
Evaluation of Gluten Exclusion for the Improvement of Rheumatoid Arthritis in Adults


Abstract
1. Introduction
1.1. Rheumatoid Arthritis
1.2. Arthritis and Diet
1.3. Arthritis and Gluten
2. Analysis and Methodology
2.1. Information Sources
2.2. Search Strategy
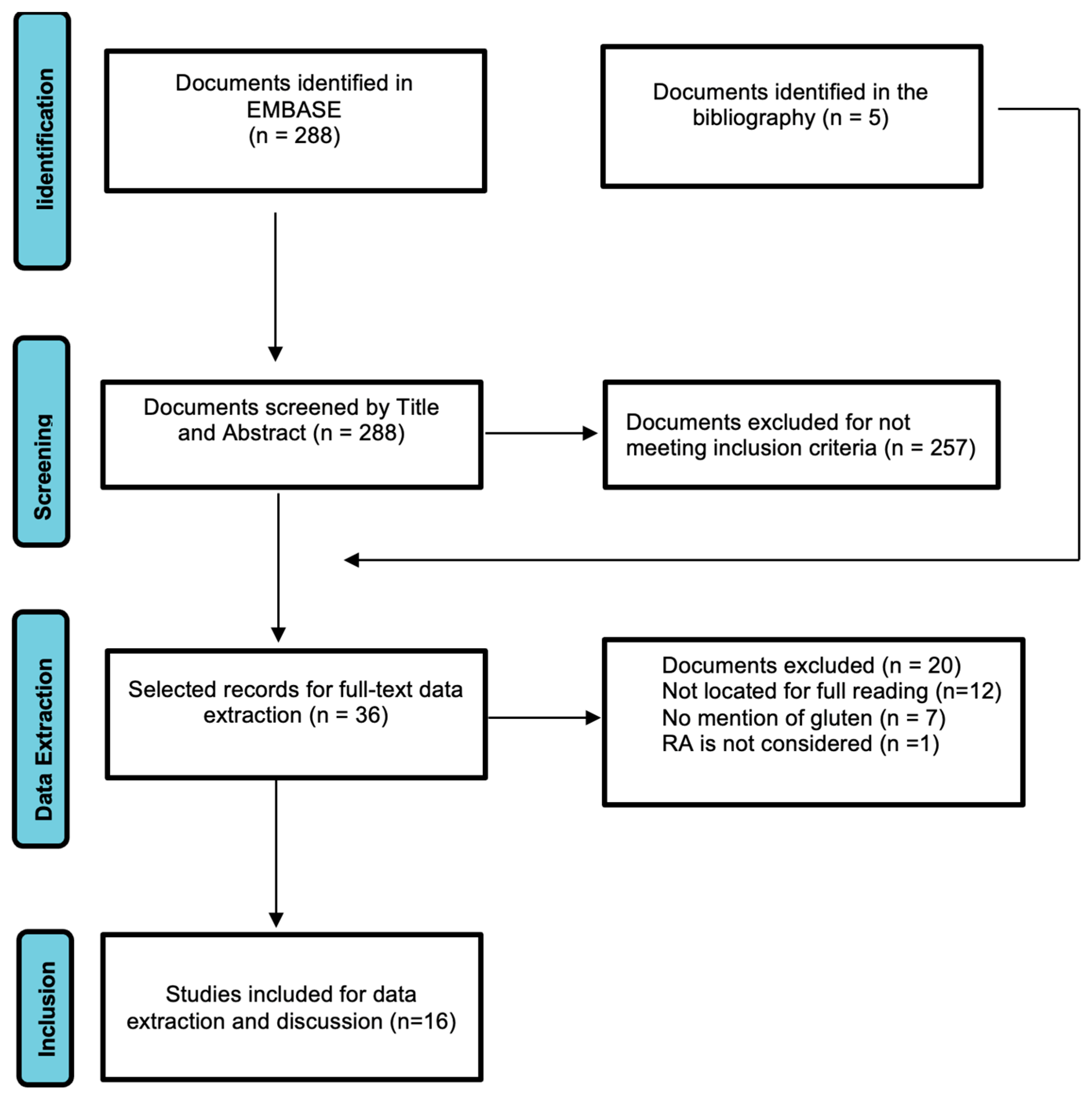
2.3. Selection of Studies
3. Results
4. Discussion
- - The actual role of gluten per se is unknown,
- - That there is no clear indication for eliminating gluten in non-coeliac patients,
- - That the evidence is limited for associating gluten-free diets with benefits in RA,
- - As the gluten-free diet has not been investigated in isolation it is premature to conclude that it has benefits for RA.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- González Cernadas, L.; Rodríguez-Romero, B.; Carballo-Costa, L. Importancia de los Aspectos Nutricionales en el Proceso Inflamatorio de Pacientes con Artritis Reumatoide; una Revisión. Nutr. Hosp. 2014, 29, 237–245. Available online: https://bit.ly/3Pm29mx (accessed on 9 December 2021). [PubMed]
- Conartritis. Coordinadora Nacional de Artritis. Available online: https://bit.ly/31QTTYs (accessed on 9 December 2021).
- Artritis Reumatoide. Arthritis Foundation. Available online: https://bit.ly/3jPoOuc (accessed on 29 October 2021).
- GUIPCAR. Sociedad Española de Reumatología. Available online: https://www.ser.es/guipcar/ (accessed on 9 December 2021).
- Genel, F.; Kale, M.; Pavlovic, N.; Flood, V.M.; Naylor, J.M.; Adie, S. Health effects of a low-inflammatory diet in adults with arthritis: A systematic review and meta-analysis. J. Nutr. Sci. 2020, 9, e37. [Google Scholar] [CrossRef] [PubMed]
- Leitzmann, C. Vegetarian diets: What are the advantages? Forum Nutr. 2005, 57, 147–156. [Google Scholar] [CrossRef]
- Vadell, A.K.E.; Bärebring, L.; Hulander, E.; Gjertsson, I.; Lindqvist, H.M.; Winkvist, A. Anti-inflammatory Diet in Rheumatoid Arthritis (ADIRA)—A randomized, controlled crossover trial indicating effects on disease activity. Am. J. Clin. Nutr. 2020, 111, 1203–1213. [Google Scholar] [CrossRef]
- Osborne, P. No Grain, No Pain. A 30-Day Diet for Eliminating the Root Cause of Chronic Pain; Atria Books: New York, NY, USA, 2016; 352p. [Google Scholar]
- Perlmutter, D.; Loberg, K. Grain Brain: The Surprising Truth about Wheat, Carbs, and Sugar-Your Brain’s Silent Killers; Little, Brown Spark: New York, NY, USA; 384p.
- Carrera, D. Aumento de las Intolerancias Alimentarias, Causas, Diagnóstico y Plan Nutricional. 2018. CEMD. Available online: https://bit.ly/3pR8RHT (accessed on 30 October 2021).
- López Iturriaga, M. La Paranoia Antigluten. El Comidista. Available online: https://bit.ly/33fxnco (accessed on 26 March 2013).
- La Injustificada Moda de la Dieta sin Gluten, BBC News. Available online: https://bbc.in/3IWweXR (accessed on 25 July 2015).
- Levinovitz, A. La Mentira del Gluten y Otros Mitos de la Alimentación; Planeta: Madrid, Spain, 2016; 304p. [Google Scholar]
- Farré, J. Alimentación en Artritis Reumatoide. Available online: https://www.centrojuliafarre.es/dietas/artritis-reumatoide/ (accessed on 30 October 2021).
- Colon, R. 10 Alimentos-Para Evitar-Si Padeces Artritis. AARP. Available online: https://bit.ly/3pVUP7Q (accessed on 30 October 2021).
- Hafstrom, I.; Ringertz, B.; Spångberg, A.; Von Zweigbergk, L.; Brannemark, S.; Nylander, I.; Rönnelid, J.; Laasonen, L.; Klareskog, L. A vegan diet free of gluten improves the signs and symptoms of rheumatoid arthritis: The effects on arthritis correlate with a reduction in antibodies to food antigens. Rheumatology 2001, 40, 1175–1179. [Google Scholar] [CrossRef]
- Siscar, J. Artritis Reumatoide: El Papel de la Dieta. Dietética sin Patrocinadores. Available online: https://bit.ly/3bqV6r1 (accessed on 13 December 2015).
- Drago, S.; El Asmar, R.; Di Pierro, M.; Grazia Clemente, M.; Tripathi, A.; Sapone, A.; Thakar, M.; Iacono, G.; Carroccio, A.; D’Agate, C.; et al. Gliadin, zonulin and gut permeability: Effects on celiac and non-celiac intestinal mucosa and intestinal cell lines. Scand. J. Gastroenterol. 2006, 41, 408–419. [Google Scholar] [CrossRef]
- Pellegrina, C.D.; Perbellini, O.; Scupoli, M.T.; Tomelleri, C.; Zanetti, C.; Zoccatelli, G.; Fusi, M.; Peruffo, A.; Rizzi, C.; Chignola, R. Effects of wheat germ agglutinin on human gastrointestinal epithelium: Insights from an experimental model of immune/epithelial cell interaction. Toxicol. Appl. Pharmacol. 2009, 237, 146–153. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 81, 19–32. [Google Scholar] [CrossRef]
- Perdiguero Gil, E. El Proceso de Búsqueda y Recuperación de la Información. FUOC. PID_00154919. Available online: https://bit.ly/3PyzHzr (accessed on 9 December 2022).
- Bonich, M.; Cervera, A.; Santos, G. Cómo Hay Que Iniciar una Búsqueda. CC-BY-SA. PID_00168881. Available online: https://bit.ly/3WbM2w2 (accessed on 9 December 2022).
- Atkinson, L.Z.; Cipriani, A. How to carry a literature search for a systematic review: A practical guide. BJPsych Adv. 2018, 24, 74–82. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomized or non-randomised studies of healthcare interventions or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Ciapponi, A. AMSTAR-2: Herramienta de Evaluación Crítica de Revisiones Sistemáticas de Estudios de Intervenciones de Salud. Evid. Actual. Pract. Ambul. 2018, 21, 4–13. Available online: https://www.evidencia.org.ar/index.php/Evidencia/article/view/6834 (accessed on 29 December 2021). [CrossRef]
- Kjeldsen-Kragh, J.; Borchgrevink, C.; Laerum, E.; Haugen, M.; Eek, M.; Førre, O.; Mowinkel, P.; Hovi, K. Controlled trial of fasting and one-year vegetarian diet in rheumatoid arthritis. Lancet 1991, 338, 899–902. [Google Scholar] [CrossRef]
- Haugen, M.A.; Kjeldsen-Kragh, J.; Skakkebæk, N.; Landaas, S.; Sjaastad, Ø.; Movinkel, P.; Førre, Ø. The Influence of fast and vegetarian diet on parameters of nutritional status in patients with rheumatoid arthritis. Clin. Rheumatol. 1993, 12, 62–69. [Google Scholar] [CrossRef]
- Kjeldsen-Kragh, J. Rheumatoid arthritis treated with vegetarian diets. Am. J. Clin. Nutr. 1999, 70, 594s–600s. [Google Scholar] [CrossRef]
- Elkan, A.-C.; Sjöberg, B.; Kolsrud, B.; Ringertz, B.; Hafström, I.; Frostegård, J. Gluten-free vegan diet induces decreased LDL and oxidized LDL levels and raised atheroprotective natural antibodies against phosphorylcholine in patients with rheumatoid arthritis: A randomized study. Arthritis Res. Ther. 2008, 10, R34. [Google Scholar] [CrossRef]
- Lidén, M.; Kristjánsson, G.; Valtysdottir, S.; Venge, P.; Hällgren, R. Self-reported food intolerance and mucosal reactivity after rectal food protein challenge in patients with rheumatoid arthritis. Scand. J. Rheumatol. 2010, 39, 292–298. [Google Scholar] [CrossRef]
- Hagen, K.B.; Byfuglien, M.G.; Falzon, L.; Olsen, S.U.; Smedslund, G. Dietary interventions for rheumatoid arthritis. Ochrane Database Syst. Rev. 2009, CD006400. [Google Scholar] [CrossRef]
- El-Chammas, K.; Danner, E. Gluten-free diet in nonceliac disease. Nutr. Clin. Pract. 2011, 26, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.; Shoenfeld, Y.; Matthias, T. Adverse effects of gluten ingestion and advantages of gluten withdrawal in nonceliac autoimmune disease. Nutr. Rev. 2017, 75, 1046–1058. [Google Scholar] [CrossRef]
- Badsha, H. Role of Diet in Influencing Rheumatoid Arthritis Disease Activity. Open Rheumatol. J. 2018, 12, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Vijayalakshmi, S.; Kripa, K.G. Dietary Approaches in the Management of Rheumatoid Arthritis-A Review. IJRPS 2018, 9, 958–964. Available online: https://pharmascope.org/index.php/ijrps/article/view/348 (accessed on 9 December 2021).
- Lerner, B.A.; Green, P.H.R.; Lebwohl, B. Going Against the Grains: Gluten-Free Diets in Patients Without Celiac Disease-Worthwhile or Not? Dig. Dis. Sci. 2019, 64, 1740–1747. [Google Scholar] [CrossRef] [PubMed]
- Bruzzese, V.; Scolieri, P.; Pepe, J. Efficacy of gluten-free diet in patients with rheumatoid arthritis. Reumatismo 2021, 72, 213–217. [Google Scholar] [CrossRef]
- Rondanelli, M.; Perdoni, F.; Peroni, G.; Caporali, R.; Gasparri, C.; Riva, A.; Petrangolini, G.; Faliva, M.A.; Infantino, V.; Naso, M.; et al. Ideal food pyramid for patients with rheumatoid arthritis: A narrative review. Clin. Nutr. 2021, 40, 661–689. [Google Scholar] [CrossRef]
- Guagnano, M.T.; D’Angelo, C.; Caniglia, D.; Di Giovanni, P.; Celletti, E.; Sabatini, E.; Speranza, L.; Bucci, M.; Cipollone, F.; Paganelli, R. Improvement of Inflammation and Pain after Three Months’ Exclusion Diet in Rheumatoid Arthritis Patients. Nutrients 2021, 13, 3535. [Google Scholar] [CrossRef]
- Jiang, Y.; Jarr, K.; Layton, C.; Gardner, C.; Ashouri, J.; Abreu, M.; Sinha, S. Therapeutic Implications of Diet in Inflammatory Bowel Disease and Related Immune-Mediated Inflammatory Diseases. Nutrients 2021, 13, 890. [Google Scholar] [CrossRef]
- Smedslund, G.; Byfuglien, M.G.; Olsen, S.U.; Hagen, K.B. Effectiveness and safety of dietary interventions for rheumatoid arthritis: A systematic review of randomized controlled trials. J. Am. Diet. Assoc. 2010, 110, 727–735. [Google Scholar] [CrossRef]
- Aho, K.; Heliövaara, M. Risk factors for rheumatoid arthritis. Ann. Med. 2004, 36, 242–251. [Google Scholar] [CrossRef]
- Lerner, A.; Matthias, T. Rheumatoid arthritis-celiac disease relationship: Joints get that gut feeling. Autoimmun. Rev. 2015, 14, 1038–1047. [Google Scholar] [CrossRef]
- Lerner, A.; Wusterhausen, P.; Ramesh, A.; Lopez, F.; Matthias, T. The gut feeling of the joints: Celiac disease and rheumatoid arthritis are related. Int. J. Celiac Dis. 2019, 7, 21–25. [Google Scholar] [CrossRef]
- Coenen, M.J.; Trynka, G.; Heskamp, S.; Franke, B.; Van Diemen, C.C.; Smolonska, J.; Van Leeuwen, M.; Brouwer, E.; Boezen, M.H.; Postma, D.S.; et al. Common and different genetic background for rheumatoid arthritis and coeliac disease. Hum. Mol. Genet. 2009, 18, 4195–4203. [Google Scholar] [CrossRef]
- Losurdo, G.; Principi, M.; Iannone, A.; Amoruso, A.; Ierardi, E.; Di Leo, A.; Barone, M. Extra-intestinal manifestations of non-celiac gluten sensitivity: An expanding paradigm. World J. Gastroenterol. 2018, 24, 1521–1530. [Google Scholar] [CrossRef]
- San Mauro, I.; Garicano, E.; Collado, L.; Ciudad, M.J. ¿Es el gluten el gran agente etiopatogénico de enfermedad en el siglo XXI? Nutr. Hosp. 2014, 30, 1203–1210. [Google Scholar] [CrossRef]
- Palmieri, B.; Vadala, M.; Laurino, C. Gluten-free diet in non-celiac patients: Beliefs, truths, advantages and disadvantages [Abstract]. Minerva Gastroenterol. Dietol. 2019, 65, 153–162. [Google Scholar] [CrossRef]
- El Khoury, D.; Balfour-Ducharme, S.; Joye, I.J. A Review on the Gluten-Free Diet: Technological and Nutritional Challenges. Nutrients 2018, 10, 1410. [Google Scholar] [CrossRef]
- Gaesser, G.A.; Angadi, S.S. Gluten-free diet: Imprudent dietary advice for the general population? J. Acad. Nutr. Diet. 2012, 112, 1330–1333. [Google Scholar] [CrossRef]


{kind=link}
| Population | Adults with Diagnosed Rheumatoid Arthritis |
|---|---|
| Intervention/Exposure factor | Exclusion of gluten from the diet for the improvement of symptomatology. |
| Comparator | Adults with gluten-free diets. |
| Patient-centered “Outcomes” of interest | Observation of improvements in arthritis symptomatology experienced by patients following dietary changes. |
| Type of design | Systematic reviews, meta-analyses, randomised controlled trials, randomised controlled trials, cohort studies, case-control studies, case-control studies |
| Evaluation of Gluten Exclusion for the Improvement of Rheumatoid Arthritis in Adults | ||||||
|---|---|---|---|---|---|---|
| ELIGIBILITY CRITERIA: screening according to information available in title and/or abstract and study design | ||||||
| Is the elimination of gluten from the diet a factor of improvement in the painful symptomatology of rheumatoid arthritis in adults versus non-elimination? | ||||||
| What is the relationship between gluten consumption and the development of rheumatoid arthritis? | ||||||
| Is non-coeliac gluten sensitivity associated with the development or progression of rheumatoid arthritis? | ||||||
| INFORMATION | YES | NO | ||||
| Specifically rheumatoid arthritis and gluten are discussed. | √ | |||||
| Other arthritis is considered but not rheumatoid arthritis. | √ | |||||
| Other arthritis in addition to rheumatoid arthritis is considered to include | √ | |||||
| Diets in general are discussed without specifying gluten. | √ | |||||
| Coeliac disease and/or gluten sensitivity is treated but not arthritis. | √ | |||||
| Gluten sensitivity and arthritis treated | √ | |||||
| Patients are not adults | √ | |||||
| DESIGN | YES | NO | ||||
| Human studies | ||||||
| Meta-analysis | √ | |||||
| Systematic Review | √ | |||||
| Observational Studies | Report and case series | √ | ||||
| Transversal | √ | |||||
| Population | √ | |||||
| Cases and controls | √ | |||||
| Cohorts | √ | |||||
| Experimental Trials | Randomised, blinded | √ | ||||
| Randomised, double-blind | √ | |||||
| Non-randomised | √ | |||||
| Animal studies (laboratory) | √ | |||||
| “In vitro” studies | √ | |||||
The Summary will be ACCEPTED if:
| ||||||
| Information | ||||||
| SI | NO | REVIEW | ||||
| Design | ||||||
| SI | ACCEPT | REJECT | ACCEPT | |||
| NO | REJECT | REJECT | ||||
| REVIEW | ACCEPT | ACCEPT | ||||
| Author Year | Population (n) Duration * Type of Study | Intervention * vs. Control | Diet | Variables | Results |
|---|---|---|---|---|---|
| Kjeldsen-Kragh et al. 1991 [27] | n = 53 13 months ECASC | Fasting (7–10 days) + DVSG (3–5 months) + DV Vs. DMO | A: herbal teas, garlic, vegetable broths, potato and parsley decoction, carrot juice, beetroot, celery. DVSG: A + introduction of gluten-free plant-based foods. DV: DVSG + dairy and gluten free DMO: not specified | Pain, duration morning stiffness, personal feeling of condition vs. initial condition, no. painful joints, swollen, grip strength, Hb, platelets, ESR, white blood cells, CRP, serum albumin | A total of 34 patients finished Significant improvements in IG for all variables except platelets and Hb. Radiographic deterioration occurred in both groups with no differences between them. >weight loss, ↓Hb and some nutritional deficiencies in GI |
| Hagen et al. 1993 [28] | n = 53 13 months ECASC | Fasting (7–10 days) + DVSG (3–5 months) + DV Vs. DMO | A: herbal teas, garlic, vegetable broths, potato and parsley decoction, carrot juice, beetroot, celery. DVSG: A+introduction of gluten-free plant-based foods. DV: DVSG+ dairy and gluten free DMO: not specified | Weight, height, upper arm circumference, PCT, BMI, Hb, albumin, Cu, Zn, ferritin, IGF1, tryptophan | For anthropometric measurements, the two groups are not compared. For analytical variables no differences were detected between the groups. A low energy and protein intake was detected in the intervention group, with a decrease in anthropometric measurements. Patients found it difficult to follow the gluten-free vegan period. |
| Kjeldsen-Kragh 1999 [29] | n = 53 13 months ECASC | Fasting (7–10 days) + DVSG (3–5 months) + DV Vs. DMO | A: herbal teas, garlic, vegetable broths, potato and parsley decoction, carrot juice, beetroot, celery. DVSG: A + introduction of gluten-free plant-based foods. DV: DVSG + dairy and gluten free DMO: not specified | Pain, duration of morning stiffness, personal feeling of condition vs. baseline, no. painful joints, swollen, grip strength, weight, Hb, platelets, ESR, white blood cells, CRP, serum albumin, fatty ac., IgG P. mirabilis, faecal flora | Possible placebo effect on DV. The data do not indicate that systemic immune reactions against food antigens were significant in most patients. The clinical effects of VD do not appear to be due to changes in eicosanoid precursors. Possible stimulation of the immune system by Proteus antigens. Changes in faecal flora possibly leading to differences in the absorption of substances which in turn influence inflammatory processes in the joints. |
| Hafström et al. 2001 [16] | n = 66 12 months ECASC | DVSG (n = 38) Vs. DE (n = 28) | DVSG: Vegetables, dried and fresh fruits and nuts, maize, rice, sunflower seeds, buckwheat, millet DE: variety of food from all food groups | Patient status ACR Food antibodies (IgG, IgA against gliadin and β-lactoglobulin) X-rays | According to the ACR, in the DVSGs there is improvement in all indicators except CRP; in the EDs, improvement is observed only in joint swelling and global physical condition. Decreases Ig in DVSG (but only in dietary responders) No difference in radiological progression |
| Elkan et al. 2008 [30] | n = 66 12 months ECASC | DVSG (n = 38) Vs. DE (n = 28) | DVSG: Vegetables, dried and fresh fruits and nuts, maize, rice, sunflower seeds, buckwheat, millet DE: variety of food from all food groups | BMI, DAS28, physical fitness, ESR, CRP, Hb, WBC, serum albumin, total cholesterol, LDL, HDL, TG, OxLDL, anti-CCP | BMI, weight, LDL < at DVSG Anti-PC Ig M > DVSG Increases Anti-PC Ig A ↓ OxLDL (trend) DVSG DAS28 > DE |
| Lidén et al. 2010 [31] | n = 241 EP | Perceived personal connection between food and different symptoms | --- | Intestinal, urticaria, itching, eczema, dyspnoea, rhinitis, anaphylaxis, fatigue, joint and muscle symptoms, etc. | Overall, 27% of patients reported food intolerances, mainly to cow’s milk (34%) and meat (33%); wheat ranked 5th (17–5% of all respondents). |
| n = 45 CCT | AR (n = 27) Vs. no AR (n = 18) | Rectal exposure to milk and gluten | MPO, ECP, NO IgA + IgG antibodies against casein, β-lactoglobulin, α-lactoalbumin, gliadin, transglutaminase | No increase in MPO, DBS, NO after the intervention. Similar antibody levels in the two groups. Mucosal sensitivity to gliadin only seen in a minority group of RA patients. | |
| Hagen et al. 2010 [32] | RS n = 837 15 studies (RCT–CCT) | --- | A, DMO, DVSG, DV, MD, ED, eD | Pain, functional status, joint stiffness, fatigue, weight loss, gastrointestinal symptoms, sick leave, quality of life | There is no certainty that diets improve pain, stiffness and the ability to move better. |
| El-Chammas et al. 2011 [33] | RB | --- | For AR refer to [33,34] | Cholesterol, anti-IgA, anti-IgM, anti-PC | The actual role of gluten per se is unknown ↓in the activity and levels of antibodies to β-lactoglobulin, and gliadin |
| Lerner et al. 2017 [34] | RB | --- | For AR refer to [33,34] | Immunogenicity, pathogenicity, intestinal permeability, microbiome, oxidative stress, epigenetic programming, cellular metabolism, cognitive function | There is no clear indication for eliminating gluten in non-coeliac patients. Human clinical studies are needed |
| Badsha 2018 [35] | RB | --- | MD, flavonoids/isoflavones, gluten, eD, DV, ED, polyunsaturated fatty acids, probiotics, alcohol, vitamins, supplements, antioxidants, A, obesity | --- | Limited evidence to link gluten-free diets to benefits in RA |
| Vijayalakshmi et al. 2018 [36] | RB | --- | DAO, DAI, DVSG, DVSG, eD, MD, ED, DE, supplementation | Refer to [33] | DVSG may be beneficial for some patients as indicated by Hafström et al. 2001 [16]. |
| Lerner et al. 2019 [37] | RB | --- | Refer to [30,33,34,36] | Refer to [30,33,34,36] | As the gluten-free diet has not been investigated in isolation for this nutrient it is premature to conclude that it has beneficial effects on RA. |
| Bruzzese et al. 2020 [38] | n = 4 10 days-10 months EC | DSG in patients with RA (no control) | Not described | DAS28 | Case 1: improvement observed at 1 month, 5 and 10 months Case 2: improvement observed after one month, but patient stops the diet after three months. Case 3: improvement observed after one month, but patient stops the diet. Case 4: after 10 days, improvement is observed. |
| Rondanelli et al. 2020 [39] | RB | --- | They refer to studies analyzing the intake of potatoes, free sugars, and the recommendation of the DGA as healthy foods (fruits, vegetables, whole grains, nuts, fatty acids). | --- | For carbohydrates, three servings per day of whole grains, preferably gluten-free, are recommended. Exclusion of sugars from the diet. |
| Guagnano et al. 2021 [40] | n = 40 3 months RCT | ED Vs. MD | ED = Mediterranean type excluding meat, gluten and dairy products Standard Mediterranean diet, without red meat | DAS28, HAQ, VAS, glucose, insulin, cholesterol, ESR, CRP, transaminases, total protein, albumin, transferrin, cytokines, adipokines, BMI, blood pressure, BIA | Results limited to 28 patients because 12 drop out before 3 months. Differences in VAS and HAQ for ED group pre-post diet; no differences in DAS28. No inter-group comparison. In anthropometric measurements, intergroup differences were only observed for muscle mass, water and systolic pressure. For analytics there are no inter-group differences. For cytokines and adipokines, without intergroup comparison, there is variation only for leptin in each of the two groups. |
| Jiang et al. 2021 [41] | RB | --- | MD, DV, DSG, A, | --- | Refer to results of [16,27]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lidón, A.-C.; Patricia, M.-L.; Vinesh, D.; Marta, M.-S. Evaluation of Gluten Exclusion for the Improvement of Rheumatoid Arthritis in Adults. Nutrients 2022, 14, 5396. https://doi.org/10.3390/nu14245396
Lidón A-C, Patricia M-L, Vinesh D, Marta M-S. Evaluation of Gluten Exclusion for the Improvement of Rheumatoid Arthritis in Adults. Nutrients. 2022; 14(24):5396. https://doi.org/10.3390/nu14245396
Chicago/Turabian StyleLidón, Avinent-Calpe, Martinez-López Patricia, Dhokia Vinesh, and Massip-Salcedo Marta. 2022. "Evaluation of Gluten Exclusion for the Improvement of Rheumatoid Arthritis in Adults" Nutrients 14, no. 24: 5396. https://doi.org/10.3390/nu14245396
APA StyleLidón, A.-C., Patricia, M.-L., Vinesh, D., & Marta, M.-S. (2022). Evaluation of Gluten Exclusion for the Improvement of Rheumatoid Arthritis in Adults. Nutrients, 14(24), 5396. https://doi.org/10.3390/nu14245396