
The Effect of Food Vouchers and an Educational Intervention on Promoting Healthy Eating in Vulnerable Families: A Pilot Study

 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
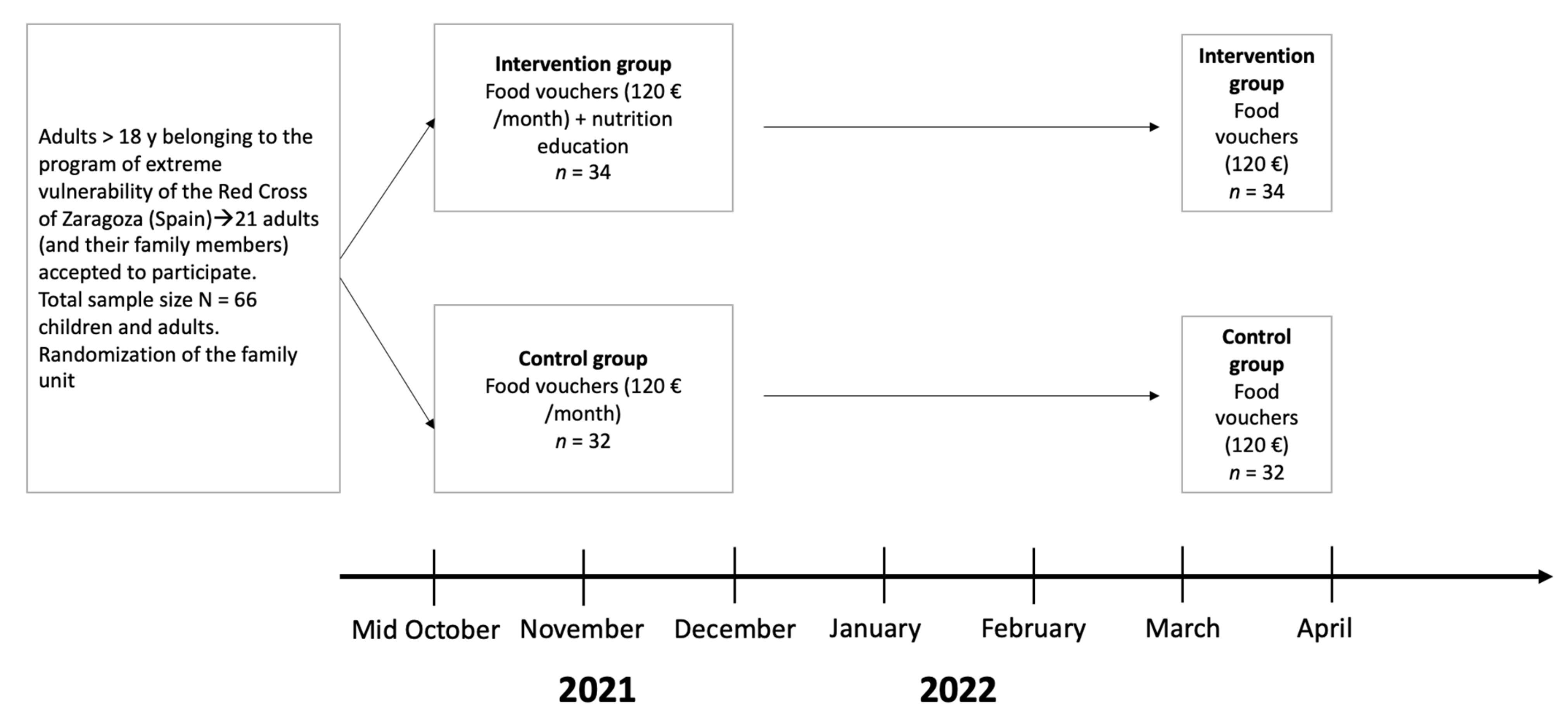
2.1. Study Design
2.2. Study Population
2.3. Intervention (Independent Variable)
2.4. Outcome Measures
2.4.1. Main Outcome: Adherence to the Mediterranean Diet
2.4.2. Dietary Assessment
2.4.3. Secondary Outcomes
Anthropometric Measures and Body Composition
Socio-Demographic Variables
Blood Pressure
Blood Analyses
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Crimarco, A.; Landry, M.J.; Gardner, C.D. Ultra-processed Foods, Weight Gain, and Co-morbidity Risk. Curr. Obes. Rep. 2021, 11, 80–92. [Google Scholar] [CrossRef] [PubMed]
- Backholer, K.; Gupta, A.; Zorbas, C.; Bennett, R.; Huse, O.; Chung, A.; Isaacs, A.; Golds, G.; Kelly, B.; Peeters, A. Differential exposure to, and potential impact of, unhealthy advertising to children by socio-economic and ethnic groups: A systematic review of the evidence. Obes. Rev. 2021, 22, e13144. [Google Scholar] [CrossRef] [PubMed]
- Chung, A.; Zorbas, C.; Peeters, A.; Backholer, K.; Browne, J. A Critical Analysis of Representations of Inequalities in Childhood Obesity in Australian Health Policy Documents. Int. J. Health Policy Manag. 2021, 11, 1767–1779. [Google Scholar] [CrossRef] [PubMed]
- Zorbas, C.; Grigsby-Duffy, L.; Backholer, K. Getting the Price Right: How Nutrition and Obesity Prevention Strategies Address Food and Beverage Pricing Within High-Income Countries. Curr. Nutr. Rep. 2020, 9, 42–53. [Google Scholar] [CrossRef]
- FAO; IFAD; UNICEF; WFP; WHO. El Estado de la Seguridad Alimentaria y la Nutrición en el Mundo 2022. Fao.org. Available online: https://www.fao.org/publications/sofi/2022/es (accessed on 21 June 2022).
- Clark, P.; Mendoza-Gutiérrez, C.F.; Montiel-Ojeda, D.; Denova-Gutiérrez, E.; López-González, D.; Moreno-Altamirano, L.; Reyes, A. A Healthy Diet Is Not More Expensive than Less Healthy Options: Cost-Analysis of Different Dietary Patterns in Mexican Children and Adolescents. Nutrients 2021, 13, 3871. [Google Scholar] [CrossRef]
- Love, P.; Whelan, J.; Bell, C.; Grainger, F.; Russell, C.; Lewis, M.; Lee, A. Healthy Diets in Rural Victoria—Cheaper than Unhealthy Alternatives, Yet Unaffordable. Int. J. Environ. Res. Public Health 2018, 15, 2469. [Google Scholar] [CrossRef]
- Zorbas, C.; Brooks, R.; Bennett, R.; Lee, A.; Marshall, J.; Naughton, S.; Lewis, M.; Peeters, A.; Backholer, K. Costing recommended (healthy) and current (unhealthy) diets in urban and inner regional areas of Australia using remote price collection methods. Public Health Nutr. 2021, 25, 528–537. [Google Scholar] [CrossRef]
- Pereira, M.; Oliveira, A.M. Poverty and food insecurity may increase as the threat of COVID-19 spreads. Public Health Nutr. 2020, 23, 3236–3240. [Google Scholar] [CrossRef]
- Zorbas, C.; Palermo, C.; Chung, A.; Iguacel, I.; Peeters, A.; Bennett, R.; Backholer, K. Factors perceived to influence healthy eating: A systematic review and meta-ethnographic synthesis of the literature. Nutr. Rev. 2018, 76, 861–874. [Google Scholar] [CrossRef]
- Riesenberg, D.; Backholer, K.; Zorbas, C.; Sacks, G.; Paix, A.; Marshall, J.; Blake, M.R.; Bennett, R.; Peeters, A.; Cameron, A.J. Price Promotions by Food Category and Product Healthiness in an Australian Supermarket Chain, 2017–2018. Am. J. Public Health 2019, 109, 1434–1439. [Google Scholar] [CrossRef]
- Watt, T.L.; Beckert, W.; Smith, R.D.; Cornelsen, L. Reducing consumption of unhealthy foods and beverages through banning price promotions: What is the evidence and will it work? Public Health Nutr. 2020, 23, 2228–2233. [Google Scholar] [CrossRef] [PubMed]
- Zorbas, C.; Eyles, H.; Orellana, L.; Peeters, A.; Ni Mhurchu, C.; Riesenberg, D.; Backholer, K. Do purchases of price promoted and generic branded foods and beverages vary according to food category and income level? Evidence from a consumer research panel. Appetite 2019, 144, 104481. [Google Scholar] [CrossRef]
- Iguacel, I.; Fernández-Alvira, J.M.; Bammann, K.; De Clercq, B.; Eiben, G.; Gwozdz, W.; Molnar, D.; Pala, V.; Papoutsou, S.; Russo, P.; et al. Associations between social vulnerabilities and dietary patterns in European children: The Identification and prevention of Dietary- and lifestyle-induced health EFfects In Children and infantS (IDEFICS) study. Br. J. Nutr. 2016, 116, 1288–1297. [Google Scholar] [CrossRef]
- Konttinen, H.; Sarlio-Lähteenkorva, S.; Silventoinen, K.; Männistö, S.; Haukkala, A. Socio-economic disparities in the consumption of vegetables, fruit and energy-dense foods: The role of motive priorities. Public Health Nutr. 2012, 16, 873–882. [Google Scholar] [CrossRef]
- McFadden, A.; Green, J.M.; Williams, V.; McLeish, J.; McCormick, F.; Fox-Rushby, J.; Renfrew, M.J. Can food vouchers improve nutrition and reduce health inequalities in low-income mothers and young children: A multi-method evaluation of the experiences of beneficiaries and practitioners of the Healthy Start programme in England. BMC Public Health 2014, 14, 148. [Google Scholar] [CrossRef] [PubMed]
- Bihan, H.; Méjean, C.; Castetbon, K.; Faure, H.; Ducros, V.; Sedeaud, A.; Galan, P.; Le Clésiau, H.; Péneau, S.; Hercberg, S. Impact of fruit and vegetable vouchers and dietary advice on fruit and vegetable intake in a low-income population. Eur. J. Clin. Nutr. 2011, 66, 369–375. [Google Scholar] [CrossRef]
- Ohly, H.; Crossland, N.; Dykes, F.; Lowe, N.; Hall-Moran, V. A realist review to explore how low-income pregnant women use food vouchers from the UK’s Healthy Start programme. BMJ Open 2017, 7, e013731. [Google Scholar] [CrossRef] [PubMed]
- Lucas, P.J.; Jessiman, T.; Cameron, A. Healthy Start: The Use of Welfare Food Vouchers by Low-Income Parents in England. Soc. Policy Soc. 2015, 14, 457–469. [Google Scholar] [CrossRef]
- Jenneson, V.L.; Pontin, F.; Greenwood, D.C.; Clarke, G.P.; Morris, M.A. A systematic review of supermarket automated electronic sales data for population dietary surveillance. Nutr. Rev. 2022, 80, 1711–1722. [Google Scholar] [CrossRef]
- Eurocities. Zaragoza. Eurocities. Available online: https://eurocities.eu/cities/zaragoza/ (accessed on 10 July 2022).
- Ayuntamiento de Zaragoza. Cifras de Zaragoza. Available online: https://www.zaragoza.es/cont/paginas/estadistica/pdf/Cifras-Zaragoza-2021.pdf (accessed on 10 July 2022).
- Personas en Extrema Vulnerabilidad—Cruz Roja. Cruzroja.es. Available online: https://www2.cruzroja.es/-/personas-en-extrema-vulnerabilidad (accessed on 8 July 2022).
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-Item Mediterranean Diet Assessment Tool and Obesity Indexes among High-Risk Subjects: The PREDIMED Trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed]
- CDC. Adult BMI Calculator. Centers for Disease Control and Prevention. 2022. Available online: https://www.cdc.gov/healthyweight/assessing/bmi/adult_BMI/english_bmi_calculator/bmi_calculator.html (accessed on 30 May 2022).
- CDC. About Child & Teen BMI. Centers for Disease Control and Prevention. 2022. Available online: https://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/about_childrens_bmi.html (accessed on 30 May 2022).
- Nagy, E.; Vicente-Rodriguez, G.; Manios, Y.; Béghin, L.; Iliescu, C.; Censi, L.; Dietrich, S.; Ortega, F.B.; De Vriendt, T.; Plada, M.; et al. Harmonization process and reliability assessment of anthropometric measurements in a multicenter study in adolescents. Int. J. Obes. 2008, 32 (Suppl. S5), S58–S65. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Adolescent Health. Available online: https://www.who.int/health-topics/adolescent-health (accessed on 11 June 2022).
- Pinket, A.-S.; Van Lippevelde, W.; De Bourdeaudhuij, I.; Deforche, B.; Cardon, G.; Androutsos, O.; Koletzko, B.; Moreno, L.A.; Socha, P.; Iotova, V.; et al. Effect and Process Evaluation of a Cluster Randomized Control Trial on Water Intake and Beverage Consumption in Preschoolers from Six European Countries: The ToyBox-Study. PLoS ONE 2016, 11, e0152928. [Google Scholar] [CrossRef] [PubMed]
- Berggreen-Clausen, A.; Hseing Pha, S.; Mölsted Alvesson, H.; Andersson, A.; Daivadanam, M. Food Environment Interactions after Migration: A Scoping Review on Low- and Middle-Income Country Immigrants in High-Income Countries. Public Health Nutr. 2022, 25, 136–158. [Google Scholar] [CrossRef] [PubMed]
- Kovalskys, I.; Cavagnari, B.M.; Zonis, L.N.; Favieri, A.L.; Guajardo, V.; Gerardi, A.; Fisberg, M. Poverty as a determinant of food quality in Argentina. Results of the Argentine Study of Nutrition and Health (EANS). Nutr. Hosp. 2020, 37, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Furey, S. Food promotions and the cost of a healthy diet. Proc. Nutr. Soc. 2021, 81, 126–133. [Google Scholar] [CrossRef]
- Latasa, P.; da Coasta Louzada, M.L.; Steele, E.M.; Monteiro, C.A. Added sugars and ultra-processed foods in Spanish households (1990–2010). Eur. J. Clin. Nutr. 2018, 72, 1404–1412. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Kim, H.B.; Park, S. The Roles of Nutrition Education and Food Vouchers in Improving Child Nutrition: Evidence from a Field Experiment in Ethiopia. J. Health Econ. 2021, 80, 102545. [Google Scholar] [CrossRef]
- Zagorsky, J.L.; Smith, P.K. Does the U.S. Food Stamp Program contribute to adult weight gain? Econ. Hum. Biol. 2009, 7, 246–258. [Google Scholar] [CrossRef] [PubMed]
- Chaparro, M.P.; Harrison, G.G.; Pebley, A.R.; Wang, M. The Relationship Between Obesity and Participation in the Supplemental Nutrition Assistance Program (SNAP): Is Mental Health a Mediator? J. Hunger. Environ. Nutr. 2014, 9, 512–522. [Google Scholar] [CrossRef]
- Andreyeva, T.; Tripp, A.S.; Schwartz, M.B. Dietary Quality of Americans by Supplemental Nutrition Assistance Program Participation Status. Am. J. Prev. Med. 2015, 49, 594–604. [Google Scholar] [CrossRef]
- White, J.S.; Vasconcelos, G.; Harding, M.; Carroll, M.M.; Gardner, C.D.; Basu, S.; Seligman, H.K. Heterogeneity in the Effects of Food Vouchers on Nutrition Among Low-Income Adults: A Quantile Regression Analysis. Am. J. Health Promot. 2020, 35, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Paolantonio, L.; Kim, S.Y.; Ramirez, J.; Roberts-Eversley, N.; Li, Y.; Melnic, I.; Wu, M.; Jutagir, D.R.; Smith, J.; Oladele, M.; et al. Food Purchasing Behavior of Food Insecure Cancer Patients Receiving Supplemental Food Vouchers. Support. Care Cancer 2019, 28, 3739–3746. [Google Scholar] [CrossRef]
- López-Sobaler, A.M.; Aparicio, A.; Salas-González, M.D.; Loria Kohen, V.; Bermejo López, L.M. Childhood obesity in Spain and associated factors. Nutr. Hosp. 2021, 38, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Rodrigo, C.; Hervás Bárbara, G.; Gianzo Citores, M.; Aranceta-Bartrina, J. Prevalence of obesity and associated cardiovascular risk factors in the Spanish population: The ENPE study. Rev. Esp. Cardiol. (Engl. Ed.) 2022, 75, 232–241. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Categorical Variables | N = 66 (%) | Group (%) | p-Value | |
|---|---|---|---|---|
| Control (n = 32) | Intervention (n = 34) | |||
| Sex | 0.121 | |||
| Male | 27 (40.9%) | 37.0 | 63.0 | |
| Female | 39 (59.1%) | 56.4 | 43.6 | |
| Age | 0.729 | |||
| Child | 10 (15.2%) | 40.0 | 60.0 | |
| Adolescent | 24 (36.4%) | 54.2 | 45.8 | |
| Adult | 32 (48.5%) | 46.9 | 53.1 | |
| BMI at baseline | 0.026 | |||
| Underweight | 5 (7.6%) | 40.0 | 60.0 | |
| Normal weight | 24 (36.4%) | 70.8 | 29.2 | |
| Overweight | 17 (25.8%) | 23.5 | 76.5 | |
| Obesity | 20 (30.3%) | 45.0 | 55.0 | |
| Weight objective achieved | 0.001 | |||
| Yes | 34 (48.5%) | 25.0 | 75.0 | |
| No | 32 (51.5%) | 70.6 | 29.4 | |
| Migrant origin | 0.072 | |||
| No | 12 (18.2%) | 25.0 | 75.0 | |
| Yes | 54 (81.8%) | 53.7 | 46.3 | |
| Educational status | 0.015 | |||
| Low | 55 (83.3%) | 41.8 | 58.2 | |
| Medium or high | 11 (16.7%) | 81.8 | 18.2 | |
| Employment status | 0.011 | |||
| Unemployed | 46 (69.7%) | 37.8 | 62.2 | |
| Employed | 20 (30.3%) | 71.4 | 28.6 | |
| Family structure | 0.018 | |||
| Traditional | 42 (63.6%) | 29.2 | 70.8 | |
| Non-traditional | 24 (36.4%) | 59.5 | 40.5 | |
| n = 34 | Pre-Intervention T0 (Mid-October 2021) | Post-Intervention T1 (End of December 2021) | Mean Differences | |||||
|---|---|---|---|---|---|---|---|---|
| Control = 17 | Intervention = 17 | Control = 17 | Intervention = 17 | Control Intervention | ||||
| Mean (SD) | Mean (SD) | p-Value | Mean (SD) | Mean (SD) | p-Value | MD (T1-T0) | MD (T1-T0) | |
| Age (years) | 11.64 (3.88) | 11.54 (4.28) | 0.934 | 11.90 (3.88) | 11.80 (4.28) | 0.934 | - | - |
| ADM | 9.82 (3.00) | 9.76 (3.36) | 0.957 | 11.58 (1.87) | 10.94 (1.51) | 0.277 | 1.76 | 1.18 |
| Weight (kg) | 44.20 (19.29) | 48.30 (24.97) | 0.596 | 45.48 (19.99) | 47.97 (24.17) | 0.327 | 1.28 | −0.33 |
| Height (m) | 147.73 (0.22) | 148.24 (0.22) | 0.948 | 147.95 (0.23) | 148.49 (0.23) | 0.953 | 0.22 | 0.25 |
| BMI (kg/m2) | 19.28 (4.74) | 20.65 (7.04) | 0.511 | 19.72 (6.66) | 20.50 (6.86) | 0.704 | 0.44 | −0.15 |
| BMI z-score | 0.00 (1.28) | 0.14 (1.68) | 0.781 | 0.12 (1.28) | 0.13 (1.60) | 0.975 | 0.12 | −0.01 |
| Fat (kg) | 10.97 (6.52) | 13.5 (10.30) | 0.433 | 12.61 (8.50) | 14.23 (12.15) | 0.655 | 1.64 | 0.73 |
| Fat Mass Index | 7.20 (3.76) | 8.75 (7.02) | 0.427 | 8.23 (4.93) | 9.20 (7.32) | 0.653 | 1.03 | 0.45 |
| Water (percentage) | 55.28 (4.80) | 54.28 (7.62) | 0.650 | 53.88 (5.78) | 53.51 (7.76) | 0.876 | −1.40 | −0.77 |
| Lean mass (kg) | 30.42 (14.43) | 32.91 (14.38) | 0.618 | 31.15 (13.14) | 31.96 (13.40) | 0.861 | 6.15 | 5.59 |
| Waist (cm) | 64.92 (10.42) | 67.80 (15.90) | 0.536 | 65.54 (10.53) | 67.32 (15.42) | 0.697 | 0.62 | −0.48 |
| Waist/height | 0.44 (0.05) | 0.45 (0.07) | 0.570 | 0.44 (0.05) | 0.45 (0.07) | 0.789 | 0 | 0 |
| Hip (in cm) | 81.54 (15.67) | 83.54 (20.97) | 0.755 | 82.57 (16.65) | 83.68 (20.31) | 0.863 | 1.03 | 0.14 |
| Uric acid (mg/dL) | 4.42 (0.99) | 4.25 (1.10) | 0.655 | 4.04 (1.08) | 4.14 (1.15) | 0.812 | −0.38 | −0.11 |
| Urea (mg/dL) | 26.46 (6.23) | 26.86 (5.99) | 0.856 | 27.40 (5.86) | 25.93 (4.87) | 0.455 | 0.94 | −0.93 |
| GOT (U/L at 37 °C) | 33.13 (7.16) | 35.68 (11.48) | 0.467 | 33.53 (10.95) | 35.68 (9.84) | 0.569 | 0.40 | 0 |
| GPT (U/L at 37 °C) | 17.66 (6.28) | 17.93 (5.57) | 0.900 | 18.73 (8.63) | 18.37 (6.11) | 0.894 | 1.07 | 0.44 |
| GGT (U/L at 37 °C) | 16.73 (3.41) | 17.75 (3.76) | 0.438 | 16.06 (1.70) | 16.75 (3.78) | 0.520 | −0.67 | −1.00 |
| TC (mg/dL) | 172.33 (28.78) | 150.81 (24.99) | 0.034 | 172.28 (26.61) | 149.59 (24.05) | 0.020 | −0.05 | −1.22 |
| TG (mg/dL) | 62.53 (24.21) | 74.12 (42.79) | 0.365 | 67.64 (26.88) | 70.93 (37.55) | 0.787 | 5.11 | −3.19 |
| HDL (mg/dL) | 54.40 (8.99) | 48.62 (10.41) | 0.110 | 58.28 (10.29) | 52.06 (11.45) | 0.131 | 3.88 | 3.44 |
| LDL (mg/dL) | 105.26 (26.28) | 87.37 (21.83) | 0.048 | 100.42 (18.78) | 83.37 (21.71) | 0.030 | −4.84 | −4 |
| Glucose (mg/dL) | 87.66 (8.38) | 83.43 (8.32) | 0.170 | 86.26 (7.33) | 84.25 (7.43) | 0.454 | −1.40 | 0.82 |
| HbA1c (%) | 5.27 (0.68) | 4.82 (0.27) | 0.021 | 5.36 (0.22) | 5.18 (0.29) | 0.071 | 0.09 | 0.36 |
| SBP (mmHg) | 115.14 (9.96) | 113.47 (12.78) | 0.673 | 108.67 (10.55) | 110.91 (12.92) | 0.585 | −6.47 | −2.56 |
| DBP (mmHg) | 68.58 (3.67) | 63.79 (9.33) | 0.057 | 68.76 (9.06) | 71.76 (9.59) | 0.356 | 0.18 | 7.97 |
| Heartrate (beats per minute) | 79.55 (14.45) | 81.85 (14.28) | 0.850 | 80.17 (12.64) | 76.91 (14.06) | 0.502 | −0.53 | 2.3 |
| n = 32 | Pre-Intervention (Mid-October 2021) | Post-Intervention (End of December 2021) | ||||
|---|---|---|---|---|---|---|
| Control = 15 | Intervention = 17 | Control = 15 | Intervention = 17 | |||
| Mean (SD) | Mean (SD) | p-Value | Mean (SD) | Mean (SD) | p-Value | |
| Age (years) | 42.60 (13.80) | 44.29 (13.53) | 0.350 | 42.84 (13.80) | 44,53 (13.53) | 0.708 |
| Adherence to Mediterranean Diet | 8.73 (2.37) | 6.47 (2.42) | 0.012 | 10.21 (2.11) | 10.35 (1.22) | 0.821 |
| Weight (kg) | 69.40 (14.75) | 87.02 (18.96) | 0.007 | 70.31 (15.32) | 85.44 (18.66) | 0.021 |
| Height (m) | 160.06 (0.08) | 169.69 (9.43) | 0.005 | 160.06 (0.08) | 169.69 (9.43) | 0.005 |
| BMI (kg/m2) | 27.20 (5.90) | 30.28 (6.31) | 0.166 | 27.56 (6.09) | 29.69 (6.05) | 0.704 |
| Fat (kg) | 22.92 (10.60) | 30.35 (13.11) | 0.070 | 23.93 (11.07) | 29.65 (12.62) | 0.195 |
| Fat Mass Index | 14.09 (6.54) | 18.01 (7.92) | 0.427 | 14.05 (7.81) | 17.57 (7.59) | 0.653 |
| Water (percentage) | 48.91 (7.40) | 46.21 (7.35) | 0.269 | 48.60 (7.09) | 46.81 (7.33) | 0.500 |
| Lean mass (kg) | 44.97 (7.52) | 53.51 (9.72) | 0.007 | 43.83 (7.57) | 52.98 (9.85) | 0.008 |
| Waist (cm) | 84.51 (13.98) | 94.90 (15.90) | 0.025 | 85.10 (14.95) | 93.50 (11.95)) | 0.093 |
| Waist/height | 0.52 (0.09) | 0.56 (0.07) | 0.249 | 0.49 (0.16) | 0.55 (0.06) | 0.238 |
| Hip (in cm) | 100.94 (11.62) | 111.47 (13.44) | 0.025 | 94.23 (28.39) | 109.45 (12.05) | 0.053 |
| Uric acid (mg/dL) | 4.52 (0.00) | 5.33 (1.08) | 0.024 | 4.19 (1.08) | 5.17 (1.15) | 0.031 |
| Urea (mg/dL) | 30.20 (10.40) | 36.78 (8.76) | 0.066 | 33.78 (14.68) | 33.43 (8.57) | 0.936 |
| GOT (U/L at 37 °C) | 31.26 (12.14) | 29.94 (11.36) | 0.752 | 32.21 (11.17) | 27.76 (5.79) | 0.164 |
| GPT (U/L at 37 °C) | 25.73 (16.60) | 26.52 (13.55) | 0.882 | 22.78 (12.42) | 21.70 (10.25) | 0.793 |
| GGT (U/L at 37 °C) | 25.73 (15.91) | 28.00 (10.54) | 0.635 | 23.92 (16.47) | 26.76 (12.50) | 0.590 |
| TC (mg/dL) | 190.53 (32.46) | 188.94 (35.96) | 0.897 | 191.92 (48.77) | 187.47 (28.51) | 0.753 |
| TG (mg/dL) | 103.40 (61.43) | 137.41 (74.41) | 0.172 | 130.50 (82.64) | 111.11 (53.89) | 0.438 |
| HDL (mg/dL) | 53.60 (15.00) | 48.17 (11.95) | 0.264 | 55.50 (18.83) | 47.78 (12.76) | 0.185 |
| LDL (mg/dL) | 114.73 (30.34) | 115.41 (27.27) | 0.947 | 113.85 (42.22) | 118.41 (21.94) | 0.702 |
| Glucose (mg/dL) | 96.06 (16.33) | 97.17 (15.77) | 0.846 | 97.23 (20.22) | 97.29 (15.88) | 0.992 |
| HbA1c (%) | 5.65 (1.00) | 5.27 (0.47) | 0.200 | 5.95 (0.86) | 5.58 (0.46) | 0.171 |
| SBP (mmHg) | 128.96 (24.94) | 138.41 (22.31) | 0.381 | 129.75 (21.68) | 138.70 (17.11) | 0.215 |
| DBP (mmHg) | 69.73 (8.63) | 78.73 (12.33) | 0.025 | 80.00 (11.65) | 86.58 (10.86) | 0.115 |
| Heartrate (beats per minute) | 72.90 (9.56) | 75.23 (8.14) | 0.850 | 71.71 (9.55) | 76.02 (9.46) | 0.502 |
| N = 66 | Children and Adolescents = 34 | Adults = 32 | ||||||
|---|---|---|---|---|---|---|---|---|
| MD (T1-T0) Control | MD (T1-T0) Intervention | MD Change (I-C) | p-Value | MD (T1-T0) Control | MD (T1-T0) Intervention | MD Change (I-C) | p-Value | |
| ADM | 1.76 | 1.18 | −0.58 | 0.499 | 1.50 | 3.88 | 2.38 | 0.016 |
| Weight (kg) | 1.28 | −0.33 | −1.61 | 0.002 | 0.91 | −1.58 | −2.49 | 0.017 |
| Height (m) | 0.22 | 0.25 | 0.03 | 0.341 | - | - | - | - |
| BMI (kg/m2) | 0.44 | −0.15 | −0.59 | 0.499 | 0.36 | −0.59 | −0.95 | 0.019 |
| BMI z-score | 0.12 | −0.01 | −0.13 | 0.066 | - | - | - | |
| Fat (kg) | 1.63 | 0.67 | −0.96 | 0.136 | 1.01 | −0.70 | −2.21 | 0.012 |
| Fat Mass Index | 1.03 | 0.45 | −0.58 | 0.128 | −0.04 | −0.44 | −0.4 | 0.601 |
| Water (percentage) | −1.40 | −0.77 | 0.63 | 0.268 | −0.31 | 0.60 | 0.91 | 0.152 |
| Lean mass (kg) | 0.73 | −0.95 | −1.68 | 0.184 | −1.14 | −0.53 | 0.61 | 0.334 |
| Waist (cm) | 0.62 | −0.48 | −1.10 | 0.075 | 0.59 | −1.40 | −1.99 | 0.108 |
| Waist/height | 0.01 | 0.01 | 0.00 | 0.091 | −0.03 | −0.01 | 0.02 | 0.249 |
| Hip (in cm) | 1.03 | 0.14 | −0.89 | 0.120 | −6.71 | −2.02 | 4.69 | 0.439 |
| Uric acid (mg/dL) | −0.38 | −0.11 | 0.27 | 0.135 | −0.32 | −0.16 | 0.12 | 0.507 |
| Urea (mg/dL) | 0.94 | −0.93 | −1.87 | 0.367 | 2.93 | −3.35 | −6.27 | 0.030 |
| GOT (U/L at 37 °C) | 0.40 | 0.00 | −0.40 | 0.905 | 0.21 | −2.18 | −2.39 | 0.360 |
| GPT (U/L at 37 °C) | 1.07 | 0.44 | −0.63 | 0.798 | −3.57 | −4.82 | −1.87 | 0.668 |
| GGT (U/L at 37 °C) | −0.67 | −1.00 | −0.33 | 0.805 | −1.81 | −1.24 | 0.55 | 0.847 |
| Cholesterol (mg/dL) | −0.05 | −1.31 | −1.26 | 0.864 | 1.39 | −1.47 | −2.86 | 0.914 |
| TG (mg/dL) | 5.11 | −3.19 | −8.30 | 0.321 | 27.10 | −26.30 | −53.40 | 0.023 |
| HDL (mg/dL) | 1.88 | 3.44 | −0.44 | 0.933 | 1.90 | −0.41 | −2.31 | 0.513 |
| LDL (mg/dL) | −4.84 | −4.00 | 0.84 | 0.576 | −0.88 | 3.00 | 3.88 | 0.446 |
| Glucose (mg/dL) | −1.4 | 0.82 | 2.22 | 0.460 | 1.17 | 0.12 | −1.05 | 0.749 |
| HbA1c (%) | 0.09 | 0.36 | 0.27 | 0.236 | 0.30 | 0.31 | 0.01 | 0.595 |
| SBP (mmHg) | −6.47 | −2.56 | 3.91 | 0.224 | 1.14 | 0.29 | −0.85 | 0.752 |
| DBP (mmHg) | 0.18 | 7.97 | 7.79 | 0.014 | 10.27 | 7.85 | −2.42 | 0.417 |
| Heartrate (beats per minute) | 0.62 | −4.94 | −5.56 | 0.077 | −1.19 | 0.79 | 1.98 | 0.717 |
| Control Group | Intervention Group | |||||
|---|---|---|---|---|---|---|
| First Month Intervention | Last Month Intervention | Post-Intervention | First Month Intervention | Last Month Intervention | Post-Intervention | |
| Cereals & cereal products | 2.90 | 1.48 | 1.06 | 2.99 | 2.67 | 0.50 |
| Pasta & rice | 2.50 | 2.80 | 3.87 | 4.04 | 5.34 | 2.85 |
| Ready-to-eat dishes | 6.45 | 8.07 | 5.11 | 2.81 | 2.81 | 1.12 |
| Dairy & dairy-free products | 9.02 | 5.77 | 7.75 | 7.02 | 5.49 | 6.07 |
| Egg & egg dishes | 2.66 | 3.62 | 2.82 | 2.72 | 4.50 | 2.85 |
| Legumes | 1.93 | 1.32 | 1.76 | 1.93 | 3.66 | 1.98 |
| Meat & meat products | 4.75 | 4.78 | 9.68 | 10.80 | 10.55 | 15.24 |
| Fish & fish dishes | 5.16 | 5.44 | 4.40 | 9.31 | 12.80 | 4.09 |
| Fruits and vegetables | 23.85 | 26.19 | 25.88 | 29.85 | 32.49 | 31.97 |
| Salty snacks | 2.10 | 3.13 | 1.76 | 0.35 | 0.00 | 1.86 |
| Nuts & seeds | 3.30 | 5.77 | 3.17 | 7.64 | 6.33 | 4.21 |
| Sugar, bakery products, cakes, and confectionery | 20.55 | 23.72 | 20.95 | 13.96 | 9.85 | 17.47 |
| Commercial sauces | 1.93 | 1.32 | 2.11 | 0.70 | 0.42 | 1.73 |
| Sweetened beverages | 8.94 | 5.77 | 8.80 | 2.90 | 1.41 | 7.06 |
| Unsaturated oils (olive oil) | 2.99 | 1.69 | 0.99 | 3.95 | 0.82 | 0.88 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miguel-Berges, M.L.; Jimeno-Martínez, A.; Larruy-García, A.; Moreno, L.A.; Rodríguez, G.; Iguacel, I. The Effect of Food Vouchers and an Educational Intervention on Promoting Healthy Eating in Vulnerable Families: A Pilot Study. Nutrients 2022, 14, 4980. https://doi.org/10.3390/nu14234980
Miguel-Berges ML, Jimeno-Martínez A, Larruy-García A, Moreno LA, Rodríguez G, Iguacel I. The Effect of Food Vouchers and an Educational Intervention on Promoting Healthy Eating in Vulnerable Families: A Pilot Study. Nutrients. 2022; 14(23):4980. https://doi.org/10.3390/nu14234980
Chicago/Turabian StyleMiguel-Berges, María L., Andrea Jimeno-Martínez, Alicia Larruy-García, Luis A. Moreno, Gerardo Rodríguez, and Isabel Iguacel. 2022. "The Effect of Food Vouchers and an Educational Intervention on Promoting Healthy Eating in Vulnerable Families: A Pilot Study" Nutrients 14, no. 23: 4980. https://doi.org/10.3390/nu14234980
APA StyleMiguel-Berges, M. L., Jimeno-Martínez, A., Larruy-García, A., Moreno, L. A., Rodríguez, G., & Iguacel, I. (2022). The Effect of Food Vouchers and an Educational Intervention on Promoting Healthy Eating in Vulnerable Families: A Pilot Study. Nutrients, 14(23), 4980. https://doi.org/10.3390/nu14234980