
A Multi-Site, International Audit of Malnutrition Risk and Energy and Protein Intakes in Patients Undergoing Treatment for Head Neck and Esophageal Cancer: Results from INFORM


 ,
,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Data Collection
2.3. Screening for Risk of Malnutrition
2.4. Nutrition Prescription and Intervention
2.5. Statistics
3. Results
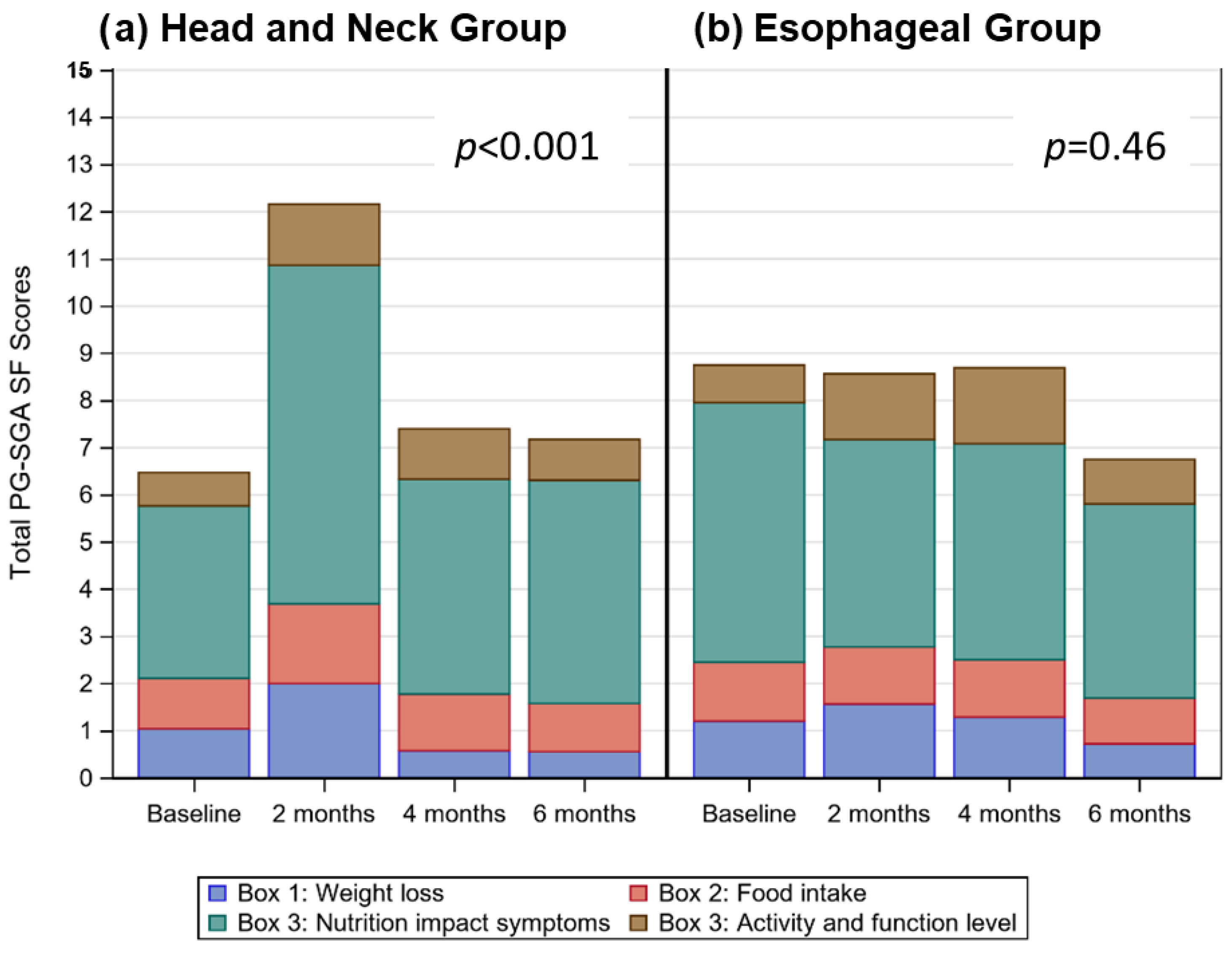
3.1. What Did the Audit Tell Us about Risk of Malnutrition?
3.1.1. HN Cancers
3.1.2. ESO Cancers
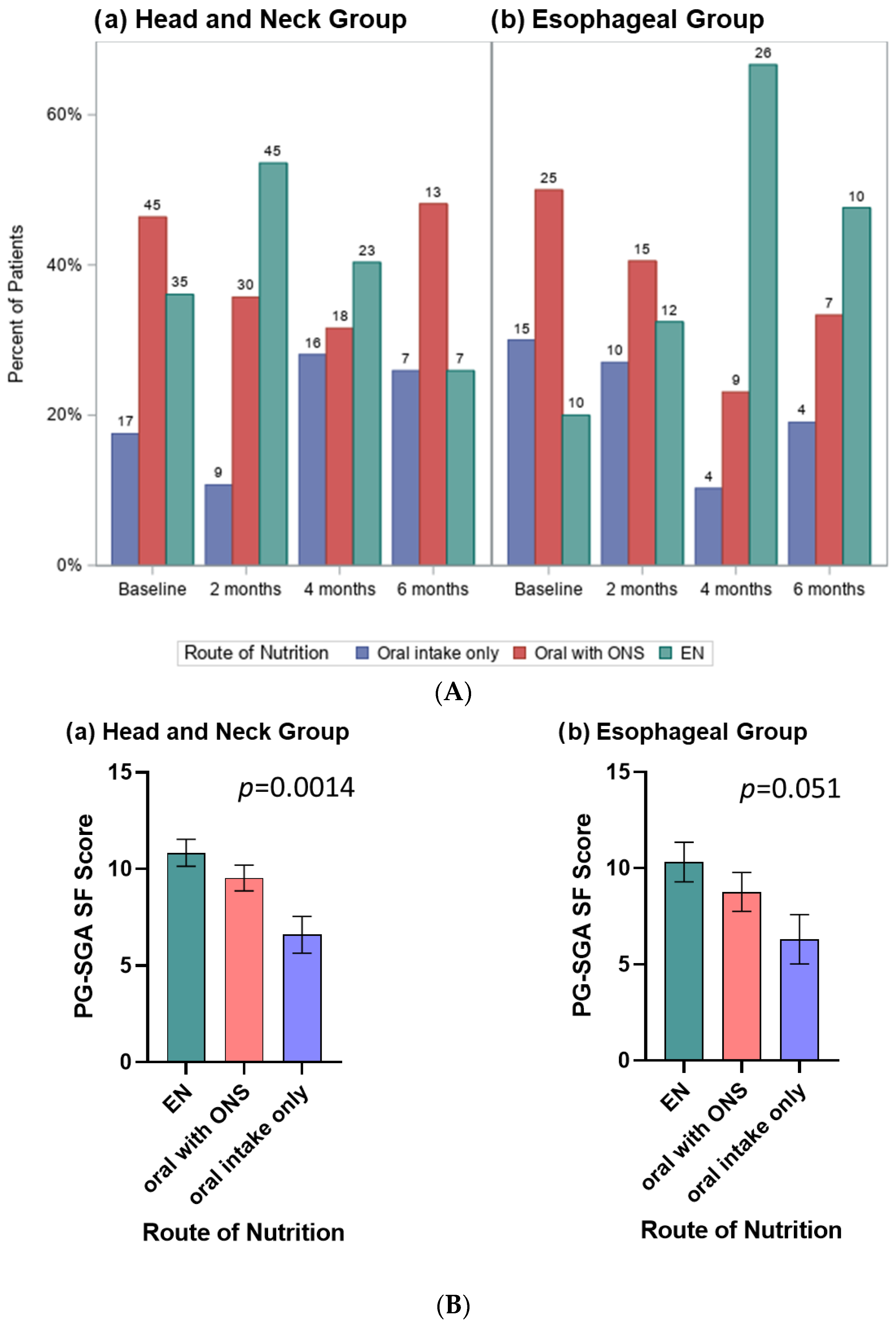
3.2. What Did the Audit Tell Us about the Timing and Type of Nutrition Route Used?
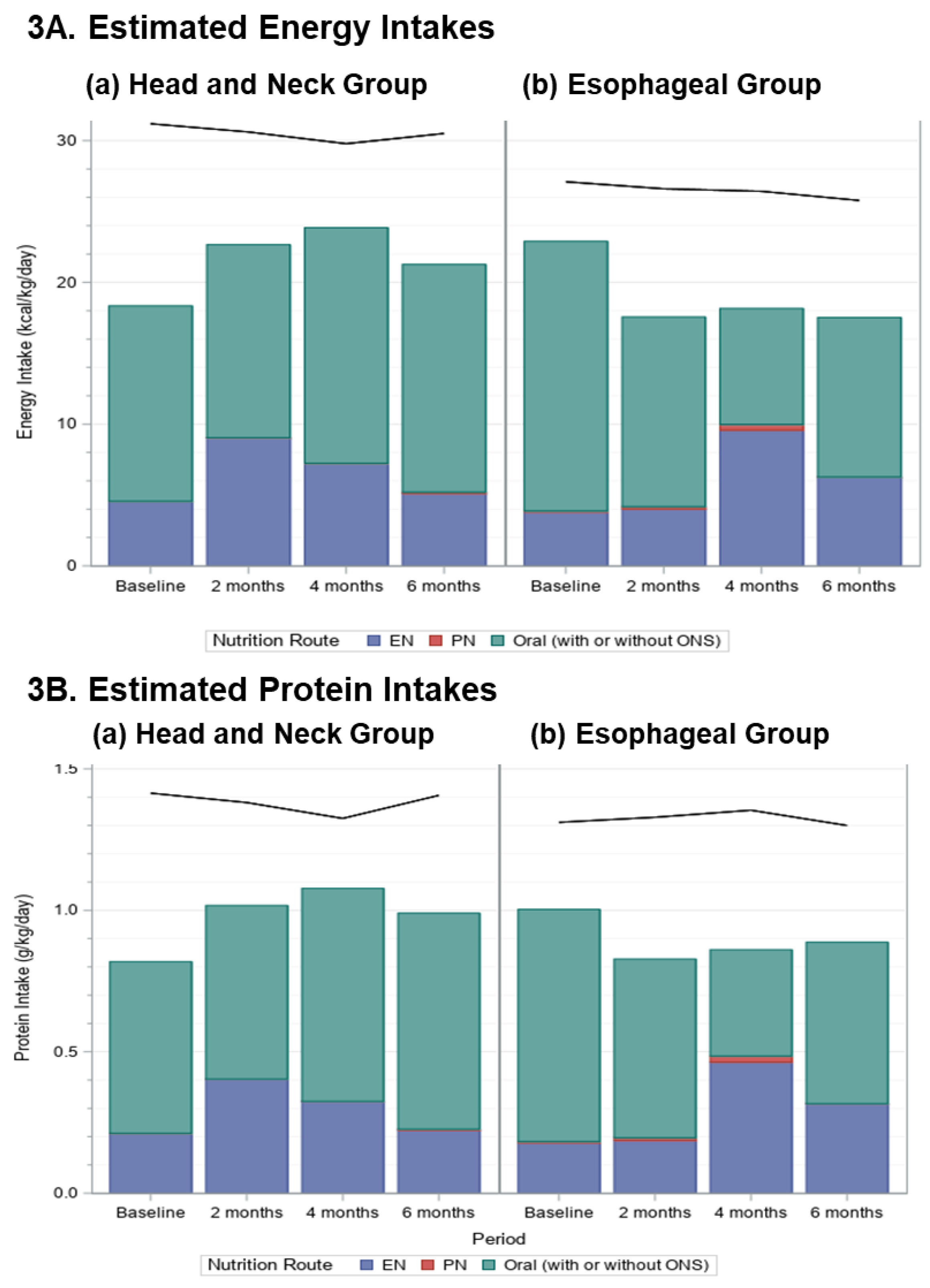
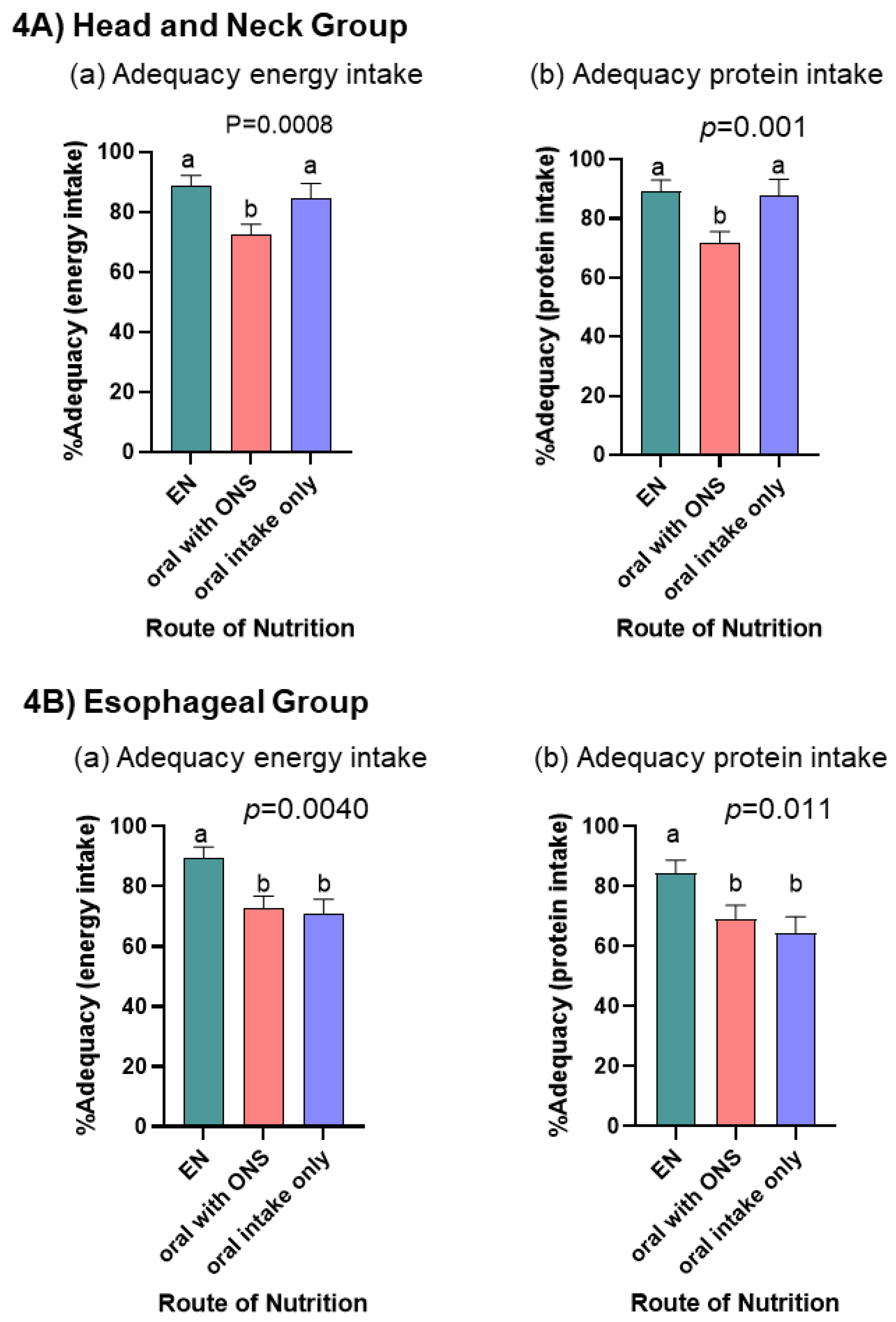
3.3. What Did the Audit Tell Us about the Adequacy of Energy and Protein Intakes According to Nutrition Route?
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dechaphunkul, T.; Martin, L.; Alberda, C.; Olson, K.; Baracos, V.; Gramlich, L. Malnutrition assessment in patients with cancers of the head and neck: A call to action and consensus. Crit. Rev. Oncol. Hematol. 2013, 88, 459–476. [Google Scholar] [CrossRef] [PubMed]
- Couch, M.E.; Dittus, K.; Toth, M.J.; Willis, M.S.; Guttridge, D.C.; George, J.R.; Barnes, C.A.; Gourin, C.G.; Der-Torossian, H. Cancer cachexia update in head and neck cancer: Definitions and diagnostic features. Head Neck 2015, 37, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Anandavadivelan, P.; Lagergren, P. Cachexia in patients with oesophageal cancer. Nat. Rev. Clin. Oncol. 2016, 13, 185–198. [Google Scholar] [CrossRef]
- Cox, S.; Powell, C.; Carter, B.; Hurt, C.; Mukherjee, S.; Crosby, T.D.L. Role of nutritional status and intervention in oesophageal cancer treated with definitive chemoradiotherapy: Outcomes from SCOPE1. Br. J. Cancer 2016, 115, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Kubrak, C.; Martin, L.; Gramlich, L.; Scrimger, R.; Jha, N.; Debenham, B.; Chua, N.; Walker, J.; Baracos, V.E. Prevalence and prognostic significance of malnutrition in patients with cancers of the head and neck. Clin. Nutr. 2020, 39, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Grace, E.M.; Shaw, C.; Lalji, A.; Mohammed, K.; Andreyev, H.J.N.; Whelan, K. Nutritional status, the development and persistence of malnutrition and dietary intake in oesophago-gastric cancer: A longitudinal cohort study. J. Hum. Nutr. Diet. 2018, 31, 785–792. [Google Scholar] [CrossRef]
- Movahed, S.; Norouzy, A.; Ghanbari-Motlagh, A.; Eslami, S.; Khadem-Rezaiyan, M.; Emadzadeh, M.; Nematy, M.; Ghayour-Mobarhan, M.; Varshoee Tabrizi, F.; Bozzetti, F.; et al. Nutritional Status in Patients with Esophageal Cancer Receiving Chemoradiation and Assessing the Efficacy of Usual Care for Nutritional Managements. Asian Pac. J. Cancer Prev. 2020, 21, 2315–2323. [Google Scholar] [CrossRef]
- Citak, E.; Tulek, Z.; Uzel, O. Nutritional status in patients with head and neck cancer undergoing radiotherapy: A longitudinal study. Support. Care Cancer 2019, 27, 239–247. [Google Scholar] [CrossRef]
- Ding, H.; Dou, S.; Ling, Y.; Zhu, G.; Wang, Q.; Wu, Y.; Qian, Y. Longitudinal Body Composition Changes and the Importance of Fat-Free Mass Index in Locally Advanced Nasopharyngeal Carcinoma Patients Undergoing Concurrent Chemoradiotherapy. Integr. Cancer Ther. 2018, 17, 1125–1131. [Google Scholar] [CrossRef] [PubMed]
- Jager-Wittenaar, H.; Dijkstra, P.U.; Dijkstra, G.; Bijzet, J.; Langendijk, J.A.; van der Laan, B.F.A.M.; Roodenburg, J.L.N. High prevalence of cachexia in newly diagnosed head and neck cancer patients: An exploratory study. Nutrition 2017, 35, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Kubrak, C.; Olson, K.; Jha, N.; Scrimger, R.; Parliament, M.; McCargar, L.; Koski, S.; Baracos, V.E. Clinical determinants of weight loss in patients receiving radiation and chemoirradiation for head and neck cancer: A prospective longitudinal view. Head Neck 2013, 35, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Neoh, M.K.; Abu Zaid, Z.; Mat Daud, Z.A.; Md Yusop, N.B.; Ibrahim, Z.; Abdul Rahman, Z.; Jamhuri, N. Changes in Nutrition Impact Symptoms, Nutritional and Functional Status during Head and Neck Cancer Treatment. Nutrients 2020, 12, 1225. [Google Scholar] [CrossRef] [PubMed]
- Langius, J.A.E.; Twisk, J.; Kampman, M.; Doornaert, P.; Kramer, M.H.H.; Weijs, P.J.M.; Leemans, C.R. Prediction model to predict critical weight loss in patients with head and neck cancer during (chemo)radiotherapy. Oral Oncol. 2016, 52, 91–96. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, L.; Jin, S.; Li, H.; Gong, L.; Wang, Y.; Jin, S.; Cao, Y.; Shih, Y.; Lu, Q. Swallowing functional outcomes and nutritional status in head and neck cancer radiotherapy: Longitudinal study. BMJ Support. Palliat. Care 2020, 10, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Arribas, L.; Hurtós, L.; Taberna, M.; Peiró, I.; Vilajosana, E.; Lozano, A.; Vazquez, S.; Mesia, R.; Virgili, N. Nutritional changes in patients with locally advanced head and neck cancer during treatment. Oral Oncol. 2017, 71, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Martin, L.; Muscaritoli, M.; Bourdel-Marchasson, I.; Kubrak, C.; Laird, B.; Gagnon, B.; Chasen, M.; Gioulbasanis, I.; Wallengren, O.; Voss, A.C.; et al. Diagnostic criteria for cancer cachexia: Reduced food intake and inflammation predict weight loss and survival in an international, multi-cohort analysis. J. Cachexia. Sarcopenia Muscle 2021, 12, 1189–1202. [Google Scholar] [CrossRef] [PubMed]
- Yanni, A.; Dequanter, D.; Lechien, J.R.; Loeb, I.; Rodriguez, A.; Javadian, R.; Van Gossum, M. Malnutrition in head and neck cancer patients: Impacts and indications of a prophylactic percutaneous endoscopic gastrostomy. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2019, 136, S27–S33. [Google Scholar] [CrossRef] [PubMed]
- Kubrak, C.; Olson, K.; Jha, N.; Jensen, L.; McCargar, L.; Seikaly, H.; Harris, J.; Scrimger, R.; Parliament, M.; Baracos, V.E. Nutrition impact symptoms: Key determinants of reduced dietary intake, weight loss, and reduced functional capacity of patients with head and neck cancer before treatment. Head Neck 2010, 32, 290–300. [Google Scholar] [CrossRef]
- Couch, M.E.; Dittus, K.; Toth, M.J.; Willis, M.S.; Guttridge, D.C.; George, J.R.; Chang, E.Y.; Gourin, C.G.; Der-Torossian, H. Cancer cachexia update in head and neck cancer: Pathophysiology and treatment. Head Neck 2015, 37, 1057–1072. [Google Scholar] [CrossRef] [PubMed]
- Baracos, V.E.; Martin, L.; Korc, M.; Guttridge, D.C.; Fearon, K.C.H. Cancer-associated cachexia. Nat. Rev. Dis. Prim. 2018, 4, 17105. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef] [PubMed]
- Roeland, E.J.; Bohlke, K.; Baracos, V.E.; Bruera, E.; Del Fabbro, E.; Dixon, S.; Fallon, M.; Herrstedt, J.; Lau, H.; Platek, M.; et al. Management of Cancer Cachexia: ASCO Guideline. J. Clin. Oncol. 2020, 38, 2438–2453. [Google Scholar] [CrossRef]
- Dort, J.C.; Farwell, D.G.; Findlay, M.; Huber, G.F.; Kerr, P.; Shea-Budgell, M.A.; Simon, C.; Uppington, J.; Zygun, D.; Ljungqvist, O.; et al. Optimal Perioperative Care in Major Head and Neck Cancer Surgery with Free Flap Reconstruction: A Consensus Review and Recommendations from the Enhanced Recovery After Surgery Society. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 292–303. [Google Scholar] [CrossRef] [PubMed]
- Low, D.E.; Allum, W.; De Manzoni, G.; Ferri, L.; Immanuel, A.; Kuppusamy, M.; Law, S.; Lindblad, M.; Maynard, N.; Neal, J.; et al. Guidelines for Perioperative Care in Esophagectomy: Enhanced Recovery After Surgery (ERAS®) Society Recommendations. World J. Surg. 2019, 43, 299–330. [Google Scholar] [CrossRef]
- Arends, J.; Strasser, F.; Gonella, S.; Solheim, T.S.; Madeddu, C.; Ravasco, P.; Buonaccorso, L.; de van der Schueren, M.A.E.; Baldwin, C.; Chasen, M.; et al. Cancer cachexia in adult patients: ESMO Clinical Practice Guidelines☆. ESMO Open 2021, 6, 100092. [Google Scholar] [CrossRef]
- Findlay, M.; Rankin, N.M.; Shaw, T.; White, K.; Boyer, M.; Milross, C.; De Abreu Lourenço, R.; Brown, C.; Collett, G.; Beale, P.; et al. Best Evidence to Best Practice: Implementing an Innovative Model of Nutrition Care for Patients with Head and Neck Cancer Improves Outcomes. Nutrients 2020, 12, 1465. [Google Scholar] [CrossRef]
- Head and Neck Guideline Steering Committee. Evidence-Based Practice Guidelines for the Nutritional Management of Adult Patients with Head and Neck Cancer. 2022. Available online: https://wiki.cancer.org.au/australia/COSA:Head_and_neck_cancer_nutrition_guidelines (accessed on 9 December 2022).
- Isenring, E.; Zabel, R.; Bannister, M.; Brown, T.; Findlay, M.; Kiss, N.; Loeliger, J.; Johnstone, C.; Camilleri, B.; Davidson, W.; et al. Updated evidence-based practice guidelines for the nutritional management of patients receiving radiation therapy and/or chemotherapy. Nutr. Diet. 2013, 70, 312–324. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN guideline: Clinical nutrition in surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef]
- Braga, M.; Ljungqvist, O.; Soeters, P.; Fearon, K.; Weimann, A.; Bozzetti, F. ESPEN Guidelines on Parenteral Nutrition: Surgery. Clin. Nutr. 2009, 28, 378–386. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Harsanyi, L.; Laviano, A.; Ljungqvist, O.; Soeters, P.; Jauch, K.W.; Kemen, M.; Hiesmayr, J.M.; Horbach, T.; et al. ESPEN Guidelines on Enteral Nutrition: Surgery including organ transplantation. Clin. Nutr. 2006, 25, 224–244. [Google Scholar] [CrossRef] [PubMed]
- Thompson, K.L.; Elliott, L.; Fuchs-Tarlovsky, V.; Levin, R.M.; Voss, A.C.; Piemonte, T. Oncology Evidence-Based Nutrition Practice Guideline for Adults. J. Acad. Nutr. Diet. 2017, 117, 297–310.e47. [Google Scholar] [CrossRef] [PubMed]
- Talwar, B.; Donnelly, R.; Skelly, R.; Donaldson, M. Nutritional management in head and neck cancer: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S32–S40. [Google Scholar] [CrossRef] [PubMed]
- Hakel-Smith, N.; Lewis, N.M. A standardized nutrition care process and language are essential components of a conceptual model to guide and document nutrition care and patient outcomes. J. Am. Diet. Assoc. 2004, 104, 1878–1884. [Google Scholar] [CrossRef] [PubMed]
- Lacey, K.; Pritchett, E. Nutrition Care Process and Model: ADA adopts road map to quality care and outcomes management. J. Am. Diet. Assoc. 2003, 103, 1061–1072. [Google Scholar] [CrossRef]
- Findlay, M.; Bauer, J.D.; Dhaliwal, R.; de van der Schueren, M.; Laviano, A.; Widaman, A.; Martin, L.; Day, A.G.; Gramlich, L.M. Translating Evidence-Based Guidelines into Practice-Are We Getting It Right? A Multi-Centre Prospective International Audit of Nutrition Care in Patients with Foregut Tumors (INFORM). Nutrients 2020, 12, 3808. [Google Scholar] [CrossRef]
- Jager-Wittenaar, H.; Ottery, F.D. Assessing nutritional status in cancer: Role of the Patient-Generated Subjective Global Assessment. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 322–329. [Google Scholar] [CrossRef]
- Jager-Wittenaar, H.; de Bats, H.F.; Welink-Lamberts, B.J.; Gort-van Dijk, D.; van der Laan, B.F.A.M.; Ottery, F.D.; Roodenburg, J.L.N. Self-Completion of the Patient-Generated Subjective Global Assessment Short Form Is Feasible and Is Associated with Increased Awareness on Malnutrition Risk in Patients with Head and Neck Cancer. Nutr. Clin. Pract. 2020, 35, 353–362. [Google Scholar] [CrossRef]
- Ottery, F.D. Definition of standardized nutritional assessment and interventional pathways in oncology. Nutrition 1996, 12, S15–S19. [Google Scholar] [CrossRef]
- McCurdy, B.; Nejatinamini, S.; Debenham, B.J.; Álvarez-Camacho, M.; Kubrak, C.; Wismer, W.V.; Mazurak, V.C. Meeting Minimum ESPEN Energy Recommendations Is Not Enough to Maintain Muscle Mass in Head and Neck Cancer Patients. Nutrients 2019, 11, 2743. [Google Scholar] [CrossRef]
- Della Valle, S.; Colatruglio, S.; La Vela, V.; Tagliabue, E.; Mariani, L.; Gavazzi, C. Nutritional intervention in head and neck cancer patients during chemo-radiotherapy. Nutrition 2018, 51–52, 95–97. [Google Scholar] [CrossRef] [PubMed]
- Bargetzi, L.; Brack, C.; Herrmann, J.; Bargetzi, A.; Hersberger, L.; Bargetzi, M.; Kaegi-Braun, N.; Tribolet, P.; Gomes, F.; Hoess, C.; et al. Nutritional support during the hospital stay reduces mortality in patients with different types of cancers: Secondary analysis of a prospective randomized trial. Ann. Oncol. 2021, 32, 1025–1033. [Google Scholar] [CrossRef] [PubMed]
- Bozzetti, F. Suboptimal nutritional support in cancer patients gets excellent results. Reply to the Letter to the Editor: ‘Nutritional support during the hospital stay reduces mortality in patients with different types of cancers: Secondary analysis of a prospective randomized trial’ by L. Bargetzi et al. Ann. Oncol. 2021, 32, 1304–1305. [Google Scholar]
- Alberda, C.; Alvadj-Korenic, T.; Mayan, M.; Gramlich, L. Nutrition Care in Patients with Head and Neck or Esophageal Cancer: The Patient Perspective. Nutr. Clin. Pract. 2017, 32, 664–674. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.; Banks, M.; Hughes, B.G.M.; Lin, C.; Kenny, L.; Bauer, J. Tube feeding during treatment for head and neck cancer—Adherence and patient reported barriers. Oral Oncol. 2017, 72, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; de van der Schueren, M.A.E.; Blauwhoff-Buskermolen, S.; Baracos, V.; Gramlich, L. Identifying the Barriers and Enablers to Nutrition Care in Head and Neck and Esophageal Cancers: An International Qualitative Study. JPEN. J. Parenter. Enteral Nutr. 2016, 40, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; Senesse, P.; Gioulbasanis, I.; Antoun, S.; Bozzetti, F.; Deans, C.; Strasser, F.; Thoresen, L.; Jagoe, R.T.; Chasen, M.; et al. Diagnostic criteria for the classification of cancer-associated weight loss. J. Clin. Oncol. 2015, 33, 90–99. [Google Scholar] [CrossRef]
- Carr, R.A.; Harrington, C.; Stella, C.; Glauner, D.; Kenny, E.; Russo, L.M.; Garrity, M.J.; Bains, M.S.; Sihag, S.; Jones, D.R.; et al. Early implementation of a perioperative nutrition support pathway for patients undergoing esophagectomy for esophageal cancer. Cancer Med. 2022, 11, 592–601. [Google Scholar] [CrossRef]
- Dijksterhuis, W.P.M.; Latenstein, A.E.J.; van Kleef, J.J.; Verhoeven, R.H.A.; de Vries, J.H.M.; Slingerland, M.; Steenhagen, E.; Heisterkamp, J.; Timmermans, L.M.; de van der Schueren, M.A.E.; et al. Cachexia and Dietetic Interventions in Patients with Esophagogastric Cancer: A Multicenter Cohort Study. J. Natl. Compr. Cancer Netw. 2021, 19, 144–152. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Head & Neck Cancers (n = 119) n (%) | Esophageal Cancers (n = 51) n (%) | |
|---|---|---|
| Demographics | ||
| Centre (Country—City) | ||
| Australia—Brisbane | 10 (8.4%) | 0 (0.0%) |
| Australia—Sydney | 20 (16.8%) | 0 (0.0%) |
| Canada—Calgary 1 | 21 (17.6%) | 10 (19.6%) |
| Canada—Edmonton 1 | 20 (16.8%) | 18 (35.3%) |
| Italy—Rome | 19 (16.0%) | 0 (0.0%) |
| Netherlands—Amsterdam | 20 (16.8%) | 23 (45.1%) |
| USA—Sacramento | 9 (7.6%) | 0 (0.0%) |
| Age, years | ||
| median (Q1, Q3) | 62 (58, 69) | 65 (56, 71) |
| Sex | ||
| Male | 93 (78.2%) | 41 (80.4%) |
| Female | 26 (21.8%) | 10 (19.6%) |
| Ethnicity | ||
| Caucasian | 111 (93.3%) | 50 (98.0%) |
| First Nations | 1 (0.8%) | 0 (0.0%) |
| Hispanic | 2 (1.7%) | 0 (0.0%) |
| Asian | 3 (2.5%) | 1 (2.0%) |
| East Indian | 1 (0.8%) | 0 (0.0%) |
| Other | 1 (0.8%) | 0 (0.0%) |
| Current Smoker | ||
| Yes | 44 (37.0%) | 13 (25.5%) |
| No | 75 (63.0%) | 38 (74.5%) |
| Alcohol use | ||
| Yes | 47 (39.5%) | 9 (17.6%) |
| No | 72 (60.5%) | 42 (82.4%) |
| ECOG Performance Status | ||
| 0 | 78 (65.5%) | 32 (62.7%) |
| 1 | 32 (26.9%) | 16 (31.4%) |
| 2 | 6 (5.0%) | 3 (5.9%) |
| 3 | 3 (2.5%) | 0 (0.0%) |
| BMI, kg/m2 median (Q1, Q3) | 25.8 (23.0, 30.0) | 27.5 (24.5, 31.0) |
| BMI Class | ||
| <18.5 | 6 (5.0%) | 1 (2.0%) |
| 18.5–24.9 | 46 (38.7%) | 13 (25.5%) |
| 25.0–29.9 | 37 (31.1%) | 21 (41.2%) |
| ≥30.0 | 30 (25.2%) | 16 (31.4%) |
| Cancer Stage | ||
| 1 | 5 (4.2%) | 4 (7.8%) |
| 2 | 8 (6.7%) | 13 (25.5%) |
| 3 | 18 (15.1%) | 15 (29.4%) |
| 4 (Any) | 74 (62.2%) | 4 (7.8%) |
| Could not assess stage | 7 (5.9%) | 9 (17.7%) |
| Not staged | 7 (5.9%) | 4 (7.8%) |
| Missing | 0 (0%) | 2 (3.9%) |
| Tumor Site—Head & Neck | ||
| Primary unknown | 3 (2.5%) | |
| Hypopharynx | 10 (8.4%) | |
| Larynx | 22 (18.5%) | |
| Nasopharynx | 5 (4.2%) | |
| Oral cavity | 32 (26.9%) | |
| Oropharynx | 39 (32.8%) | |
| Other | 3(2.5%) | |
| Salivary gland | 5 (4.2%) | |
| Treatment Modality 2 | n = 100 | n = 51 |
| None | 5 (5.0%) | 4 (7.8%) |
| Chemotherapy—definitive | 0 (0.0%) | 2 (3.9%) |
| Chemotherapy—adjuvant | 0 (0.0%) | 1 (2.0%) |
| Radiotherapy—definitive | 15 (15.0%) | 0 (0.0%) |
| Surgery | 10 (10.0%) | 2 (3.9%) |
| Chemoradiotherapy—definitive | 54 (54.0%) | 7 (13.7%) |
| Surgery + adj/neoadj RT | 7 (7.0%) | 0 (0.0%) |
| Surgery + adj/neoadj CRT | 9 (9.0%) | 35 (68.6%) |
| Head & Neck Cancers | Esophageal Cancers | |||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | 2 Months | 4 Months | 6 Months | Baseline | 2 Months | 4 Months | 6 Months | |
| n = 116 | n = 104 | n = 105 | n = 90 | n = 44 | n = 38 | n = 38 | n = 36 | |
| PG-SGA total score, median (Q1, Q3) | 5 (1, 10) | 12 (7, 18) | 7 (4, 10) | 6 (2, 11) | 8 (4, 11) | 7 (2, 15) | 9 (6, 10) | 5 (2, 9) |
| PG-SGA Triage, n(%) | ||||||||
| 0–1 1 | 33 (28) | 8 (8) | 13 (13) | 15 (17) | 4 (9) | 6 (16) | 1 (3) | 4 (11) |
| 2–3 2 | 13 (11) | 6 (6) | 12 (12) | 15 (17) | 6 (14) | 5 (13) | 5 (13) | 6 (17) |
| 4–8 3 | 33 (28) | 21 (20) | 39 (37) | 27 (30) | 14 (32) | 11 (29) | 12 (32) | 17 (47) |
| ≥9 4 | 37 (32) | 69 (66) | 40 (38) | 32 (36) | 20 (45) | 16 (42) | 20 (53) | 9 (25) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin, L.; Findlay, M.; Bauer, J.D.; Dhaliwal, R.; de van der Schueren, M.; Laviano, A.; Widaman, A.; Baracos, V.E.; Day, A.G.; Gramlich, L.M. A Multi-Site, International Audit of Malnutrition Risk and Energy and Protein Intakes in Patients Undergoing Treatment for Head Neck and Esophageal Cancer: Results from INFORM. Nutrients 2022, 14, 5272. https://doi.org/10.3390/nu14245272
Martin L, Findlay M, Bauer JD, Dhaliwal R, de van der Schueren M, Laviano A, Widaman A, Baracos VE, Day AG, Gramlich LM. A Multi-Site, International Audit of Malnutrition Risk and Energy and Protein Intakes in Patients Undergoing Treatment for Head Neck and Esophageal Cancer: Results from INFORM. Nutrients. 2022; 14(24):5272. https://doi.org/10.3390/nu14245272
Chicago/Turabian StyleMartin, Lisa, Merran Findlay, Judith D. Bauer, Rupinder Dhaliwal, Marian de van der Schueren, Alessandro Laviano, Adrianne Widaman, Vickie E. Baracos, Andrew G. Day, and Leah M. Gramlich. 2022. "A Multi-Site, International Audit of Malnutrition Risk and Energy and Protein Intakes in Patients Undergoing Treatment for Head Neck and Esophageal Cancer: Results from INFORM" Nutrients 14, no. 24: 5272. https://doi.org/10.3390/nu14245272
APA StyleMartin, L., Findlay, M., Bauer, J. D., Dhaliwal, R., de van der Schueren, M., Laviano, A., Widaman, A., Baracos, V. E., Day, A. G., & Gramlich, L. M. (2022). A Multi-Site, International Audit of Malnutrition Risk and Energy and Protein Intakes in Patients Undergoing Treatment for Head Neck and Esophageal Cancer: Results from INFORM. Nutrients, 14(24), 5272. https://doi.org/10.3390/nu14245272