Household Water Access, Dietary Diversity and Nutritional Status among Preschoolers in Poor, Rural Areas of Central and Western China


Abstract
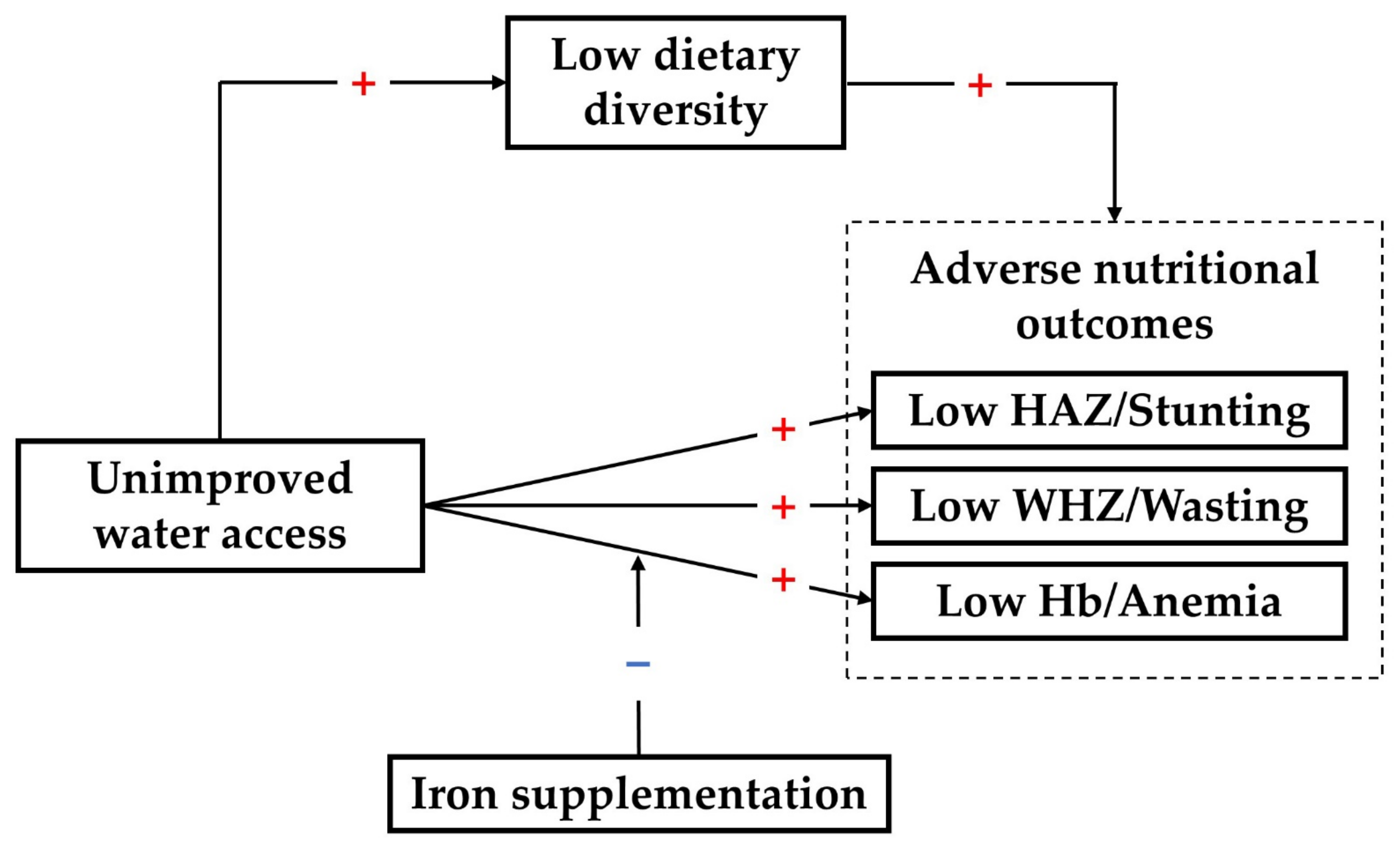
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Exposures
2.3. Outcomes
2.4. A Priori Confounding Variables
2.5. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Association between Household Water Access and Dietary Diversity
3.3. Association between Household Water Access and Nutritional Outcomes
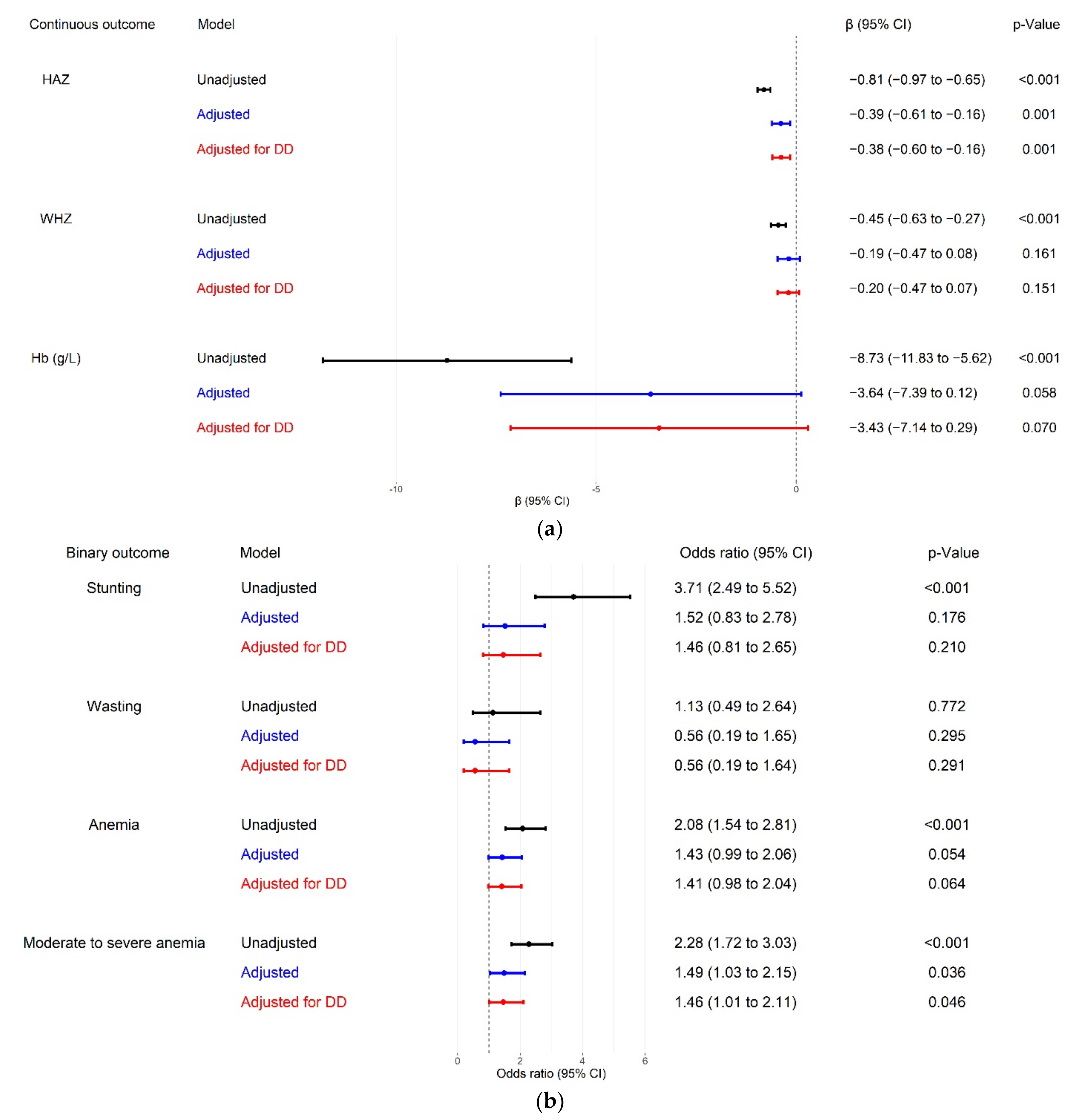
3.4. The Mediating Effect of Dietary Diversity
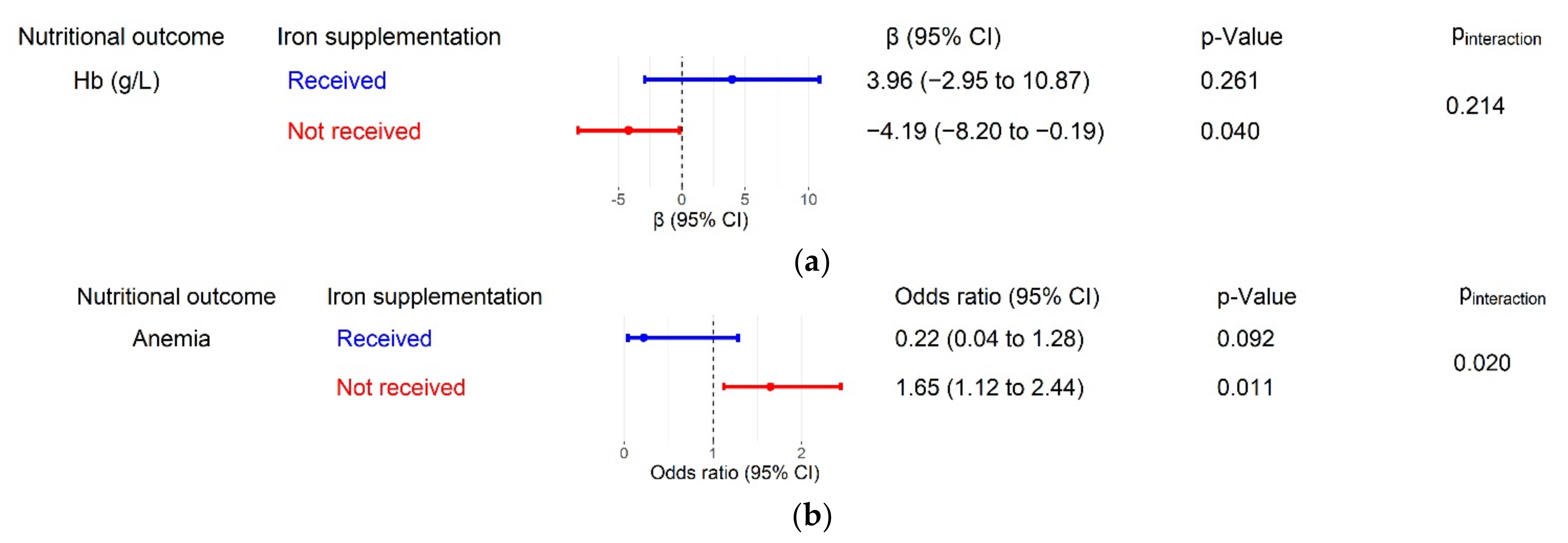
3.5. The Moderating Effect of Iron Supplementation
4. Discussion
4.1. Principal Findings
4.2. Comparison with Other Studies
4.3. Strength and Limitations
4.4. Implications for Future Research
4.5. Policy Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Global Anaemia Estimates, 2021 Edition. Available online: https://www.who.int/data/gho/data/themes/topics/anaemia_in_women_and_children (accessed on 18 October 2021).
- United Nations Children’s Fund; World Health Organization; World Bank Group. UNICEF/WHO/The World Bank Group Joint Child Malnutrition Estimates: Levels and Trends in Child Malnutrition: Key Findings of the 2021 Edition; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- United Nations Children’s Fund. Malnutrition. Available online: https://data.unicef.org/topic/nutrition/malnutrition/ (accessed on 11 January 2022).
- World Health Organization. Prevalence of Anaemia in Children Aged 6–59 Months (%). Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-anaemia-in-children-under-5-years-(-) (accessed on 11 January 2022).
- Fang, H.; Yu, D.; Guo, Q. Anemia prevalence of among 0-5 years old children in China, 2013. China J. Public Health 2018, 34, 1654–1657. [Google Scholar]
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.; Webb, P.; Lartey, A.; Black, R.E. Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? Lancet 2013, 382, 452–477. [Google Scholar] [CrossRef]
- World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices: Definitions and Measurement Methods; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Onyango, A.W.; Borghi, E.; de Onis, M.; Casanovas Mdel, C.; Garza, C. Complementary feeding and attained linear growth among 6-23-month-old children. Public Health Nutr. 2014, 17, 1975–1983. [Google Scholar] [CrossRef]
- Li, Z.; Kim, R.; Vollmer, S.; Subramanian, S.V. Factors Associated with Child Stunting, Wasting, and Underweight in 35 Low- and Middle-Income Countries. JAMA Netw. Open 2020, 3, e203386. [Google Scholar] [CrossRef] [Green Version]
- Saaka, M.; Galaa, S.Z. How is dietary diversity related to haematological status of preschool children in Ghana? Food Nutr. Res. 2017, 61, 1333389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations Children’s Fund. Diets. Available online: https://data.unicef.org/topic/nutrition/diets/ (accessed on 18 October 2021).
- Wang, A.; Scherpbier, R.W.; Huang, X.; Guo, S.; Yang, Y.; Josephs-Spaulding, J.; Ma, C.; Zhou, H.; Wang, Y. The dietary diversity and stunting prevalence in minority children under 3 years old: A cross-sectional study in forty-two counties of western China. Br. J. Nutr. 2017, 118, 840–848. [Google Scholar] [CrossRef] [Green Version]
- Solomon, D.; Aderaw, Z.; Tegegne, T.K. Minimum dietary diversity and associated factors among children aged 6-23 months in Addis Ababa, Ethiopia. Int. J. Equity Health 2017, 16, 181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woldegebriel, A.G.; Desta, A.A.; Gebreegziabiher, G.; Berhe, A.A.; Ajemu, K.F.; Woldearegay, T.W. Dietary Diversity and Associated Factors among Children Aged 6-59 Months in Ethiopia: Analysis of Ethiopian Demographic and Health Survey 2016 (EDHS 2016). Int. J. Pediatrics 2020, 2020, 3040845. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Progress towards the Sustainable Development Goals. Report of the Secretary-General; UN Economic and Social Council: New York, NY, USA, 2016. [Google Scholar]
- Wolf, J.; Prüss-Ustün, A.; Cumming, O.; Bartram, J.; Bonjour, S.; Cairncross, S.; Clasen, T.; Colford, J.M., Jr.; Curtis, V.; De France, J.; et al. Assessing the impact of drinking water and sanitation on diarrhoeal disease in low- and middle-income settings: Systematic review and meta-regression. Trop. Med. Int. Health 2014, 19, 928–942. [Google Scholar] [CrossRef] [PubMed]
- Fink, G.; Günther, I.; Hill, K. The effect of water and sanitation on child health: Evidence from the demographic and health surveys 1986–2007. Int. J. Epidemiol. 2011, 40, 1196–1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorsey, J.L.; Manohar, S.; Neupane, S.; Shrestha, B.; Klemm, R.D.W.; West, K.P., Jr. Individual, household, and community level risk factors of stunting in children younger than 5 years: Findings from a national surveillance system in Nepal. Matern. Child Nutr. 2018, 14, e12434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kothari, M.T.; Coile, A.; Huestis, A.; Pullum, T.; Garrett, D.; Engmann, C. Exploring associations between water, sanitation, and anemia through 47 nationally representative demographic and health surveys. Ann. N. Y. Acad. Sci. 2019, 1450, 249–267. [Google Scholar] [CrossRef] [PubMed]
- Yu, E.X.; Addo, O.Y.; Williams, A.M.; Engle-Stone, R.; Ou, J.; Huang, W.; Guo, J.; Suchdev, P.S.; Young, M.F. Association between anemia and household water source or sanitation in preschool children: The Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) project. Am. J. Clin. Nutr. 2020, 112, 488S–497S. [Google Scholar] [CrossRef] [PubMed]
- Hess, T.; Sutcliffe, C. The exposure of a fresh fruits and vegetable supply chain to global water-related risks. Water Int. 2018, 43, 746–761. [Google Scholar] [CrossRef] [Green Version]
- Choudhary, N.; Schuster, R.C.; Brewis, A.; Wutich, A. Household Water Insecurity Affects Child Nutrition Through Alternative Pathways to WASH: Evidence from India. Food Nutr. Bull. 2021, 42, 170–187. [Google Scholar] [CrossRef]
- Zhou, H.; Qu, X.; Yang, Y.; Kc, A.; Liu, X.; Yang, C.; Wang, A.; Huang, Y.; Sun, J.; Huang, X.; et al. Relationship between moderate to late preterm, diet types and developmental delay in less-developed rural China. Nutr. Neurosci. 2020, 1–10. [Google Scholar] [CrossRef]
- Huang, Y.; Wang, Y.; Chen, C.; Gao, Y.; Kc, A.; Wang, X.; Zou, S.; Zhou, H. Association between Violent Discipline at Home and Risk of Illness and Injury in Children: Findings from a Cross-sectional Study in Rural Western China. J. Interpers. Violence 2021, 886260521991895. [Google Scholar] [CrossRef]
- Song, Q.; Yang, Y.; Liu, X.; Yang, C.; Huang, X.; Zhou, H.; Wang, Y. Breastfeeding Practices and Overweight/Obesity Among Children Under 5 Years of Age: A Multistage Random Sampling Survey in Central and Western China. Matern. Child Health J. 2020, 24, 998–1007. [Google Scholar] [CrossRef]
- Dewey, K.G.; Chaparro, C.M. Session 4: Mineral metabolism and body composition Iron status of breast-fed infants: Symposium on ‘Nutrition in early life: New horizons in a new century’. Proc. Nutr. Soc. 2007, 66, 412–422. [Google Scholar] [CrossRef]
- United Nations Children’s Fund; World Health Organization. Core Questions and Indicators for Monitoring WASH in Health Care Facilities in the Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- United Nations Children’s Fund. Multiple Indicator Cluster Survey (MICS). Available online: http://mics.unicef.org (accessed on 22 May 2020).
- World Health Organization. Nutrition Landscape Information System (NLIS) Country Profile Indicators: Interpretation Guide; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- World Health Organization. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- The INACG Steering Committee. Adjusting Hemoglobin Values in Program Surveys; International Nutritional Anaemia Consultative Group: Washington, DC, USA, 2002. [Google Scholar]
- World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- World Food Programme. Vulnerability Analysis & Mapping Guidance Paper-Creation of a Wealth Index; World Food Programme: Rome, Italy, 2017. [Google Scholar]
- Tusting, L.S.; Gething, P.W.; Gibson, H.S.; Greenwood, B.; Knudsen, J.; Lindsay, S.W.; Bhatt, S. Housing and child health in sub-Saharan Africa: A cross-sectional analysis. PLoS Med. 2020, 17, e1003055. [Google Scholar] [CrossRef] [Green Version]
- Cumming, O.; Cairncross, S. Can water, sanitation and hygiene help eliminate stunting? Current evidence and policy implications. Matern. Child Nutr. 2016, 12 (Suppl. 1), 91–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, S.M.; Mbullo Owuor, P.; Miller, J.D.; Boateng, G.O.; Wekesa, P.; Onono, M.; Young, S.L. ‘I know how stressful it is to lack water!’ Exploring the lived experiences of household water insecurity among pregnant and postpartum women in western Kenya. Glob. Public Health 2019, 14, 649–662. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Jun, Y.; Xu, Z.; Rozelle, S.; Li, N. Agricultural trade liberalization and poverty in China. China Econ. Rev. 2007, 18, 244–265. [Google Scholar] [CrossRef]
- Anato, A.; Baye, K.; Tafese, Z.; Stoecker, B.J. Maternal depression is associated with child undernutrition: A cross-sectional study in Ethiopia. Matern. Child Nutr. 2020, 16, e12934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, L.C.; Neupane, S.; Sparling, T.M.; Shrestha, M.; Joshi, N.; Lohani, M.; Thorne-Lyman, A. Maternal depression is associated with less dietary diversity among rural Nepali children. Matern. Child Nutr. 2021, 17, e13221. [Google Scholar] [CrossRef]
- Gao, Y.; Wang, Y.; Mi, X.; Zhou, M.; Zou, S.; Zhou, H. Intimate Partner Violence against Women Living in Inadequate Conditions in Sub-Saharan Africa: A Meta-Analysis of Demographic and Health Survey Data. Int. J. Env. Res. Public Health 2021, 18, 10138. [Google Scholar] [CrossRef] [PubMed]
- Tsedal, D.M.; Yitayal, M.; Abebe, Z.; Tsegaye, A.T. Effect of intimate partner violence of women on minimum acceptable diet of children aged 6–23 months in Ethiopia: Evidence from 2016 Ethiopian demographic and health survey. BMC Nutr. 2020, 6, 28. [Google Scholar] [CrossRef]
- Caleyachetty, R.; Uthman, O.A.; Bekele, H.N.; Martín-Cañavate, R.; Marais, D.; Coles, J.; Steele, B.; Uauy, R.; Koniz-Booher, P. Maternal exposure to intimate partner violence and breastfeeding practices in 51 low-income and middle-income countries: A population-based cross-sectional study. PLoS Med. 2019, 16, e1002921. [Google Scholar] [CrossRef] [Green Version]
- Esrey, S.A. Water, waste, and well-being: A multicountry study. Am. J. Epidemiol. 1996, 143, 608–623. [Google Scholar] [CrossRef] [Green Version]
- Harris, M.; Alzua, M.L.; Osbert, N.; Pickering, A. Community-Level Sanitation Coverage More Strongly Associated with Child Growth and Household Drinking Water Quality than Access to a Private Toilet in Rural Mali. Environ. Sci. Technol. 2017, 51, 7219–7227. [Google Scholar] [CrossRef] [Green Version]
- Villamor, E.; Mbise, R.; Spiegelman, D.; Ndossi, G.; Fawzi, W.W. Vitamin A supplementation and other predictors of anemia among children from Dar Es Salaam, Tanzania. Am. J. Trop. Med. Hyg. 2000, 62, 590–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tengco, L.W.; Rayco-Solon, P.; Solon, J.A.; Sarol, J.N., Jr.; Solon, F.S. Determinants of anemia among preschool children in the Philippines. J. Am. Coll. Nutr. 2008, 27, 229–243. [Google Scholar] [CrossRef] [PubMed]
- Li, P. Groundwater Quality in western China: Challenges and Paths Forward for Groundwater Quality Research in western China. Expo. Health 2016, 8, 305–310. [Google Scholar] [CrossRef] [Green Version]
- Jurek, A.M.; Greenland, S.; Maldonado, G.; Church, T.R. Proper interpretation of non-differential misclassification effects: Expectations vs observations. Int. J. Epidemiol. 2005, 34, 680–687. [Google Scholar] [CrossRef] [Green Version]
- Dewey, K.G.; Mayers, D.R. Early child growth: How do nutrition and infection interact? Matern. Child Nutr. 2011, 7 (Suppl. 3), 129–142. [Google Scholar] [CrossRef]
- Li, Z.; Tian, Y.; Gong, Z.; Qian, L. Health Literacy and Regional Heterogeneities in China: A Population-Based Study. Front. Public Health 2021, 9, 603325. [Google Scholar] [CrossRef]
- United Nations Children’s Fund; World Health Organization. Implications of Recent WASH and Nutrition Studies for WASH Policy and Practice; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Humphrey, J.H.; Mbuya, M.N.N.; Ntozini, R.; Moulton, L.H.; Stoltzfus, R.J.; Tavengwa, N.V.; Mutasa, K.; Majo, F.; Mutasa, B.; Mangwadu, G.; et al. Independent and combined effects of improved water, sanitation, and hygiene, and improved complementary feeding, on child stunting and anaemia in rural Zimbabwe: A cluster-randomised trial. Lancet. Glob. Health 2019, 7, e132–e147. [Google Scholar] [CrossRef] [Green Version]
- Stewart, C.P.; Dewey, K.G.; Lin, A.; Pickering, A.J.; Byrd, K.A.; Jannat, K.; Ali, S.; Rao, G.; Dentz, H.N.; Kiprotich, M.; et al. Effects of lipid-based nutrient supplements and infant and young child feeding counseling with or without improved water, sanitation, and hygiene (WASH) on anemia and micronutrient status: Results from 2 cluster-randomized trials in Kenya and Bangladesh. Am. J. Clin. Nutr. 2019, 109, 148–164. [Google Scholar] [CrossRef] [Green Version]
- Larson, L.M.; Young, M.F.; Ramakrishnan, U.; Webb Girard, A.; Verma, P.; Chaudhuri, I.; Srikantiah, S.; Martorell, R. A Cross-Sectional Survey in Rural Bihar, India, Indicates That Nutritional Status, Diet, and Stimulation Are Associated with Motor and Mental Development in Young Children. J. Nutr. 2017, 147, 1578–1585. [Google Scholar] [CrossRef]
- Allali, S.; Brousse, V.; Sacri, A.S.; Chalumeau, M.; de Montalembert, M. Anemia in children: Prevalence, causes, diagnostic work-up, and long-term consequences. Expert Rev. Hematol. 2017, 10, 1023–1028. [Google Scholar] [CrossRef]
- De Sanctis, V.; Soliman, A.; Alaaraj, N.; Ahmed, S.; Alyafei, F.; Hamed, N. Early and Long-term Consequences of Nutritional Stunting: From Childhood to Adulthood. Acta Bio Med. 2021, 92, e2021168. [Google Scholar] [CrossRef]
- National Development and Reform Commission. Management of Rural Drinking Water Safety Projects. Available online: http://www.gov.cn/gongbao/content/2014/content_2661995.htm (accessed on 11 January 2022).
- Ministry of Water Resources. Statements from the Ministry of Water Resources on Rural Drinking Water Safety Projects in Extremely Impoverished Areas. Available online: http://www.mwr.gov.cn/zwgk/gknr/201802/t20180209_1442749.html (accessed on 11 January 2022).
- The World Bank. Innovating Water and Sanitation Services in China’s Rural Areas. Available online: https://www.worldbank.org/en/news/press-release/2020/03/03/innovating-water-and-sanitation-services-in-chinas-rural-areas (accessed on 11 January 2022).
- United Nations Children’s Fund. Drinking Water. Available online: https://data.unicef.org/topic/water-and-sanitation/drinking-water/ (accessed on 11 January 2022).
- Independent Group of Scientists Appointed by the Secretary-General. Global Sustainable Development Report 2019: The Future is Now—Science for Achieving Sustainable Development; United Nations: New York, NY, USA, 2019. [Google Scholar]
- Li, Z.; Li, X.; Sudfeld, C.R.; Liu, Y.; Tang, K.; Huang, Y.; Fawzi, W. The Effect of the Yingyangbao Complementary Food Supplement on the Nutritional Status of Infants and Children: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 2404. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| WHO Food Groups | Food Items in the Questionnaire |
|---|---|
| Breast milk | Breast milk |
| Grains, roots and tubers | Bread, rice, noodles, white potatoes, white yams, manioc, cassava |
| Legumes, nuts and seeds | Beans, peas, lentils, nuts |
| Dairy products | Infant formula, milk from animals (fresh, tinned or powdered), yogurt, hard or soft cheese |
| Flesh foods | Liver, kidney, heart, beef, pork, lamb, goat, chicken, duck, fresh or dried fish, shellfish, shrimps |
| Eggs | Eggs |
| Vitamin A-rich fruits and vegetables | Pumpkin, carrots, sweet red peppers, squash or sweet potatoes that are yellow or orange inside; dark green leafy vegetables such as spinach; ripe mangoes, ripe papayas, tomato, Chinese hawthorn, persimmon |
| Other fruits and vegetables | Any other fruits and vegetables |
| Characteristics | Total Sample (N = 3727) 2 | Household Water Access | |
|---|---|---|---|
| Improved (N = 3228, 86.6%) | Unimproved (N = 499, 13.4%) | ||
| Age (months) 1 | 28.0 (14.8) | 28.5 (14.9) | 24.4 (13.9) |
| Sex | |||
| Female | 1687 (45.3) | 1453 (45.0) | 234 (46.9) |
| Male | 2040 (54.7) | 1775 (55.0) | 265 (53.1) |
| Birth order | |||
| First-born | 1493 (40.1) | 1346 (41.7) | 147 (29.5) |
| Later-born | 2234 (59.9) | 1882 (58.3) | 352 (70.5) |
| Primary caregiver | |||
| Mother | 2496 (67.0) | 2168 (67.2) | 328 (65.7) |
| Father | 290 (7.8) | 252 (7.8) | 38 (7.6) |
| Grandmother | 716 (19.2) | 611 (18.9) | 105 (21.0) |
| Grandfather | 185 (5.0) | 167 (5.2) | 18 (3.6) |
| Others | 40 (1.1) | 30 (0.9) | 10 (2.0) |
| Left-behind | |||
| Yes | 1721 (46.2) | 1442 (44.7) | 279 (55.9) |
| No | 2006 (53.8) | 1786 (55.3) | 220 (44.1) |
| Education level | |||
| Illiterate | 666 (17.9) | 380 (11.8) | 286 (57.3) |
| Primary school | 844 (22.6) | 722 (22.4) | 122 (24.4) |
| Middle school | 1570 (42.1) | 1497 (46.4) | 73 (14.6) |
| High school | 415 (11.1) | 404 (12.5) | 11 (2.2) |
| College and above | 232 (6.2) | 225 (7.0) | 7 (1.4) |
| Currently smoking | |||
| Yes | 300 (8.0) | 225 (7.0) | 75 (15.0) |
| No | 3427 (92.0) | 3003 (93.0) | 424 (85.0) |
| Household wealth quintile 3 | |||
| 1 | 730 (19.6) | 400 (12.4) | 330 (66.1) |
| 2 | 735 (19.7) | 639 (19.8) | 96 (19.2) |
| 3 | 745 (20.0) | 709 (22.0) | 36 (7.2) |
| 4 | 752 (20.2) | 733 (22.7) | 19 (3.8) |
| 5 | 765 (20.5) | 747 (23.1) | 18 (3.6) |
| Household sanitation facilities | |||
| Improved | 2561 (68.7) | 2171 (67.3) | 390 (78.2) |
| Unimproved | 1122 (30.1) | 1038 (32.2) | 84 (16.8) |
| Unknown | 44 (1.2) | 19 (0.6) | 25 (5.0) |
| Handwashing with soap | |||
| Yes | 2456 (65.9) | 2269 (70.3) | 187 (37.5) |
| No | 1207 (32.4) | 937 (29.0) | 270 (54.1) |
| Unknown | 64 (1.7) | 22 (0.7) | 42 (8.4) |
| Food Groups | Total Sample (N = 1646) 1 | Household Water Access | Unadjusted | Adjusted 3 | |||
|---|---|---|---|---|---|---|---|
| Improved (N = 1369, 83.2%) 2 | Unimproved (N = 277, 16.8%) 2 | OR (95% CI) | p-Value | OR (95% CI) | p-Value | ||
| Breast milk | 596 (38.9) | 495 (38.8) | 101 (39.1) | 1.02 (0.72 to 1.43) | 0.932 | 0.56 (0.33 to 0.95) | 0.032 |
| Grains, roots and tubers | 1472 (89.4) | 1235 (90.2) | 237 (85.6) | 0.64 (0.42 to 0.99) | 0.043 | 0.90 (0.53 to 1.53) | 0.695 |
| Legumes, nuts and seeds | 366 (22.3) | 339 (24.8) | 27 (9.8) | 0.33 (0.20 to 0.55) | <0.001 | 0.71 (0.39 to 1.28) | 0.252 |
| Dairy products | 989 (60.1) | 879 (64.2) | 110 (39.7) | 0.37 (0.27 to 0.51) | <0.001 | 0.98 (0.62 to 1.53) | 0.913 |
| Flesh foods | 944 (57.4) | 822 (60.0) | 122 (44.0) | 0.52 (0.39 to 0.71) | <0.001 | 0.89 (0.62 to 1.30) | 0.561 |
| Eggs | 777 (47.3) | 691 (50.5) | 86 (31.0) | 0.44 (0.31 to 0.62) | <0.001 | 1.08 (0.72 to 1.64) | 0.709 |
| Vitamin A-rich fruits and vegetables | 1174 (71.3) | 1040 (76.0) | 134 (48.4) | 0.30 (0.22 to 0.40) | <0.001 | 0.51 (0.35 to 0.75) | 0.001 |
| Other fruits and vegetables | 834 (50.9) | 768 (56.2) | 66 (24.1) | 0.25 (0.17 to 0.36) | <0.001 | 0.55 (0.36 to 0.83) | 0.004 |
| Dietary diversity | 820 (49.8) | 760 (55.5) | 60 (21.7) | 0.22 (0.16 to 0.31) | <0.001 | 0.65 (0.44 to 0.98) | 0.039 |
| Nutritional Outcomes | Total Sample (N = 3727) 1 | Improved Water Access (N = 3228, 86.6%) | Unimproved Water Access (N = 499, 13.4%) | Unadjusted | Adjusted 2 | ||
|---|---|---|---|---|---|---|---|
| Continuous Outcomes | Mean (SD) | Mean (SD) | Mean (SD) | β (95% CI) | p-Value | β (95% CI) | p-Value |
| HAZ | −0.42 (1.21) | −0.33 (1.18) | −1.06 (1.21) | −0.73 (−0.86 to −0.61) | <0.001 | −0.34 (−0.49 to −0.19) | <0.001 |
| WHZ | 0.43 (1.13) | 0.46 (1.11) | 0.22 (1.21) | −0.25 (−0.37 to −0.13) | <0.001 | −0.11 (−0.27 to 0.06) | 0.205 |
| Hb concentration (g/L) | 109.97 (16.62) | 111.08 (15.99) | 102.79 (18.70) | −8.29 (−10.59 to −5.99) | <0.001 | −2.78 (−5.16 to −0.41) | 0.022 |
| Binary Outcomes | N (%) | N (%) | N (%) | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Stunting | 317 (8.5) | 216 (6.7) | 101 (20.2) | 3.54 (2.69 to 4.66) | <0.001 | 1.50 (1.01 to 2.25) | 0.047 |
| Wasting | 74 (2.0) | 62 (1.9) | 12 (2.4) | 1.26 (0.65 to 2.43) | 0.495 | 0.56 (0.24 to 1.30) | 0.174 |
| Anemia | 1649 (44.2) | 1349 (41.8) | 300 (60.1) | 2.10 (1.67 to 2.64) | <0.001 | 1.34 (1.02 to 1.77) | 0.037 |
| Moderate to severe anemia | 860 (23.1) | 674 (20.9) | 186 (37.3) | 2.25 (1.78 to 2.85) | <0.001 | 1.25 (0.94 to 1.67) | 0.128 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, Y.; Sheng, J.; Mi, X.; Zhou, M.; Zou, S.; Zhou, H. Household Water Access, Dietary Diversity and Nutritional Status among Preschoolers in Poor, Rural Areas of Central and Western China. Nutrients 2022, 14, 458. https://doi.org/10.3390/nu14030458
Gao Y, Sheng J, Mi X, Zhou M, Zou S, Zhou H. Household Water Access, Dietary Diversity and Nutritional Status among Preschoolers in Poor, Rural Areas of Central and Western China. Nutrients. 2022; 14(3):458. https://doi.org/10.3390/nu14030458
Chicago/Turabian StyleGao, Yaqing, Jie Sheng, Xiaoyi Mi, Mo Zhou, Siyu Zou, and Hong Zhou. 2022. "Household Water Access, Dietary Diversity and Nutritional Status among Preschoolers in Poor, Rural Areas of Central and Western China" Nutrients 14, no. 3: 458. https://doi.org/10.3390/nu14030458
APA StyleGao, Y., Sheng, J., Mi, X., Zhou, M., Zou, S., & Zhou, H. (2022). Household Water Access, Dietary Diversity and Nutritional Status among Preschoolers in Poor, Rural Areas of Central and Western China. Nutrients, 14(3), 458. https://doi.org/10.3390/nu14030458