

Predictive Value of Temporal Muscle Thickness for Sarcopenia after Acute Stroke in Older Patients
 , , , ,
, , , ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Temporal Muscle Thickness
2.3. Sarcopenia Parameters
2.4. Other Parameters
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nishiyama, A.; Wakabayashi, H.; Nishioka, S.; Nagano, A.; Momosaki, R. Energy Intake at Admission for Improving Activities of Daily Living and Nutritional Status among Convalescent Stroke Patients. Neurol. Med. Chir. 2019, 59, 313–320. [Google Scholar] [CrossRef]
- Nishioka, S.; Wakabayashi, H.; Nishioka, E.; Yoshida, T.; Mori, N.; Watanabe, R. Nutritional Improvement Correlates with Recovery of Activities of Daily Living among Malnourished Elderly Stroke Patients in the Convalescent Stage: A Cross-Sectional Study. J. Acad. Nutr. Diet. 2016, 116, 837–843. [Google Scholar] [CrossRef]
- Kokura, Y.; Wakabayashi, H.; Nishioka, S.; Maeda, K. Nutritional intake is associated with activities of daily living and complications in older inpatients with stroke. Geriatr. Gerontol. Int. 2018, 18, 1334–1339. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, Y.; Wakabayashi, H.; Bise, T.; Nagano, F.; Shimazu, S.; Shiraishi, A.; Yamaga, M.; Koga, H. Sarcopenia is associated with worse recovery of physical function and dysphagia and a lower rate of home discharge in Japanese hospitalized adults undergoing convalescent rehabilitation. Nutrition 2019, 61, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, Y.; Wakabayashi, H.; Bise, T.; Tanoue, M. Prevalence of sarcopenia and its association with activities of daily living and dysphagia in convalescent rehabilitation ward inpatients. Clin. Nutr. 2018, 37, 2022–2028. [Google Scholar] [CrossRef]
- Nozoe, M.; Noguchi, M.; Kubo, H.; Kanai, M.; Shimada, S. Association between the coexistence of premorbid sarcopenia, frailty, and disability and functional outcome in older patients with acute stroke. Geriatr. Gerontol. Int. 2022, 22, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Yue, T.; Liu, Y. New understanding of the pathogenesis and treatment of stroke-related sarcopenia. Biomed. Pharmacother. 2020, 131, 110721. [Google Scholar] [CrossRef]
- Gingrich, A.; Volkert, D.; Kiesswetter, E.; Thomanek, M.; Bach, S.; Sieber, C.C.; Zopf, Y. Prevalence and overlap of sarcopenia, frailty, cachexia and malnutrition in older medical inpatients. BMC Geriatr. 2019, 19, 120. [Google Scholar] [CrossRef]
- Shimizu, A.; Fujishima, I.; Maeda, K.; Murotani, K.; Ohno, T.; Nomoto, A.; Nagami, S.; Nagano, A.; Sato, K.; Ueshima, J.; et al. Association between food texture levels consumed and the prevalence of malnutrition and sarcopenia in older patients after stroke. Eur. J. Clin. Nutr. 2022, 76, 1576–1582. [Google Scholar] [CrossRef]
- Nii, M.; Maeda, K.; Wakabayashi, H.; Nishioka, S.; Tanaka, A. Nutritional Improvement and Energy Intake Are Associated with Functional Recovery in Patients after Cerebrovascular Disorders. J. Stroke Cerebrovasc. Dis. 2016, 25, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Kokura, Y.; Kato, M.; Taniguchi, Y.; Kimoto, K.; Okada, Y. Energy intake during the acute phase and changes in femoral muscle thickness in older hemiplegic inpatients with stroke. Nutrition 2020, 70, 110582. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. J. Cachexia Sarcopenia Muscle 2019, 10, 207–217. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Katsuki, M.; Kakizawa, Y.; Nishikawa, A.; Yamamoto, Y.; Uchiyama, T.; Agata, M.; Wada, N.; Kawamura, S.; Koh, A. Temporal Muscle and Stroke-A Narrative Review on Current Meaning and Clinical Applications of Temporal Muscle Thickness, Area, and Volume. Nutrients 2022, 14, 687. [Google Scholar] [CrossRef] [PubMed]
- Nozoe, M.; Kubo, H.; Kanai, M.; Yamamoto, M.; Okakita, M.; Suzuki, H.; Shimada, S.; Mase, K. Reliability and validity of measuring temporal muscle thickness as the evaluation of sarcopenia risk and the relationship with functional outcome in older patients with acute stroke. Clin. Neurol. Neurosurg. 2021, 201, 106444. [Google Scholar] [CrossRef]
- Steindl, A.; Leitner, J.; Schwarz, M.; Nenning, K.H.; Asenbaum, U.; Mayer, S.; Woitek, R.; Weber, M.; Schöpf, V.; Berghoff, A.S.; et al. Sarcopenia in Neurological Patients: Standard Values for Temporal Muscle Thickness and Muscle Strength Evaluation. J. Clin. Med. 2020, 9, 1272. [Google Scholar] [CrossRef]
- Li, Y.X.; Hou, J.; Liu, W.Y. Long-term prognostic significance of sarcopenia in acute ischemic stroke. Medicine 2022, 101, e30031. [Google Scholar] [CrossRef] [PubMed]
- Sporns, P.B.; Muhle, P.; Hanning, U.; Suntrup-Krueger, S.; Schwindt, W.; Eversmann, J.; Warnecke, T.; Wirth, R.; Zimmer, S.; Dziewas, R. Atrophy of Swallowing Muscles Is Associated With Severity of Dysphagia and Age in Patients With Acute Stroke. J. Am. Med. Dir. Assoc. 2017, 18, 635.e1–635.e7. [Google Scholar] [CrossRef] [PubMed]
- Katsuki, M.; Kakizawa, Y.; Nishikawa, A.; Yamamoto, Y.; Uchiyama, T. Temporal muscle thickness and area are an independent prognostic factors in patients aged 75 or younger with aneurysmal subarachnoid hemorrhage treated by clipping. Surg. Neurol. Int. 2021, 12, 151. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, Y.; Yoshida, M.; Sato, A.; Fujimoto, Y.; Minematsu, T.; Sugama, J.; Sanada, H. Temporal muscle thickness as a new indicator of nutritional status in older individuals. Geriatr. Gerontol. Int. 2019, 19, 135–140. [Google Scholar] [CrossRef]
- Miyai, I.; Sonoda, S.; Nagai, S.; Takayama, Y.; Inoue, Y.; Kakehi, A.; Kurihara, M.; Ishikawa, M. Results of new policies for inpatient rehabilitation coverage in Japan. Neurorehabil. Neural Repair 2011, 25, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, A.B.; Dobson, E.T.A.; Rueden, C.T.; Tomancak, P.; Jug, F.; Eliceiri, K.W. The ImageJ ecosystem: Open-source software for image visualization, processing, and analysis. Protein Sci. 2021, 30, 234–249. [Google Scholar] [CrossRef]
- Yamada, Y.; Yamada, M.; Yoshida, T.; Miyachi, M.; Arai, H. Validating muscle mass cutoffs of four international sarcopenia-working groups in Japanese people using DXA and BIA. J. Cachexia Sarcopenia Muscle 2021, 12, 1000–1010. [Google Scholar] [CrossRef] [PubMed]
- van Swieten, J.C.; Koudstaal, P.J.; Visser, M.C.; Schouten, H.J.; van Gijn, J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z.; Harker, J.O.; Salvà, A.; Guigoz, Y.; Vellas, B. Screening for undernutrition in geriatric practice: Developing the short-form mini-nutritional assessment (MNA-SF). J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Kidd, D.; Stewart, G.; Baldry, J.; Johnson, J.; Rossiter, D.; Petruckevitch, A.; Thompson, A.J. The Functional Independence Measure: A comparative validity and reliability study. Disabil. Rehabil. 1995, 17, 10–14. [Google Scholar] [CrossRef]
- Cho, J.; Park, M.; Moon, W.J.; Han, S.H.; Moon, Y. Sarcopenia in patients with dementia: Correlation of temporalis muscle thickness with appendicular muscle mass. Neurol. Sci. 2022, 43, 3089–3095. [Google Scholar] [CrossRef]
- Gomes, G.G.C.; Palinkas, M.; da Silva, G.P.; Gonçalves, C.R.; Lopes, R.F.T.; Verri, E.D.; Fabrin, S.C.V.; Fioco, E.M.; Siéssere, S.; Regalo, S.C.H. Bite Force, Thickness, and Thermographic Patterns of Masticatory Muscles Post-Hemorrhagic Stroke. J. Stroke Cerebrovasc. Dis. 2022, 31, 106173. [Google Scholar] [CrossRef]
- Park, S.; Kim, Y.; Kim, S.A.; Hwang, I.; Kim, D.E. Utility of ultrasound as a promising diagnostic tool for stroke-related sarcopenia: A retrospective pilot study. Medicine 2022, 101, e30245. [Google Scholar] [CrossRef]
- Dhariwal, S.; Roy, A.; Taneja, S.; Bansal, A.; Gorsi, U.; Singh, S.; De, A.; Verma, N.; Premkumar, M.; Duseja, A.; et al. Assessment of Sarcopenia Using Muscle Ultrasound in Patients With Cirrhosis and Sarcopenic Obesity (AMUSE STUDY). J. Clin. Gastroenterol. 2022. [Google Scholar] [CrossRef]
- Nijholt, W.; Scafoglieri, A.; Jager-Wittenaar, H.; Hobbelen, J.S.M.; van der Schans, C.P. The reliability and validity of ultrasound to quantify muscles in older adults: A systematic review. J. Cachexia Sarcopenia Muscle 2017, 8, 702–712. [Google Scholar] [CrossRef]
- Miura, Y.; Tamai, N.; Kitamura, A.; Yoshida, M.; Takahashi, T.; Mugita, Y.; Tobita, I.; Arita, M.; Urai, T.; Dai, M.; et al. Diagnostic accuracy of ultrasound examination in detecting aspiration and pharyngeal residue in patients with dysphagia: A systematic review and meta-analysis. Jpn. J. Nurs. Sci. 2021, 18, e12396. [Google Scholar] [CrossRef]
- Yesil Cinkir, H.; Colakoglu Er, H. Is temporal muscle thickness a survival predictor in newly diagnosed glioblastoma multiforme? Asia Pac. J. Clin. Oncol. 2020, 16, e223–e227. [Google Scholar] [CrossRef]
- Kameyama, Y.; Ashizawa, R.; Honda, H.; Take, K.; Yoshizawa, K.; Yoshimoto, Y. Sarcopenia Affects Functional Independence Measure motor Scores in Elderly Patients with Stroke. J. Stroke Cerebrovasc. Dis. 2022, 31, 106615. [Google Scholar] [CrossRef]
- Lee, H.; Lee, I.H.; Heo, J.; Baik, M.; Park, H.; Lee, H.S.; Nam, H.S.; Kim, Y.D. Impact of Sarcopenia on Functional Outcomes Among Patients With Mild Acute Ischemic Stroke and Transient Ischemic Attack: A Retrospective Study. Front. Neurol. 2022, 13, 841945. [Google Scholar] [CrossRef]
- Nagano, A.; Nishioka, S.; Wakabayashi, H. Rehabilitation Nutrition for Iatrogenic Sarcopenia and Sarcopenic Dysphagia. J. Nutr. Health Aging 2019, 23, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Nishioka, S.; Aragane, H.; Suzuki, N.; Yoshimura, Y.; Fujiwara, D.; Mori, T.; Kanehisa, Y.; Iida, Y.; Higashi, K.; Yoshimura-Yokoi, Y.; et al. Clinical practice guidelines for rehabilitation nutrition in cerebrovascular disease, hip fracture, cancer, and acute illness: 2020 update. Clin. Nutr. ESPEN 2021, 43, 90–103. [Google Scholar] [CrossRef]
- Sakai, K.; Katayama, M.; Nakajima, J.; Inoue, S.; Koizumi, K.; Okada, S.; Suga, S.; Nomura, T.; Matsuura, N. Temporal muscle thickness is associated with the severity of dysphagia in patients with acute stroke. Arch. Gerontol. Geriatr. 2021, 96, 104439. [Google Scholar] [CrossRef]


{kind=link}
| Total Cohort n = 230 | |
|---|---|
| Sex, Male, n (%) | 125 (54.3) |
| Age, year | 77.2 ± 7.2 |
| Type of stroke, n (%) | |
| - Cerebral infarction | 136 (9.1) |
| - Cerebral hemorrhage | 87 (37.8) |
| - Subarachnoid hemorrhage | 7 (3.0) |
| Stroke onset to admission, days | 26 (19–36) |
| Charlson Comorbidity Index score | 1 (1–2) |
| Body mass index, kg/m2 C-reactive protein, mg/dL | 21.5 ± 3.5 0.69 ± 1.60 |
| Mini Nutritional Assessment—Short Form score | 7 (5–9) |
| Modified Rankin Scale score at stroke onset | 4 (3–4) |
| Functional Independence Measure score | 72 (49–92) |
| SMI, kg/m2 | 6.12 ± 1.09 |
| - Men | 6.61 ± 1.08 |
| - Women | 5.54 ± 0.76 |
| TMT, mm | 3.57 ± 1.45 |
| - Men | 3.98 ± 1.52 |
| - Women | 3.07 ± 1.20 |
| HGS, kg | 20.2 ± 9.8 |
| - Men | 25.1 ± 9.1 |
| - Women | 14.3 ± 7.0 |
| Total Cohort n = 235 | |
|---|---|
| Sex, Male, n (%) | 125 (53.2) |
| Age, year | 76.4 ± 6.95 |
| Type of stroke, n (%) | |
| -Cerebral infarction | 144 (61.3) |
| -Cerebral hemorrhage | 84 (35.7) |
| -Subarachnoid hemorrhage | 7 (3.0) |
| Stroke onset to admission, days | 26 (19–34) |
| Charlson Comorbidity Index score | 1 (1–2) |
| Body mass index, kg/m2 C-reactive protein, mg/dL | 21.6 ± 3.3 0.68 ± 1.90 |
| Mini Nutritional Assessment—Short Form score | 7 (5–9) |
| Modified Rankin Scale score at stroke onset | 4 (3–4) |
| Functional Independence Measure score | 77 (51–95) |
| HGS, kg -Men -Women | 20.9 ± 9.9 26.3 ± 8.65 14.7 ± 7.3 |
| SMI, kg/m2 -Men -Women | 6.25 ± 1.04 6.83 ± 0.94 5.60 ± 0.70 |
| TMT, mm -Men -Women | 3.63 ± 1.48 4.09 ± 1.53 3.10 ± 1.20 |
| Low SMI, n | 135 (57.4) |
| Low TMT, n | 103 (43.8) |
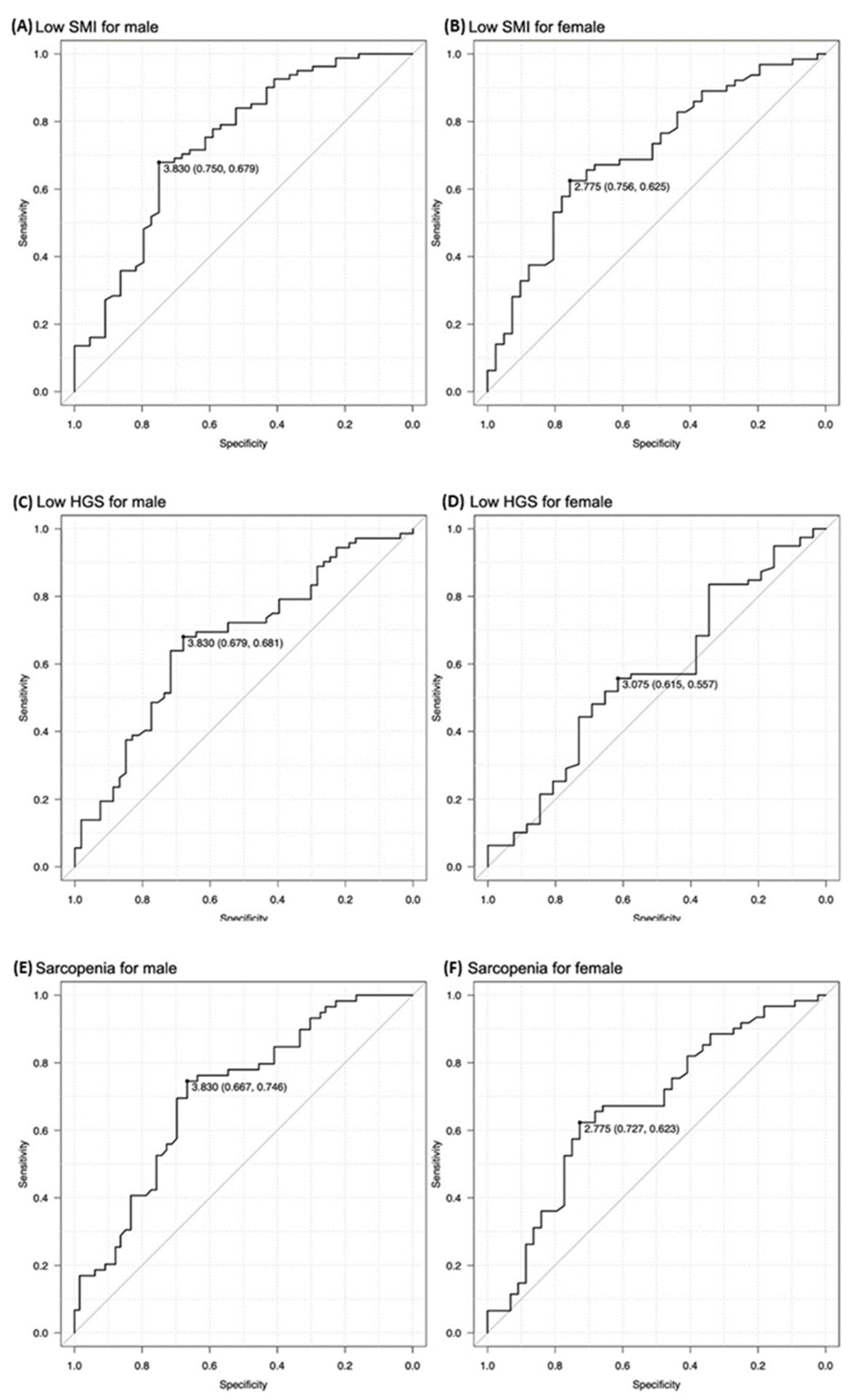
| Sensitivity | Specificity | AUC | PPV | NPV | |
|---|---|---|---|---|---|
| Low SMI | |||||
| -Men | 0.774 | 0.583 | 0.735 | 0.577 | 0.778 |
| -Women | 0.700 | 0.517 | 0.704 | 0.547 | 0.674 |
| Sarcopenia | |||||
| -Men | 0.642 | 0.750 | 0.726 | 0.654 | 0.740 |
| -Women | 0.660 | 0.567 | 0.681 | 0.559 | 0.667 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagano, A.; Shimizu, A.; Maeda, K.; Ueshima, J.; Inoue, T.; Murotani, K.; Ishida, Y.; Mori, N. Predictive Value of Temporal Muscle Thickness for Sarcopenia after Acute Stroke in Older Patients. Nutrients 2022, 14, 5048. https://doi.org/10.3390/nu14235048
Nagano A, Shimizu A, Maeda K, Ueshima J, Inoue T, Murotani K, Ishida Y, Mori N. Predictive Value of Temporal Muscle Thickness for Sarcopenia after Acute Stroke in Older Patients. Nutrients. 2022; 14(23):5048. https://doi.org/10.3390/nu14235048
Chicago/Turabian StyleNagano, Ayano, Akio Shimizu, Keisuke Maeda, Junko Ueshima, Tatsuro Inoue, Kenta Murotani, Yuria Ishida, and Naoharu Mori. 2022. "Predictive Value of Temporal Muscle Thickness for Sarcopenia after Acute Stroke in Older Patients" Nutrients 14, no. 23: 5048. https://doi.org/10.3390/nu14235048
APA StyleNagano, A., Shimizu, A., Maeda, K., Ueshima, J., Inoue, T., Murotani, K., Ishida, Y., & Mori, N. (2022). Predictive Value of Temporal Muscle Thickness for Sarcopenia after Acute Stroke in Older Patients. Nutrients, 14(23), 5048. https://doi.org/10.3390/nu14235048