
Gut Microbiota Profile in Adults Undergoing Bariatric Surgery: A Systematic Review

 ,
, 

Abstract
1. Introduction
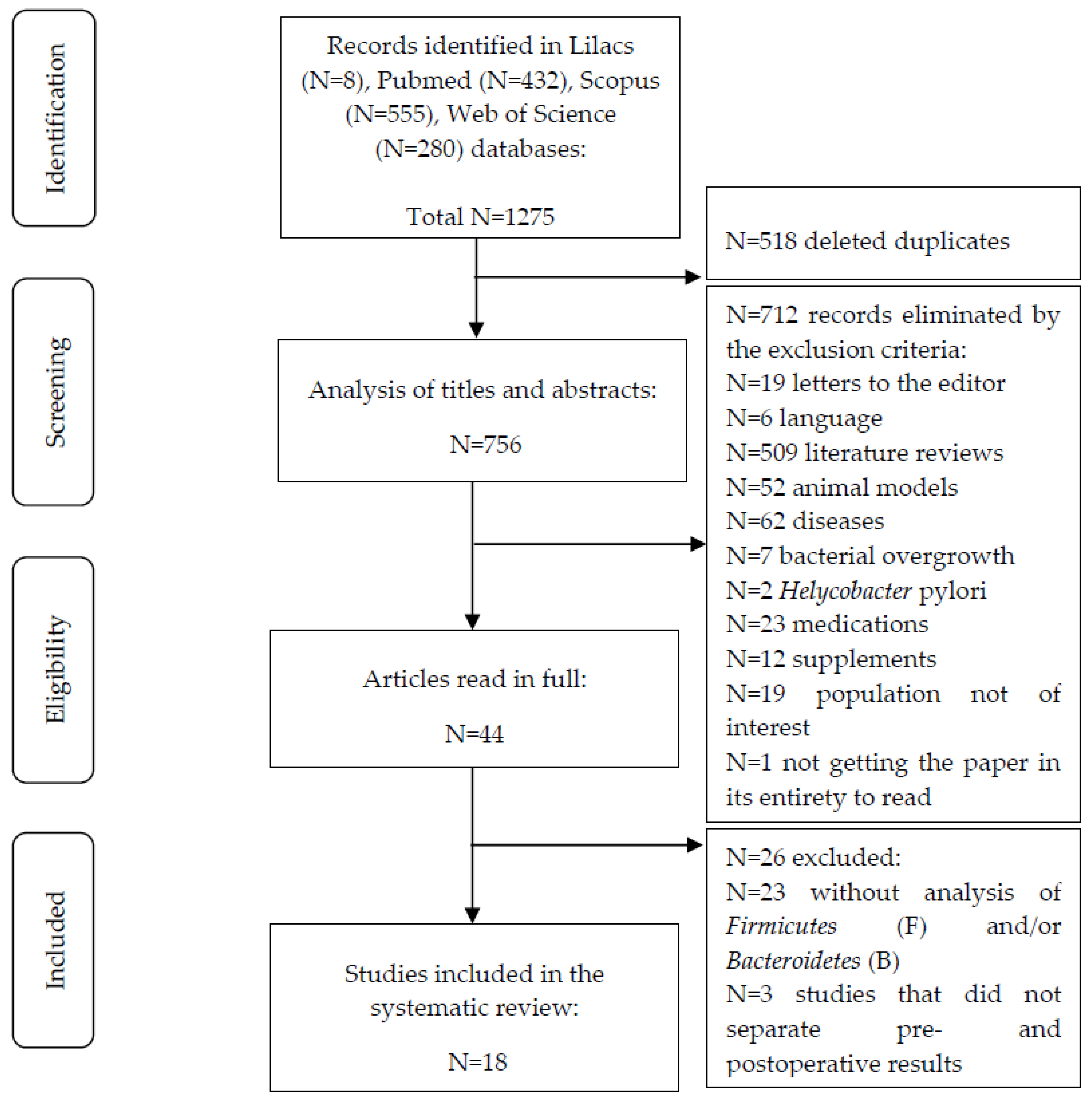
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO World Health Statistics 2016: Monitoring Health for the SDGs 2016. Available online: https://reliefweb.int/report/world/world-health-statistics-2016-monitoring-health-sdgs?gclid=Cj0KCQjwyt-ZBhCNARIsAKH1175VaFltqNiNjiLQjrWZswvD9yAIZmuL_W52N4Jyj5AZFvlZ6RDpBXIaAr8iEALw_wcB (accessed on 1 June 2021).
- ABESO Diretrizes Brasileiras de Obesidade 2016. Available online: https://abeso.org.br/wp-content/uploads/2019/12/Diretrizes-Download-Diretrizes-Brasileiras-de-Obesidade-2016.pdf (accessed on 1 March 2021).
- Zhou, H.; Urso, C.J.; Jadeja, V. Saturated Fatty Acids in Obesity-Associated Inflammation. J. Inflamm. Res. 2020, 13, 1–14. [Google Scholar] [CrossRef]
- Backhed, F.; Ding, H.; Wang, T.; Hooper, L.V.; Koh, G.Y.; Nagy, A.; Semenkovich, C.F.; Gordon, J.I. The Gut Microbiota as an Environmental Factor That Regulates Fat Storage. Proc. Natl. Acad. Sci. USA 2004, 101, 15718–15723. [Google Scholar] [CrossRef] [PubMed]
- Medina, D.A.; Pedreros, J.P.; Turiel, D.; Quezada, N.; Pimentel, F.; Escalona, A.; Garrido, D. Distinct Patterns in the Gut Microbiota after Surgical or Medical Therapy in Obese Patients. PeerJ 2017, 5, e3443. [Google Scholar] [CrossRef] [PubMed]
- Pajecki, D.; de Oliveira, L.C.; Sabino, E.C.; de Souza-Basqueira, M.; Dantas, A.C.B.; Nunes, G.C.; de Cleva, R.; Santo, M.A. Changes in the Intestinal Microbiota of Superobese Patients after Bariatric Surgery. Clinics 2019, 74, e1198. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Barrea, L.; Aprano, S.; Framondi, L.; Matteo, R.D.; Laudisio, D.; Pugliese, G.; Savastano, S.; Colao, A. Sleep Quality in Obesity: Does Adherence to the Mediterranean Diet Matter? Nutrients 2020, 12, 1364. [Google Scholar] [CrossRef] [PubMed]
- El Aidy, S.; Dinan, T.G.; Cryan, J.F. Gut Microbiota: The Conductor in the Orchestra of Immune–Neuroendocrine Communication. Clin. Ther. 2015, 37, 954–967. [Google Scholar] [CrossRef] [PubMed]
- Albaugh, V.L.; Banan, B.; Ajouz, H.; Abumrad, N.N.; Flynn, C.R. Bile Acids and Bariatric Surgery. Mol. Aspects. Med. 2017, 56, 75–89. [Google Scholar] [CrossRef] [PubMed]
- Ciobârcă, D.; Cătoi, A.F.; Copăescu, C.; Miere, D.; Crișan, G. Bariatric Surgery in Obesity: Effects on Gut Microbiota and Micronutrient Status. Nutrients 2020, 12, 235. [Google Scholar] [CrossRef]
- Furet, J.-P.; Kong, L.-C.; Tap, J.; Poitou, C.; Basdevant, A.; Bouillot, J.-L.; Mariat, D.; Corthier, G.; Dore, J.; Henegar, C.; et al. Differential Adaptation of Human Gut Microbiota to Bariatric Surgery-Induced Weight Loss: Links With Metabolic and Low-Grade Inflammation Markers. Diabetes 2010, 59, 3049–3057. [Google Scholar] [CrossRef]
- Palmisano, S.; Campisciano, G.; Silvestri, M.; Guerra, M.; Giuricin, M.; Casagranda, B.; Comar, M.; de Manzini, N. Changes in Gut Microbiota Composition after Bariatric Surgery: A New Balance to Decode. J. Gastrointest. Surg. 2019, 24, 1736–1746. [Google Scholar] [CrossRef]
- Aron-Wisnewsky, J.; Clément, K. The Gut Microbiome, Diet, and Links to Cardiometabolic and Chronic Disorders. Nat. Rev. Nephrol. 2016, 12, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a Web and Mobile App for Systematic Reviews. Syst. Ver. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Juárez-Fernández, M.; Román-Sagüillo, S.; Porras, D.; García-Mediavilla, M.V.; Linares, P.; Ballesteros-Pomar, M.D.; Urioste-Fondo, A.; Álvarez-Cuenllas, B.; González-Gallego, J.; Sánchez-Campos, S.; et al. Long-Term Effects of Bariatric Surgery on Gut Microbiota Composition and Faecal Metabolome Related to Obesity Remission. Nutrients 2021, 13, 2519. [Google Scholar] [CrossRef]
- Chen, G.; Zhuang, J.; Cui, Q.; Jiang, S.; Tao, W.; Chen, W.; Yu, S.; Wu, L.; Yang, W.; Liu, F.; et al. Two Bariatric Surgical Procedures Differentially Alter the Intestinal Microbiota in Obesity Patients. Obes. Surg. 2020, 30, 2345–2361. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.; O’Sullivan, J.M.; Plank, L.D.; Murphy, R. Gut Microbial Predictors of Type 2 Diabetes Remission Following Bariatric Surgery. Obes. Surg. 2020, 30, 3536–3548. [Google Scholar] [CrossRef]
- Faria, S.L.; Santos, A.; Magro, D.O.; Cazzo, E.; Assalin, H.B.; Guadagnini, D.; Vieira, F.T.; Dutra, E.S.; Saad, M.J.A.; Ito, M.K. Gut Microbiota Modifications and Weight Regain in Morbidly Obese Women After Roux-En-Y Gastric Bypass. Obes. Surg. 2020, 12, 4958–4966. [Google Scholar] [CrossRef] [PubMed]
- Farin, W.; Oñate, F.P.; Plassais, J.; Bonny, C.; Beglinger, C.; Woelnerhanssen, B.; Nocca, D.; Magoules, F.; Le Chatelier, E.; Pons, N.; et al. Impact of Laparoscopic Roux-En-Y Gastric Bypass and Sleeve Gastrectomy on Gut Microbiota: A Metagenomic Comparative Analysis. Surg. Obes. Relat. Dis. 2020, 16, 852–862. [Google Scholar] [CrossRef] [PubMed]
- Koffert, J.; Lahti, L.; Nylund, L.; Salmine, S.; Hannukainen, J.C.; Salminen, P.; de Vos, W.M.; Nuutila, P. Partial restoration of normal intestinal microbiota in morbidly obese women six months after bariatric surgery. PeerJ 2020, 8, e10442. [Google Scholar] [CrossRef] [PubMed]
- Al Assal, K.; Prifti, E.; Belda, E.; Sala, P.; Clément, K.; Dao, M.-C.; Doré, J.; Levenez, F.; Taddei, C.R.; Fonseca, D.C.; et al. Gut Microbiota Profile of Obese Diabetic Women Submitted to Roux-En-Y Gastric Bypass and Its Association with Food Intake and Postoperative Diabetes Remission. Nutrients 2020, 12, 278. [Google Scholar] [CrossRef]
- Gutiérrez-Repiso, C.; Moreno-Indias, I.; de Hollanda, A.; Martín-Núñez, G.M.; Vidal, J.; Tinahones, F.J. Gut Microbiota Specific Signatures Are Related to the Successful Rate of Bariatric Surgery. Am. J. Transl. Res. 2019, 11, 942–952. [Google Scholar]
- Lee, C.J.; Florea, L.; Sears, C.L.; Maruthur, N.; Potter, J.J.; Schweitzer, M.; Magnuson, T.; Clark, J.M. Changes in Gut Microbiome after Bariatric Surgery Versus Medical Weight Loss in a Pilot Randomized Trial. Obes. Surg. 2019, 29, 3239–3245. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.Y.; Lin, W.-D.; Huang, C.-K.; Hsin, M.-C.; Lin, W.-Y.; Pryor, A.D. Changes of Gut Microbiota between Different Weight Reduction Programs. Surg. Obes. Relat. Dis. 2019, 15, 749–758. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Alcoholado, L.; Gutiérrez-Repiso, C.; Gómez-Pérez, A.M.; García-Fuentes, E.; Tinahones, F.J.; Moreno-Indias, I. Gut Microbiota Adaptation after Weight Loss by Roux-En-Y Gastric Bypass or Sleeve Gastrectomy Bariatric Surgeries. Surg. Obes. Relat. Dis. 2019, 15, 1888–1895. [Google Scholar] [CrossRef]
- Cortez, R.V.; Petry, T.; Caravatto, P.; Pessôa, R.; Sanabani, S.S.; Martinez, M.B.; Sarian, T.; Salles, J.E.; Cohen, R.; Taddei, C.R. Shifts in Intestinal Microbiota after Duodenal Exclusion Favor Glycemic Control and Weight Loss: A Randomized Controlled Trial. Surg. Obes. Relat. Dis. 2018, 14, 1748–1754. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, R.; Irie, J.; Yamada-Goto, N.; Kikkawa, E.; Seki, Y.; Kasama, K.; Itoh, H. The Impact of Laparoscopic Sleeve Gastrectomy with Duodenojejunal Bypass on Intestinal Microbiota Differs from That of Laparoscopic Sleeve Gastrectomy in Japanese Patients with Obesity. Clin. Drug Investig. 2018, 38, 545–552. [Google Scholar] [CrossRef]
- Chen, H.; Qian, L.; Lv, Q.; Yu, J.; Wu, W.; Qian, H. Change in Gut Microbiota Is Correlated with Alterations in the Surface Molecule Expression of Monocytes after Roux-En-Y Gastric Bypass Surgery in Obese Type 2 Diabetic Patients. Am. J. Transl. Res. 2017, 9, 1243–1254. [Google Scholar]
- Sanmiguel, C.P.; Jacobs, J.; Gupta, A.; Ju, T.; Stains, J.; Coveleskie, K.; Lagishetty, V.; Balioukova, A.; Chen, Y.; Dutson, E.; et al. Surgically Induced Changes in Gut Microbiome and Hedonic Eating as Related to Weight Loss: Preliminary Findings in Obese Women Undergoing Bariatric Surgery. Psychosom. Med. 2017, 79, 880–887. [Google Scholar] [CrossRef]
- Murphy, R.; Tsai, P.; Jüllig, M.; Liu, A.; Plank, L.; Booth, M. Differential Changes in Gut Microbiota After Gastric Bypass and Sleeve Gastrectomy Bariatric Surgery Vary According to Diabetes Remission. Obes. Surg. 2016, 27, 917–925. [Google Scholar] [CrossRef]
- Ward, E.K.; Schuster, D.P.; Stowers, K.H.; Royse, A.K.; Ir, D.; Robertson, C.E.; Frank, D.N.; Austin, G.L. The Effect of PPI Use on Human Gut Microbiota and Weight Loss in Patients Undergoing Laparoscopic Roux-En-Y Gastric Bypass. Obes. Surg. 2014, 24, 1567–1571. [Google Scholar] [CrossRef]
- Campisciano, G.; Palmisano, S.; Cason, C.; Giuricin, M.; Silvestri, M.; Guerra, M.; Macor, D.; De Manzini, N.; Crocé, L.S.; Comar, M. Gut Microbiota Characterisation in Obese Patients before and after Bariatric Surgery. Benef. Microbes 2018, 9, 367–373. [Google Scholar] [CrossRef]
- Gralka, E.; Luchinat, C.; Tenori, L.; Ernst, B.; Thurnheer, M.; Schultes, B. Metabolomic Fingerprint of Severe Obesity Is Dynamically Affected by Bariatric Surgery in a Procedure-Dependent Manner. Am. J. Clin. Nutr. 2015, 102, 1313–1322. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Shu, X.-O.; Howard, E.F.; Long, J.; English, W.J.; Flynn, C.R. Fecal Metagenomics and Metabolomics Reveal Gut Microbial Changes after Bariatric Surgery. Surg. Obes. Relat. Dis. 2020, 16, 1772–1782. [Google Scholar] [CrossRef] [PubMed]
- Shen, N.; Caixàs, A.; Ahlers, M.; Patel, K.; Gao, Z.; Dutia, R.; Blaser, M.J.; Clemente, J.C.; Laferrère, B. Longitudinal Changes of Microbiome Composition and Microbial Metabolomics after Surgical Weight Loss in Individuals with Obesity. Surg. Obes. Relat. Dis. 2019, 15, 1367–1373. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.-H.; Lin, T.-L.; Lee, W.-J.; Chen, S.-C.; Lai, W.-F.; Lu, C.-C.; Lai, H.-C.; Chen, C.-Y. Impact of Metabolic Surgery on Gut Microbiota and Sera Metabolomic Patterns among Patients with Diabetes. Int. J. Mol. Sci. 2022, 23, 7797. [Google Scholar] [CrossRef] [PubMed]
- Graessler, J.; Qin, Y.; Zhong, H.; Zhang, J.; Licinio, J.; Wong, M.-L.; Xu, A.; Chavakis, T.; Bornstein, A.B.; Ehrhart-Bornstein, M.; et al. Metagenomic Sequencing of the Human Gut Microbiome before and after Bariatric Surgery in Obese Patients with Type 2 Diabetes: Correlation with Inflammatory and Metabolic Parameters. Pharm. J. 2013, 13, 514–522. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameters | Defined Criteria |
|---|---|
| Population | Individuals over the age of 18 with obesity or who were overweight. |
| Intervention | Bariatric surgery: sleeve gastrectomy (SG) and Roux-en-Y gastric bypass. |
| Comparison | Comparison of the gut microbiota profile at different pre- and postsurgical stages. |
| Outcomes | Identification of the impact of the BS on the composition of the GM. |
| Designs | Cohort studies, prospective longitudinal, nonrandomized, randomized clinical trial, and randomized controlled clinical trials. |
| Authors, Country | Study Population at Baseline (Age, BMI) | Sample Size (Surgical Procedures, Sex) | Study Design | Sequencing/Genetic Analysis | Stool Collection Period | Time of Followup |
|---|---|---|---|---|---|---|
| Juaréz-Fernandes et al., 2021 [15], Spain | Age (years): 18–60 BMI (kg/m²): 45.46 ± 2.05 | (N = 9) RYGB: (N = 1) SG: (N = 6) BPD: (N = 2) (M:F): 2:7 | Longitudinal | 16S rRNA (V3–V4) gene sequencing | Before and four years after BS | 4 years |
| Chen et al., 2020 [16], China | Age (years): 30.92 ± 9.17 RYGB: 33.24 ± 10.13 SG: 29.50 ± 8.31 BMI (kg/m²): 40.84 ± 10.67 RYGB: 45.75 ± 14.26 SG: 37.84 ± 6.16 | (N = 87) RYGB: (N = 33) (M:F): 14:19 SG: (N = 54) (M:F): 13:41 | Longitudinal | 16S rDNA (V3-V4) sequencing, RT-PCR | Before and 3 months after BS | 9.60 ± 3.92 months |
| Davies et al., 2020 [17], New Zealand | Age (years): 20–56 RYGB *: 48.5 ± 5.5 SG *: 47.7 ± 6.9 BMI (kg/m²): 35–65 RYGB *: 38.2 ± 5.7 SG *: 40.0 ± 5.9 | (N = 44) RYGB: (N = 22) (M:F): 7:15 SG: (N = 22) (M:F): 14:8 | Randomized Controlled Trial | Genome shotgun sequencing | 2 days before and 1 year after BS | 12 months |
| Faria et al., 2020 [18], Brazil | Age (years): 18–65 BMI (kg/m²): 35–49.9 | (N = 34) CG (preoperative patients): (N = 8) F: 8 RYGB: (N = 26 ) Non-regain: (N = 12) Regain: (N = 14) F: 26 | Cross-sectional | 16S rRNA gene sequencing (V3–V4) | RYGB non-regain: before and 55 months after BS RYGB regain: before and 84 months after BS | At least 5 years RYGB non-regain *: 54.9 ± 34.5 months RYGB regain *: 83.8 ± 40.8 months |
| Farin et al., 2020 [19], France | Age (years): ≥18 BMI (kg/m²): ≥35 | (N = 197) RYGB: (N = 89) SG: (N = 108) Both sexes | Cohort | Shotgun metagenomic sequencing | 1 month before and 6 months after BS | 6 months |
| Koffert et al., 2020 [20], Finland | Age (years): 18–60 BMI (kg/m²): ≥35 40.9 ± 4.2 | (N = 27) RYGB: (N = 6) SG: (N = 7) Controls: (N = 14) F:27 | Clinical trial | 16S rRNA gene sequences | Before and 6 months after BS | 6 months |
| Al Assal et al., 2019 [21], Brazil | Age (years): 18–60 RYGB *: 45.80 ± 7.95 BMI (kg/m²): ≥35 RYGB *: 46.40 ± 5.48 | (N = 25) RYGB: (N = 25) F: 25 | Cohort | 16S rRNA gene sequencing (V4) | Before and 3 and 12 months after BS | 12 months |
| Gutiérrez-Repiso et al., 2019 [22], Spain | Age (years): ≥18 RYGB *: 43.33 ± 9.97 BMI* (kg/m²): 47.03 ± 6.01 | (N = 24) RYGB: (N = 24) Both sexes | Prospective cohort | 16S rRNA (V2, 3, 4, 6-7, 8, and 9) metagenomic sequencing | Before and 8.3 ± 1.7 * years after BS | 8.3 ± 1.7 * years |
| Lee et al., 2019 [23], USA | Age ** (years): 52.5 (32–62) RYGB **: 57 (43–60) SG **: 45 (41–53) BMI (kg/m²): 30–40 RYGB **: 35.1 (31.3–38.6) SG **: 35.8 (33.0–37.6) | (N = 12) MWL: (N = 4) RYGB: (N = 4) SG: (N = 4) F: 12 | Randomized controlled pilot trial | 16S rRNA (V3–V4) amplicon sequencing | RYGB: Before and 1.8 (0.9–5.6) ** after BS SG: Before and 2.3 (2.1–4.3) ** after BS | 3.4 (0.9–9.6) ** months RYGB **: 1.8 (0.9–5.6) SG**: 2.3 (2.1–4.3) |
| Lin et al., 2019 [24], USA | Age (years): 20–64 SG *: 36.2 ± 9.9 BMI (kg/m²): ≥30 SG*: 35.9 ± 4.0 | (N = 10) SG: (N = 10) (M:F): 4:6 | Longitudinal | 16S rRNA (V4) amplicon sequencing | Before and 1 and 3 months after BS | 3 months |
| Sánchez-Alcoholado et al., 2019 [25], Spain | Age (years): 26–63 BMI (kg/m²): RYGB: 43.7 ± 5.3 SG: 46.9 ± 6.6 | (N = 28) RYGB: (N = 14) (M:F): 4:10 SG: (N = 14) (M:F): 4:10 | Longitudinal | 16S rDNA genes next-generation sequencing | Before and 3 months after BS | 3 months |
| Cortez et al., 2018 [26], Brazil | Age (years): 18–64 DJBm *: 47 ± 8 BMI (kg/m²): 25.0–39.9 DJBm *: 29.7 ± 1.9 | (N = 21) Standard medical treatment: (N = 10) DJBm: (N = 11) Sex: not stated | Randomized controlled trial | 16S rRNA (V4) gene sequencing | Before and after 6 and 12 months | 12 months |
| Kikuchi et al., 2018 [27], Japan | Age (years): 18–65 LSG-DJB *: 48.0 ± 2.5 SG *: 40.7 ± 2.0 BMI (kg/m²): >30 | (N = 44) LSG-DJB: (N = 18) (M:F): 10:8 SG: (N = 22) (M:F): 11:11 LAGB: (N = 4) (M:F): 0:4 | Nonrandomized prospective observational clinical trial | 16S rDNA sequencing, RT-PCR | 1, 3 and 6 months | 6 months |
| Chen et al., 2017 [28], China | Age * (years): 51.5 ± 9.6 BMI (kg/m²): ≥40 RYGB *: 46.3 ± 4.7 | (N = 24) RYGB: (N = 24) (M:F): 14:10 | Cohort | 16S rDNA sequencing, RT-PCR | Before and 180 days after BS | 6 months |
| Medina et al., 2017 [5], Chile | Age (years): 18–60 BMI (kg/m²): 30–50 RYGB *: 37.1 ± 2.8 SG *: 35.2 ± 2.4 | (N = 19) MD: (N = 9) RYGB: (N = 5) SG: (N = 5) Sex: not stated | Cohort | 16S rRNA gene sequencing (V3–V4), RT-PCR | Before and 6 months after BBS | 12 months |
| Sanmiguel et al., 2017 [29], EUA | Age * (years): 39.5 ± 8.7 BMI * (kg/m²): 44.1 ± 5.6 | (N = 8) SG: (N = 8) F: 8 | Longitudinal | 16S rRNA gene sequencing (V4) | Before and 1 month after BS | 1 month |
| Murphy et al., 2016 [30], New Zealand | Age (years): RYGB *: 48.6 ± 6.1 SG *: 48.3 ± 6.1 BMI (kg/m²): RYGB *: 38.4 ± 5.2 SG *: 36.9 ± 5.1 | (N = 14) RYGB: (N = 7) (M:F): 3:4 SG: (N = 7) (M:F): 5:2 | Double-blind clinical trial | Shotgun metagenomic sequencing | Before and 1 year after BS | 12 months |
| Ward et al., 2014 [31], USA | Age (years): 18–70 BMI (kg/m²): ≥40 RYGB *: 47.1 ± 4.8 | (N = 8) RYGB: (N = 8) (M:F): 1:7 | Longitudinal | 16S rRNA gene sequencing (V4) | 1 month before and 6 months after BS | 6 months |
| Surgical Procedures | Bacteroidetes | Firmicutes | Firmicutes and Bacteroidetes Ratio | Specific Bacteria |
|---|---|---|---|---|
| RYGB | Increased: 6 months [5,26,28]; 12 months [17,26]. Decreased: 3 months [16]; 6 months [20]; 5–7 years [18]. | Increased: 12 months [17,30]. Stable: 3 months [16]. Decreased: 6 months [5,19,26]; 4 years [15]. | Decreased: 6 months [5]. | B: Increased in 6 months for Succiniclastum sp., Bacteroides, Bacteroides coprophilus, Bacteroides eggerthii [5], Bacteroides, Alistipes [20,26]. F: Increased in 6 months for Clostridiaceae, Clostridium, Veillonella, Granucatiella, Oscillospira [25], Streptococcus [20,21], Sporobacter termitidis [20], Veillonella [21], Gemella, Granulicatella [16], Lactobacillus, Enterococcus [28], Lactobacillales sp. [5], Dialister, Ruminococcus, Roseburia, Acidamicoccus [25], Streptococcus, Veillonella, Roseburia, Enterococcus faecalis [19]; in 9 months for Faecalibacterium prausnitzii [23]; in 4 years for Clostridiaceae [14]; in 5–7 years for Streptococcus, Enterococcus, Lachnobacterium [18]. Decreased in 3 months for Peptostreptococcaceae [25]; in 4 years for Coprococcus Acinetobacter, Coprococcus, Lachnospira, Lactococcus, Megamonas, Oribacterium, Phascolarctobacterium [14]; in 5–7 years for Faecalibacterium [18]. |
| SG | Increased: 1 and 3 months [27]; 12 months [17,29]. Decreased: 6 months [5,20]. | Increased: 6 months [5]. Stable: 3 months [16]. Decreased: 6 months [19]; 12 months [29]; 4 years [15]. | Trend of Increase: 1 and 3 months [27]. Increased: 6 months [5]. Decreased: 12 months [29]. | B: Decreased in 3 months for Butyricimonas [16]. Increased in 6 months for Alistipes [20]. F: Increased in 1 and 3 months for Streptococcus [27]; in 3 months for Gemella, Granulicatella, Faecalibacterium [16]; in 6 months for Streptococcus luteciae [5], Streptococcus spp. [20], Sporobacter termitidis [20], Clostridium, Anaerostipes hadrus, Flavonifractor plautii, Ruminococcus gnavus, Oscillibacter sp. KLE, Veillonela, Streptococcus [19]; in 12 months for Roseburia intestinalis, Streptococcus, Lactobacillus [30], Bulleidia [29]; in 4 years for Clostridiaceae, Acinetobacter, Coprococcus, Lachnospira, Lactococcus, Megamonas, Oribacterium, Phascolarctobacterium [15]. Decreased in 3 months for Clostridiaceae, Anaerostipes [25]; in 6 months for Ruminococcus gnavus, Faecalibacterium prausnitzii [19]; in 4 years for Coprococcus [15]. |
| Surgical Procedures | Actinobacteria | Proteobacteria | Diversity | Specific Bacteria |
|---|---|---|---|---|
| RYGB | Increased: 6 months [5]; 9 months [23]; 12 months [30]. | Increased: 6 months [5]; 9 months [23]; 12 months [17]; 4 years [15]; 5–7 years [18]. | Trend of increase: 9 months [23]; 12 months [21]. Increased: 3 months [16]; 6 months [14,19,26]; 12 months [26,30]; 4 years [15]; 5–7 years [18]. Stable before and after BS: 3 months [25]; 6 months [31]; 12 months [17]. Decreased: 8,3 ± 1,7 years [22]. | A: Increased in 6 months for Bifidobacterium [28]; in 3 months for Slackia. Decreased in 3 months for Bifidobacteriaceae, Bifidobacterium, Collinsella [25]; in 6 months for Bifidobacteria bifidum [19]. P: Increased in 3 months for Enterobacteriacea [25], Neisseria [21], Klebsiella, Haemophilus [16]; in 6 months for Citrobacter [5]; in 12 months for Enterobacteriales [17], Escherichia coli, Klebsiella pneumoniae, Haemophilus parainfluenzae [19]; in 4 years for Enterobacteriaceae, Sinobacteriaceae [15]; in 5–7 years for Succinivibrio, Klebsiella [18]. Decreased in 6 months for Escherichia [28]; in 4 years for Acinetobacter [15]. Verrucomicrobia (Akkermansia muciniphila): Increased in median 1.75 months [23]; in 6 and 12 months [26]; in 9.60 ± 3.92 months [16]; in non-regain group in 5 years. Stable in regain group (15% weight gain increase after the lowest weight after BS) in 5 years [18]. |
| SG | _ | Increased: 6 months [5]; 4 years [15]. | Increased: 3 months [16,24]; 6 months [19,20]; 4 years [15]. Stable before and after BS: 12 months [17]. Stable between RYGB and Sleeve: 3 months [25]. | A: Increased in 12 months for Atopobium [29]. Decreased in 3 months for Bifidobacteriaceae, Bifidobacterium [25], Actinomyces [16]; in 6 months for Bifidobacteria dentium [19]; in 12 months for Bifidobacteriaceae [29]. P: Increased in 3 months for Haemophilus, Klebsiella [16]; in 6 months for Enterobacteriales Bulleidia, Escherichia coli [5], Klebsiella pneumoniae, Haemophilus parainfluenzae [19]; in 4 years for Enterobacteriaceae, Sinobacteriaceae [14]. Decreased in 3 months for Oxalobacter, Sutterella, Desulfovibrio [16]; in 4 years for Acinetobacter [14]. Verrucomicrobia (Akkermansia muciniphila): Increased in 3 months [27]; in 6 months [5]; in 9.60 ± 3.92 months [16]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coimbra, V.O.R.; Crovesy, L.; Ribeiro-Alves, M.; Faller, A.L.K.; Mattos, F.; Rosado, E.L. Gut Microbiota Profile in Adults Undergoing Bariatric Surgery: A Systematic Review. Nutrients 2022, 14, 4979. https://doi.org/10.3390/nu14234979
Coimbra VOR, Crovesy L, Ribeiro-Alves M, Faller ALK, Mattos F, Rosado EL. Gut Microbiota Profile in Adults Undergoing Bariatric Surgery: A Systematic Review. Nutrients. 2022; 14(23):4979. https://doi.org/10.3390/nu14234979
Chicago/Turabian StyleCoimbra, Vívian O. R., Louise Crovesy, Marcelo Ribeiro-Alves, Ana Luísa K. Faller, Fernanda Mattos, and Eliane L. Rosado. 2022. "Gut Microbiota Profile in Adults Undergoing Bariatric Surgery: A Systematic Review" Nutrients 14, no. 23: 4979. https://doi.org/10.3390/nu14234979
APA StyleCoimbra, V. O. R., Crovesy, L., Ribeiro-Alves, M., Faller, A. L. K., Mattos, F., & Rosado, E. L. (2022). Gut Microbiota Profile in Adults Undergoing Bariatric Surgery: A Systematic Review. Nutrients, 14(23), 4979. https://doi.org/10.3390/nu14234979