



Medium-Chain Fatty Acids and Breast Cancer Risk by Receptor and Pathological Subtypes
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection of Subjects
2.2. Estimation of Lipid Profiles
2.3. Medium-Chain Fatty Acid Analysis
3. Statistical Analysis
4. Results
4.1. General Characteristics of the Study Population
4.2. Comparison of Biochemical Parameters in the Study Population
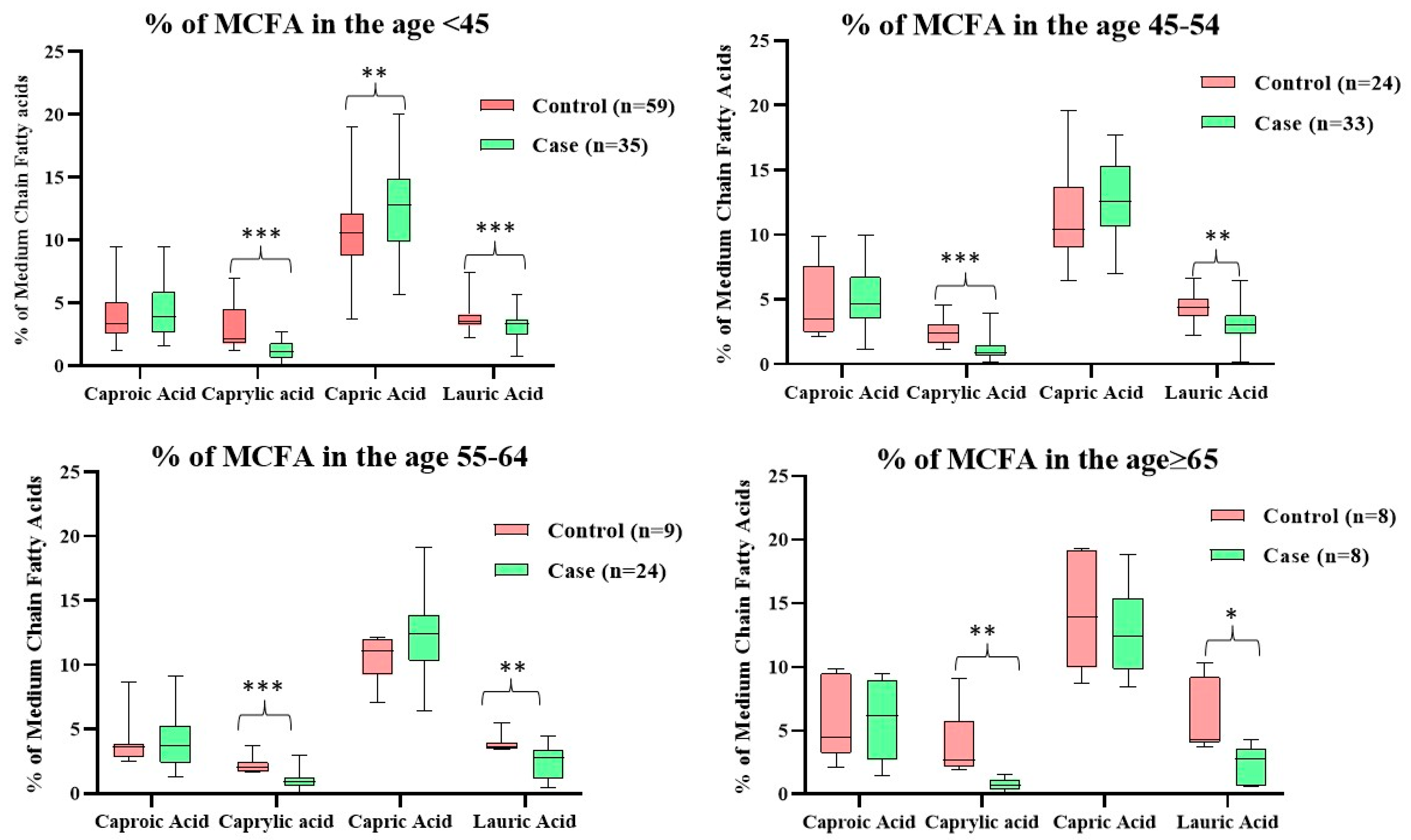
4.3. Age-Wise Distribution of MCFA Levels in the Study Population
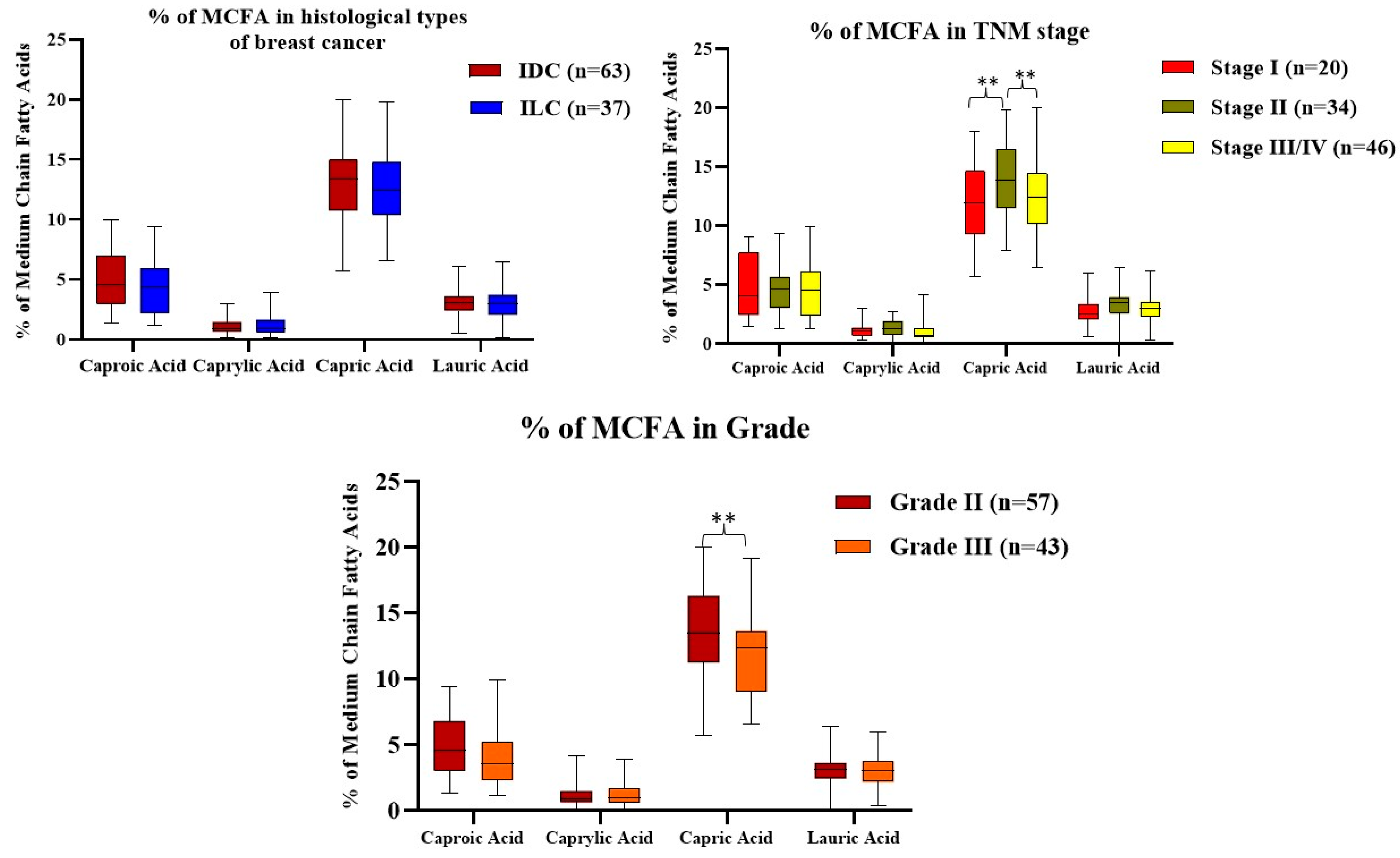
4.4. Comparison of MCFA Levels Regarding Histological Types, TNM Stage, and Grade of Breast Cancer Subjects
4.5. Distribution of MCFAs Levels with Respect to the Receptor Status of the Breast Cancer Subjects
4.6. Correlation between Hematological Parameters, Lipid Profile, Kidney Function Test, Liver Function Test, and Medium-Chain Fatty Acids in Breast Cancer
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjo Mataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenwald, P. Role of dietary fat in the causation of breast cancer: Point. Cancer Epidemiol. Biomark. Prev. 1999, 8, 3–7. [Google Scholar]
- Cottet, V.; Vaysse, C.; Scherrer, M.L.; Ortega-Deballon, P.; Lakkis, Z.; Delhorme, J.B.; Deguelte-Lardiere, S.; Combe, N.; Bonithon-Kopp, C. Fatty acid composition of adipose tissue and colorectal cancer: A case-control study. Am. J. Clin. Nutr. 2015, 101, 192–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenyon, M.A.; Hamilton, J.A. 13C NMR studies of the binding of medium-chain fatty acids to human serum albumin. J. Lipid Res. 1994, 35, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Vorum, H.; Pedersen, A.; Honoré, B. Fatty acid and drug binding to a low-affinity component of human serum albumin, purified by affinity chromatography. Int. J. Pept. Protein Res. 1992, 40, 415–422. [Google Scholar] [CrossRef]
- Nagao, K.; Yanagita, T. Medium-chain fatty acids: Functional lipids for the prevention and treatment of the metabolic syndrome. Pharmacol. Res. 2010, 61, 208–212. [Google Scholar] [CrossRef]
- Sheela, D.L.; Narayanankutty, A.; Nazeem, P.A.; Raghavamenon, A.C.; Muthangaparambil, S.R. Lauric acid induce cell death in colon cancer cells mediated by the epidermal growth factor receptor downregulation: An in silico and in vitro study. Hum. Exp. Toxicol. 2019, 38, 753–761. [Google Scholar] [CrossRef]
- Crotti, S.; Agnoletto, E.; Cancemi, G.; di Marco, V.; Traldi, P.; Pucciarelli, S.; Nitti, D.; Agostini, M. Altered plasma levels of decanoic acid in colorectal cancer as a new diagnostic biomarker. Anal. Bioanal. Chem. 2016, 408, 6321–6328. [Google Scholar] [CrossRef]
- Krauss-Etschmann, S.; Shadid, R.; Campoy, C.; Hoster, E.; Demmelmair, H.; Jiménez, M.; Gil, A.; Rivero, M.; Veszprémi, B.; Decsi, T.; et al. Effects of fish-oil and folate supplementation of pregnant women on maternal and fetal plasma concentrations of docosahexaenoic acid and eicosapentaenoic acid: A European randomized multicenter trial. Am. J. Clin. Nutr. 2007, 85, 1392–1400. [Google Scholar]
- Buege, J.A.; Aust, S.D. Microsomal lipid peroxidation. Methods Enzymol. 1978, 52, 302–310. [Google Scholar]
- Metcalfe, L.D.; Schmitz, A.A.; Pelka, J.R. Preparation of fatty acid esters from lipids for gas chromatography. Anal. Chem. 1966, 38, 514–515. [Google Scholar] [CrossRef]
- Ray, G.; Husain, S.A. Role of lipids, lipoproteins and vitamins in women with breast cancer. Clin. Biochem. 2001, 34, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K.; Sachdanandam, P.; Arivazhagan, R. Studies on the changes in plasma lipids and lipoproteins in patients with benign and malignant breast cancer. Biochem. Int. 1991, 23, 581–589. [Google Scholar] [PubMed]
- Thangaraju, M.; Rameshbabu, J.; Vasavi, H.; Ilanchezhian, S.; Vinitha, S.; Sachdanandam, P. The salubrious effect of tamaxifen on serum marker enzymes, glycoproteins, and lysosomal enzymes level in breast cancer women. Mol. Cell. Biochem. 1998, 185, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Fatima, T.; Roohi, N.; Abid, R. Circulatory Proteins in Women with Breast Cancer and their Chemotherapeutic Responses. Pak. J. Zool. 2013, 45, 1207–1213. [Google Scholar]
- Lis, C.G.; Grutsch, J.F.; Vashi, P.G.; Lammersfeld, C.A. Is serum albumin an independent predictor of survival in patients with breast cancer? J. Parenter. Enter. Nutr. 2003, 27, 10–15. [Google Scholar] [CrossRef]
- Wheler, J.; Tsimberidou, A.M.; Moulder, S.; Cristofanilli Mong, D.; Naing, A.; Pathak, R.; Liu, S.; Feng, L.; Kurzrock, R. Clinical outcomes of patients with breast cancer in a phase I clinic: The MD Anderson cancer center experience. Clin. Breast Cancer 2010, 10, 46–51. [Google Scholar] [CrossRef]
- Devi, L.I.; Ralte, L.; Ali, M.A. Serum Biochemical Profile of Breast cancer patients. Eur. J. Pharm. Med. Res. 2015, 2, 210–214. [Google Scholar]
- Brunello, A.; Kapoor, R.; Extermann, M. Hyperglycemia during chemotherapy for hematologic and solid tumors is correlated with increased toxicity. Am. J. Clin. Oncol. Cancer Clin. Trials 2011, 34, 292–296. [Google Scholar] [CrossRef]
- Fares, M.S.M.; Karuppannan, M.; Abdulrahman, E.; Suriyon Uitrakul, B.A.H.R.; Mohammed, A.H. Prevalence and associated factors of anemia among breast cancer patients undergoing chemotherapy: A prospective study. Adv. Pharmacol. Pharm. Sci. 2022, 2022, 7611733. [Google Scholar]
- Guillot, E.; Vaugelade, P.; Lemarchali, P.; Rat, A.R. Intestinal absorption, and liver uptake of medium-chain fatty acids in non-anaesthetized pigs. Br. J. Nutr. 1993, 69, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Papamandjaris, A.A.; Macdougall, D.E.; Jones, P.J. Medium chain fatty acid metabolism and energy expenditure: Obesity treatment implications. Life Sci. 1998, 62, 1203–1215. [Google Scholar] [CrossRef]
- Lieber, C.S.; Lefèvre, A.; Spritz, N.; Feinman, L.; DeCarli, L.M. Difference in Hepatic Metabolism of Long- and Medium-Chain Fatty Acids: The Role of Fatty Acid Chain Length in the Production of the Alcoholic Fatty Liver. J. Clin. Investig. 1967, 46, 1451–1460. [Google Scholar] [CrossRef] [Green Version]
- Saerens, S.M.G.; Verstrepen, K.; Van Laere, S.D.M.; Voet, A.; Van Dijck, P.; Delvaux, F.R.; Thevelein, J. The Saccharomyces cerevisiae EHT1 and EEB1 Genes Encode Novel Enzymes with Medium-chain Fatty Acid Ethyl Ester Synthesis and Hydrolysis Capacity. J. Biol. Chem. 2006, 281, 4446–4456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddy, M.V.; Mohan, S.V.; Chang, Y.-C. Sustainable production of medium chain fatty acids (MCFA) with an enriched mixed bacterial culture: Microbial characterization using molecular methods. Sustain. Energy Fuels 2018, 2, 372–380. [Google Scholar] [CrossRef]
- Diender, M.; Stams, A.J.M.; Sousa, D.Z. Production of medium-chain fatty acids and higher alcohols by a synthetic co-culture grown on carbon monoxide or syngas. Biotechnol. Biofuels 2016, 9, 82. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.M.; Kim, B.W.; Franke, A.A.; Roberts, J.D. 13C NMR studies of butyric fermentation in Clostridium kluyveri. J. Biol. Chem. 1985, 260, 13509–13512. [Google Scholar] [CrossRef]
- Weimer, P.J.; Stevenson, D.M. Isolation, characterization, and quantification of Clostridium kluyveri from the bovine rumen. Appl. Microbiol. Biotechnol. 2012, 94, 461–466. [Google Scholar] [CrossRef]
- Kenealy, W.R.; Cao, Y.; Weimer, P.J. Production of caproic acid by cocultures of ruminal cellulolytic bacteria a and Clostridium kluyveri grown on cellulose and ethanol. Appl. Microbiol. Biotechnol. 1995, 44, 507–513. [Google Scholar] [CrossRef]
- Amalaradjou, M.A.R.; Annamalai, T.; Marek, P.; Rezamand, P.; Schreiber, D.; Hoagland, T.; Venkitanarayanan, K. Inactivation of Escherichia coli O157:H7 in Cattle Drinking Water by Sodium Caprylate. J. Food 2006, 69, 2248–2252. [Google Scholar] [CrossRef]
- Valipe, S.R.; Nadeau, J.A.; Annamali, T.; Venkitanarayanan, K.; Hoagland, T. In vitro antimicrobial properties of caprylic acid, monocaprylin, and sodium caprylate against Dermatophilus congolensis. Am. J. Vet. Res. 2011, 72, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Lemarié, F.; Beauchamp, E.; Legrand, P.; Rioux, V. Revisiting the metabolism and physiological functions of caprylic acid (C8:0) with special focus on ghrelin octanoylation. Biochimie 2016, 120, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Roopashree, P.G.; Shilpa Shetty, S.; Suchetha Kumari, N. Effect of medium chain fatty acid in human health and disease. J. Funct. Foods 2021, 87, 104724. [Google Scholar] [CrossRef]
- Kadochi, Y.; Mori, S.; Fujiwara-Tani, R.; Luo, Y.; Nishiguchi, Y.; Kishi, S.; Fujii, K.; Ohmori, H.; Kuniyasu, H. Remodeling of energy metabolism by a ketone body and medium-chain fatty acid suppressed the proliferation of CT26 mouse colon cancer cells. Oncol. Lett. 2017, 14, 673–680. [Google Scholar] [CrossRef] [Green Version]
- Tiuca, I.D.; Nagy, K.; Oprean, R. Development and optimization of a gaschromatographic separation method of fatty acids in human serum. World J. Pharm. Sci. 2015, 3, 1713–1719. [Google Scholar]
- Zhang, X.; Zhang, P.; Liu, Y.; Xu, Q.; Zhang, Y.; Li, H.; Liu, L.; Liu, Y.; Yang, X.; Xue, C. Caprylic Acid Improves Lipid Metabolism, Suppresses the Inflammatory Response and Activates the ABCA1/p-JAK2/pSTAT3 Signaling Pathway in C57BL/6J Mice and RAW264.7 Cells. Biomed. Environ. Sci. 2022, 35, 95–106. [Google Scholar]
- Yamasaki, M.; Soda, S.; Sakakibara, Y.; Suiko, M.; Nishiyama, K. The importance of 1,2-dithiolane structure in α-lipoic acid for the downregulation of cell surface β1-integrin expression of human bladder cancer cells. Biosci. Biotechnol. Biochem. 2014, 78, 1939–1942. [Google Scholar] [CrossRef] [Green Version]
- Jansen, R.J.; Robinson, D.P.; Frank, R.D.; Anderson, K.E.; Bamlet, W.R.; Oberg, A.L.; Rabe, K.G.; Olson, J.E.; Sinha, R.; Petersen, G.M.; et al. Fatty acids found in dairy, protein and unsaturated fatty acids are associated with risk of pancreatic cancer in a case–control study. Int. J. Cancer 2014, 134, 1935–1946. [Google Scholar] [CrossRef]
- Wang, C.; Wang, J.; Chen, K.; Pang, H.; Li, X.; Zhu, J.; Ma, Y.; Qiu, T.; Li, W.; Xie, J.; et al. Caprylic acid (C8:0) promotes bone metastasis of prostate cancer by dysregulated adi-po-osteogenic balance in bone marrow. Cancer Sci. 2020, 111, 3600–3612. [Google Scholar] [CrossRef]
- Iemoto, T.; Nishiumi, S.; Kobayashi, T.; Fujigaki, S.; Hamaguchi, T.; Kato, K.; Shoji, H.; Matsumura, Y.; Honda, K.; Yoshida, M. Serum level of octanoic acid predicts the efficacy of chemotherapy for colorectal cancer. Oncol. Lett. 2019, 17, 831–842. [Google Scholar] [CrossRef]
- Lappano, R.; Sebastiani, A.; Cirillo, F.; Rigiracciolo, D.C.; Galli, G.R.; Curcio, R.; Malaguarnera, R.; Belfiore, A.; Cappello, A.R.; Maggiolini, M. The lauric acid-activated signaling prompts apoptosis in cancer cells. Cell Death Discov. 2017, 3, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gukas, I.D.; Jennings, B.A.; Mandong, B.M.; Manasseh, A.N.; Harvey, I.; Leinster, S.J. A comparison of the pattern of occurrence of breast cancer in Nigerian and British women. Breast 2006, 15, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Robinson, D.; Bell, J.; Møller, H.; Salman, A. A 13-year follow-up of patients with breast cancer presenting to a District General Hospital breast unit in southeast England. Breast 2006, 15, 173–180. [Google Scholar] [CrossRef]
- Mirtavoos-Mahyari, H.; Khosravi, A.; Esfahani-Monfared, Z. Human epidermal growth factor receptor 2 and estrogen receptor status in respect to tumor characteristics in non-metastatic breast cancer. Tanaffos 2014, 13, 26–34. [Google Scholar] [PubMed]
- Hasiniatsy, N.R.; Vololonantenaina, C.R.; Rabarikoto, H.F.; Razafimanjato, N.; Ranoharison, H.D.; Rakotoson, J.L.; Samison, L.H.; Rafaramino, F. First results of hormone receptors’ status in Malagasy women with invasive breast cancer. Pan Afr. Med. J. 2014, 17, 153. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Control (n = 100) | Case (n = 100) | p Value |
|---|---|---|---|
| Age | |||
| Total | 46.731 ± 10.846 | 50.04 ± 10.611 | <0.04 * |
| <45 | 59 | 35 | 0.072 |
| 45–54 | 24 | 33 | |
| 55–64 | 9 | 24 | |
| ≥65 | 8 | 8 | |
| BMI | |||
| Total | 21.232 ± 2.870 | 22.117 ± 3.448 | <0.001 ** |
| <18.5 | 3 | 2 | 0.050 |
| 18.5–24.9 | 70 | 58 | |
| ≥25 | 27 | 40 | |
| Menopausal status (%) | |||
| Pre-menopausal | 52 | 31 | 0.072 |
| Post-menopausal | 48 | 69 | |
| First-degree family history (%) | |||
| Yes | 2 | 11 | <0.040 * |
| No | 98 | 89 | |
| Diet (%) | |||
| Mixed | 87 | 85 | 0.833 |
| Vegetarian | 13 | 15 | |
| Tumor Characteristics | Invasive Ductal Carcinoma n (%) (n = 63) | Invasive Lobular Carcinoma n (%) (n = 37) | p Value |
|---|---|---|---|
| TNM Stage | |||
| I | 11 (18) | 9 (24) | 0.477 |
| II | 24 (38) | 10 (27) | |
| III/IV | 28 (44) | 18 (49) | |
| Tumor size (cm) | |||
| <2.0 | 16 (25) | 16 (43) | 0.105 |
| 2.0–4.9 | 20 (32) | 6 (16) | |
| ≥5.0 | 27 (43) | 15 (41) | |
| Lymph Node status | |||
| Positive | 42 (67) | 25 (68) | 0.553 |
| Negative | 21 (33) | 12 (32) | |
| Receptor status | |||
| ER + Ve | 6 (10) | 11 (30) | 0.144 |
| HER2 + Ve | 14 (22) | 4 (11) | |
| ER/PR + Ve | 11 (18) | 5 (13) | |
| ER/HER2 + Ve | 11 (17) | 7 (19) | |
| ER/PR/HER2 + Ve | 11 (17) | 4 (11) | |
| TNBC | 10 (16) | 6 (16) | |
| Grade | |||
| 2 | 41 (65) | 16 (43) | <0.027 * |
| 4 | 22 (35) | 21 (57) | |
| Parameters | Control (n = 100) | Breast Cancer (n = 100) | p Value |
|---|---|---|---|
| RBS (mg/dL) | 105.332 ± 7.695 | 136.600 ± 72.074 | <0.001 ** |
| Hematological Parameters | |||
| Hb (g/dL) | 13.273 ± 0.849 | 10.894 ± 1.375 | <0.001 ** |
| Platelet count (103/µL) | 336.549 ± 107.376 | 252.360 ± 93.006 | 0.061 |
| Lipid Profiles | |||
| TC (mg/dL) | 157.430 ± 27.185 | 197.180 ± 33.065 | <0.021 * |
| TG (mg/dL) | 123.191 ± 34.028 | 152.228 ± 53.672 | <0.001 ** |
| HDL-C (mg/dL) | 59.075 ± 19.592 | 53.766 ± 15.669 | <0.017 * |
| LDL-C (mg/dL) | 60.279 ± 19.865 | 65.568 ± 19.777 | 0.888 |
| VLDL-C (mg/dL) | 24.546 ± 7.046 | 29.977 ± 11.191 | <0.001 ** |
| Lipid Peroxidation | |||
| MDA (µM/L) | 3.867 ± 1.882 | 4.137 ± 0.441 | <0.04 * |
| Liver Function tests | |||
| ALP (IU/L) | 107.381 ± 30.061 | 107.520 ± 29.892 | 0.586 |
| AST (IU/L) | 24.448 ± 16.435 | 26.686 ± 9.913 | 0.571 |
| ALT (IU/L) | 17.553 ± 9.814 | 33.087 ± 15.573 | <0.001 ** |
| Total Bilirubin (mg/dL) | 0.464 ± 0.166 | 1.257 ± 0.520 | 0.137 |
| Kidney Function tests | |||
| Blood Urea (mg/dL) | 18.314 ± 6.224 | 14.539 ± 4.752 | <0.001 ** |
| Serum Creatinine (mg/dL) | 0.707 ± 0.140 | 1.607 ± 8.526 | <0.032 * |
| Albumin (g/dL) | 3.958 ± 0.856 | 4.290 ± 0.635 | <0.011 * |
| Globulin (g/dL) | 2.840 ± 0.280 | 3.167 ± 0.434 | <0.001 ** |
| A/G Ratio | 1.574 ± 0.680 | 1.676 ± 0.733 | 0.306 |
| Total Protein (mg/dL) | 7.256 ± 0.946 | 7.394 ± 0.860 | 0.086 |
| Na+ (mmol/L) | 137.442 ± 15.349 | 139.442 ± 6.509 | 0.796 |
| K+ (mmol/L) | 4.180 ± 0.485 | 4.333 ± 0.694 | <0.013 * |
| Cl− (mmol/L) | 99.604 ± 11.432 | 102.323 ± 4.176 | 0.937 |
| Medium-chain fatty acids | |||
| Caproic Acid (%, C:6) | 3.594 (2.684–5.309) | 4.516 (2.671–6.529) | 0.302 |
| Caprylic Acid (%, C:8) | 2.256 (1.794–3.318) | 0.902 (0.624–1.547) | <0.001 # |
| Capric Acid (%, C:10) | 10.709 (9.198–12.544) | 12.559 (10.393–14.956) | <0.002 # |
| Lauric Acid (%, C:12) | 3.882 (3.470–4.761) | 3.083 (2.366–3.700) | <0.001 # |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roopashree, P.G.; Shetty, S.S.; Shetty, V.V.; Nalilu, S.K. Medium-Chain Fatty Acids and Breast Cancer Risk by Receptor and Pathological Subtypes. Nutrients 2022, 14, 5351. https://doi.org/10.3390/nu14245351
Roopashree PG, Shetty SS, Shetty VV, Nalilu SK. Medium-Chain Fatty Acids and Breast Cancer Risk by Receptor and Pathological Subtypes. Nutrients. 2022; 14(24):5351. https://doi.org/10.3390/nu14245351
Chicago/Turabian StyleRoopashree, Padmanabha Ganeshkodi, Shilpa S. Shetty, Vijith Vittal Shetty, and Suchetha Kumari Nalilu. 2022. "Medium-Chain Fatty Acids and Breast Cancer Risk by Receptor and Pathological Subtypes" Nutrients 14, no. 24: 5351. https://doi.org/10.3390/nu14245351
APA StyleRoopashree, P. G., Shetty, S. S., Shetty, V. V., & Nalilu, S. K. (2022). Medium-Chain Fatty Acids and Breast Cancer Risk by Receptor and Pathological Subtypes. Nutrients, 14(24), 5351. https://doi.org/10.3390/nu14245351