
Promoting Protein Intake in an Ageing Population: Product Design Implications for Protein Fortification

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Overview
2.2. Initial Literature and Market Review on Protein-Fortified Products
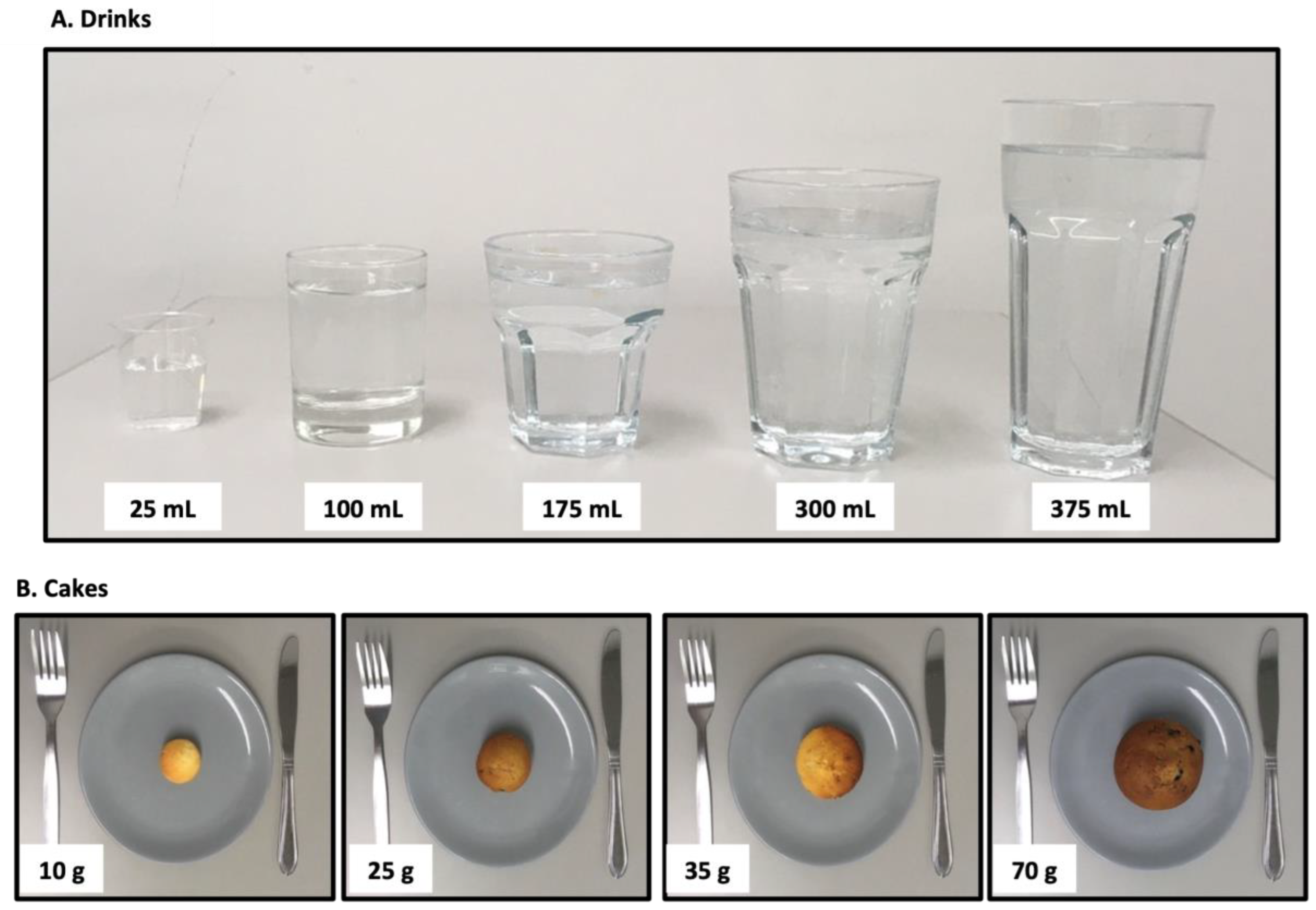
2.3. Questionnaire Design
2.4. Statistical Analysis
3. Results
3.1. Initial Literature and Market Review on Protein-Fortified Products
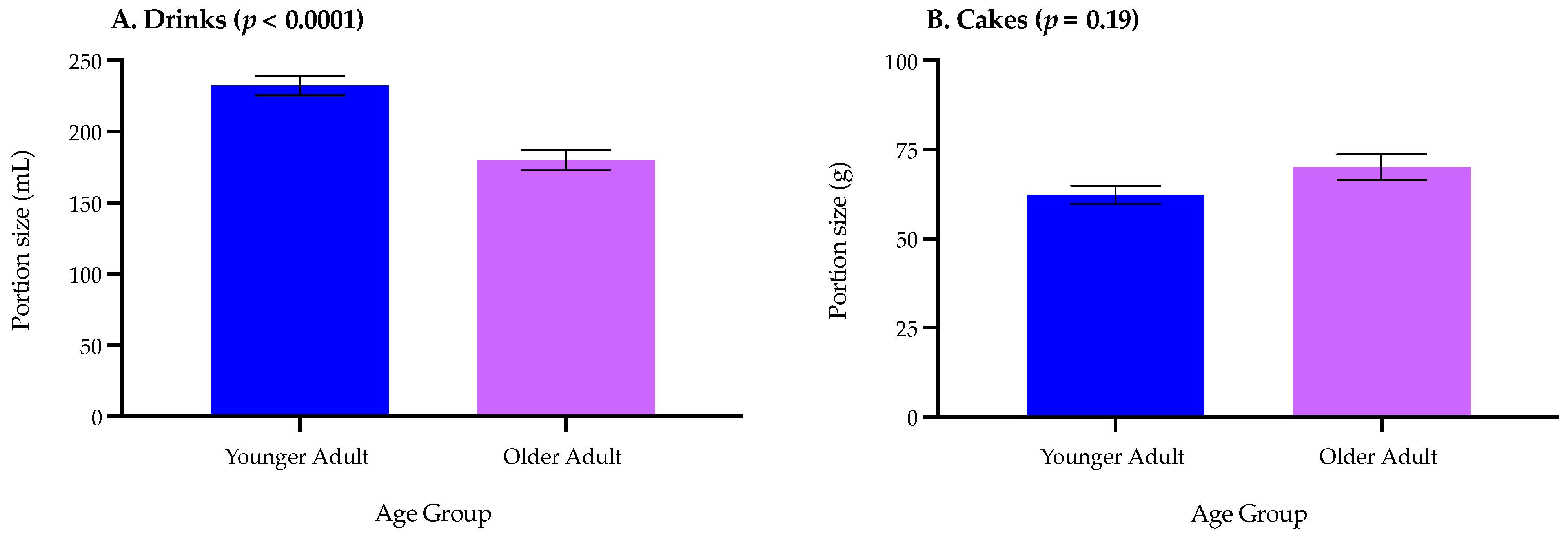
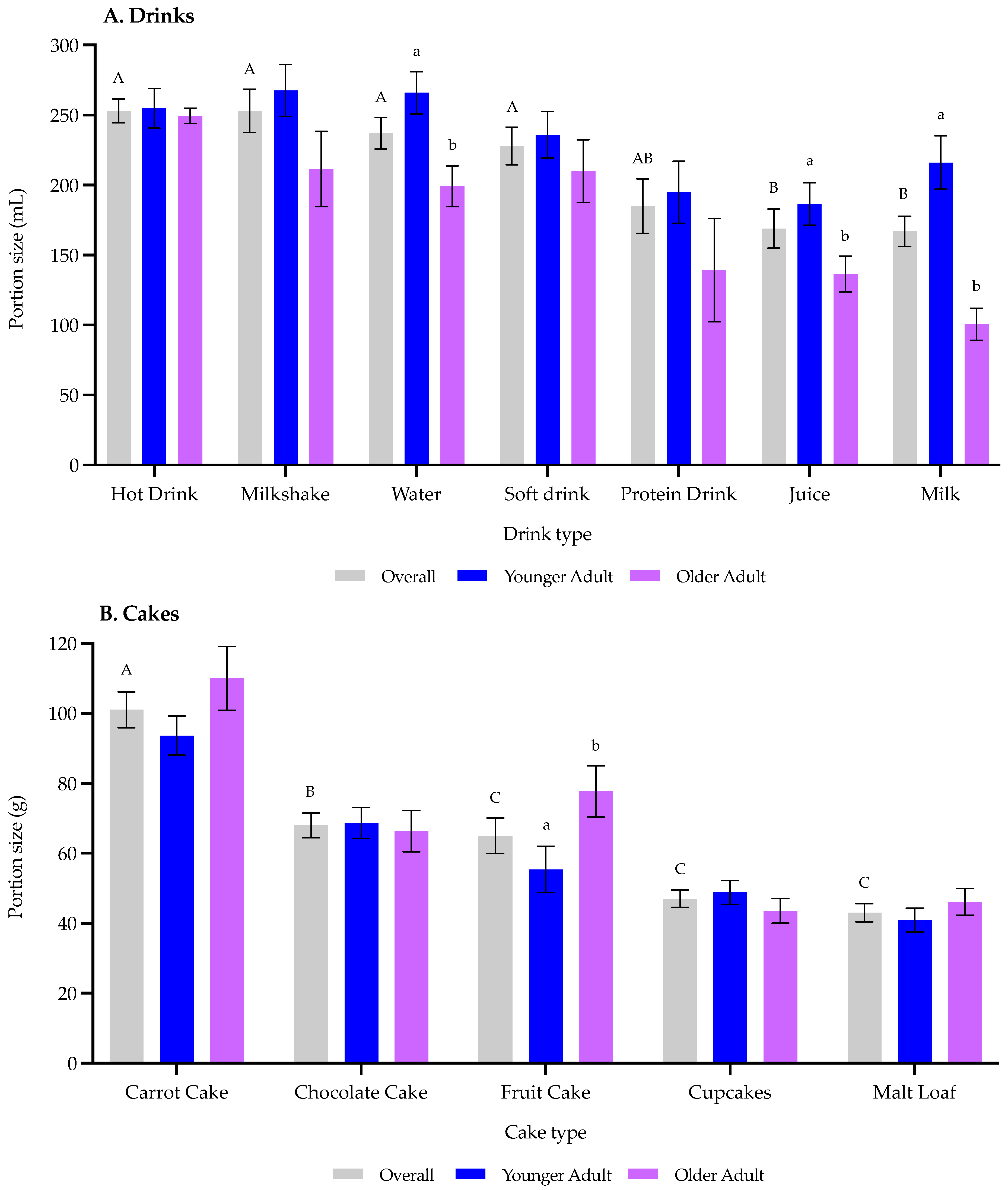
3.2. Portion Size Questionnaire
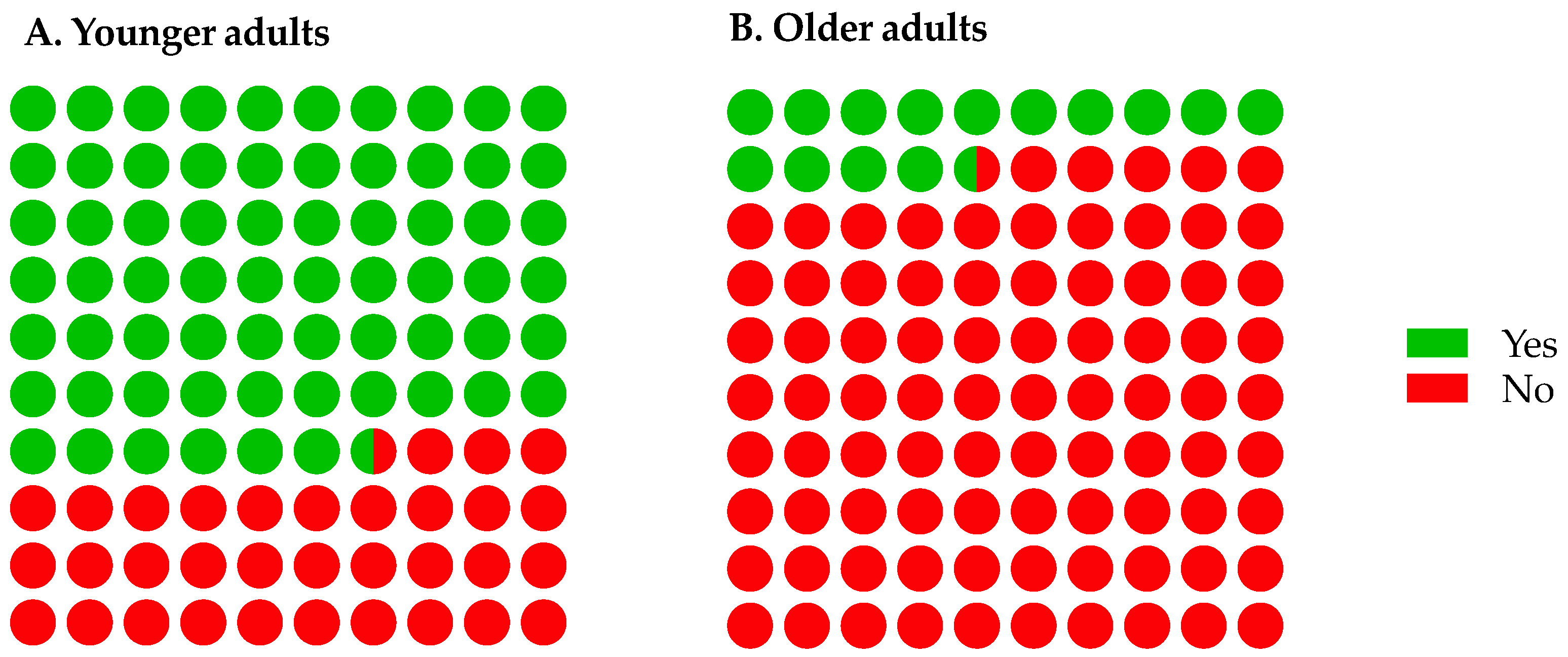
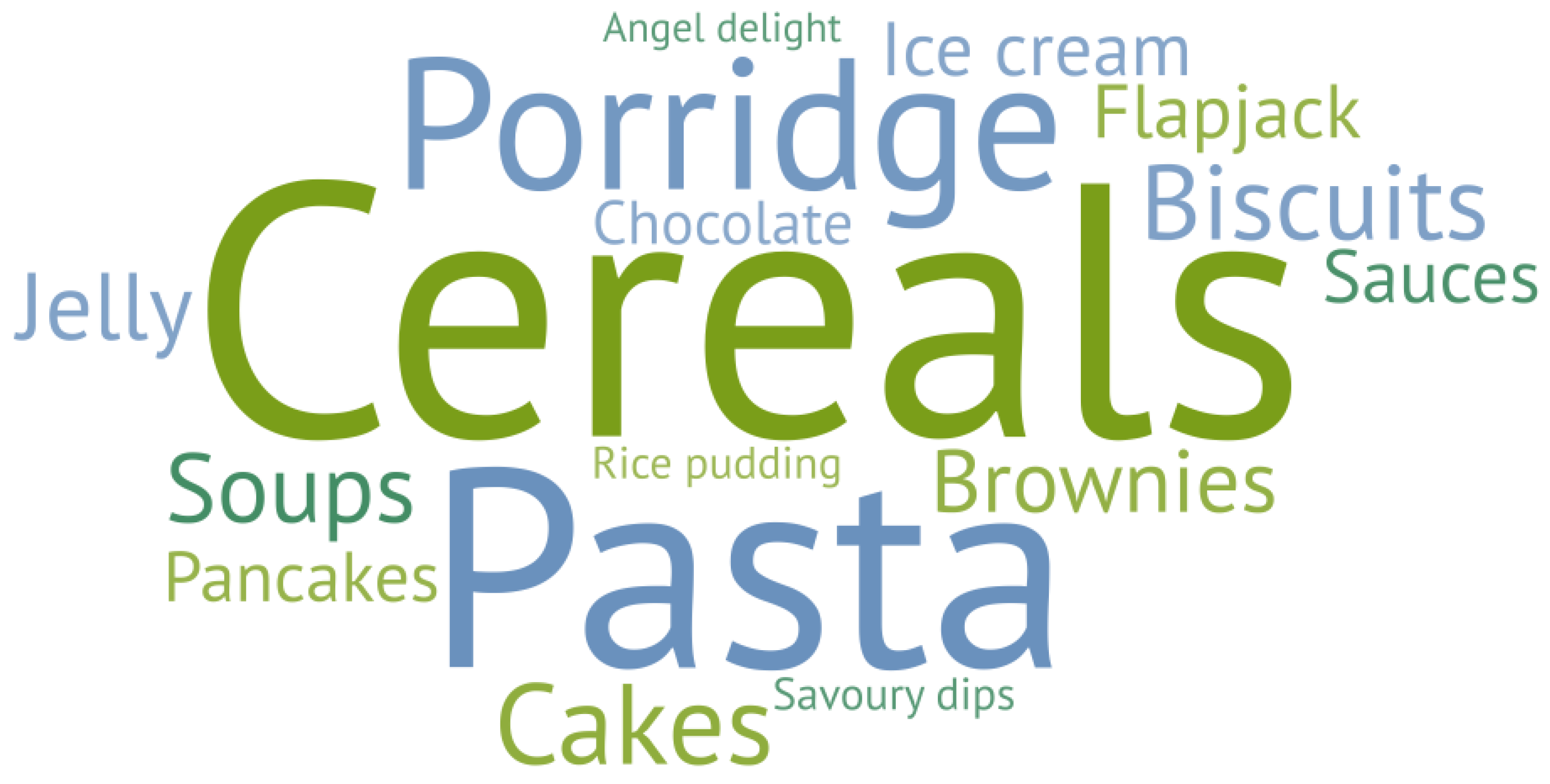
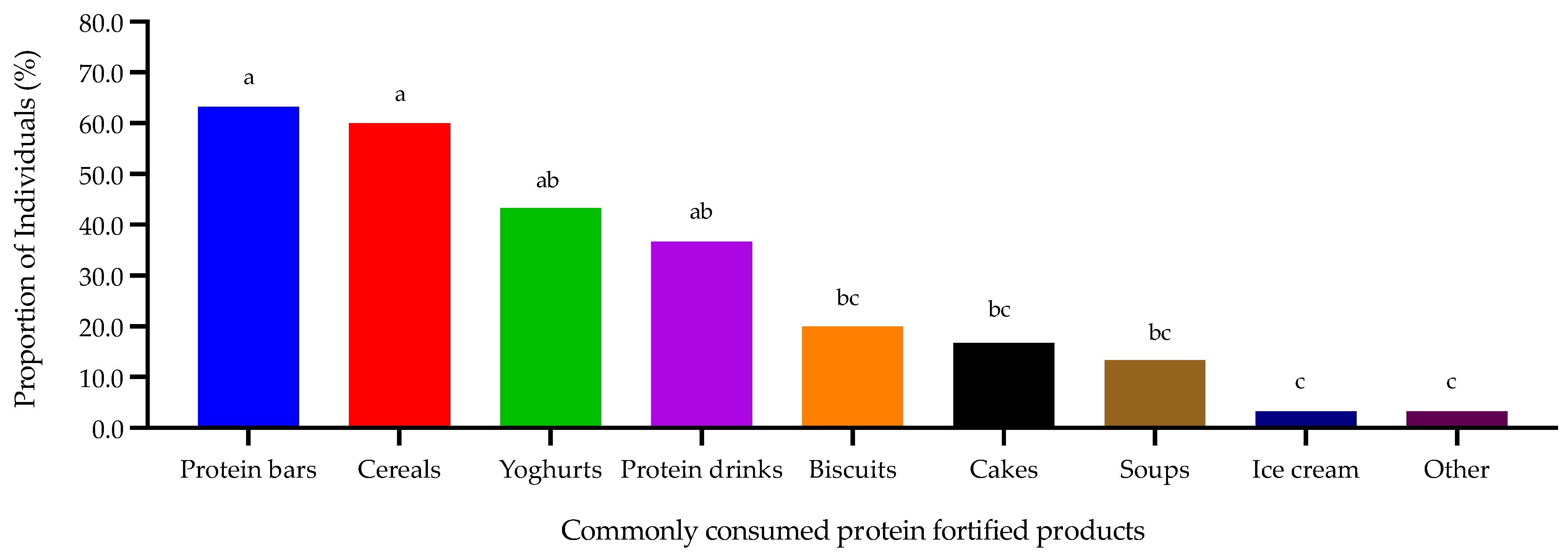
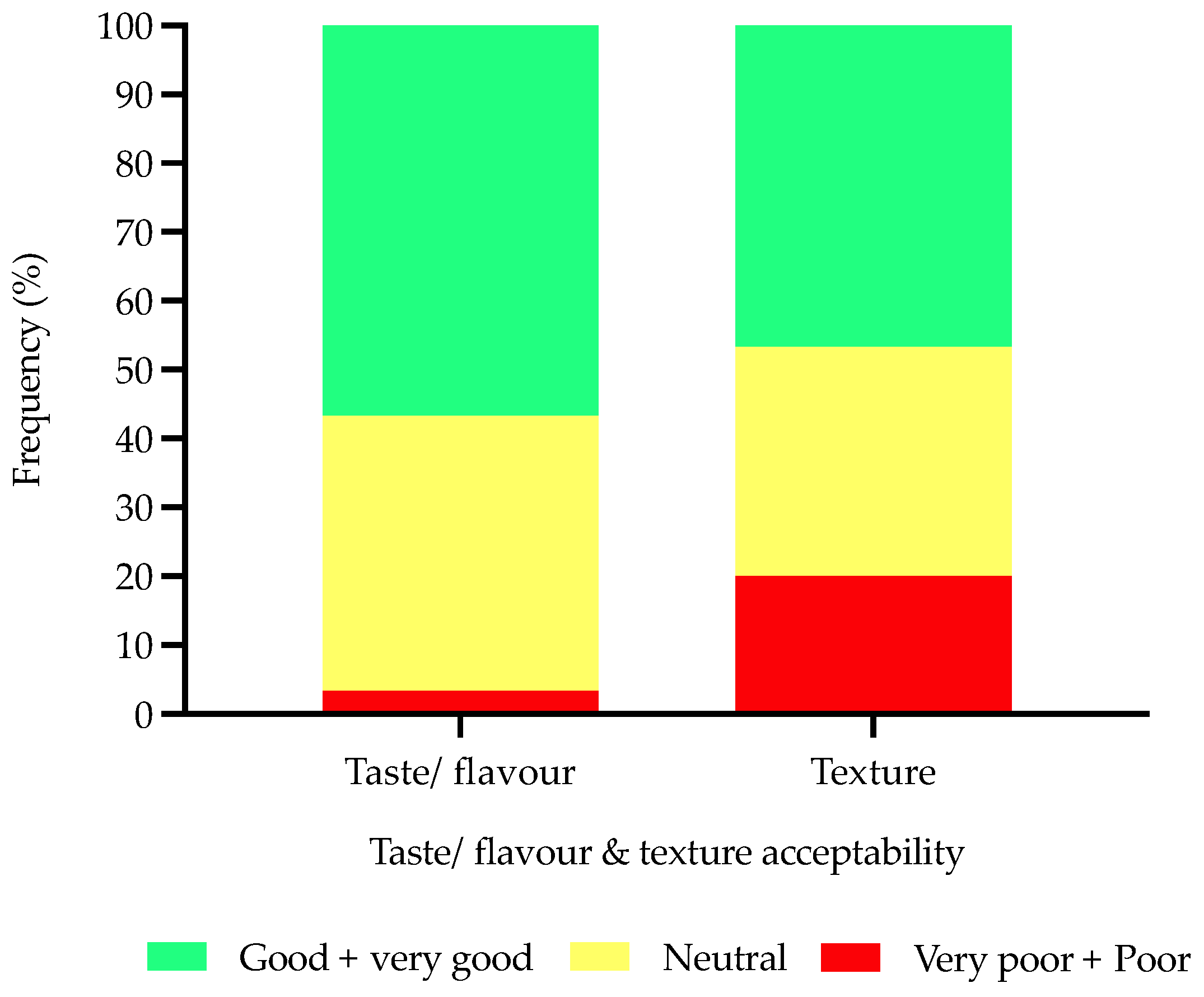
3.3. Protein Fortification Attitudes Questionnaire
4. Discussion
4.1. Initial Literature and Market Review on Protein-Fortified Products
4.2. Portion Size Questionnaire
4.3. Protein Fortification Attitudes Questionnaire
4.4. Practical Suggestions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Office for National Statistics. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/articles/overviewoftheukpopulation/november2018 (accessed on 2 January 2019).
- Armarya, S.; Singh, K.; Sabharwal, M. Changes during ageing and their association with malnutrition. J. Clin. Gerontol. Geriatr. 2015, 6, 78–84. [Google Scholar] [CrossRef]
- Stratton, R.; Smith, T.; Gabe, S. Managing Malnutrition to Improve Lives and Save Money. Available online: https://www.bapen.org.uk/pdfs/reports/mag/managing-malnutrition.pdf (accessed on 3 January 2019).
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Philips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence based recommendation for optimal dietary protein intake in older people: A position paper from the PROT-AGE study group. JAMA 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Deutz, N.E.P.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A. Protein intake and exercise for optimal muscle function with ageing: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Hengeveld, L.M.; Boer, J.M.A.; Gaudreau, P.; Heymans, M.W.; Jagger, C.; Mendonça, N.; Ocke, M.C.; Presse, N.; Sette, S.; Simonsick, E.M.; et al. Prevalence of protein intake below recommended in community-dwelling older adults: A meta-analysis across cohorts from the PROMISS consortium. J. Cachexia Sarcopenia Muscle 2020, 11, 1212–1222. [Google Scholar] [CrossRef]
- Harper, W.J. Model food systems and protein functionality. In Milk Proteins: From Expression to Food, 1st ed.; Thompson, A., Boland, M., Singh, H., Eds.; Academic Press: New York, NY, USA, 2009; pp. 409–422. [Google Scholar]
- Dangin, M.; Guillet, C.; Garcia-Rodenas, C.; Gachon, P.; Bouteloup-Demange, C.; Reiffers-Magnani, K.; Fauquant, J.; Ballevre, O.; Beaufrere, B. The rate of protein digestion affects protein gain differently during ageing in humans. J. Physiol. 2003, 549, 635–644. [Google Scholar] [CrossRef]
- Hoffman, J.R.; Falvo, M.J. Protein—Which is best? J. Sci. Med. 2004, 3, 118–130. [Google Scholar]
- Madureira, A.R.; Pereira, C.I.; Gomes, A.M.P.; Pintado, M.E.; Malcata, F.X. Bovine whey proteins—Overview on their main biological properties. Food Res. Int. 2007, 40, 1197–1211. [Google Scholar] [CrossRef]
- Pennings, B.; Boirie, Y.; Senden, J.M.; Gijsen, A.P.; Kuipers, H.; van Loon, L.J. Whey protein stimulates postprandial muscle protein accretion more effectively than do casein and casein hydrolysate in older men. Am. J. Clin. Nutr. 2011, 93, 997–1005. [Google Scholar] [CrossRef]
- Solak, B.B.; Akin, N. Health benefits of whey protein: A review. J. Food Sci. Eng. 2012, 2, 129–137. [Google Scholar]
- Sahathevan, S.; Se, C.H.; Ng, S.H.; Khor, B.H.; Chinna, K.; Goh, B.L.; Gafor, H.A.; Bavanandan, S.; Ahmad, G.; Karupaiah, T. Clinical efficacy and feasibility of whey protein isolates supplementation in malnourished peritoneal dialysis patients: A multi- centre, parallel, open-label randomised controlled trial. Clin. Nutr. ESPEN 2018, 25, 68–77. [Google Scholar] [CrossRef]
- Giezenaar, C.; Trahair, L.G.; Rigda, R.; Hutchison, A.T.; Feinle-Bisset, C.; Luscombe-Marsh, N.D.; Hausken, T.; Jones, K.L. Lesser suppression of energy intake by orally ingested whey protein in healthy older men compared with young controls. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2015, 309, 845–854. [Google Scholar] [CrossRef] [PubMed]
- Giezenaar, C.; Trahair, L.G.; Luscombe-Marsh, N.D.; Hausken, T.; Standfield, S.; Jones, K.L.; Lange, K.; Horowitz, M.; Chapman, I.; Soenen, S. Effects of randomized whey-protein loads on energy intake, appetite, gastric emptying, and plasma gut hormone concentrations in older men and women. Am. J. Clin. Nutr. 2017, 106, 865–877. [Google Scholar] [CrossRef] [PubMed]
- Ben-Harchache, S.; Roche, H.M.; Corish, C.A.; Horner, K.M. The Impact of Protein Supplementation on Appetite and Energy Intake in Healthy Older Adults: A Systematic Review with Meta-Analysis. Adv. Nutr. 2021, 12, 490–502. [Google Scholar] [CrossRef] [PubMed]
- Pires, M.A.; Pastrana, L.M.; Fucinos, P.; Abreu, C.S.; Oliveira, S.M. Sensorial Perception of Astringency: Oral Mechanisms and Current Analysis Methods. Foods 2020, 9, 1124. [Google Scholar] [CrossRef] [PubMed]
- Carter, B.G.; Foegeding, E.A.; Drake, M.A. Invited review: Astringency in whey protein beverages. J. Dairy Sci. 2020, 103, 5793–5804. [Google Scholar] [CrossRef]
- Norton, V.; Lignou, S.; Methven, L. Influence of Age and Individual Differences on Mouthfeel Perception of Whey Protein-Fortified Products: A Review. Foods 2021, 10, 433. [Google Scholar] [CrossRef]
- Hubbard, G.P.; Elia, M.; Holdoway, A.; Stratton, R.J. A systematic review of compliance to oral nutritional supplements. Clin. Nutr. 2012, 31, 293–312. [Google Scholar] [CrossRef]
- Gosney, M. Are we wasting our money on food supplements in elder care wards? J. Adv. Nurs. 2003, 43, 275–280. [Google Scholar] [CrossRef]
- Nieuwenhuizen, W.F.; Weenen, H.; Rigby, P.; Hetherington, M.M. Older adults and patients in need of nutritional support: Review of current treatment options and factors influencing nutritional intake. Clin. Nutr. 2010, 29, 160–169. [Google Scholar] [CrossRef]
- Munk, T.; Beck, A.M.; Holst, M.; Rosenbom, E.; Rasmussen, H.H.; Nielsen, M.A.; Thomsen, T. Positive effect of protein supplementation hospital food on protein intake in patients at nutritional risk: A randomised controlled trial. J. Hum. Nutr. Diet. 2014, 27, 122–132. [Google Scholar] [CrossRef]
- Appleton, K.M.; Smith, E. A role for identification in the gradual decline in the pleasantness of flavours with age. J. Gerontol. Psychol. Sci. 2015, 71, 987–994. [Google Scholar] [CrossRef]
- Morilla-Herrera, J.C.; Martin-Santos, F.J.; Caro-Bautista, J.; Saucedo-Figueredo, C.; Garcia-Mayor, S.; Morales-Asencio, J.M. Effectiveness of food based fortification in older people a systematic review and meta-analysis. J. Nutr. Health Aging 2016, 20, 178–184. [Google Scholar] [CrossRef]
- Beelen, J.; de Roos, N.M.; de Groot, L.C.P.G.M. Protein enrichment of familiar foods as an innovative strategy to increase protein intake in institutionalized elderly. J. Nutr. Health Aging 2017, 21, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Beelen, J.; de Roos, N.M.; de Groot, L.C.P.G.M. A 12 week intervention with protein enriched foods and drinks improved protein intake but not physical performance of older patients during the first 6 months after hospital release: A randomised controlled trial. Br. J. Nutr. 2017, 117, 1541–1549. [Google Scholar] [CrossRef]
- Mills, S.R.; Wilcox, C.R.; Ibrahim, K.; Roberts, H.C. Can fortified foods and snacks increase the energy and protein intake of hospitalised older patients? A systematic review. J. Hum. Nutr. Diet. 2018, 31, 379–389. [Google Scholar] [CrossRef]
- Norton, V.; Lignou, S.; Faka, F.; Methven, L. Individual variation in mouthfeel sensitivity: Investigating influences of whey protein content, consumer age, food format and fat addition. Food Qual. Prefer. 2022, 101, 104638. [Google Scholar] [CrossRef]
- Morley, J. Workshop: Anorexia during disease—From research to clinical practice anorexia, sarcopenia and ageing. Nutrition 2001, 17, 660–663. [Google Scholar] [CrossRef]
- Methven, L.; Allen, V.; Withers, C.; Gosney, M.A. Ageing and Taste. Proc. Nutr. Soc. 2012, 71, 556–565. [Google Scholar] [CrossRef]
- Vandenberghe-Descamps, M.; Sulmont-Rosse, C.; Septier, C.; Feron, G.; Laboure, H. Using food comfortability to compare foods sensory characteristics expectations of elderly people with or without oral health problems. J. Texture Stud. 2017, 48, 280–287. [Google Scholar] [CrossRef]
- Hung, Y.; Wijnhoven, H.A.H.; Visser, M.; Verbeke, W. Appetite and protein intake strata of older adults in the European Union: Socio-demographic and health characteristics, diet-related and physical activity behaviours. Nutrients 2019, 11, 777. [Google Scholar] [CrossRef] [PubMed]
- British Association for Parenteral and Enteral Nutrition. Available online: https://www.bapen.org.uk/nutrition-support/nutrition-by-mouth/oral-nutritional-supplements (accessed on 8 January 2019).
- European Commission. Available online: https://ec.europa.eu/food/safety/labelling_nutrition/claims/nutrition_claims_en (accessed on 12 September 2019).
- National Institute for Health and Care Excellence. Available online: https://bnf.nice.org.uk/borderline-substance-taxonomy/nutritional-supplements-5-g-or-more-protein100-ml.html (accessed on 28 May 2019).
- British Dietetic Association. Available online: https://www.bda.uk.com/uploads/assets/c24296fe-8b4d-4626-aeebb6cf2d92fccb/NutritionHydrationDigest.pdf (accessed on 10 January 2019).
- Phillips, S.M.; Chevalier, S.; Leidy, H.J. Protein ‘requirements’ beyond the RDA: Implications for optimizing health. Appl. Physiol. Nutr. Metab. 2016, 41, 565–572. [Google Scholar] [CrossRef]
- Roberts, H.C.; Lim, S.E.R.; Cox, N.J.; Ibrahim, K. The challenges of managing undernutrition in older people with frailty. Nutrients 2019, 11, 808. [Google Scholar] [CrossRef] [PubMed]
- Norton, V.; Lignou, S.; Bull, S.P.; Gosney, M.A.; Methven, L. Consistent effects of whey protein fortification on consumer perception and liking of solid food matrices (cakes and biscuits) regardless of age and saliva flow. Foods 2020, 9, 1328. [Google Scholar] [CrossRef] [PubMed]
- Van Til, A.J.; Naumann, E.; Cox-Claessens, I.J.H.M.; Kremer, S.; Boelsma, E.; De Van Der Schueren, M.A.E. Effects of the daily consumption of protein enriched bread and protein enriched drinking yoghurt on the total protein intake in older adults in a rehabilitation centre: A single blinded randomised controlled trial. J. Nutr. Health Aging 2015, 19, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Stelten, S.; Dekker, I.M.; Ronday, E.M.; Thijs, A.; Boelsma, E.; Peppelenbos, H.W.; de van der Schueren, M.A.E. Protein-enriched ‘regular products’ and their effect on protein intake in acute hospitalized older adults; a randomized controlled trial. Clin. Nutr. 2015, 34, 409–414. [Google Scholar] [CrossRef]
- Beelen, J.; Vasse, E.; Janssen, N.; Janse, A.; de Roos, N.M.; de Groot, L.C.P.G.M. Protein-enriched familiar foods and drinks improve protein intake of hospitalized older patients: A randomized controlled trial. Clin. Nutr. 2018, 37, 1186–1192. [Google Scholar] [CrossRef]
- Mortensen, M.N.; Larsen, A.K.; Skadhauge, L.B.; Hogsted, R.H.; Beermann, T.; Cook, M.E.; Rasmussen, H.H.; Mikkelsen, B.E.; Holst, M. Protein and energy intake improved by in-between meals: An intervention study in hospitalized patients. Clin. Nutr. ESPEN 2019, 30, 113–118. [Google Scholar] [CrossRef]
- Campbell, K.L.; Webb, L.; Vivanti, A.; Varghese, P.; Ferguson, M. Comparison of three interventions in the treatment of malnutrition in hospitalised older adults: A clinical trial. Nutr. Diet. 2014, 70, 325–331. [Google Scholar] [CrossRef]
- Borkent, J.W.; Beelen, J.; Linschooten, J.O.; Roodenbury, A.J.C.; de van der Schueren, M.A.E. The ConsuMEER study: A randomised trial towards the effectiveness of protein-rich ready-made meals and protein-rich dairy products in increasing protein intake of community-dwelling older adults after switching from self-prepared meals towards ready-made meals. J. Nutr. Sci. 2019, 8, e30. [Google Scholar]
- Tsikritzi, R.; Moynihan, P.J.; Gosney, M.A.; Allen, V.J.; Methven, L. The effect of macro- and micro-nutrient fortification of biscuits on their sensory properties and on hedonic liking of older people. J. Sci. Food Agric. 2014, 94, 2040–2048. [Google Scholar] [CrossRef]
- Tsikritzi, R.; Wang, J.; Collins, V.J.; Allen, V.J.; Mavrommatis, Y.; Moynihan, P.J.; Gosney, M.A.; Kennedy, O.B.; Methven, L. The effect of nutrient fortification of sauces on product stability, sensory properties, and subsequent liking by older adults. J. Food Sci. 2015, 80, 1100–1110. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Perez-Cueto, F.J.A.; Bredie, W.L. Sensory-driven development of protein-enriched rye bread and cream cheese for the nutritional demands of older adults. Nutrients 2018, 10, 1006. [Google Scholar] [CrossRef]
- Wendin, K.; Hoglund, E.; Andersson, M.; Rothenberg, E. Protein enriched foods and healthy ageing: Effects of protein fortification on muffin characteristics. Agro. Food Ind. Hi-Tech. 2017, 28, 16–18. [Google Scholar]
- Hoglund, E.; Albinsson, B.; Stuhr-Olsson, G.; Signas, M.; Karlsson, C.; Rothenberg, E.; Wendin, K. Protein and energy enriched muffins designed for nutritional needs of older adults. Int. J. Food Sci. Nutr. 2017, 2, 555592. [Google Scholar] [CrossRef]
- Van Wymelbeke, V.; Brondel, L.; Bon, F.; Martin-Pfitzenmeyer, L.; Manckoundia, P. An innovative brioche enriched in protein and energy improves the nutritional status of malnourished nursing home residents compared to oral nutritional supplement and usual breakfast: FARINE+ project. Clin. Nutr. ESPEN 2016, 15, 93–100. [Google Scholar] [CrossRef]
- Ridge, A.; Devine, A.; Lyons-Walls, P.; Conlon, J.; Lo, J. The impact of whey protein supplementation in older adults on nutrient intakes and satiety over an 11-week exercise intervention. Food Qual. Prefer. 2018, 68, 72–79. [Google Scholar] [CrossRef]
- Bauer, J.M.; Verlaan, S.; Bautmans, I.; Brandt, K.; Donini, L.M.; Maggio, M.; McMurdo, M.E.T.; Mets, T.; Seal, C.; Wijers, S.L.; et al. Effects of a vitamin D and leucine-enriched whey protein nutritional supplement on measures of sarcopenia in older adults, the PROVIDE study: A randomised, double blind, placebo controlled trial. J. Am. Med. Dir. Assoc. 2015, 16, 740–747. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Somoto, Y.; Mitsuyama, E.; Tanaka, A.; Yuda, N.; Nakada, H.; Yamada, A.; Yamauchi, K.; Abe, F.; Nagasawa, T. Supplementation of protein-free diet with whey protein hydrolysates prevents skeletal muscle mass loss in rats. JNIM 2016, 4, 1–5. [Google Scholar] [CrossRef]
- Norton, V.; Lignou, S.; Bull, S.P.; Gosney, M.A.; Methven, L. An investigation of the influence of age and saliva flow on the oral retention of whey protein and its potential effect on the perception and acceptance of whey protein beverages. Nutrients 2020, 12, 2506. [Google Scholar] [CrossRef]
- Norton, V.; Lignou, S.; Methven, L. Whey protein derived mouthdrying found to relate directly to retention post consumption but not to induced differences in salivary flow rate. Foods 2021, 10, 587. [Google Scholar] [CrossRef]
- Norton, V.; Lignou, S.; Faka, M.; Rodriguez-Garcia, J.; Methven, L. Investigating methods to mitigate whey protein derived mouthdrying. Foods 2021, 10, 2066. [Google Scholar] [CrossRef] [PubMed]
- Withers, C.A.; Lewis, M.J.; Gosney, M.A.; Methven, L. Potential sources of mouth drying in beverages fortified with dairy proteins: A comparison of casein- and whey-rich ingredients. J. Dairy Sci. 2014, 97, 1233–1247. [Google Scholar] [CrossRef] [PubMed]
- Lampmann, L.; Hannink, A.; Kiesswetter, E.; Emberger-Klein, A.; Volkert, D.; Menrad, K. Protein for Community-Dwelling Older People: Aspects That Influence the Perception of Commercially Available Protein Drinks. Front. Nutr. 2020, 7, 100. [Google Scholar] [CrossRef] [PubMed]
- Van den Heuvel, E.; Newbury, A.; Appleton, K.M. The psychology of nutrition with advancing age: Focus on food neophobia. Nutrients 2019, 11, 151. [Google Scholar] [CrossRef]
- Kennedy, O.; Law, C.; Methven, L.; Mottram, D.; Gosney, M. Investigating age related changes in taste and affects on sensory perceptions of oral nutritional supplements. Age Ageing 2010, 39, 733–738. [Google Scholar] [CrossRef]
- Van der Zanden, L.D.T.; van Kleef, E.; de Wijk, R.A.; van Trijp, H.C. Knowledge, perceptions and preferences of elderly regarding protein-enriched functional food. Appetite 2014, 80, 16–22. [Google Scholar] [CrossRef]
- Song, X.; Federico, J.A.; Pérez-Cueto, F.J.; Bølling Laugesen, S.M.; van der Zanden, L.D.T.; Giacalone, D. Older consumers’ attitudes towards food carriers for protein-enrichment. Appetite 2019, 135, 10–19. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Products | Portion Size | |||||
|---|---|---|---|---|---|---|
| Drinks | ||||||
| Water | 25 mL | 100 mL | 175 mL | 300 mL | 375 mL | Comment |
| Juice | 25 mL | 100 mL | 175 mL | 300 mL | 375 mL | Comment |
| Soft drink | 25 mL | 100 mL | 175 mL | 300 mL | 375 mL | Comment |
| Milk | 25 mL | 100 mL | 175 mL | 300 mL | 375 mL | Comment |
| Milkshake | 25 mL | 100 mL | 175 mL | 300 mL | 375 mL | Comment |
| Protein beverage | 25 mL | 100 mL | 175 mL | 300 mL | 375 mL | Comment |
| Hot drink | - | 190 mL | 220 mL | 225 mL | 260 mL | Comment |
| Cakes | ||||||
| Carrot cake | - | - | 50 g | 100 g | 200 g | Comment |
| Chocolate cake | - | 40 g | 70 g | 138 g | - | Comment |
| Fruit cake | - | 26 g | 60 g | 121 g | - | Comment |
| Malt loaf | - | 30 g | 61 g | 91 g | - | Comment |
| Cupcakes | 10 g | 25 g | 35 g | 70 g | - | Comment |
| Food Matrix | Protein Source | Serving Size | Protein (g) | |||
|---|---|---|---|---|---|---|
| Serving Size | 100 g or mL | |||||
| Literature-based studies | Bread [26,27,41,42,43] | - † | 27–35 g † | 5.6–7.9 | - | |
| Yoghurt [41,42] | WPC | 100–250 mL | 8.0–20.0 | 8.0 ^ | ||
| Fruit juices [26,27,43] | - | 150–200 mL | 10.0–10.6 | - | ||
| Soups [23,26,27,43] | -MP ^ | 75–79 g & 150 mL | 6.9–10.1 | - | ||
| Mashed potato [26,27,43] | - | 150 g | 8.4–10.5 | - | ||
| Dairy drinks [27,43] | - | 150 mL | 10.1 | - | ||
| Cakes [27,43] | - | 65 g | 9.9 | - | ||
| Ice cream [27,43] | - | 100 mL | 10.0 | 10.0 ^ | ||
| Meat [27,43] | - | 50–80 g | 12.4–22.0 | - | ||
| Milkshake (orange) [44] |  | Combined approach of high protein products & protein powder (using whey, gelatin or pea protein) | 150 g | 16.0 | - | |
| Chocolate cake [44] | 56 g | 7.6 | - | |||
| Pizza bun [44] | 40 g | 6.0 | - | |||
| Fruit salad [44] | 65 g | 8.4 | - | |||
| Bun [44] | 40 g | 4.9 | - | |||
| Cheese crackers [44] | 10 g | 1.4 | - | |||
| Sandwich (ham) [44] | 40 g | 5.3 | - | |||
| Jelly (apple & cream) [44] | 50 g | 9.5 | - | |||
| Enriched breakfast dishes [23] | MP | 60–100 g | 7.4–11.5 | 11.5 ^ | ||
| Enriched fish dishes [23] | MP | 55–70 g | 7.6–8.9 | - | ||
| Enriched meat dishes [23] | MP | 55–75 g | 6.5–7.9 | - | ||
| Enriched side dishes [23] | MP | 47–75 g | 6.1–7.7 | - | ||
| Enriched desserts [23] | MP | 52–110 g | 6.2–7.6 | 6.9 ^ | ||
| High energy and/or protein snacks [45] | - | - | 0.0–6.0 | - | ||
| Protein rich ready meals [46] | - | 500–550 g | 30.5 (av) | - | ||
| Protein rich dairy products [46] | - | 30 g & 150 mL | 5.1–11.6 | - | ||
| Biscuit [47] | WPI | 40 g | 5.0 | 12.4 | ||
| Sauces [48] | WPI | 50 g | 0.5–2.3 | 0.9–4.5 | ||
| Rye bread [49] | WPH & WPI | 35 g | 4.8–7.0 | - | ||
| Cream cheese [49] | WPH & WPI | 25 g | 2.9–3.0 | 11.6–11.9 | ||
| Muffins [50,51] | WP, AF & SF | 100 g | 9.1–14.1 | 9.1–14.1 | ||
| Brioche [52] | RP, MP | 65 g | 12.8 | - | ||
| Beverages [53,54] | WPC, WP | 150–200 mL | 20.7–24.0 | - | ||
| Clinical settings (ONS products) | ONS * | MP, MPC, SP, MPI, SPI & CA | 125–200 mL | 11.2–20.0 | 5.6–10.0 | |
| ONS soup * | MP, PP, SMP, MPC | 150–200 mL | 6.0–20.0 | 4.2–16.1 | ||
| ONS juice * | WP, WPI, MP, SPI | 150–220 mL | 7.8–11.0 | 3.9–16.2 | ||
| ONS yoghurt * | WP, MPI, SMP | 125 g & 200 mL | 9.3–15.0 | 5.9–7.5 | ||
| ONS dessert * | MP, MPC, MPI, SPI & CA | 125 g | 7.1–12.5 | 7.5–10.0 | ||
| ONS other * | WI & CH | 118 mL | 20.0 | 16.9 | ||
| Retail market-based products | Protein milk * | WP, MP, MPC | 330–500 mL | 25.0 | 5.0–7.6 | |
| Protein yoghurt * | Quark (milk) | 150–200 g | 15.0–22.0 | 10.0–11.4 | ||
| Protein cereals * | WPC, MPC, SMP & SPI | 40–75 g | 8.4–20.6 | 19.0–27.4 | ||
| Protein bars * | WPC, WPI, WP, SPI, MP, CA, MPI, WPH & PPI | 30–65 g | 4.5–20.0 | 15.0–34.0 | ||
| Protein flapjack * | WPC, WP, HWPI, SMP, MP, PP & HWHP | 40–88 g | 10.0–22.0 | 23.0–25.0 ^ | ||
| Protein balls * | WPI, WP, SP & MP | 35–50 g | 9.8–15.0 | 20.5–43.0 | ||
| Protein brownies * | WP, WPC, HWHP, CA, MP & SP | 40–75 g | 10.6–23.0 | 20.0–30.0 | ||
| Protein cakes * | WPC, WP, MPI, SPI & MP | 30–60 g | 7.9–15.0 | 25.0–26.0 | ||
| Protein pancakes * | WPC, SMP | 45 g | 16.0 | 35.5 | ||
| Protein cookies * | WPI, MP, MPI, SP & HWHP | 59–75 g | 13.0–38.0 | 18.0–50.0 ^ | ||
| Protein chocolate * | WPI | 70 g | 19.0–19.5 | 27.0–27.9 | ||
| Protein chocolate bars * | WPC, WP, SMP, MP & MPI | 47–51 g | 10.1–15.0 | 20.2–30.0 | ||
| Protein crisps * | WPI, WP, CA, MPI & SP | 32–50 g | 18.0–20.0 | - | ||
| Protein other * | WPI, WP, SMP, SPI & SPC | 23–36 g | 7.7–9.0 | 25.0–33.4 | ||
| Protein milk * | WP, MP, MPC | 330–500 mL | 25.0 | 5.0–7.6 | ||
| Protein yoghurt * | Quark (milk) | 150–200 g | 15.0–22.0 | 10.0–11.4 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Norton, V.; Lignou, S.; Methven, L. Promoting Protein Intake in an Ageing Population: Product Design Implications for Protein Fortification. Nutrients 2022, 14, 5083. https://doi.org/10.3390/nu14235083
Norton V, Lignou S, Methven L. Promoting Protein Intake in an Ageing Population: Product Design Implications for Protein Fortification. Nutrients. 2022; 14(23):5083. https://doi.org/10.3390/nu14235083
Chicago/Turabian StyleNorton, Victoria, Stella Lignou, and Lisa Methven. 2022. "Promoting Protein Intake in an Ageing Population: Product Design Implications for Protein Fortification" Nutrients 14, no. 23: 5083. https://doi.org/10.3390/nu14235083
APA StyleNorton, V., Lignou, S., & Methven, L. (2022). Promoting Protein Intake in an Ageing Population: Product Design Implications for Protein Fortification. Nutrients, 14(23), 5083. https://doi.org/10.3390/nu14235083