is associated with inferior tumor necrosis. Pediatr. Blood Cancer 2015, 62, 1892–1896. [Google Scholar] [CrossRef] [PubMed]
- Brinksma, A.; Roodbol, P.F.; Sulkers, E.; Kamps, W.A.; de Bont, E.S.; Boot, A.M.; Burgerhof, J.G.; Tamminga, R.Y.; Tissing, W.J. Changes in nutritional status in childhood cancer patients: A prospective cohort study. Clin. Nutr. 2015, 34, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Arpaci, T.; Toruner, E.K.; Altay, N. Assessment of Nutritional Problems in Pediatric Patients with Cancer and the Information Needs of Their Parents: A Parental Perspective. Asia Pac. J. Oncol. Nurs. 2018, 5, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Halton, J.M.; Nazir, D.J.; McQueen, M.J.; Barr, R.D. Blood lipid profiles in children with acute lymphoblastic leukemia. Cancer 1998, 83, 379–384. [Google Scholar] [CrossRef]
- Moschovi, M.; Trimis, G.; Apostolakou, F.; Papassotiriou, I.; Tzortzatou-Stathopoulou, F. Serum lipid alterations in acute lymphoblastic leukemia of childhood. J. Pediatr. Hematol. Oncol. 2004, 26, 289–293. [Google Scholar] [CrossRef]
- Warris, L.T.; van den Akker, E.L.; Bierings, M.B.; van den Bos, C.; Zwaan, C.M.; Sassen, S.D.; Tissing, W.J.; Veening, M.A.; Pieters, R.; van den Heuvel-Eibrink, M.M. Acute Activation of Metabolic Syndrome Components in Pediatric Acute Lymphoblastic Leukemia Patients Treated with Dexamethasone. PLoS ONE 2016, 11, e0158225. [Google Scholar] [CrossRef] [Green Version]
- Esbenshade, A.J.; Simmons, J.H.; Koyama, T.; Koehler, E.; Whitlock, J.A.; Friedman, D.L. Body mass index and blood pressure changes over the course of treatment of pediatric acute lymphoblastic leukemia. Pediatr. Blood Cancer 2011, 56, 372–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hingorani, P.; Seidel, K.; Krailo, M.; Mascarenhas, L.; Meyers, P.; Marina, N.; Conrad, E.U.; Hawkins, D.S. Body mass index (BMI) at diagnosis is associated with surgical wound complications in patients with localized osteosarcoma: A report from the Children’s Oncology Group. Pediatr. Blood Cancer 2011, 57, 939–942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egnell, C.; Ranta, S.; Banerjee, J.; Merker, A.; Niinimäki, R.; Lund, B.; Mogensen, P.R.; Jonsson, Ó.G.; Vaitkeviciene, G.; Lepik, K.; et al. Impact of body mass index on relapse in children with acute lymphoblastic leukemia treated according to Nordic treatment protocols. Eur. J. Haematol. 2020, 105, 797–807. [Google Scholar] [CrossRef] [PubMed]
- van Santen, H.M.; Geskus, R.B.; Raemaekers, S.; van Trotsenburg, A.S.P.; Vulsma, T.; van der Pal, H.J.H.; Caron, H.N.; Kremer, L.C.M. Changes in body mass index in long-term childhood cancer survivors. Cancer 2015, 121, 4197–4204. [Google Scholar] [CrossRef] [Green Version]
- Paul, S.; Pascal, A.; Yves, B.; Camille, V.; Claire, O.; Audrey, C.; Dominique, P.; Marilyne, P.; Stéphane, D.; Justyna, K.; et al. Metabolic syndrome in long-term survivors of childhood acute leukemia treated without hematopoietic stem cell transplantation: An L.E.A. study. Haematologica 2016, 101, 1603–1610. [Google Scholar] [CrossRef]
- Schadler, K.L.; Kleinerman, E.S.; Chandra, J. Diet and exercise interventions for pediatric cancer patients during therapy: Tipping the scales for better outcomes. Pediatr. Res. 2018, 8.83, 50–56. [Google Scholar] [CrossRef]
- Zhang, F.F.; Kelly, M.J.; Must, A. Early Nutrition and Physical Activity Interventions in Childhood Cancer Survivors. Curr. Obes. Rep. 2017, 6, 168–177. [Google Scholar] [CrossRef]
- Stern, M.; Lamanna, J.; Russell, C.; Ewing, L.; Thompson, A.; Trapp, S.; Bitsko, M.; Mazzeo, S. Adaptation of an obesity intervention program for pediatric cancer survivors (NOURISH-T). Clin. Pract. Pediatr. Psychol. 2013, 1, 264–275. [Google Scholar] [CrossRef]
- Beaulieu-Gagnon, S.; Bélanger, V.; Marcil, V. Food habits during treatment of childhood cancer: A critical review. Nutr. Res. Rev. 2019, 32, 265–281. [Google Scholar] [CrossRef]
- Hill, R.; Hamby, T.; Bashore, L.; Rapisand, S.; Galipp, K.; Heym, K.; Bowman, W.P. Early Nutrition Intervention Attenuates Weight Gain for Pediatric Acute Lymphoblastic Leukemia Patients in Maintenance Therapy. J. Pediatr. Hematol. Oncol. 2018, 40, 104–110. [Google Scholar] [CrossRef]
- Zhang, F.F.; Kelly, M.; Du, M.; Welch, J.G.; Santacruz, N.; Rhoades, J.; Kamins, C.L.; Dreyer, Z.; Scheurer, M.E. Early Lifestyle Intervention for Obesity Prevention in Pediatric Survivors of Acute Lymphoblastic Leukemia. Nutrients 2019, 11, 2631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orsmond, G.I.; Cohn, E.S. The Distinctive Features of a Feasibility Study: Objectives and Guiding Questions. OTJR Occup. Particip. Health 2015, 35, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Thabane, L.; Ma, J.; Chu, R.; Cheng, J.; Ismaila, A.; Rios, L.P.; Robson, R.; Thabane, M.; Giangregorio, L.; Goldsmith, C.H. A tutorial on pilot studies: The what, why and how. BMC Med. Res. Methodol. 2010, 10, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arain, M.; Campbell, M.J.; Cooper, C.L.; Lancaster, G.A. What is a pilot or feasibility study? A review of current practice and editorial policy. BMC Med. Res. Methodol. 2010, 10, 67. [Google Scholar] [CrossRef] [Green Version]
- Caru, M.; Duhamel, G.; Marcil, V.; Sultan, S.; Meloche, C.; Bouchard, I.; Drouin, S.; Bertout, L.; Laverdiere, C.; Sinnett, D.; et al. The VIE study: Feasibility of a physical activity intervention in a multidisciplinary program in children with cancer. Support. Care Cancer 2020, 28, 2627–2636. [Google Scholar] [CrossRef]
- Ogez, D.; Bourque, C.J.; Péloquin, K.; Ribeiro, R.; Bertout, L.; Curnier, D.; Drouin, S.; Laverdière, C.; Marcil, V.; Rondeau, É.; et al. Definition and improvement of the concept and tools of a psychosocial intervention program for parents in pediatric oncology: A mixed-methods feasibility study conducted with parents and healthcare professionals. Pilot Feasibility Stud. 2019, 5, 20. [Google Scholar] [CrossRef] [Green Version]
- Gibson, E.L.; Kreichauf, S.; Wildgruber, A.; Vögele, C.; Summerbell, C.D.; Nixon, C.; Moore, H.; Douthwaite, W.; Manios, Y. A narrative review of psychological and educational strategies applied to young children’s eating behaviours aimed at reducing obesity risk. Obes Rev. 2012, 13 (Suppl. S1), 85–95. [Google Scholar] [CrossRef]
- Birch, L.L.; Gunder, L.; Grimm-Thomas, K.; Laing, D.G. Infants’ consumption of a new food enhances acceptance of similar foods. Appetite 1998, 30, 283–295. [Google Scholar] [CrossRef]
- Fleming, C.A.; Cohen, J.; Murphy, A.; Wakefield, C.E.; Cohn, R.J.; Naumann, F.L. Parent feeding interactions and practices during childhood cancer treatment. A qualitative investigation. Appetite 2015, 89, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Jansen, E.; Mulkens, S.; Jansen, A. Do not eat the red food!: Prohibition of snacks leads to their relatively higher consumption in children. Appetite 2007, 49, 572–577. [Google Scholar] [CrossRef]
- Secker, D. Promoting optimal monitoring of child growth in Canada: Using the new WHO growth charts. Can. J. Diet. Pract. Res. 2010, 71, e1–e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodd, C.; Metzger, D.L.; Sharma, A. Extending World Health Organization weight-for-age reference curves to older children. BMC Pediatr. 2014, 14, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Must, A.; Anderson, S.E. Body mass index in children and adolescents: Considerations for population-based applications. Int. J. Obes. 2006, 30, 590–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Browne, E.K.; Zhou, Y.; Chemaitilly, W.; Panetta, J.C.; Ness, K.K.; Kaste, S.C.; Cheng, C.; Relling, M.V.; Pui, C.H.; Inaba, H. Changes in body mass index, height, and weight in children during and after therapy for acute lymphoblastic leukemia. Cancer 2018, 124, 4248–4259. [Google Scholar] [CrossRef]
- Munns, C.F.; Shaw, N.; Kiely, M.; Specker, B.L.; Thacher, T.D.; Ozono, K.; Michigami, T.; Tiosano, D.; Mughal, M.Z.; Mäkitie, O.; et al. Global Consensus Recommendations on Prevention and Management of Nutritional Rickets. J. Clin. Endocrinol. Metab. 2016, 101, 394–415. [Google Scholar] [CrossRef]
- Knox, E.; Glazebrook, C.; Randell, T.; Leighton, P.; Guo, B.; Greening, J.; Davies, E.B.; Amor, L.; Blake, H. SKIP (Supporting Kids with diabetes In Physical activity): Feasibility of a randomised controlled trial of a digital intervention for 9-12 year olds with type 1 diabetes mellitus. BMC Public Health 2019, 19, 371. [Google Scholar] [CrossRef] [Green Version]
- McPherson, A.C.; Biddiss, E.; Chen, L.; Church, P.T.; de Groot, J.F.; Keenan, S.; King, G.; Lui, T.; Maltais, D.B.; Mérette, C.; et al. Children and Teens in Charge of their Health (CATCH): A protocol for a feasibility randomised controlled trial of solution-focused coaching to foster healthy lifestyles in childhood disability. BMJ Open 2019, 9, e025119. [Google Scholar] [CrossRef]
- Fladeboe, K.M.; O’Donnell, M.B.; Barton, K.S.; Bradford, M.C.; Steineck, A.; Junkins, C.C.; Yi-Frazier, J.P.; Rosenberg, A.R. A novel combined resilience and advance care planning intervention for adolescents and young adults with advanced cancer: A feasibility and acceptability cohort study. Cancer 2021, 127, 4504–4511. [Google Scholar] [CrossRef]
- Blake, H.; Quirk, H.; Leighton, P.; Randell, T.; Greening, J.; Guo, B.; Glazebrook, C. Feasibility of an online intervention (STAK-D) to promote physical activity in children with type 1 diabetes: Protocol for a randomised controlled trial. Trials 2016, 17, 583. [Google Scholar] [CrossRef]
- Samaan, M.C.; Scheinemann, K.; Burrow, S.; Dillenburg, R.F.; Barr, R.D.; Wang, K.W.; Valencia, M.; Thabane, L. Recruitment feasibility to a cohort study of endocrine and metabolic health among survivors of childhood brain tumours: A report from the Canadian study of Determinants of Endometabolic Health in ChIlDrEn (CanDECIDE). BMJ Open 2014, 4, e005295. [Google Scholar] [CrossRef] [Green Version]
- Government of Canada. Dietary Reference Intakes Tables. Available online: https://www.canada.ca/content/dam/hc-sc/migration/hc-sc/fn-an/alt_formats/hpfb-dgpsa/pdf/nutrition/dri_tables-eng.pdf (accessed on 14 October 2021).
- Orgel, E.; Sposto, R.; Malvar, J.; Seibel, N.L.; Ladas, E.; Gaynon, P.S.; Freyer, D.R. Impact on survival and toxicity by duration of weight extremes during treatment for pediatric acute lymphoblastic leukemia: A report from the Children’s Oncology Group. J. Clin. Oncol 2014, 32, 1331–1337. [Google Scholar] [CrossRef] [PubMed]
- Joffe, L.; Dwyer, S.; Glade Bender, J.L.; Frazier, A.L.; Ladas, E.J. Nutritional status and clinical outcomes in pediatric patients with solid tumors: A systematic review of the literature. Semin. Oncol. 2019, 46, 48–56. [Google Scholar] [CrossRef]
- Loeffen, E.A.; Brinksma, A.; Miedema, K.G.; de Bock, G.H.; Tissing, W.J. Clinical implications of malnutrition in childhood cancer patients--infections and mortality. Support. Care Cancer 2015, 23, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Brinksma, A.; Sanderman, R.; Roodbol, P.F.; Sulkers, E.; Burgerhof, J.G.; de Bont, E.S.; Tissing, W.J. Malnutrition is associated with worse health-related quality of life in children with cancer. Support. Care Cancer 2015, 23, 3043–3052. [Google Scholar] [CrossRef] [Green Version]
- Moyer-Mileur, L.J.; Ransdell, L.; Bruggers, C.S. Fitness of children with standard-risk acute lymphoblastic leukemia during maintenance therapy: Response to a home-based exercise and nutrition program. J. Pediatr. Hematol. Oncol. 2009, 31, 259–266. [Google Scholar] [CrossRef]
- Birch, L.L.; Fisher, J.O. Development of eating behaviors among children and adolescents. Pediatrics 1998, 101, 539–549. [Google Scholar] [CrossRef]
- Green, R.; Horn, H.; Erickson, J.M. Eating Experiences of Children and Adolescents With Chemotherapy-Related Nausea and Mucositis. J. Pediatr. Hematol./Oncol. Nurs. 2010, 27, 209–216. [Google Scholar] [CrossRef]
- Williams, L.K.; McCarthy, M.C. Parent perceptions of managing child behavioural side-effects of cancer treatment: A qualitative study. Child. Care Health Dev. 2015, 41, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.F.; Rodday, A.M.; Kelly, M.J.; Must, A.; MacPherson, C.; Roberts, S.B.; Saltzman, E.; Parsons, S.K. Predictors of being overweight or obese in survivors of pediatric acute lymphoblastic leukemia (ALL). Pediatr. Blood Cancer 2014, 61, 1263–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, K.L.; Kern, K.D.; Chambers, T.M.; Lupo, P.J.; Kamdar, K.Y.; Scheurer, M.E.; Brown, A.L. Weight trends in a multiethnic cohort of pediatric acute lymphoblastic leukemia survivors: A longitudinal analysis. PLoS ONE 2019, 14, e0217932. [Google Scholar] [CrossRef]
- Folta, S.; Chang, W.; Hill, R.; Kelly, M.; Meagher, S.; Bowman, W.P.; Zhang, F.F. Parent and Health Care Provider Perceptions for Development of a Web-Based Weight Management Program for Survivors of Pediatric Acute Lymphoblastic Leukemia: A Mixed Methods Study. JMIR Cancer 2017, 3, 1. [Google Scholar] [CrossRef]
- Dolgin, M.J.; Phipps, S.; Fairclough, D.L.; Sahler, O.J.Z.; Askins, M.; Noll, R.B.; Butler, R.W.; Varni, J.W.; Katz, E.R. Trajectories of Adjustment in Mothers of Children with Newly Diagnosed Cancer: A Natural History Investigation. J. Pediatr. Psychol. 2007, 32, 771–782. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Donnella, H.; Knouse, P.; Raber, M.; Crawford, K.; Swartz, M.C.; Wu, J.; Liu, D.; Chandra, J. A randomized nutrition counseling intervention in pediatric leukemia patients receiving steroids results in reduced caloric intake. Pediatr. Blood Cancer 2017, 64, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Eldridge, S.M.; Lancaster, G.A.; Campbell, M.J.; Thabane, L.; Hopewell, S.; Coleman, C.L.; Bond, C.M. Defining Feasibility and Pilot Studies in Preparation for Randomised Controlled Trials: Development of a Conceptual Framework. PLoS ONE 2016, 11, e0150205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barr, R.D.; Ferrari, A.; Ries, L.; Whelan, J.; Bleyer, W.A. Cancer in Adolescents and Young Adults: A Narrative Review of the Current Status and a View of the Future. JAMA Pediatr. 2016, 170, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Lassi, Z.S.; Salam, R.A.; Das, J.K.; Wazny, K.; Bhutta, Z.A. An unfinished agenda on adolescent health: Opportunities for interventions. Semin. Perinatol. 2015, 39, 353–360. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Participants | |
|---|---|
| Sex, n (%) | n = 62 |
| Male | 32 (51.6) |
| Female | 30 (48.4) |
| Age at recruitment, year | n = 62 |
| Mean ± SD | 8.5 ± 5.1 |
| Median (min–max) | 7.4 (1.4–17.3) |
| Age category, n (%) | n = 62 |
| Preschoolers (<5 y.o.) | 22 (35.5) |
| Children (5 to 12 y.o.) | 22 (35.5) |
| Adolescents (≥13 y.o.) | 18 (29.0) |
| Marital status, n (%) | n = 53 |
| Married/common-law partners | 42 (79.2) |
| Separated/divorced/widower | 11 (20.8) |
| Parental education level, n (%) | n = 55 |
| Unfinished high school | 2 (3.6) |
| High school | 13 (23.6) |
| College | 9 (16.4) |
| University | 31 (56.4) |
| Approximated gross family income, n (%) | n = 51 |
| <$29,999 | 4 (7.8) |
| $30,000–$69,999 | 12 (23.5) |
| $70,000–$109,999 | 17 (33.3) |
| $110,000–$150,000 | 11 (21.6) |
| >$150,000 | 7 (13.7) |
| Cancer diagnosis, n (%) | n = 62 |
| Leukemia 1 | 29 (46.8) |
| Lymphoma 2 | 12 (19.4) |
| Sarcoma 3 | 10 (16.1) |
| Other 4 | 11 (17.7) |
| Cancer evolution, n (%) | n = 62 |
| Responders | 51 (82.3) |
| Non responders 5 | 11 (17.7) |
| BMI or W/L, z-score | n = 61 |
| Mean ± SD | 0.3 ± 1.1 |
| Median (min–max) | 0.1 (−1.9–2.8) |
| Nutritional status, n (%) | n = 61 |
| Normal | 47 (75.8) |
| Overweight/Obese | 15 (24.2) |
| Serum 25(OH)D, nmol/L | n = 52 |
| Mean ± SD | 59.8 ± 24.4 |
| Median (min–max) | 58.2 (22.0–168.0) |
| Vitamin D status, n (%) | n = 52 |
| Sufficiency | 36 (69.2) |
| Insufficiency | 13 (25.0) |
| Deficiency | 3 (5.8) |
| Participants | Retained | Excluded | ||
|---|---|---|---|---|
| n = 61 | n = 45 | n = 16 | p-Value | |
| Duration of the intervention, months | - | |||
| Mean ± SD | N/A | N/A | 4.6 ± 3.3 | |
| Median (min–max) | N/A | N/A | 4.9 (0–10.8) | |
| Time between diagnosis and initial evaluation, weeks | 0.34 | |||
| Mean ± SD | 13.2 ± 7.1 | 13.1 ± 7.7 | 13.7 ± 4.9 | |
| Median (min–max) | 11.9 (3.1–43.0) | 11.7 (3.1–43.0) | 12.4 (5.86–22.0) | |
| Engagement level 1, n (%) | n = 55 | n = 45 | n = 10 | <0.01 |
| Low | 9 (16.4) | 4 (8.9) | 5 (50.0) | |
| Moderate | 15 (27.3) | 15 (33.3) | 0 | |
| High | 31 (56.4) | 26 (57.8) | 5 (50.0) | |
| Participation in follow-up visits | ||||
| Number of follow-up visits completed, n | <0.001 | |||
| Mean ± SD | 3.2 ± 1.7 | 4.0 ± 1.1 | 1.2 ± 1.2 | |
| Median (min–max) | 4.0 (0–6.0) | 4.0 (2.0–6.0) | 1.0 (0–4.0) | |
| Rate 2, % | <0.001 | |||
| Mean ± SD | 53.8 ± 27.6 | 65.9 ± 18.5 | 19.8 ± 19.5 | |
| Median (min–max) | 66.7 (0–100) | 66.7 (33.3–100) | 16.7 (0–66.7) |
| Initial Evaluation | 2-Month Follow-Up | 4-Month Follow-Up | 6-Month Follow-up | 8-Month Follow-Up | 10-Month Follow-Up | 12-Month Follow-Up | All Visits | |
|---|---|---|---|---|---|---|---|---|
| Attendance | ||||||||
| Actual/ potential, n | 61/62 | 47/56 | 38/55 | 35/51 | 32/47 | 23/46 | 22/45 | 258/362 |
| Rate (%) | (98.4) | (83.9) | (69.1) | (68.6) | (68.0) | (50.0) | (48.9) | (71.3) |
| Completion rates, n (%) | ||||||||
| Study measures | (n = 61) | (n = 47) | (n = 38) | (n = 35) | (n = 32) | (n = 23) | (n = 22) | Mean (95% CI) |
| 3-day food record | 23 (37.7) | - | - | - | - | - | - | - |
| Blood sample | 55 (90.2) | - | - | - | - | - | - | - |
| 24H-R | 53 (86.9) | 42 (89.4) | 31 (81.6) | 28 (80.0) | 27 (84.4) | 20 (87.0) | 16 (72.7) | 83.1 (78.6–87.6) |
| BMI or W/L | 61 (100) | 45 (95.7) | 35 (92.1) | 34 (97.1) | 30 (93.8) | 22 (95.7) | 19 (86.4) | 94.4 (91.0–97.8) |
| WC | 20 (32.8) | 7 (14.9) | 3 (7.9) | 3 (8.6) | 3 (9.4) | 1 (4.4) | 7 (31.8) | 15.7 (6.3–25.1) |
| MUAC | 37 (60.7) | 19 (40.4) | 14 (36.8) | 8 (22.9) | 7 (21.9) | 5 (21.7) | 9 (40.9) | 35.0 (23.6–46.4) |
| TSFT | 29 (47.5) | 18 (38.3) | 11 (29.0) | 6 (17.1) | 7 (21.9) | 4 (17.4) | 7 (31.8) | 29.0 (20.0–38.0) |
| SSFT | 23 (37.7) | 14 (29.8) | 8 (21.1) | 4 (11.4) | 6 (18.8) | 1 (4.4) | 5 (22.7) | 20.8 (11.9–29.7) |
| Participation Level | ||||
|---|---|---|---|---|
| Low | Moderate | High | ||
| (0–1 visit) | (2–3 Visits) | (≥4 Visits) | ||
| n = 11 | n = 19 | n = 31 | p-Value | |
| Sex, n (%) | 0.40 | |||
| Male | 5 (45.5) | 8 (42.1) | 19 (61.3) | |
| Female | 6 (54.5) | 11 (57.9) | 12 (38.7) | |
| Age at recruitment, year | 0.36 | |||
| Mean ± SD | 9.7 ± 5.7 | 9.4 ± 5.2 | 7.4 ± 4.9 | |
| Median (min–max) | 8.9 (2.4–17.1) | 8.8 (1.9–16.3) | 5.2 (1.3–17.1) | |
| Age category, n (%) | 0.06 | |||
| Children (<13 y.o.) | 6 (54.5) | 11 (57.9) | 26 (83.9) | |
| Adolescents (≥13 y.o.) | 5 (45.5) | 8 (42.1) | 5 (16.1) | |
| Marital status, n (%) | n = 10 | n = 16 | n = 27 | 0.74 |
| Married/common-law partners | 9 (90.0) | 12 (75.0) | 21 (77.8) | |
| Separated/divorced/widower | 1 (9.1) | 4 (25.0) | 6 (22.2) | |
| Parental education level, n (%) | n = 10 | n = 16 | n = 29 | 0.86 |
| Unfinished high school/high school | 4 (40.0) | 4 (25.0) | 7 (24.1) | |
| College | 1 (10.0) | 2 (12.5) | 6 (20.7) | |
| University | 5 (50.0) | 10 (62.5) | 16 (55.2) | |
| Mean gross family revenue, n (%) | n = 9 | n = 14 | n = 28 | 0.08 |
| <$29,999 | 1 (11.1) | 1 (7.1) | 2 (7.1) | |
| $30,000–$69,999 | 1 (11.1) | 2 (14.3) | 9 (32.1) | |
| $70,000–$109,999 | 7 (77.8) | 3 (21.4) | 7 (25.0) | |
| $110,000–$150,000 | 1 (11.1) | 4 (28.6) | 7 (25.0) | |
| >$150,000 | 0 | 4 (28.6) | 3 (10.7) | |
| Diagnosis, n (%) | 0.31 | |||
| Leukemia | 3 (27.3) | 9 (47.4) | 16 (51.6) | |
| Lymphoma | 2 (18.2) | 4 (21.1) | 6 (19.4) | |
| Sarcoma | 2 (18.2) | 5 (26.3) | 3 (9.7) | |
| Other | 4 (36.4) | 1 (5.3) | 6 (19.4) | |
| BMI or W/L, z-score | 1.00 | |||
| Mean ± SD | 0.3 ± 1.1 | 0.3 ± 1.3 | 0.3 ± 1.1 | |
| Median (min–max) | −0.1 (−1.0–2.5) | −0.1 (−1.9–2.8) | 0.1 (−1.7–2.3) | |
| Nutritional status, n (%) | 0.92 | |||
| Normal | 9 (81.8) | 14 (73.7) | 25 (80.6) | |
| Overweight/Obese | 2 (18.2) | 5 (26.3) | 7 (19.4) | |
| Cancer evolution, n (%) | 0.68 | |||
| Responders | 8 (72.7) | 16 (84.2) | 26 (83.9) | |
| Non responders 1 | 3 (27.3) | 3 (15.8) | 5 (16.1) | |
| Engagement level 2, n (%) | n = 7 | n = 17 | n = 31 | 0.001 |
| Low | 5 (71.4) | 3 (17.6) | 1 (3.2) | |
| Moderate | 0 | 7 (41.2) | 8 (25.8) | |
| High | 2 (28.6) | 7 (41.2) | 22 (71.0) | |
| Participation Level | ||||
|---|---|---|---|---|
| Low | Moderate | High | ||
| (0–1 Visit) | (2–3 Visits) | (≥4 Visits) | ||
| n = 9 | n = 19 | n = 25 | p-Value | |
| Energy | ||||
| Kcal | ||||
| Mean (min–max) | 1976 (767–3040) | 1418 (224–2698) | 1702 (9–3751) | 0.22 |
| Median (IQR) | 2077 (1696–2522) | 1452 (842–2058) | 1508 (1075–2149) | |
| Kcal/kg | ||||
| Mean (min–max) | 77.3 (19.5–194.0) | 51.4 (4.9–115.1) | 64.8 (0.4–159.5) | 0.48 |
| Median (IQR) | 48.8 (39.5–112.3) | 51.9 (27.9–74.4) | 50.5 (35.2–86.1) | |
| Fat | ||||
| g/kg | ||||
| Mean (min–max) | 3.4 (0.9–8.6) | 2.0 (0.2–4.9) | 2.7 (0–8.7) | 0.40 |
| Median (IQR) | 2.1 (1.4–4.8) | 2.0 (0.8–2.7) | 2.2 (1.0–3.4) | |
| % Energy | ||||
| Mean (min–max) | 38.4 (27.5–49.4) | 35.2 (23.6–53.3) | 35.4 (2.3–56.1) | 0.50 |
| Median (IQR) | 38.0 (36.9–39.9) | 35.1 (29.5–40.0) | 37.4 (31.0–39.5) | |
| Protein | ||||
| g/kg | ||||
| Mean (min–max) | 2.7 (0.6–7.8) | 2.1 (0.1–4.2) | 2.8 (0–7.5) | 0.66 |
| Median (IQR) | 1.6 (1.2–3.7) | 2.5 (1.0–3.1) | 2.2 (1.4–4.1) | |
| % Energy | ||||
| Mean (min–max) | 13.5 (11.4–16.1) | 15.9 (5.0–20.3) | 16.7 (1.0–22.9) | 0.02 |
| Median (IQR) | 13.3 (12.8–14.2) | 16.0 (13.9–19.1) | 18.1 (13.7–19.3) | |
| % RDA | ||||
| Mean (min–max) | 273.1 (67.0–741.9) | 218.0 (7.2–440.8) | 289.0 (0–712.1) | 0.69 |
| Median (IQR) | 184.1 (144.4–354.6) | 267.1 (107.1–325.0) | 232.4 (146.8–404.7) | |
| Dietary fiber | ||||
| Energy-adjusted (g/1000 kcal) | ||||
| Mean (min–max) | 9.8 (3.1201321.3) | 8.2 (3.4–15.0) | 7.6 (0–18.0) | 0.50 |
| Median (IQR) | 9.2 (6.6–10.8) | 7.7 (6.2–10.2) | 7.4 (5.3–9.4) | |
| % AI | ||||
| Mean (min–max) | 88.9 (12.3–283.0) | 45.1 (5.9–92.8) | 43.9 (0–107.0) | 0.05 |
| Median (IQR) | 73.6 (58.8–83.7) | 50.5 (19.8–63.6) | 41.5 (32.5–56.7) | |
| Sodium | ||||
| Energy-adjusted (mg/1000 kcal) | ||||
| Mean (min–max) | 1305.7 (423.2–1976.1) | 1373.8 (551.5–2781.3) | 1609.4 (29.9–7390.6) | 0.81 |
| Median (IQR) | 1538.4 (954.7–1695.1) | 1273.7 (1031.7–1665.3) | 1484.3 (1118.7–1591.1) | |
| % UL | ||||
| Mean (min–max) | 129.4 (63.3–224.0) | 97.9 (12.0–240.8) | 133.0 (0–313.1) | 0.20 |
| Median (IQR) | 107.9 (71.2–178.5) | 79.4 (42.9–143.8) | 123.7 (80.2–165.5) | |
| Calcium | ||||
| Energy-adjusted (mg/1000 kcal) | ||||
| Mean (min–max) | 464.5 (129.6–1016.6) | 657.5 (65.1–1392.3) | 619.1 (44.9–1175.7) | 0.34 |
| Median (IQR) | 449.7 (285.1–536.5) | 637.7 (466.3–792.4) | 665.8 (276.1–875.5) | |
| % RDA | ||||
| Mean (min–max) | 101.1 (7.7–260.4) | 92.3 (2.5–224.6) | 103.0 (0–334.3) | 0.99 |
| Median (IQR) | 71.9 (58.7–124.8) | 93.2 (46.6–120.8) | 71.9 (40.0–177.2) | |
| Vitamin C | ||||
| Energy-adjusted (mg/1000 kcal) | ||||
| Mean (min–max) | 59.2 (0–132.9) | 46.6 (1.9–161.4) | 81.3 (0.3–390.5) | 0.56 |
| Median (IQR) | 68.3 (22.8–87.3) | 29.2 (14.0–64.9) | 58.2 (25.4–99.0) | |
| % RDA | ||||
| Mean (min–max) | 329.5 (0.1–772.6) | 251.0 (4.9–1379.9) | 414.0 (0.9–2132.1) | 0.52 |
| Median (IQR) | 275.4 (154.1–403.5) | 101.7 (30.9–289.8) | 220.5 (87.8–508.0) | |
| Vitamin D | ||||
| Energy-adjusted (μg/1000 kcal) | ||||
| Mean (min–max) | 2.6 (0.0–8.8) | 3.5 (0–10.6) | 3.9 (0–13.3) | 0.22 |
| Median (IQR) | 2.0 (1.6–2.5) | 2.8 (1.1–4.3) | 4.1 (1.6–4.9) | |
| % RDA | ||||
| Mean (min–max) | 33.4 (0–105.5) | 32.8 (0–79.8) | 38.9 (0–101.0) | 0.59 |
| Median (IQR) | 31.2 (8.0–39.5) | 22.6 (11.7–48.9) | 38.7 (22.3–55.3) |
| n = 21 Pairs | Difference 1 | |||
|---|---|---|---|---|
| Initial Evaluation | Post-Intervention | Mean (95% CI) | p-Value | |
| Energy | ||||
| Kcal | ||||
| Mean (min–max) | 1584 (9–3751) | 1822 (882–3386) | 299 (–236–833) | 0.25 |
| Median (IQR) | 1479 (1075–1900) | 1727 (1362–2071) | ||
| Kcal/kg | ||||
| Mean (min–max) | 61.4 (0.4–159.5) | 60.9 (17.9–120.4) | −0.4 (−17.2–16.4) | 0.79 |
| Median (IQR) | 51.9 (38.3–78.4) | 61.9 (41.0–78.0) | ||
| Fat | ||||
| g/kg | ||||
| Mean (min–max) | 2.7 (0–8.7) | 2.3 (0.6–5.7) | −0.5 (−1.5–0.5) | 0.73 |
| Median (IQR) | 2.2 (1.7–3.4) | 2.0 (1.3–3.1) | ||
| % Energy | ||||
| Mean (min–max) | 37.1 (2.3–56.1) | 33.2 (17.1–52.1) | −3.8 (−9.9–2.2) | 0.20 |
| Median (IQR) | 38.5 (33.6–39.5) | 28.7 (26.1–44.3) | ||
| Protein | ||||
| g/kg | ||||
| Mean (min–max) | 2.8 (0–7.5) | 2.7 (0.4–5.7) | −0.1 (−1.0–0.7) | 0.92 |
| Median (IQR) | 2.6 (1.5–3.3) | 2.6 (1.8–3.5) | ||
| % Energy | ||||
| Mean (min–max) | 16.8 (1.0–22.3) | 17.4 (9.3–42.5) | 0.6 (−3.4–4.6) | 0.87 |
| Median (IQR) | 18.9 (15.3–19.4) | 16.6 (14.2–18.9) | ||
| % RDA | ||||
| Mean (min–max) | 289.0 (0–712.1) | 281.9 (49.4–600.0) | −7.1 (−89.7–75.6) | 0.86 |
| Median (IQR) | 268.0 (165.5–346.6) | 282.1 (187.4–363.2) | ||
| Dietary fiber | ||||
| Energy–adjusted (g/1000 kcal) | ||||
| Mean (min–max) | 7.9 (0–18.0) | 7.2 (1.9–15.1) | −0.7 (−2.9–1.5) | 0.51 |
| Median (IQR) | 7.7 (5.9–9.9) | 7.4 (5.7–8.3) | ||
| % AI | ||||
| Mean (min–max) | 44.5 (0–92.8) | 48.1 (6.6–91.2) | 3.5 (−11.1–18.2) | 0.62 |
| Median (IQR) | 42.3 (32.5–57.5) | 47.9 (41.1–53.2) | ||
| Sodium | ||||
| Energy–adjusted (mg/1000 kcal) | ||||
| Mean (min–max) | 1612.5 (29.9–7390.6) | 1078.4 (727.7–1403.6) | −564.1 (−1193.1–64.9) | 0.03 |
| Median (IQR) | 1542.5 (1078.4–1665.6) | 1065.3 (950.7–1190.6) | ||
| % UL | ||||
| Mean (min–max) | 132.4 (0–313.1) | 100.1 (59.1–206.6) | −32.3 (−81.9–17.4) | 0.19 |
| Median (IQR) | 109.8 (74.9–165.5) | 93.5 (68.2–114.8) | ||
| Calcium | ||||
| Energy–adjusted (mg/1000 kcal) | ||||
| Mean (min–max) | 614.9 (44.9–969.1) | 581.2 (80.0–1520.2) | −33.7 (−181.6–114.3) | 0.64 |
| Median (IQR) | 637.7 (549.7–773.5) | 465.7 (349.2–723.7) | ||
| % RDA | ||||
| Mean (min–max) | 102.8 (0–334.3) | 96.3 (20.5–216.4) | −6.5 (−43.8–30.8) | 0.79 |
| Median (IQR) | 93.2 (64.2–109.8) | 76.1 (45.7–140.6) | ||
| Vitamin C | ||||
| Energy–adjusted (mg/1000 kcal) | ||||
| Mean (min–max) | 70.8 (0.3–390.5) | 86.8 (4.5–268.8) | 15.9 (−35.0–66.9) | 0.36 |
| Median (IQR) | 30.1 (16.4–63.5) | 63.2 (33.6–111.3) | ||
| % RDA | ||||
| Mean (min–max) | 292.1 (0.9–2132.1) | 436.0 (16.0–1307.7) | 143.9 (−80.8–368.7) | 0.08 |
| Median (IQR) | 98.1 (62.2–317.7) | 366.6 (149.5–679.9) | ||
| Vitamin D | ||||
| Energy–adjusted (μg/1000 kcal) | ||||
| Mean (min–max) | 3.7 (0–13.3) | 4.5 (0.3–33.1) | 0.7 (−2.7–4.2) | 1.00 |
| Median (IQR) | 4.0 (1.8–4.9) | 3.0 (0.9–5.1) | ||
| % RDA | ||||
| Mean (min–max) | 36.4 (0–80.4) | 47.9 (3.2–300.4) | 3.5 (−11.1–18.2) | 0.95 |
| Median (IQR) | 38.7 (20.3–53.0) | 35.3 (8.7–58.1) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bélanger, V.; Delorme, J.; Napartuk, M.; Bouchard, I.; Meloche, C.; Curnier, D.; Sultan, S.; Laverdière, C.; Sinnett, D.; Marcil, V. Early Nutritional Intervention to Promote Healthy Eating Habits in Pediatric Oncology: A Feasibility Study. Nutrients 2022, 14, 1024. https://doi.org/10.3390/nu14051024
Bélanger V, Delorme J, Napartuk M, Bouchard I, Meloche C, Curnier D, Sultan S, Laverdière C, Sinnett D, Marcil V. Early Nutritional Intervention to Promote Healthy Eating Habits in Pediatric Oncology: A Feasibility Study. Nutrients. 2022; 14(5):1024. https://doi.org/10.3390/nu14051024
Chicago/Turabian StyleBélanger, Véronique, Josianne Delorme, Mélanie Napartuk, Isabelle Bouchard, Caroline Meloche, Daniel Curnier, Serge Sultan, Caroline Laverdière, Daniel Sinnett, and Valérie Marcil. 2022. "Early Nutritional Intervention to Promote Healthy Eating Habits in Pediatric Oncology: A Feasibility Study" Nutrients 14, no. 5: 1024. https://doi.org/10.3390/nu14051024
APA StyleBélanger, V., Delorme, J., Napartuk, M., Bouchard, I., Meloche, C., Curnier, D., Sultan, S., Laverdière, C., Sinnett, D., & Marcil, V. (2022). Early Nutritional Intervention to Promote Healthy Eating Habits in Pediatric Oncology: A Feasibility Study. Nutrients, 14(5), 1024. https://doi.org/10.3390/nu14051024