


Wernicke Encephalopathy Presenting with Dysphagia: A Case Report and Systematic Literature Review

Abstract
1. Introduction
2. Case Report
3. Literature Review
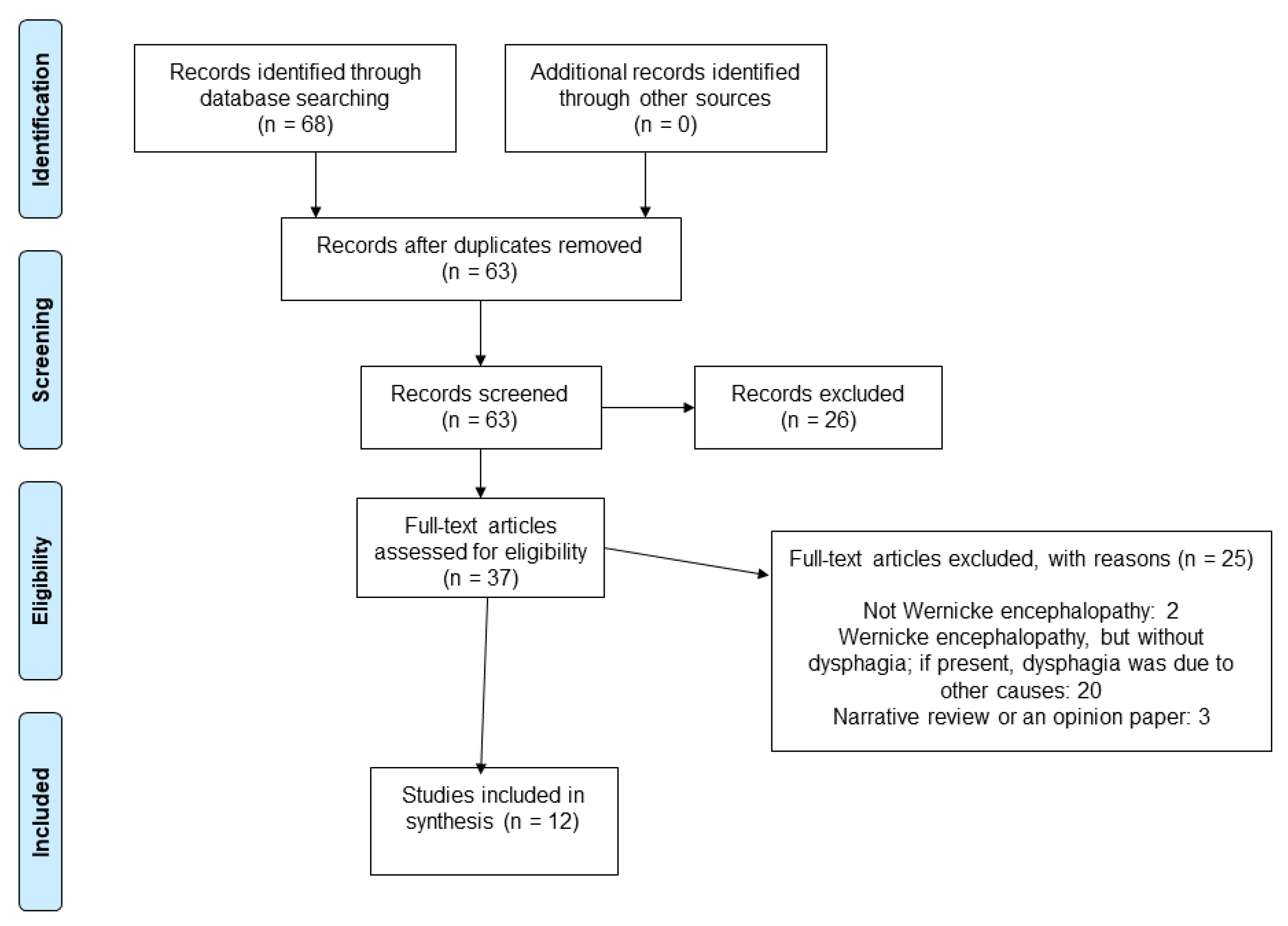
3.1. Materials and Methods
- Is dysphagia a symptom of WE?
- If yes, what is the timing of the onset of dysphagia? Could it be the presenting symptom of WE?
3.2. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reuler, J.B.; Girard, D.E.; Cooney, T.G. Current concepts. Wernicke’s encephalopathy. N. Engl. J. Med. 1985, 312, 1035–1039. [Google Scholar] [CrossRef] [PubMed]
- Galvin, R.; Bråthen, G.; Ivashynka, A.; Hillbom, M.; Tanasescu, R.; Leone, M.A. EFNS guidelines for diagnosis, therapy and prevention of Wernicke encephalopathy. Eur. J. Neurol. 2010, 17, 1408–1418. [Google Scholar] [CrossRef] [PubMed]
- Nikjoo, A.; Rashid, H.; Chung, R.; Sadat, M.A. A rare case of Wernicke encephalopathy in stage IV gastric cancer. Neurocase 2022, 28, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Wang, F.; Cheng, L.; Chen, L.; Wu, Z. Wernicke encephalopathy following advanced caecum cancer. Rev. Esp. Enferm. Dig. 2021, 113, 856–857. [Google Scholar] [CrossRef]
- Barrie, H.J. Wernicke’s encephalopathy in surgical practice; report of three cases. Lancet 1947, 2, 278. [Google Scholar] [CrossRef]
- Oudman, E.; Wijnia, J.W.; Oey, M.J.; van Dam, M.; Postma, A. Wernicke’s encephalopathy in Crohn’s disease and ulcerative colitis. Nutrition 2021, 86, 111182. [Google Scholar] [CrossRef]
- Oudman, E.; Wijnia, J.W.; van Dam, M.; Biter, L.U.; Postma, A. Preventing Wernicke Encephalopathy After Bariatric Surgery. Obes. Surg. 2018, 28, 2060–2068. [Google Scholar] [CrossRef]
- Erick, M. Gestational malnutrition, hyperemesis gravidarum, and Wernicke’s encephalopathy: What is missing? Nutr. Clin. Pract. 2022, 37, 1273–1290. [Google Scholar] [CrossRef]
- Oudman, E.; Wijnia, J.W.; Oey, M.J.; van Dam, M.; Postma, A. Wernicke-Korsakoff syndrome despite no alcohol abuse: A summary of systematic reports. J. Neurol. Sci. 2021, 426, 117482. [Google Scholar] [CrossRef]
- Nadel, A.M.; Burger, P.C. Wernicke encephalopathy following prolonged intravenous therapy. JAMA 1976, 235, 2403–2405. [Google Scholar] [CrossRef]
- Hutcheon, D.A. Malnutrition-induced Wernicke’s encephalopathy following a water-only fasting diet. Nutr. Clin. Pract. 2015, 30, 92–99. [Google Scholar] [CrossRef]
- Oudman, E.; Wijnia, J.W.; Oey, M.J.; van Dam, M.J.; Postma, A. Preventing Wernicke’s encephalopathy in anorexia nervosa: A systematic review. Psychiatry Clin. Neurosci. 2018, 72, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Vasan, S.; Kumar, A. Wernicke Encephalopathy. In StatPearls; StatPearls Publishing Copyright © 2022 LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Harper, C. The incidence of Wernicke’s encephalopathy in Australia—A neuropathological study of 131 cases. J. Neurol. Neurosurg. Psychiatry 1983, 46, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Sakakibara, R.; Hattori, T.; Yasuda, K.; Yamanishi, T.; Tojo, M.; Mori, M. Micturitional disturbance in Wernicke’s encephalopathy. Neurourol. Urodyn. 1997, 16, 111–115. [Google Scholar] [CrossRef]
- Samanta, D. Dry beriberi preceded Wernicke’s encephalopathy: Thiamine deficiency after laparoscopic sleeve gastrectomy. J. Pediatr. Neurosci. 2015, 10, 297–299. [Google Scholar] [CrossRef]
- Rolfe, M. Beri-beri: Endemic amongst urban Gambians. Afr. Health 1994, 16, 22–23. [Google Scholar]
- Osiezagha, K.; Ali, S.; Freeman, C.; Barker, N.C.; Jabeen, S.; Maitra, S.; Olagbemiro, Y.; Richie, W.; Bailey, R.K. Thiamine deficiency and delirium. Innov. Clin. Neurosci. 2013, 10, 26–32. [Google Scholar]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Khalil, H.; Larsen, P.; Marnie, C.; Pollock, D.; Tricco, A.C.; Munn, Z. Best practice guidance and reporting items for the development of scoping review protocols. JBI Evid. Synth. 2022, 20, 953–968. [Google Scholar] [CrossRef]
- Peters, M.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.; Khalil, H. Chapter 11: Scoping Reviews (2020 Version). Available online: https://jbi-global-wiki.refined.site/space/MANUAL/3283910770/Chapter+11%3A+Scoping+reviews (accessed on 22 December 2021).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid.-Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Antel, K.; Singh, N.; Chisholm, B.; Heckmann, J.M. Encephalopathy after persistent vomiting: Three cases of non-alcohol-related wernicke’s encephalopathy. South Afr. Med. J. 2015, 105, 442–443. [Google Scholar] [CrossRef][Green Version]
- Arita, T.; Komatsu, S.; Kosuga, T.; Konishi, H.; Morimura, R.; Murayama, Y.; Kuriu, Y.; Shiozaki, A.; Ikoma, H.; Nakanishi, M.; et al. Laparoscopic Gastrostomy for a Patient with Wernicke’s Encephalopathy after Gastrectomy--A Case Report with a Literature Review. Gan Kagaku Ryoho. Cancer Chemother. 2015, 42, 2037–2039. [Google Scholar]
- Cefalo, M.G.; De Ioris, M.A.; Cacchione, A.; Longo, D.; Staccioli, S.; Arcioni, F.; Bernardi, B.; Mastronuzzi, A. Wernicke encephalopathy in pediatric neuro-oncology: Presentation of 2 cases and review of literature. J. Child Neurol. 2014, 29, NP181–NP185. [Google Scholar] [CrossRef] [PubMed]
- Delavar Kasmaei, H.; Baratloo, A.; Soleymani, M.; Nasiri, Z. Imaging-based diagnosis of Wernicke encephalopathy: A case report. Trauma Mon. 2014, 19, 36–38. [Google Scholar] [CrossRef] [PubMed]
- Dirani, M.; Chahine, E.; Dirani, M.; Kassir, R.; Chouillard, E. More than a Case Report? Should Wernicke Encephalopathy After Sleeve Gastrectomy be a Concern? Obes. Surg. 2017, 27, 2684–2687. [Google Scholar] [CrossRef] [PubMed]
- Karaiskos, I.; Katsarolis, I.; Stefanis, L. Severe dysphagia as the presenting symptom of Wernicke-Korsakoff syndrome in a non-alcoholic man. Neurol. Sci. 2008, 29, 45–46. [Google Scholar] [CrossRef]
- Kikuchi, A.; Chida, K.; Misu, T.; Okita, N.; Nomura, H.; Konno, H.; Takase, S.; Takeda, A.; Itoyama, Y. A case of Wernicke-Korsakoff syndrome with dramatic improvement in consciousness immediately after intravenous infusion of thiamine. Brain Nerve 2000, 52, 59–63. [Google Scholar]
- Mutti, C.; Ciliento, R.; Parrino, L.; Florindo, I.; Pavesi, G.; Zinno, L. Apathetic encephalopathy in thyreotoxicosis: An unsual cause of wernicke encephalopathy and osmotic demyelinating syndrome. Acta Biomed. 2021, 92, e2021055. [Google Scholar] [CrossRef]
- Ros Forteza, F.J.; Cabrera, H.; Bousende, M. Malnutrition in the elderly and Wernicke encephalopathy. Neurologia 2019, 34, 543–546. [Google Scholar] [CrossRef]
- Truedsson, M.; Ohlsson, B.; Sjöberg, K. Wernicke’s encephalopathy presenting with severe dysphagia: A case report. Alcohol Alcohol. 2002, 37, 295–296. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Truong, J.; Shalchian, S.; Myressiotis, S.; Maertens de Noordhout, A.; Fumal, A. About a case of Wernicke’s encephalopathy after sleeve gastrectomy. Eat. Weight. Disord. 2016, 21, 721–723. [Google Scholar] [CrossRef] [PubMed]
- Bano, S.; Nawaz, A.; Asmar, A.; Aemaz Ur Rehman, M.; Farooq, H.; Ali, H. Gradenigo’s syndrome presenting as IX and X cranial nerve palsy without clinically apparent ear infection: A case report and review of literature. eNeurologicalSci 2022, 27, 100397. [Google Scholar] [CrossRef] [PubMed]
- Lutter, S.A.; Kerschner, J.E.; Chusid, M.J. Gradenigo syndrome: A rare but serious complication of otitis media. Pediatr. Emerg. Care 2005, 21, 384–386. [Google Scholar] [CrossRef]
- Fisher, M. An unusual variant of acute idiopathic polyneuritis (syndrome of ophthalmoplegia, ataxia and areflexia). N. Engl. J. Med. 1956, 255, 57–65. [Google Scholar] [CrossRef]
- Rocha Cabrero, F.; Morrison, E.H. Miller Fisher Syndrome. In StatPearls; StatPearls Publishing Copyright © 2022 LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Vasa, M.; Baudendistel, T.E.; Ohikhuare, C.E.; Grace, E.M.; Yan, W.; Josephson, S.A.; Tierney, L.M., Jr. Clinical problem-solving. The eyes have it. N. Engl. J. Med. 2012, 367, 938–943. [Google Scholar] [CrossRef]
- Ashrafian, H.; Davey, P. A review of the causes of central pontine myelinosis: Yet another apoptotic illness? Eur. J. Neurol. 2001, 8, 103–109. [Google Scholar] [CrossRef]
- Gascón-Bayarri, J.; Campdelacreu, J.; García-Carreira, M.C.; Estela, J.; Martínez-Yélamos, S.; Palasí, A.; Delgado, T.; Reñé, R. Wernicke’s encephalopathy in non-alcoholic patients: A series of 8 cases. Neurologia 2011, 26, 540–547. [Google Scholar] [CrossRef]
- Sullivan, E.V.; Pfefferbaum, A. Neuroimaging of the Wernicke-Korsakoff syndrome. Alcohol Alcohol. 2009, 44, 155–165. [Google Scholar] [CrossRef]
- Ota, Y.; Capizzano, A.A.; Moritani, T.; Naganawa, S.; Kurokawa, R.; Srinivasan, A. Comprehensive review of Wernicke encephalopathy: Pathophysiology, clinical symptoms and imaging findings. Jpn. J. Radiol. 2020, 38, 809–820. [Google Scholar] [CrossRef]
- Thomson, A.D.; Cook, C.C.; Guerrini, I.; Sheedy, D.; Harper, C.; Marshall, E.J. Wernicke’s encephalopathy revisited. Translation of the case history section of the original manuscript by Carl Wernicke ’Lehrbuch der Gehirnkrankheiten fur Aerzte and Studirende’ (1881) with a commentary. Alcohol Alcohol. 2008, 43, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Chandrakumar, A.; Bhardwaj, A.; Jong, G.W.t. Review of thiamine deficiency disorders: Wernicke encephalopathy and Korsakoff psychosis. J. Basic Clin. Physiol. Pharmacol. 2019, 30, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Zuccoli, G.; Santa Cruz, D.; Bertolini, M.; Rovira, A.; Gallucci, M.; Carollo, C.; Pipitone, N. MR imaging findings in 56 patients with Wernicke encephalopathy: Nonalcoholics may differ from alcoholics. AJNR Am. J. Neuroradiol. 2009, 30, 171–176. [Google Scholar] [CrossRef]
- Charness, M.E. Brain lesions in alcoholics. Alcohol Clin. Exp. Res. 1993, 17, 2–11. [Google Scholar] [CrossRef]
- Sechi, G.; Serra, A. Wernicke’s encephalopathy: New clinical settings and recent advances in diagnosis and management. Lancet Neurol. 2007, 6, 442–455. [Google Scholar] [CrossRef] [PubMed]
- McBride, W.G. Thalidomide and congenital abnormalities. Lancet 1961, 2, 90927–90928. [Google Scholar]
- Carey, J.C. The importance of case reports in advancing scientific knowledge of rare diseases. Adv. Exp. Med. Biol. 2010, 686, 77–86. [Google Scholar] [CrossRef]
- Bazerbachi, F.; Haffar, S.; Leise, M.D.; Sharma, A.; Mukewar, S.; Sugihara, T.; Murad, M.H.; Watt, K.D. Liver function tests and pattern of hepatic injury in glycogenic hepatopathy associated with insulin-dependent diabetes mellitus: A systematic review and analysis of 172 cases. Hepatology 2017, 66, 441A. [Google Scholar]
- Rosca, E.C.; Tudor, R.; Cornea, A.; Simu, M. Central Nervous System Involvement in Trichinellosis: A Systematic Review. Diagnostics 2021, 11, 945. [Google Scholar] [CrossRef]


{kind=link}
| Study | Age (Years) | Gender | Neurological Symptoms and Signs | Laboratory Tests | Neuroimaging | Treatment and Outcome | Notes |
|---|---|---|---|---|---|---|---|
| Antel 2015 [24] | 22 | Male | Bilateral ophthalmoplegia and ptosis, dysphagia, severe spastic anarthria without any volitional movement of the bulbar musculature. Ataxic gait. Absent tendon reflexes. Able to communicate in writing. Respiratory insufficiency. | All laboratory investigations were normal, including thyroid tests, liver function tests, and CSF examination. HIV and syphilis serology were negative. | Normal brain MRI. | IV immunoglobulin and prednisone without clinical improvement. IV thiamine (100 mg 8-hourly) for 7 days, then 100 mg daily orally. The patient responded within days, with resolution of eye signs and recovery of bulbar function. PEG was removed within 1 month. | Dysphagia at onset. Illicit substance abuse. Non-alcoholic. Severe vomiting and diarrhea the week before admission. |
| Arita 2015 [25] | 58 | Male | Dysphagia. | N/A | MRI: suggestive of Wernicke encephalopathy. | IV thiamine After thiamine treatment, dysphagia improved. | Dysphagia at onset. Non-alcoholic. Distal gastrectomy for gastric cancer. Vomiting, anorexia. |
| Cefalo 2013 [26] | 12 | Male | Acute and rapidly progressive alteration of mental status consisting of hallucinations, aphasia, dysphagia, tremors, bilateral mydriasis, and impairment of consciousness. | Low thiamine level (31.6 nM/L). | MRI: bilateral and symmetric high T2 signal in the thalamic region and mammillary bodies. | IV thiamine (500 mg for 5 days), followed by intramuscular injection (100 mg/day for 20 days and then 100 mg three times a week), with slight neurologic improvement. Oral lorazepam (0.08 mg/kg) with abrupt change in vigilance, with full consciousness, recovery of spontaneous speech, progressive capability of oral alimentation, increase of movements, and postural changes. | Dysphagia at onset. Primitive fronto-parietal neuroectodermal tumor with resection. Chemotherapy. Radiotherapy. Autologous peripheral hemopoietic stem cell rescue therapy. Prolonged parenteral nutrition. |
| Delavar Kasmaei 2014 [27] | 41 | Male | Diplopia, dysarthria, dysphagia, followed by gait disturbances and progressive ataxia accompanied by confusion, apathy, and disorientation. Bilateral horizontal nystagmus in lateral gaze, left abducens nerve palsy, upward gaze palsy. Absent gag reflex. | N/A | MRI: changes consistent with Wernicke encephalopathy. | Thiamine led to partial resolution of his upward gaze palsy and nystagmus on the first day. At the end of the third day of treatment, except for gate ataxia, all other symptoms were fully corrected, and he was totally conscious. After the fifth day, his gait became normal, and after one week, he was discharged in good general condition. | Dysphagia at onset. Non-alcoholic. Severe nausea and vomiting. Untreated Crohn’s disease. |
| Dirani 2017 [28] | 20 | Male | Dysphagia. Diplopia. Bilateral 6th nerve palsy, nystagmus. Bifrontal headache, photophobia, and phonophobia with mildly reduced visual acuity. | Low levels of vitamin D and vitamin B1 and microcytic anemia. | MRI: normal. | IV thiamine (500 mg every 8 h for 2 days) and 500 mg intramuscularly once daily for an additional 5 days in combination with magnesium and other vitamins in the B group. Symptoms improved gradually. | Dysphagia at onset. Non-alcoholic. Laparoscopic sleeve gastrectomy. Persistent vomiting 3 weeks after surgery. Fistula with thoraco-abdominal abscess (5 weeks after surgery). |
| Karaiskos 2008 [29] | 44 | Male | Bilateral abducens nerve palsies with coarse horizontal and vertical upbeat nystagmus. Dysphagia, dysarthria. Dense amnestic deficit consistent with Korsakoff syndrome. Ataxia. | CSF: normal. | MRI: symmetric high signal intensities in the medial thalami, periaqueductal gray matter, and in the floor of the 4th ventricle on T2 and FLAIR sequences. | IV thiamine (100 mg/day) IV antibiotics. Improvement. The gastrostomy tube was removed 8 days after initiation of thiamine. | Dysphagia at onset. Non-alcoholic. Severe malnutrition, prolonged fasting. Bilateral pleural effusions and a pericardial effusion. Fever. Slow onset and progression. |
| Kikuchi 2000 [30] | 68 | Male | Numbness in the feet, followed by dysphagia, unsteady gait, and diplopia. Total ophthalmoplegia. Absence of doll’s eye movement. Absent deep tendon reflexes. Short-term memory impairment. | Serum thiamine level: 9 ng/mL (normal range 20–50 ng/mL). | Symmetrical high intensity lesions in the periaqueductal area of the midbrain, dorsomedial nuclei of bilateral thalami, and vestibular nuclei. | IV thiamine. Marked improvement. | Non-alcoholic. Proximal subtotal gastrectomy and reconstructive surgery of the jejunal interposition for gastric cancer. Fever. Slow onset, chronic progression, and then rapid worsening after fever. |
| Mutti 2021 [31] | 65 | Male | Apathy, forgetfulness, abulia, and mild cognitive impairment, leading to serious malnutrition. Dysphagia. | Hypoalbuminemia. Mild iron deficiency anemia. Suppressed TSH level, high levels of thyroid hormones (FT3 = 12.90 pg/mL, FT4 = 5.09 ng/dL), high positive values of anti-thyroid receptor antibodies (antiTSH-R = 35.55 uU/L). Hypotension, sinusal tachycardia. | MRI: bilateral and symmetrical FLAIR and T2-hyperintense lesions diffused along the periaqueductal area, tectal plate, thalami, and mamillary bodies. | Parenteral nutrition enriched with multivitamins and minerals (in the following months). Twenty-four months after discharge, he recovered from his psychiatric and focal neurological symptoms, except ataxia. | Non-alcoholic. Solitary thyroid nodule and thyroiditis. Central pontine myelinolysis (1 month later). |
| Ros Forteza 2019 [32] | 81 | Female | Gait impairment. Hypotonia. Somnolence, disorientation to time but not space, incoherent speech. Strabismus (exotropia of the right eye), isochoric and reactive pupils (preserved photomotor and consensual reflexes), persistent horizontal-rotary nystagmus, dysphagia for liquids. | CSF: normal. Serum thiamine level: 27 ng/mL (normal range 28–85 ng/mL). Anemia. Vitamin B12: 158 pg/mL (187–883 pg/mL); vitamin D: 17 ng/mL (30–100 ng/mL); magnesium: 1.37 mg/dL (1.6–2.6 mg/dL); sodium: 135 mg/dL (136–145 mg/dL); proteins: 5.3 g/dL (6.4–8.3 g/dL), and albumin: 2.9 g/dL (3.2–4.6 g/dL). | Lesion in the periaqueductal gray matter and tectum and bilateral thalamic lesions. | Thiamine 500 mg IV every 8 h (2 days), 500 mg IV every 24 h (5 days), then 100 mg IV every 8 h during the remaining hospitalization period. Multivitamin solution (vitamins A, B, H (biotin), and F). Protein-calorie supplementation. A significant improvement was noted at 3 months. | Non-alcoholic. Hiatal hernia diagnosed 18 years previously, anti-reflux surgery 15 years previously, cholecystectomy, and acute biliary pancreatitis. Three weeks after influenza infection, anorexia, dehydration, mental confusion, altered sleep–wake cycle, and visual and gait impairment. |
| Sakakibara 1997 [15] | 24 | Female | Staggering gait, ataxia. Vertigo, ophthalmoplegia, ptosis, diplopia, facial paresis, gaze-evoked nystagmus, dysphagia, dysarthria, weak neck flexion. Diminished tendon reflexes. Memory disturbance. Mild dyspnea. Urge urinary incontinence that changed to reflex-type incontinence. | CSF: normal. Nerve conduction studies: decreased motor action potential in the deep peroneal nerve and absent F wave in the median, tibial, and deep peroneal nerves, suggesting mild polyneuropathy. | Abnormal intensities in medial thalamic/ hypothalamic regions and periaqueductal area. | Double filtration plasmapheresis (Guillain–Barre’ syndrome). Thiamine 100 mg/day (6 weeks). Six weeks after the administration of thiamine, incontinence and neurological signs disappeared almost completely. | Non-alcoholic. Pregnant with hyperemesis gravidarum. |
| Truedsson 2002 [33] | 62 | Male | Gait ataxia. Lateral rectus palsy, horizontal nystagmus, dysphagia. Absence of deep tendon reflexes, positive Babinski’s sign on the right side. | Plasma ASAT: 2.65 μkat/L (normal level < 0.80 μkat/L), ALAT: 2.02 μkat/L (normal limit < 0.80 μkat/L), amylase: 0.88 μkat/L (normal range 0.20–0.80 μkat/L), erythrocyte sedimentation rate: 75 mm/h (normal level < 22 mm/h), serum α1-antitrypsin: 1.93 g/L (normal range 0.97–1.68 g/L), serum orosomucoid: 1.61 g/L (normal range 0.54–1.17 g/L). Serum C-reactive protein: 8.9 mg/L (normal limit: < 3.0 mg/L), serum ceruloplasmin: 0.53 g/L (normal range 0.22–0.38 g/L), serum immunoglobulin IgA: 6.30 g/L (normal range 0.70–3.65 g/L), plasma creatinine: 106 μM (normal range 63–105 μM), plasma sodium: 134 mM (normal range 136–146 mM). | N/A | IV glucose. Two injections of thiamine (50 mg/mL, 100 mg per dose) IV. The period between the two doses was 16 h. Neurological signs disappeared after 24 h. | Dysphagia at onset. Alcoholism. A 10 kg weight loss. Emphysema. Fatty liver. |
| Truong 2016 [34] | 27 | Female | Confusion, dysphagia, ataxia, dizziness, diplopia and blurred vision. In 3 days, she developed tetraparesis, facial diparesis, horizontal nystagmus, and vigilance troubles. | Serum thiamine: 15.9 ng/mL (normal range 20–100 ng/mL). CSF: increased proteins (509 mg/L; normal range 150–450 mg/L). Electroneuromyography: normal in four limbs. | MRI: high-intensity Flair in the periaqueductal region and bilateral paraventricular regions of the thalami. | IV thiamine (750 mg/day for 2 weeks, followed by 500 mg/day oral). After 1 month, the patient recovered normal vigilance. Diplopia and visual abnormalities, facial diparesis, and dysphagia disappeared. After a follow-up of 14 months, she still had ataxia and cognitive deficits. | Dysphagia at onset. Non-alcoholic. Sleeve gastrectomy (2 months earlier). One month after surgery, she presented with nausea and recurrent vomiting. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cornea, A.; Lata, I.; Simu, M.; Rosca, E.C. Wernicke Encephalopathy Presenting with Dysphagia: A Case Report and Systematic Literature Review. Nutrients 2022, 14, 5294. https://doi.org/10.3390/nu14245294
Cornea A, Lata I, Simu M, Rosca EC. Wernicke Encephalopathy Presenting with Dysphagia: A Case Report and Systematic Literature Review. Nutrients. 2022; 14(24):5294. https://doi.org/10.3390/nu14245294
Chicago/Turabian StyleCornea, Amalia, Irina Lata, Mihaela Simu, and Elena Cecilia Rosca. 2022. "Wernicke Encephalopathy Presenting with Dysphagia: A Case Report and Systematic Literature Review" Nutrients 14, no. 24: 5294. https://doi.org/10.3390/nu14245294
APA StyleCornea, A., Lata, I., Simu, M., & Rosca, E. C. (2022). Wernicke Encephalopathy Presenting with Dysphagia: A Case Report and Systematic Literature Review. Nutrients, 14(24), 5294. https://doi.org/10.3390/nu14245294