Anti-Inflammatory and Anti-Catabolic Effects of Creatine Supplementation: A Brief Review


{kind=link}
{kind=link}
Abstract
:1. Introduction
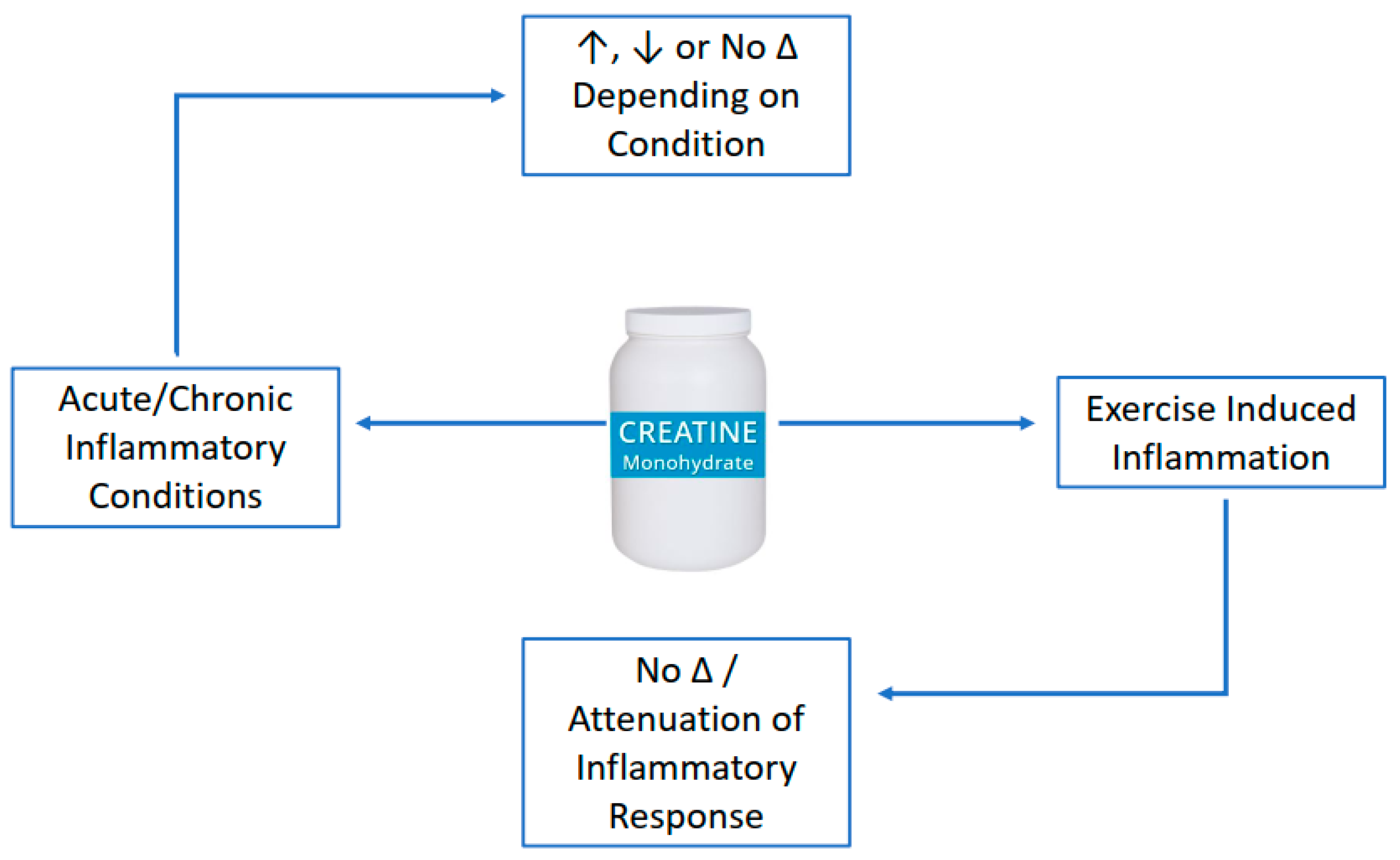
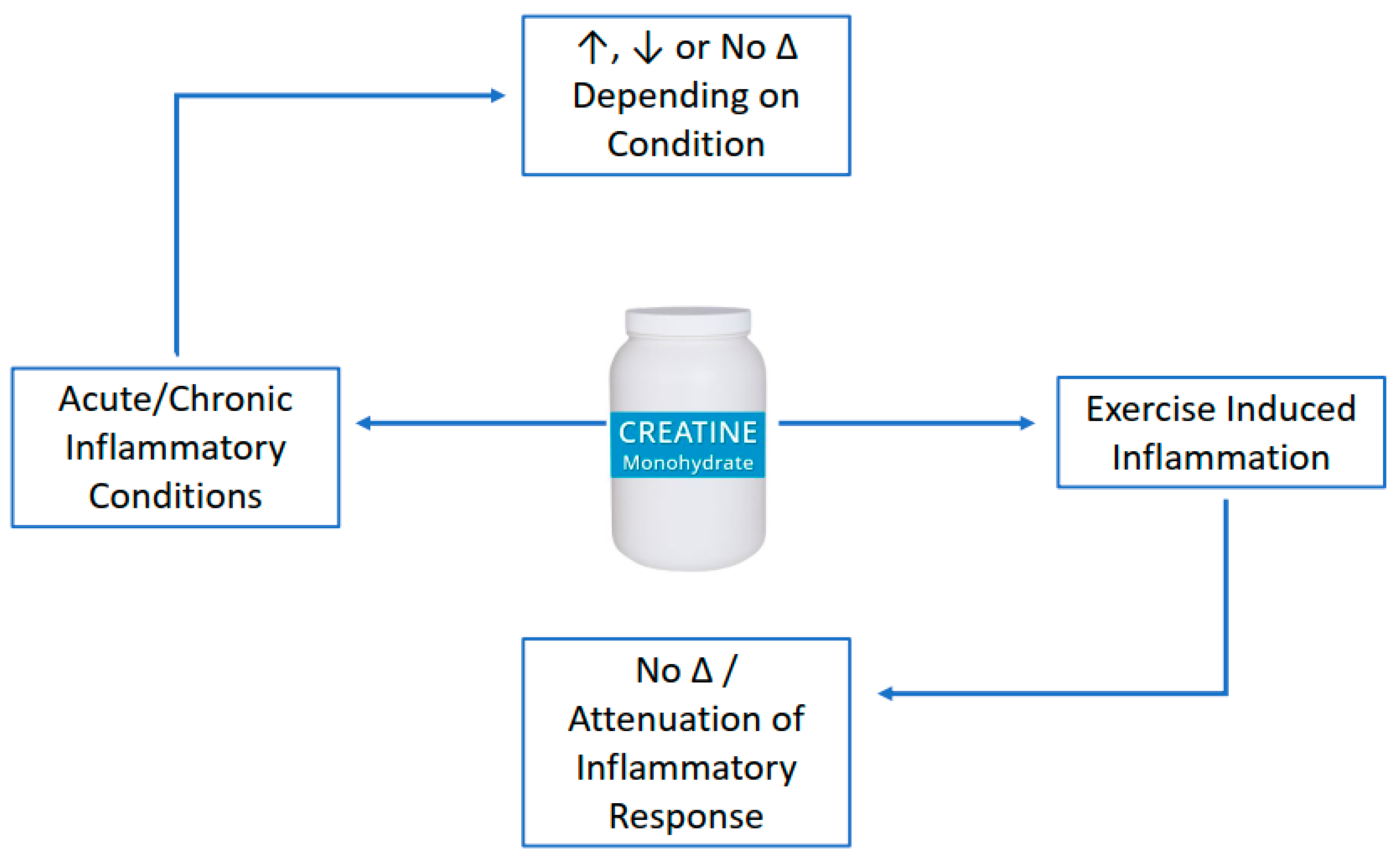
2. Anti-Inflammatory Effects of Creatine Supplementation
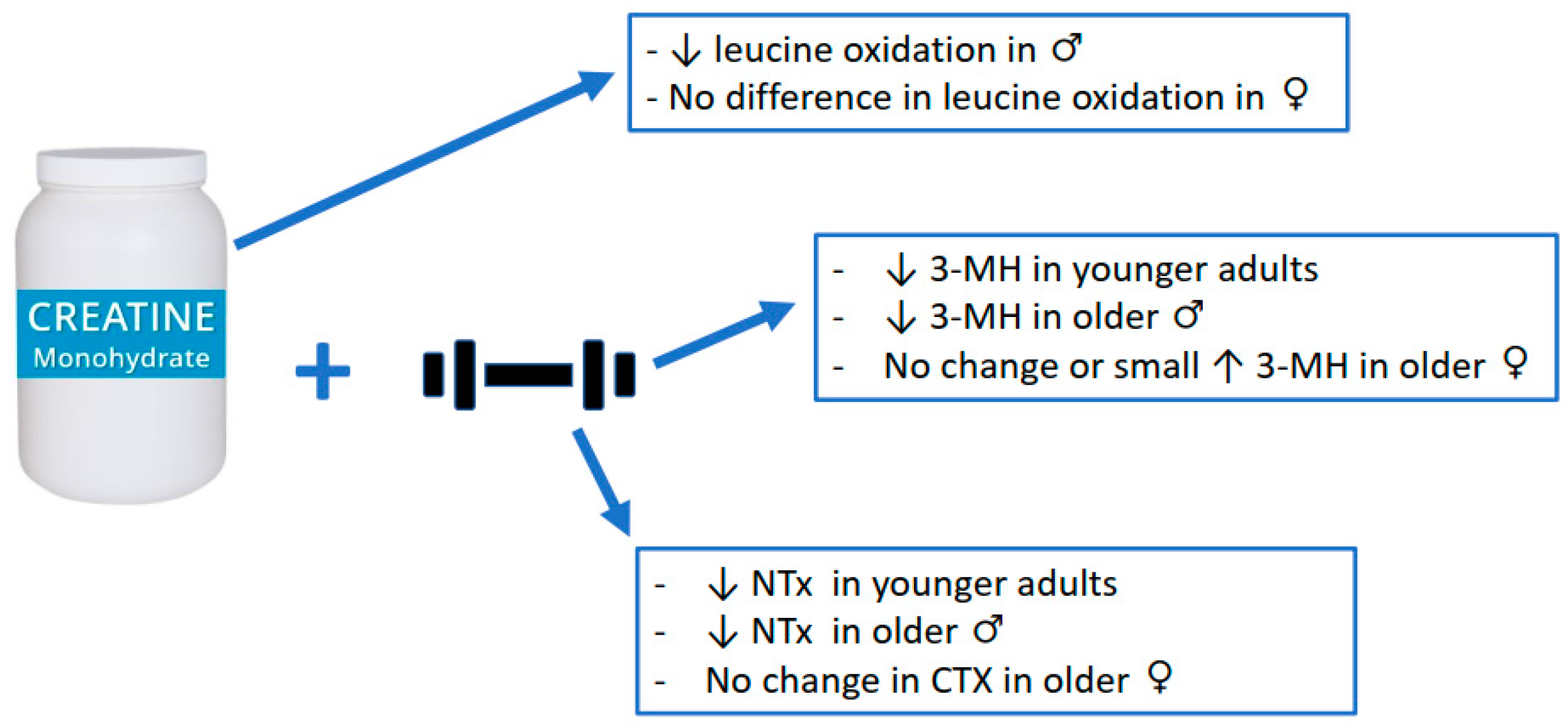
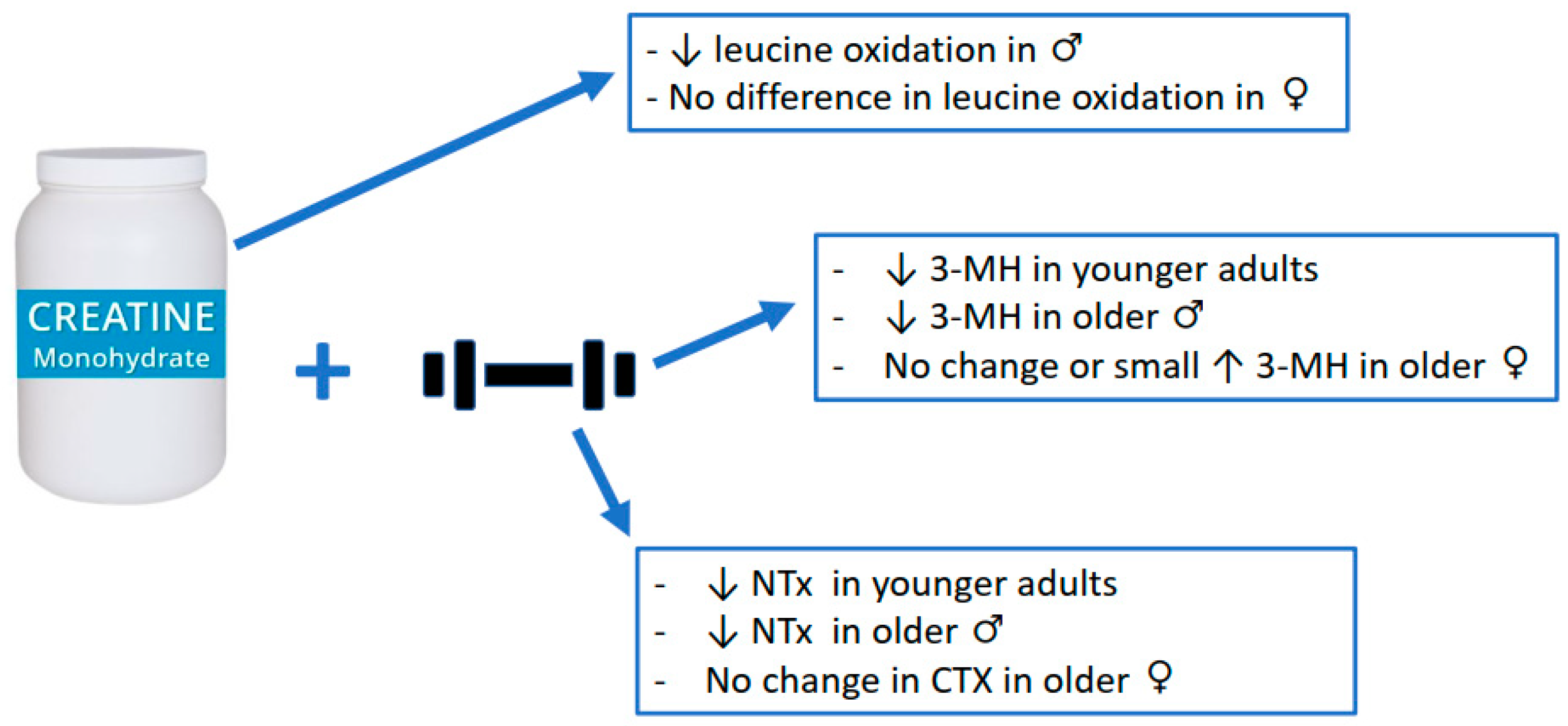
3. Anti-Catabolic Effects of Creatine Supplementation
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harris, R.C.; Söderlund, K.; Hultman, E. Elevation of Creatine in Resting and Exercised Muscle of Normal Subjects by Creatine Supplementation. Clin. Sci. 1992, 83, 367–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Branch, J.D. Effect of Creatine Supplementation on Body Composition and Performance: A Meta-Analysis. Int. J. Sport Nutr. Exerc. Metab. 2003, 13, 198–226. [Google Scholar] [CrossRef] [PubMed]
- Devries, M.C.; Phillips, S.M. Creatine Supplementation during Resistance Training in Older Adults—A Meta-Analysis. Med. Sci. Sports Exerc. 2014, 46, 1194–1203. [Google Scholar] [CrossRef]
- Chilibeck, P.; Kaviani, M.; Candow, D.; Zello, G.A. Effect of Creatine Supplementation during Resistance Training on Lean Tissue Mass and Muscular Strength in Older Adults: A Meta-Analysis. OAJSM 2017, 8, 213–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forbes, S.C.; Candow, D.G.; Ostojic, S.M.; Roberts, M.D.; Chilibeck, P.D. Meta-Analysis Examining the Importance of Creatine Ingestion Strategies on Lean Tissue Mass and Strength in Older Adults. Nutrients 2021, 13, 1912. [Google Scholar] [CrossRef] [PubMed]
- Dolan, E.; Artioli, G.G.; Pereira, R.M.R.; Gualano, B. Muscular Atrophy and Sarcopenia in the Elderly: Is There a Role for Creatine Supplementation? Biomolecules 2019, 9, 642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Candow, D.G.; Forbes, S.C.; Kirk, B.; Duque, G. Current Evidence and Possible Future Applications of Creatine Supplementation for Older Adults. Nutrients 2021, 13, 745. [Google Scholar] [CrossRef] [PubMed]
- Candow, D.G.; Forbes, S.C.; Chilibeck, P.D.; Cornish, S.M.; Antonio, J.; Kreider, R.B. Effectiveness of Creatine Supplementation on Aging Muscle and Bone: Focus on Falls Prevention and Inflammation. JCM 2019, 8, 488. [Google Scholar] [CrossRef] [Green Version]
- Kirk, B.; Feehan, J.; Lombardi, G.; Duque, G. Muscle, Bone, and Fat Crosstalk: The Biological Role of Myokines, Osteokines, and Adipokines. Curr. Osteoporos. Rep. 2020, 18, 388–400. [Google Scholar] [CrossRef]
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.I.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-Related Loss of Muscle Mass and Function. Physiol. Rev. 2019, 99, 427–511. [Google Scholar] [CrossRef]
- Bennett, J.M.; Reeves, G.; Billman, G.E.; Sturmberg, J.P. Inflammation–Nature’s Way to Efficiently Respond to All Types of Challenges: Implications for Understanding and Managing “the Epidemic” of Chronic Diseases. Front. Med. 2018, 5, 316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michaud, M.; Balardy, L.; Moulis, G.; Gaudin, C.; Peyrot, C.; Vellas, B.; Cesari, M.; Nourhashemi, F. Proinflammatory Cytokines, Aging, and Age-Related Diseases. J. Am. Med. Dir. Assoc. 2013, 14, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Jensen, G.L. Inflammation: Roles in Aging and Sarcopenia. JPEN J. Parenter Enter. Nutr. 2008, 32, 656–659. [Google Scholar] [CrossRef] [PubMed]
- Abdelmagid, S.M.; Barbe, M.F.; Safadi, F.F. Role of Inflammation in the Aging Bones. Life Sci. 2015, 123, 25–34. [Google Scholar] [CrossRef]
- Yin, F.; Sancheti, H.; Patil, I.; Cadenas, E. Energy Metabolism and Inflammation in Brain Aging and Alzheimer’s Disease. Free Radic Biol. Med. 2016, 100, 108–122. [Google Scholar] [CrossRef] [Green Version]
- Coussens, L.M.; Werb, Z. Inflammation and Cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef]
- Murdoch, J.R.; Lloyd, C.M. Chronic Inflammation and Asthma. Mutat. Res./Fundam. Mol. Mech. Mutagenesis 2010, 690, 24–39. [Google Scholar] [CrossRef]
- Goldring, M.B.; Otero, M. Inflammation in Osteoarthritis. Curr. Opin. Rheumatol. 2011, 23, 471–478. [Google Scholar] [CrossRef]
- Riehle, C.; Bauersachs, J. Key Inflammatory Mechanisms Underlying Heart Failure. Herz 2019, 44, 96–106. [Google Scholar] [CrossRef] [Green Version]
- Lakatos, L. Immunology of Inflammatory Bowel Diseases. Acta Physiol. Hung. 2000, 87, 355–372. [Google Scholar]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic Inflammation in the Etiology of Disease across the Life Span. Nat. Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef]
- Ostojic, S.M. Diagnostic and Pharmacological Potency of Creatine in Post-Viral Fatigue Syndrome. Nutrients 2021, 13, 503. [Google Scholar] [CrossRef] [PubMed]
- Bredahl, E.C.; Eckerson, J.M.; Tracy, S.M.; McDonald, T.L.; Drescher, K.M. The Role of Creatine in the Development and Activation of Immune Responses. Nutrients 2021, 13, 751. [Google Scholar] [CrossRef] [PubMed]
- Madan, B.R.; Khanna, N.K. Effect of Aminoacids on the Carrageenan-Induced Paw Oedema in Rats: A Preliminary Report. Indian J. Physiol. Pharmacol. 1976, 8, 227–229. [Google Scholar]
- Madan, B.R.; Khanna, N.K. Effect of Creatinine on Various Experimentally Induced Inflammatory Models. Indian J. Physiol. Pharmacol. 1979, 23, 1–7. [Google Scholar] [PubMed]
- Khanna, N.K.; Madan, B.R. Studies on the Anti-Inflammatory Activity of Creatine. Arch. Int. Pharmacodyn. Ther. 1978, 231, 340–350. [Google Scholar]
- Nomura, A.; Zhang, M.; Sakamoto, T.; Ishii, Y.; Morishima, Y.; Mochizuki, M.; Kimura, T.; Uchida, Y.; Sekizawa, K. Anti-Inflammatory Activity of Creatine Supplementation in Endothelial Cells in Vitro. Br. J. Pharmacol. 2003, 139, 715–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarnopolsky, M.A.; Bourgeois, J.M.; Snow, R.; Keys, S.; Roy, B.D.; Kwiecien, J.M.; Turnbull, J. Histological Assessment of Intermediate- and Long-Term Creatine Monohydrate Supplementation in Mice and Rats. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2003, 285, R762–R769. [Google Scholar] [CrossRef] [Green Version]
- Santos, R.V.T.; Bassit, R.A.; Caperuto, E.C.; Costa Rosa, L.F.B.P. The Effect of Creatine Supplementation upon Inflammatory and Muscle Soreness Markers after a 30 km Race. Life Sci. 2004, 75, 1917–1924. [Google Scholar] [CrossRef]
- Rawson, E.S.; Conti, M.P.; Miles, M.P. Creatine Supplementation Does Not Reduce Muscle Damage or Enhance Recovery from Resistance Exercise. J. Strength Cond. Res. 2007, 21, 1208–1213. [Google Scholar] [CrossRef]
- Vieira, R.P.; Duarte, A.C.S.; Claudino, R.C.; Perini, A.; Santos, A.B.G.; Moriya, H.T.; Arantes-Costa, F.M.; Martins, M.A.; Carvalho, C.R.F.; Dolhnikoff, M. Creatine Supplementation Exacerbates Allergic Lung Inflammation and Airway Remodeling in Mice. Am. J. Respir. Cell Mol. Biol. 2007, 37, 660–667. [Google Scholar] [CrossRef]
- Bassit, R.A.; Curi, R.; Costa Rosa, L.F.B.P. Creatine Supplementation Reduces Plasma Levels of Pro-Inflammatory Cytokines and PGE2 after a Half-Ironman Competition. Amino Acids 2008, 35, 425–431. [Google Scholar] [CrossRef]
- Bassit, R.A.; da Justa Pinheiro, C.H.; Vitzel, K.F.; Sproesser, A.J.; Silveira, L.R.; Curi, R. Effect of Short-Term Creatine Supplementation on Markers of Skeletal Muscle Damage after Strenuous Contractile Activity. Eur. J. Appl. Physiol. 2010, 108, 945–955. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, S.C.; Toledo, A.C.; Hage, M.; Santos, A.B.G.; Medeiros, M.C.R.; Martins, M.A.; Carvalho, C.R.F.; Dolhnikoff, M.; Vieira, R.P. Creatine Activates Airway Epithelium in Asthma. Int. J. Sports Med. 2010, 31, 906–912. [Google Scholar] [CrossRef] [PubMed]
- Leland, K.M.; McDonald, T.L.; Drescher, K.M. Effect of Creatine, Creatinine, and Creatine Ethyl Ester on TLR Expression in Macrophages. Int. Immunopharmacol. 2011, 11, 1341–1347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, L.A.; Tromm, C.B.; Da Rosa, G.; Bom, K.; Luciano, T.F.; Tuon, T.; De Souza, C.T.; Pinho, R.A. Creatine Supplementation Does Not Decrease Oxidative Stress and Inflammation in Skeletal Muscle after Eccentric Exercise. J. Sports Sci. 2013, 31, 1164–1176. [Google Scholar] [CrossRef]
- Deminice, R.; Rosa, F.T.; Franco, G.S.; Jordao, A.A.; de Freitas, E.C. Effects of Creatine Supplementation on Oxidative Stress and Inflammatory Markers after Repeated-Sprint Exercise in Humans. Nutrition 2013, 29, 1127–1132. [Google Scholar] [CrossRef] [Green Version]
- Campos-Ferraz, P.L.; Gualano, B.; das Neves, W.; Andrade, I.T.; Hangai, I.; Pereira, R.T.S.; Bezerra, R.N.; Deminice, R.; Seelaender, M.; Lancha, A.H. Exploratory Studies of the Potential Anti-Cancer Effects of Creatine. Amino Acids 2016, 48, 1993–2001. [Google Scholar] [CrossRef]
- Almeida, F.M.; Oliveira-Junior, M.C.; Souza, R.A.; Petroni, R.C.; Soto, S.F.; Soriano, F.G.; de Carvalho, P.T.C.; Albertini, R.; Damaceno-Rodrigues, N.R.; Lopes, F.D.T.Q.S.; et al. Creatine Supplementation Attenuates Pulmonary and Systemic Effects of Lung Ischemia and Reperfusion Injury. J. Heart Lung Transplant. 2016, 35, 242–250. [Google Scholar] [CrossRef]
- Cornish, S.M.; Peeler, J.D. No Effect of Creatine Monohydrate Supplementation on Inflammatory and Cartilage Degradation Biomarkers in Individuals with Knee Osteoarthritis. Nutr. Res. 2018, 51, 57–66. [Google Scholar] [CrossRef]
- Li, B.; Yang, L. Creatine in T Cell Antitumor Immunity and Cancer Immunotherapy. Nutrients 2021, 13, 1633. [Google Scholar] [CrossRef] [PubMed]
- Di Biase, S.; Ma, X.; Wang, X.; Yu, J.; Wang, Y.-C.; Smith, D.J.; Zhou, Y.; Li, Z.; Kim, Y.J.; Clarke, N.; et al. Creatine Uptake Regulates CD8 T Cell Antitumor Immunity. J. Exp. Med. 2019, 216, 2869–2882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izurieta-Munoz, H.; Gonzales, E.B.; Sumien, N. Effects of Creatine Supplementation on Nociception in Young Male and Female Mice. Pharm. Rep. 2018, 70, 316–321. [Google Scholar] [CrossRef]
- Hemati, F.; Rahmani, A.; Asadollahi, K.; Soleimannejad, K.; Khalighi, Z. Effects of Complementary Creatine Monohydrate and Physical Training on Inflammatory and Endothelial Dysfunction Markers among Heart Failure Patients. Asian J. Sports Med. 2016, 7, e28578. [Google Scholar] [CrossRef] [Green Version]
- Che, L.; Li, D. The Effects of Exercise on Cardiovascular Biomarkers: New Insights, Recent Data, and Applications. Adv. Exp. Med. Biol. 2017, 999, 43–53. [Google Scholar] [CrossRef]
- Wallimann, T.; Hall, C.; Colgan, S.; Glover, L. Creatine Supplementation for Patients with Inflammatory Bowel Diseases: A Scientific Rationale for a Clinical Trial. Nutrients 2021, 13, 1429. [Google Scholar] [CrossRef]
- Oliveira, C.L.P.; de Moura Mello Antunes, B.; Gomes, A.C.; Lira, F.S.; Pimentel, G.D.; Boulé, N.G.; Mota, J.F. Creatine Supplementation Does Not Promote Additional Effects on Inflammation and Insulin Resistance in Older Adults: A Pilot Randomized, Double-Blind, Placebo-Controlled Trial. Clin. Nutr. ESPEN 2020, 38, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Bell, K.E.; Snijders, T.; Zulyniak, M.A.; Kumbhare, D.; Parise, G.; Chabowski, A.; Phillips, S.M. A Multi-Ingredient Nutritional Supplement Enhances Exercise Training-Related Reductions in Markers of Systemic Inflammation in Healthy Older Men. Appl. Physiol. Nutr. Metab. 2018, 43, 299–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayward, S.; Wilborn, C.D.; Taylor, L.W.; Urbina, S.L.; Outlaw, J.J.; Foster, C.A.; Roberts, M.D. Effects of a High Protein and Omega-3-Enriched Diet with or Without Creatine Supplementation on Markers of Soreness and Inflammation During 5 Consecutive Days of High Volume Resistance Exercise in Females. J. Sports Sci. Med. 2016, 15, 704–714. [Google Scholar]
- Parise, G.; Mihic, S.; MacLennan, D.; Yarasheski, K.E.; Tarnopolsky, M.A. Effects of Acute Creatine Monohydrate Supplementation on Leucine Kinetics and Mixed-Muscle Protein Synthesis. J. Appl. Physiol. 2001, 91, 1041–1047. [Google Scholar] [CrossRef] [Green Version]
- Cornish, S.M.; Candow, D.G.; Jantz, N.T.; Chilibeck, P.D.; Little, J.P.; Forbes, S.; Abeysekara, S.; Zello, G.A. Conjugated Linoleic Acid Combined with Creatine Monohydrate and Whey Protein Supplementation during Strength Training. Int. J. Sport Nutr. Exerc. Metab. 2009, 19, 79–96. [Google Scholar] [CrossRef] [PubMed]
- Candow, D.G.; Little, J.P.; Chilibeck, P.D.; Abeysekara, S.; Zello, G.A.; Kazachkov, M.; Cornish, S.M.; Yu, P.H. Low-Dose Creatine Combined with Protein during Resistance Training in Older Men. Med. Sci. Sports Exerc. 2008, 40, 1645–1652. [Google Scholar] [CrossRef] [PubMed]
- Johannsmeyer, S.; Candow, D.G.; Brahms, C.M.; Michel, D.; Zello, G.A. Effect of Creatine Supplementation and Drop-Set Resistance Training in Untrained Aging Adults. Exp. Gerontol. 2016, 83, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Candow, D.G.; Zello, G.A.; Ling, B.; Farthing, J.P.; Chilibeck, P.D.; McLeod, K.; Harris, J.; Johnson, S. Comparison of Creatine Supplementation Before Versus After Supervised Resistance Training in Healthy Older Adults. Res. Sports Med. 2014, 22, 61–74. [Google Scholar] [CrossRef]
- Northeast, B.; Clifford, T. The Effect of Creatine Supplementation on Markers of Exercise-Induced Muscle Damage: A Systematic Review and Meta-Analysis of Human Intervention Trials. Int. J. Sport Nutr. Exerc. Metab. 2021, 31, 276–291. [Google Scholar] [CrossRef]
- Fernández-Landa, J.; Calleja-González, J.; León-Guereño, P.; Caballero-García, A.; Córdova, A.; Mielgo-Ayuso, J. Effect of the Combination of Creatine Monohydrate Plus. Nutrients 2019, 11, 2528. [Google Scholar] [CrossRef] [Green Version]
- Forsberg, A.M.; Nilsson, E.; Werneman, J.; Bergström, J.; Hultman, E. Muscle Composition in Relation to Age and Sex. Clin. Sci. 1991, 81, 249–256. [Google Scholar] [CrossRef] [Green Version]
- Chilibeck, P.D.; Candow, D.G.; Landeryou, T.; Kaviani, M.; Paus-Jenssen, L. Effects of Creatine and Resistance Training on Bone Health in Postmenopausal Women. Med. Sci. Sports Exerc. 2015, 47, 1587–1595. [Google Scholar] [CrossRef]
- Louis, M.; Lebacq, J.; Poortmans, J.R.; Belpaire-Dethiou, M.-C.; Devogelaer, J.-P.; Van Hecke, P.; Goubel, F.; Francaux, M. Beneficial Effects of Creatine Supplementation in Dystrophic Patients. Muscle Nerve 2003, 27, 604–610. [Google Scholar] [CrossRef]
- Tarnopolsky, M.A.; Mahoney, D.J.; Vajsar, J.; Rodriguez, C.; Doherty, T.J.; Roy, B.D.; Biggar, D. Creatine Monohydrate Enhances Strength and Body Composition in Duchenne Muscular Dystrophy. Neurology 2004, 62, 1771–1777. [Google Scholar] [CrossRef] [Green Version]
- Gualano, B.; Macedo, A.R.; Alves, C.R.R.; Roschel, H.; Benatti, F.B.; Takayama, L.; de Sá Pinto, A.L.; Lima, F.R.; Pereira, R.M.R. Creatine Supplementation and Resistance Training in Vulnerable Older Women: A Randomized Double-Blind Placebo-Controlled Clinical Trial. Exp. Gerontol. 2014, 53, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Lobo, D.M.; Tritto, A.C.; da Silva, L.R.; de Oliveira, P.B.; Benatti, F.B.; Roschel, H.; Nieß, B.; Gualano, B.; Pereira, R.M.R. Effects of Long-Term Low-Dose Dietary Creatine Supplementation in Older Women. Exp. Gerontol. 2015, 70, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Sales, L.P.; Pinto, A.J.; Rodrigues, S.F.; Alvarenga, J.C.; Gonçalves, N.; Sampaio-Barros, M.M.; Benatti, F.B.; Gualano, B.; Rodrigues Pereira, R.M. Creatine Supplementation (3 g/d) and Bone Health in Older Women: A 2-Year, Randomized, Placebo-Controlled Trial. J. Gerontol. Ser. A 2020, 75, 931–938. [Google Scholar] [CrossRef] [PubMed]
- Gerber, I.; ap Gwynn, I.; Alini, M.; Wallimann, T. Stimulatory Effects of Creatine on Metabolic Activity, Differentiation and Mineralization of Primary Osteoblast-like Cells in Monolayer and Micromass Cell Cultures. Eur. Cell Mater. 2005, 10, 8–22. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, H.; Shima, N.; Nakagawa, N.; Mochizuki, S.-I.; Yano, K.; Fujise, N.; Sato, Y.; Goto, M.; Yamaguchi, K.; Kuriyama, M.; et al. Identity of Osteoclastogenesis Inhibitory Factor (OCIF) and Osteoprotegerin (OPG): A Mechanism by Which OPG/OCIF Inhibits Osteoclastogenesis in Vitro. Endocrinology 1998, 139, 1329–1337. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cordingley, D.M.; Cornish, S.M.; Candow, D.G. Anti-Inflammatory and Anti-Catabolic Effects of Creatine Supplementation: A Brief Review. Nutrients 2022, 14, 544. https://doi.org/10.3390/nu14030544
Cordingley DM, Cornish SM, Candow DG. Anti-Inflammatory and Anti-Catabolic Effects of Creatine Supplementation: A Brief Review. Nutrients. 2022; 14(3):544. https://doi.org/10.3390/nu14030544
Chicago/Turabian StyleCordingley, Dean M., Stephen M. Cornish, and Darren G. Candow. 2022. "Anti-Inflammatory and Anti-Catabolic Effects of Creatine Supplementation: A Brief Review" Nutrients 14, no. 3: 544. https://doi.org/10.3390/nu14030544
APA StyleCordingley, D. M., Cornish, S. M., & Candow, D. G. (2022). Anti-Inflammatory and Anti-Catabolic Effects of Creatine Supplementation: A Brief Review. Nutrients, 14(3), 544. https://doi.org/10.3390/nu14030544