The Multidimension of Malnutrition among School Children in a Rural Area, South Africa: A Mixed Methods Approach



Abstract
1. Introduction
2. Methods and Materials
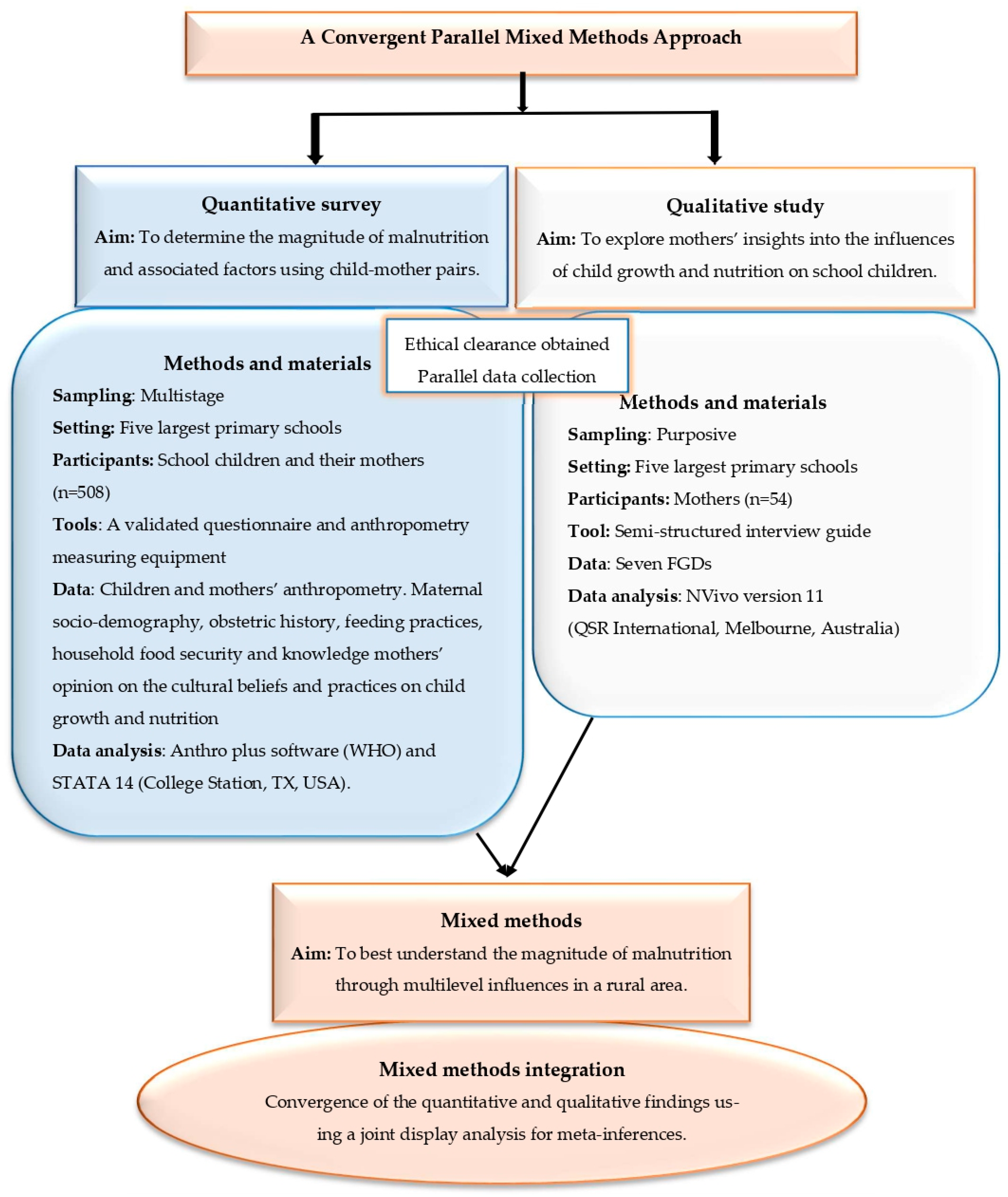
2.1. Study Design and Population
2.2. Sampling, Data Collection and Analysis
2.2.1. Quantitative Survey
2.2.2. Qualitative Study
3. Results
3.1. Quantitative Results
3.2. Qualitative Findings
3.3. Mixed Methods Integration
4. Discussion
5. Strengths and Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bronfenbrenner, U. Ecology of the family as a context for human development: Research perspectives. Dev. Psychol. 1986, 22, 723–742. [Google Scholar] [CrossRef]
- United Nations International Children’s Emergency Fund (UNICEF). Conceptual frameworks. In UNICEF M&E Training Resources; Oxford University Press: New York, NY, USA, 1998. [Google Scholar]
- Tanner, J.M.; Tanner, J.M. F Foetus into Man: Physical Growth from Conception to Maturity; Harvard University Press: Cambridge, MA, USA, 1990. [Google Scholar]
- Martorell, R.; Schroeder, D.G.; Rivera, J.A.; Kaplowitz, H.J. Patterns of linear growth in rural Guatemalan adolescents and children. J. Nutr. 1995, 125 (Suppl. 4), 1060S–1067S. [Google Scholar] [PubMed]
- Partnership for Child Development. The anthropometric status of schoolchildren in five countries in the partnership for child development. Proc. Nutr. Soc. 1998, 57, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Stoltzfus, R.J.; Albonico, M.; Tielsch, J.M.; Chwaya, H.M.; Savioli, L. Linear growth retardation in Zanzibari school children. J. Nutr. 1997, 127, 1099–1105. [Google Scholar] [CrossRef]
- Mosley, W.H.; Chen, L.C. An analythical framework for the study of child survival in developing countries. Bull. World Health Organ. 2003, 81, 140–145. [Google Scholar] [PubMed]
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.; Webb, P.; Lartey, A.; Black, R.E.; Lancet Nutrition Interventions Review Group, the Maternal and Child Nutrition Study Group. Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? Lancet 2013, 382, 452–477. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Adair, L.; Fall, C.; Hallal, P.C.; Martorell, R.; Richter, L.; Sachdev, H.S.; Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: Consequences for adult health and human capital. Lancet 2008, 371, 340–357. [Google Scholar] [CrossRef]
- Martins, V.J.; Toledo Florêncio, T.M.; Grillo, L.P.; Franco, M.D.C.P.; Martins, P.A.; Clemente, A.P.G.; Santos, C.D.; Vieira, M.D.F.A.; Sawaya, A.L. Long-lasting effects of undernutrition. Int. J. Environ. Res. Public Health 2011, 8, 1817–1846. [Google Scholar] [CrossRef]
- Kopelman, P.G. Obesity as a medical problem. Nature 2000, 404, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Malnutrition As a Multifactorial Health Problem Report Example Topics and Well Written Essays—1000 Words. Available online: https://studentshareorg/medical-science/2064392-malnutrition-as-a-multifactorial-health-problem (accessed on 17 October 2022).
- Akseer, N.; Vaivada, T.; Rothschild, O.; Ho, K.; Bhutta, Z.A. Understanding multifactorial drivers of child stunting reduction in Exemplar countries: A mixed-methods approach. Am. J. Clin. Nutr. 2020, 112 (Suppl. 2), 792s–805s. [Google Scholar] [CrossRef]
- Guetterman, T.; Fetters, M.D.; Creswell, J.W. Integrating quantitative and qualitative results in health science mixed methods research through joint displays. Ann. Fam. Med. 2015, 13, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Young, H.; Marshak, A. Persistent Global Acute Malnutrition; Feinstein International Center, Tufts University: Somerville, MA, USA, 2018; Available online: http://fictuftsedu/publication-item/persistent-globalacutemalnutrition-discussion-paper (accessed on 20 October 2022).
- Greene, J.C.; Caracelli, V.J.; Graham, W.F. Toward a Conceptual Framework for Mixed-Method Evaluation Designs. Educ. Eval. Policy Anal. 1989, 11, 255–274. [Google Scholar] [CrossRef]
- Almeida, F.; Faria, D.; Queirós, A. Strengths and Limitations of Qualitative and Quantitative Research Methods. Eur. J. Educ. Stud. 2017, 3, 369–387. [Google Scholar]
- Onwuegbuzie, A.; Johnson, R. The Validity Issues in Mixed Research. Res. Sch. 2006, 13, 48–63. [Google Scholar]
- Hattangadi, V. Mixed Method Research is Most Suitable. 2018. Available online: https://drvidyahattangadicom/mixed-method-research-is-most-suitable/ (accessed on 10 October 2022).
- Teddlie, C.; Tashakkori, A. A general typology of research designs featuring mixed methods. Res. Sch. 2006, 13, 12–28. [Google Scholar]
- Asgary, R.; Liu, M.; Naderi, R.; Grigoryan, Z.; Malachovsky, M. Malnutrition prevalence and nutrition barriers in children under 5 years: A mixed methods study in Madagascar. Int. Health 2015, 7, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.; Henretty, N.; Chary, A.; Webb, M.F.; Wehr, H.; Moore, J.; Baird, C.; Díaz, A.K.; Rohloff, P. Mixed-methods study identifies key strategies for improving infant and young child feeding practices in a highly stunted rural indigenous population in G uatemala. Matern. Child Nutr. 2016, 12, 262–277. [Google Scholar] [CrossRef] [PubMed]
- Moore, L.; O’Mahony, S.; Shevlin, M.; Hyland, P.; Barthorp, H.; Vallières, F. Towards identifying malnutrition among infants under 6 months: A mixed-methods study of South-Sudanese refugees in Ethiopia. Public Health Nutr. 2020, 24, 1265–1274. [Google Scholar] [CrossRef]
- Dukhi, N.; Sartorius, B.; Taylor, M. A behavioural change intervention study for the prevention of childhood obesity in South Africa: Protocol for a randomized controlled trial. BMC Public Health 2020, 20, 179. [Google Scholar] [CrossRef] [PubMed]
- Nepfumbada, G.; Dzinamarira, T.; Mashamba-Thompson, T.P. Development of an acceptable indigenous food diet for Pedi children under five years in early childhood development centers in rural Limpopo, South Africa. Arch. Public Health 2021, 79, 217. [Google Scholar] [CrossRef] [PubMed]
- Schneider, H.; van der Merwe, M.; Marutla, B.; Cupido, J.; Kauchali, S. The whole is more than the sum of the parts: Establishing an enabling health system environment for reducing acute child malnutrition in a rural South African district. Health Policy Plan. 2019, 34, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, S.; van den Bold, M. Stories of Change in nutrition: An overview. Glob. Food Secur. 2017, 13, 1–11. [Google Scholar] [CrossRef]
- Headey, D.; Hoddinott, J.; Park, S. Accounting for nutritional changes in six success stories: A regression-decomposition approach. Glob. Food Secur. 2017, 13, 12–20. [Google Scholar] [CrossRef]
- Modjadji, P.; Mashishi, J. Persistent Malnutrition and Associated Factors among Children under Five Years Attending Primary Health Care Facilities in Limpopo Province, South Africa. Int. J. Environ. Res. Public Health 2020, 17, 7580. [Google Scholar] [CrossRef]
- Modjadji, P.; Molokwane, D.; Ukegbu, P.O. Dietary Diversity and Nutritional Status of Preschool Children in North West Province, South Africa: A Cross Sectional Study. Children 2020, 7, 174. [Google Scholar] [CrossRef] [PubMed]
- Modjadji, P.; Pitso, M. Maternal Tobacco and Alcohol Use in Relation to Child Malnutrition in Gauteng, South Africa: A Retrospective Analysis. Children 2021, 8, 133. [Google Scholar] [CrossRef] [PubMed]
- Modjadji, P.; Masilela, L.N.; Cele, L.; Mathibe, M.; Mphekgwana, P.M. Evidence of Concurrent Stunting and Obesity among Children under 2 Years from Socio-Economically Disadvantaged Backgrounds in the Era of the Integrated Nutrition Programme in South Africa. Int. J. Environ. Res. Public Health 2022, 19, 12501. [Google Scholar] [CrossRef] [PubMed]
- Modjadji, P.; Madiba, S. The double burden of malnutrition in a rural health and demographic surveillance system site in South Africa: A study of primary schoolchildren and their mothers. BMC Public Health 2019, 19, 1087. [Google Scholar] [CrossRef] [PubMed]
- Modjadji, P. Socio-demographic Determinants of Overweight and Obesity Among Mothers ofPrimary School Children Living in a Rural Health and DemographicSurveillance System Site, South Africa. Open J. Public Health 2020, 13, 518–528. [Google Scholar] [CrossRef]
- Kimani-Murage, E.W.; Muthuri, S.K.; Oti, S.O.; Mutua, M.K.; van de Vijver, S.; Kyobutungi, C. Evidence of a double burden of malnutrition in urban poor settings in Nairobi, Kenya. PLoS ONE 2015, 10, e0129943. [Google Scholar] [CrossRef]
- Popkin, B.M. The nutrition transition in the developing world. Dev. Policy Rev. 2003, 21, 581–597. [Google Scholar] [CrossRef]
- Modjadji, P. Growth Patterns and Socio-Cultural Beliefs And Prcatices in Dikgale, Limpopo Province: A Mixed Method Study of Primary School Children and Their Mothers. Doctoral Thesis, Sefako Makgatho Health Sciences University, Ga-Rankuwa, South Africa, 2019. [Google Scholar]
- Modjadji, P.; Madiba, S. Childhood Undernutrition and Its Predictors in a Rural Health and Demographic Surveillance System Site in South Africa. Int. J. Environ. Res. Public Health 2019, 16, 3021. [Google Scholar] [CrossRef] [PubMed]
- Modjadji, P. Engaging Mothers on the Growth of School-Age Children in a Rural South African Health and Demographic Site: A Qualitative Insight. Healthcare 2021, 9, 225. [Google Scholar] [CrossRef]
- Alberts, M.; Dikotope, S.A.; Choma, S.R.; Masemola, M.L.; Modjadji, S.E.; Mashinya, F.; Burger, S.; Cook, I.; Brits, S.J.; Byass, P. Health & demographic surveillance system profile: The Dikgale health and demographic surveillance system. Int. J. Epidemiol. 2015, 44, 1565–1571. [Google Scholar] [PubMed]
- WHO. Obesity: Preventing and Managing The Global Epidemic; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- WHO. WHO AnthroPlus for Personal Computers Manual: Software for Assessing Growth of the World’s Children and Adolescents; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Maimela, E.; Alberts, M.; Modjadji, S.E.; Choma, S.S.; Dikotope, S.A.; Ntuli, T.S.; Van Geertruyden, J.P. The prevalence and determinants of chronic non-communicable disease risk factors amongst adults in the Dikgale health demographic and surveillance system (HDSS) site, Limpopo Province of South Africa. PLoS ONE 2016, 11, e0147926. [Google Scholar] [CrossRef] [PubMed]
- Modjadji, S.E.P. Nutritional Factors Involved in Development of Neural Tube Defects in Offspring of Women Residing in A High Risk Area: Doctoral Thesis, University of Limpopo (Turfloop campus); University of Limpopo: Polokwane, South Africa, 2009. [Google Scholar]
- Steyn, K.; Jooste, P.L.; Bourne, L.T.; Fourie, J.; Badenhorst, C.J.; Bourne, D.E.; Langenhoven, M.L.; Lombard, C.J.; Truter, H.; Ketzenellenbogen, J.; et al. Risk factors for coronary heart disease in the black population of the Cape Peninsula. The BRISK study. South Afr. Med. J. Suid-Afrik. Tydskr. Vir Geneeskd. 1991, 79, 480–485. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Shenton, A. Strategies for Ensuring Trustworthiness in Qualitative Research Projects. Educ. Inf. 2004, 22, 63–75. [Google Scholar] [CrossRef]
- Tashakkori, A.; Teddlie, C. Handbook of Mixed Methods in Social and Behavioural Research; SAGE: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Razali, F.M.; Aziz, N.A.A.; Rasli, R.M.; Zulkefly, N.F.; Salim, S.A. Using Convergent Parallel Design Mixed Method to Assess the Usage of Multi-Touch Hand Gestures Towards Fine Motor Skills Among Pre-School Children. Int. J. Acad. Res. Bus. Soc. Sci. 2019, 9, 153–166. [Google Scholar] [CrossRef]
- Chakona, G. Social circumstances and cultural beliefs influence maternal nutrition, breastfeeding and child feeding practices in South Africa. Nutr. J. 2020, 19, 47. [Google Scholar] [CrossRef]
- Galgamuwa, L.S.; Iddawela, D.; Dharmaratne, S.D.; Galgamuwa, G. Nutritional status and correlated socio-economic factors among preschool and school children in plantation communities, Sri Lanka. BMC Public Health 2017, 17, 377. [Google Scholar] [CrossRef] [PubMed]
- Manyike, P.C.; Chinawa, J.M.; Ubesie, A.; Obu, H.A.; Odetunde, O.I.; Chinawa, A.T. Prevalence of malnutrition among pre-school children in, South-east Nigeria. Italian journal of pediatrics 2014, 40, 75. [Google Scholar] [CrossRef] [PubMed]
- WHO. Malnutrition. 2021. Available online: https://wwwwhoint/news-room/fact-sheets/detail/malnutrition#:~:text=It%20is%20the%20result%20of%20chronic%20or%20recurrent,back%20from%20reaching%20their%20physical%20and%20cognitive%20potential (accessed on 22 October 2022).
- National Department of Health (NDoH), SAMRC and ICF. South Africa Demographic and Health Survey 2016; National Department of Health (NDoH), SAMRC and ICF: Pretoria, South Africa; Rockville, MD, USA, 2019. [Google Scholar]
- Shisana, O.; Labadarios, D.; Rehle, T.; Simbayi, L.; Zuma, K.; Dhansay, A.; Reddy, P.; Parker, W.; Hoosain, E.; Naidoo, P.; et al. South African National Health and Nutrition Examination Survey (SANHNES-1); HSRC Press: Cape Town, South Africa, 2013. [Google Scholar]
- Certified Nutritiojn Specialist (CNS); Test preparation and study guide. How Socioeconomic Status Affects Nutrition. 2015. Available online: https://study.com/academy/lesson/how-socioeconomic-status-affects-nutrition.html (accessed on 17 October 2022).
- Dieffenbach, S.; Stein, A.D. Stunted child/overweight mother pairs represent a statistical artifact, not a distinct entity. J. Nutr. 2012, 142, 771–773. [Google Scholar] [CrossRef] [PubMed]
- Mushaphi, L.; Mbhenyane, X.; Khoza, L.; Amey, A. Infant-feeding practices of mothers and the nutritional status of infants in the Vhembe District of Limpopo Province. South Afr. J. Clin. Nutr. 2008, 21, 36–41. [Google Scholar] [CrossRef]
- Goon, D.T.; Ajayi, A.I.; Adeniyi, O.V. Sociodemographic and lifestyle correlates of exclusive breastfeeding practices among mothers on antiretroviral therapy in the Eastern Cape, South Africa. Int. Breastfeed. J. 2021, 16, 18. [Google Scholar] [CrossRef]
- Labadarios, D.; Mchiza, Z.J.R.; Steyn, N.P.; Gericke, G.; Maunder, E.M.W.; Davids, Y.D.; Parker, W.A. Food security in South Africa: A review of national surveys. Bull. World Health Organ. 2011, 89, 891–899. [Google Scholar] [CrossRef]
- Alaimo, K.; Olson, C.M.; Frongillo, E.A., Jr. Food insufficiency and American school-aged children’s cognitive, academic, and psychosocial development. Pediatrics 2001, 108, 44–53. [Google Scholar] [CrossRef]
- Kaiser, L.L.; Melgar-Quiñonez, H.R.; Lamp, C.L.; Johns, M.C.; Sutherlin, J.M.; Harwood, J.O. Food security and nutritional outcomes of preschool-age Mexican-American children. J. Am. Diet. Assoc. 2002, 102, 924–929. [Google Scholar] [CrossRef]
- Appoh, L.Y.; Krekling, S. Maternal nutritional knowledge and child nutritional status in the Volta region of Ghana. Matern. Child Nutr. 2005, 1, 100–110. [Google Scholar] [CrossRef]
- Fadare, O.; Amare, M.; Mavrotas, G.; Akerele, D.; Ogunniyi, A. Mother’s nutrition-related knowledge and child nutrition outcomes: Empirical evidence from Nigeria. PLoS ONE 2019, 14, e0212775. [Google Scholar]
- Molina Mdel, C.; de Faria, C.P.; Montero, P.; Cade, N.V. Correspondence between children’s nutritional status and mothers’ perceptions: A population-based study. Cad. Saude Publica 2009, 25, 2285–2290. [Google Scholar] [CrossRef] [PubMed]
- Warschburger, P.; Kröller, K. Maternal perception of weight status and health risks associated with obesity in children. Pediatrics 2009, 124, e60–e68. [Google Scholar] [CrossRef]
- De Onis, M.; Branca, F. Childhood stunting: A global perspective. Matern. Child Nutr. 2016, 12, 12–26. [Google Scholar] [CrossRef]
- Goudet, S.M.; Faiz, S.; Bogin, B.A.; Griffiths, P.L. Pregnant Women’s and Community Health Workers’ Perceptions of Root Causes of Malnutrition among Infants and Young Children in the Slums of Dhaka, Bangladesh; American Public Health Association: Washington, DC, USA, 2011. [Google Scholar]
- Gilbert, N.L.; Casapía, M.; Joseph, S.A.; Ryan, J.A.; Gyorkos, T.W. Inadequate prenatal care and the risk of stillbirth in the Peruvian Amazon. Int. J. Gynecol. Obstet. 2010, 109, 155–156. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.M.; Coolman, M.; Steegers, E.A.; Jaddoe, V.W.; Moll, H.A.; Hofman, A.; Mackenbach, J.P.; Raat, H. Low socioeconomic status is a risk factor for preeclampsia: The Generation R Study. J. Hypertens. 2008, 26, 1200–1208. [Google Scholar] [CrossRef]
- Tette, E.M.; Sifah, E.K.; Nartey, E.T. Factors affecting malnutrition in children and the uptake of interventions to prevent the condition. BMC Pediatr. 2015, 15, 189. [Google Scholar] [CrossRef]
- Amsterdam, C. School Infrastructure in South Africa: Views and experiences of educators and learners. Canada International Conference on Education. At. Toronto, Canada. May 2010; pp.1–5. Available online: https://www.researchgate.net/publication/259290274 (accessed on 15 October 2022).
- Machengete, T. The fight for decent school infrastructure is far from over. 2021. Available online: http://wwwleadershiponlinecoza/2021/11/18/schools-infrastructure/#:~:text=The%20prevalence%20of%20schools%20with%20inadequate%20infrastructure%20is,in%20South%20Africa%2C%20rooted%20in%20colonialism%20and%20apartheid. (accessed on 15 October 2022).
- Calfas, K.J.; Sallis, J.F.; Nader, P.R. The development of scales to measure knowledge and preference for diet and physical activity behavior in 4-to 8-year-old children. J. Dev. Behav. Pediatr. 1991, 12, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A. Taste preferences and food intake. Annu. Rev. Nutr. 1997, 17, 237. [Google Scholar] [CrossRef] [PubMed]
- Cullen, K.W.; Eagan, J.; Baranowski, T.; Owens, E. Effect of a la carte and snack bar foods at school on children’s lunchtime intake of fruits and vegetables. J. Am. Diet. Assoc. 2000, 100, 1482–1486. [Google Scholar] [CrossRef] [PubMed]
- Okeyo, A.P.; Seekoe, E.; de Villiers, A.; Faber, M.; Nel, J.H.; Steyn, N.P. The Food and Nutrition Environment at Secondary Schools in the Eastern Cape, South Africa as Reported by Learners. Int. J. Environ. Res. Public Health 2020, 17, 4038. [Google Scholar] [CrossRef]
- Karmacharya, C.; Cunningham, K.; Choufani, J.; Kadiyala, S. Grandmothers’ knowledge positively influences maternal knowledge and infant and young child feeding practices. Public Health Nutr. 2017, 20, 2114–2123. [Google Scholar] [CrossRef] [PubMed]
- Pemunta, N.V.; Fubah, M.A. Socio-cultural determinants of infant malnutrition in Cameroon. J. Biosoc. Sci. 2015, 47, 423–448. [Google Scholar] [CrossRef]
- Birch, L.L. Research in Review. Children’s Eating: The Development of Food-Acceptance Patterns. Young Child. 1995, 50, 71–78. [Google Scholar]


{kind=link}
| Constructs | Main Results |
|---|---|
| Children: stunting (22%), underweight (24%), thinness (25%); coexistence of stunting and underweight (43%), underweight and thinness (66%). Factors associated with undernutrition: child sex, learning grade, and age, and maternal age, BMI, and short stature, as well as household access to water and using a refrigerator to store food. |
| Mothers: mean age (37 ± 7 years), overweight (27%), obesity (42%), combined overweight/obesity (69%). Factors associated with overweight/obesity: age, marital status, living with a spouse as a household head, low household income/month, age of first pregnancy, and more than one pregnancy. | |
| Mothers: single (63%), unemployment (82%), low literacy (41%), household head (38%). Household: income/month between R1000–R5000 (51%), recipient of child social grant (87%), ≥5 household members (64%), ≥3 children in household (68%), water access (74%), poor sanitation (i.e., using pit toilets) (96%), and using a refrigerator to store food (65%). |
| Age of first pregnancy (>30 years) (30%), number of pregnancies (2–4) (68%), parity [1 (22%), 2–4 (69%), and 5+ (9%)], and pregnancy complications and outcomes (26%). |
| Child eats breakfast every-day (75%), takes lunch box to school every day (48%). Mother worried that child has insufficient food at school (53%) or home (56%), is responsible for purchasing food at home (77%), can buy food for everyday needs (45%), eats less food due to insufficient food (47%), and no food at home sometimes, due to insufficient funds (41%). |
| Mothers believed that: Child is growing according his/her age (82%) Child growth can be affected by number of children a mother has (31%), mother’s health conditions (51%) and sickness (66%), mother’s employment status (44%), number of household members (38%), household income (53%), mother’s feeding knowledge (63%) and practice (93%), feeding them same food (53%), and genetics/heredity (60%). |
| Societal cultural beliefs and practices influence child growth (37%), mother’s cultural beliefs and practices affect child growth (33%), cultural beliefs influence the way children are fed (24%), there are cultural beliefs that prescribe which food is good for child’s growth (65%), there are cultural belief that prescribe which food is not good for child’s growth (37%), religion influences what to eat and not eat during pregnancy (52%). Most mothers (63%) did not know in which way do cultural beliefs and practices influence child growth. |
| Themes | Main Findings |
|---|---|
| 1. Perception about child growth | Mothers seemed to believe that their children are growing well, but differently. Factors that they considered to affect the growth of their children included socioeconomic status and poverty, genetics, and parents/family physical stature (i.e., heredity from the family), food consumption, maternal feeding practices, and household environment. |
| 2. Food unavailability | Some mothers expressed substantial concerns over food not always being available or enough in the household, with the understanding that food is important for child growth. |
| 3. Food affordability | Mothers narrated in a hypothetical manner that having enough food in their households would entail having the basic foods such as mealie meal flour, sugar, and tea, in addition to fruits and vegetables which they have only when they can afford to it. |
| 4. Feeding beliefs and practices | Mothers indicated the importance of feeding on child growth. Feeding beliefs and practices included early and childhood feeding practices, provision of lunchboxes for school, as well as the types of foods. |
| 5. Decision to purchase food | Most mothers described their buying practices in terms of what informs the food they purchased, in addition to them taking the decision, based on their objective. |
| 6. Perceptions on school feeding programme | Most mothers perceived the food at school to be better than the food at home; they described a variety of foods, such as samp, beans, pap, and milk, that were available at schools compared to their households. Some mothers made suggestions as to how the feeding scheme at schools could be improved to meet the needs of the children. |
| 7. Child food preference | Mothers reported that child eating behaviours such as food preference influence child growth. Mothers described that, children like and dislike certain foods, both at home and at school. |
| 8. Food knowledge | Mothers have limited knowledge on what constitutes healthy food. They were however able to identify nutritious foods that they served their families, such as traditional foods which they believed were good for their children and described healthy foods for child growth. |
| 9. Beliefs and practices during pregnancy | Mothers shared beliefs or practices adopted during pregnancy as expected by their parents or the community; most practices were related to what to eat and not to eat during pregnancy. |
| 10. Societal cultural beliefs and practices | Most mothers did not report any cultural practices that influenced how they raised their children, except for very few ambiguous insinuations. |
| Qualitative Themes | Quantitative Constructs | Comment (Meta-Inferences) |
|---|---|---|
| Anthropometry of children. Knowledge on child growth and nutrition. | Discordant—mothers believed that their children were growing well, yet undernutrition was prevalent. Congruent—the perceptions of mothers on child growth were comparable to their lack of knowledge on child growth and nutrition. |
| Socio demography. Anthropometry of children. Household food security. | Congruent—food unavailability agreed with the presence of childhood undernutrition and poor socio-demography. Discordant—food unavailability articulated during interviews was not supported by the household food insecurity observed in quantitative analysis. |
| Anthropometry of children. Socio-demography. Household food security. | Congruent—childhood undernutrition was affirmed by food affordability issues and agrees with poor socio-demography. Discordant—the household food insecurity discussed in the interviews was contrary to quantitative analysis. |
| Anthropometry of children. Socio-demography. Knowledge on child growth and nutrition. Cultural influence. Household food security. | Congruent—there were agreements on childhood undernutrition with feeding belief and practices, as well as socio demography, knowledge on child growth and nutrition, and to some extent, with cultural influence. Discordant—feeding beliefs and practices reported during interviews were not supported by household food security reported in quantitative analysis. |
| Anthropometry of children. Socio-demography. Household food security. | Congruent—childhood undernutrition was confirmed by challenges on the decision to purchase foods due to poverty articulated in the interviews and agrees with poor socio-demography. Discordant—decision to purchase foods was not supported by the household food security in the quantitative analysis. |
| Anthropometry of children. Knowledge on child growth and nutrition. | Discordant—childhood undernutrition did not agree with mothers’ perceptions on school feeding regarding food to be enough at the schools, and knowledge of mothers on child growth and nutrition. |
| Anthropometry of children | Congruent—child food preference, mainly at school, where children were selective of foods, they eat due to allergies they experience, suffer from diarrhoea and vomiting, which was confirmed by childhood undernutrition. |
| Knowledge on child growth and nutrition. Anthropometry of children | Congruent—food knowledge was confirmed by mothers’ lack of knowledge on child growth and nutrition and agreed with childhood undernutrition. |
| Obstetric history. Cultural influence | Congruent—beliefs and practices during pregnancy were confirmed by their obstetric complications and, and to some extent, the cultural influence. |
| Cultural influence | Congruent—the ambiguity of the societal cultural beliefs and practices narrated during interviews were substantiated to be unclear in qualitative analysis. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Modjadji, P.; Madiba, S. The Multidimension of Malnutrition among School Children in a Rural Area, South Africa: A Mixed Methods Approach. Nutrients 2022, 14, 5015. https://doi.org/10.3390/nu14235015
Modjadji P, Madiba S. The Multidimension of Malnutrition among School Children in a Rural Area, South Africa: A Mixed Methods Approach. Nutrients. 2022; 14(23):5015. https://doi.org/10.3390/nu14235015
Chicago/Turabian StyleModjadji, Perpetua, and Sphiwe Madiba. 2022. "The Multidimension of Malnutrition among School Children in a Rural Area, South Africa: A Mixed Methods Approach" Nutrients 14, no. 23: 5015. https://doi.org/10.3390/nu14235015
APA StyleModjadji, P., & Madiba, S. (2022). The Multidimension of Malnutrition among School Children in a Rural Area, South Africa: A Mixed Methods Approach. Nutrients, 14(23), 5015. https://doi.org/10.3390/nu14235015