

Malnutrition Defined by Geriatric Nutritional Risk Index Predicts Outcomes in Severe Stroke Patients: A Propensity Score-Matched Analysis


Abstract
1. Introduction
2. Materials and Methods
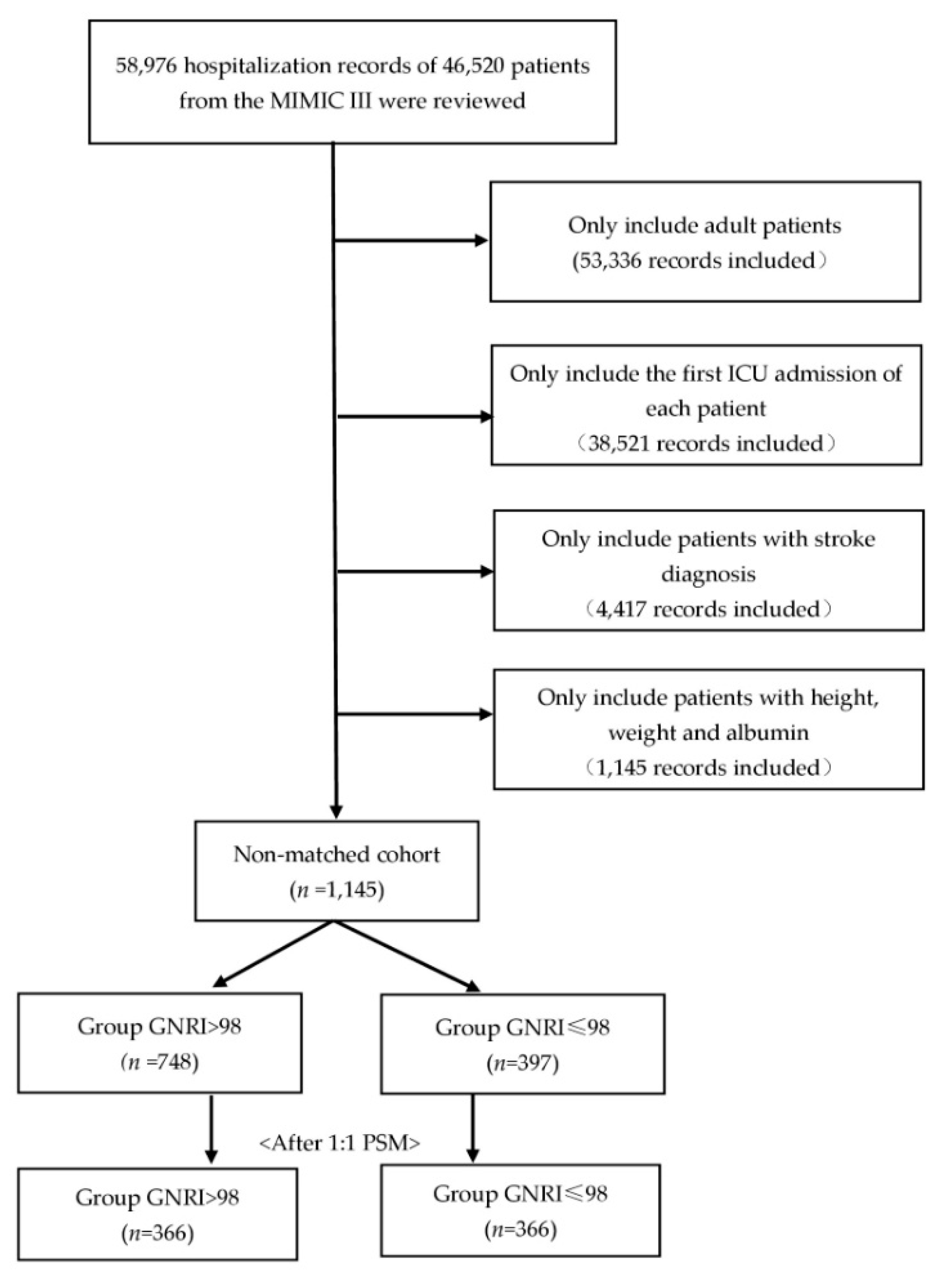
2.1. Study Population
2.2. Malnutrition Screening Tools and Endpoints Assessment
2.3. Data Extraction
2.4. Statistical Methods
2.5. Sensitivity Analyses
3. Results
3.1. Patient Characteristics
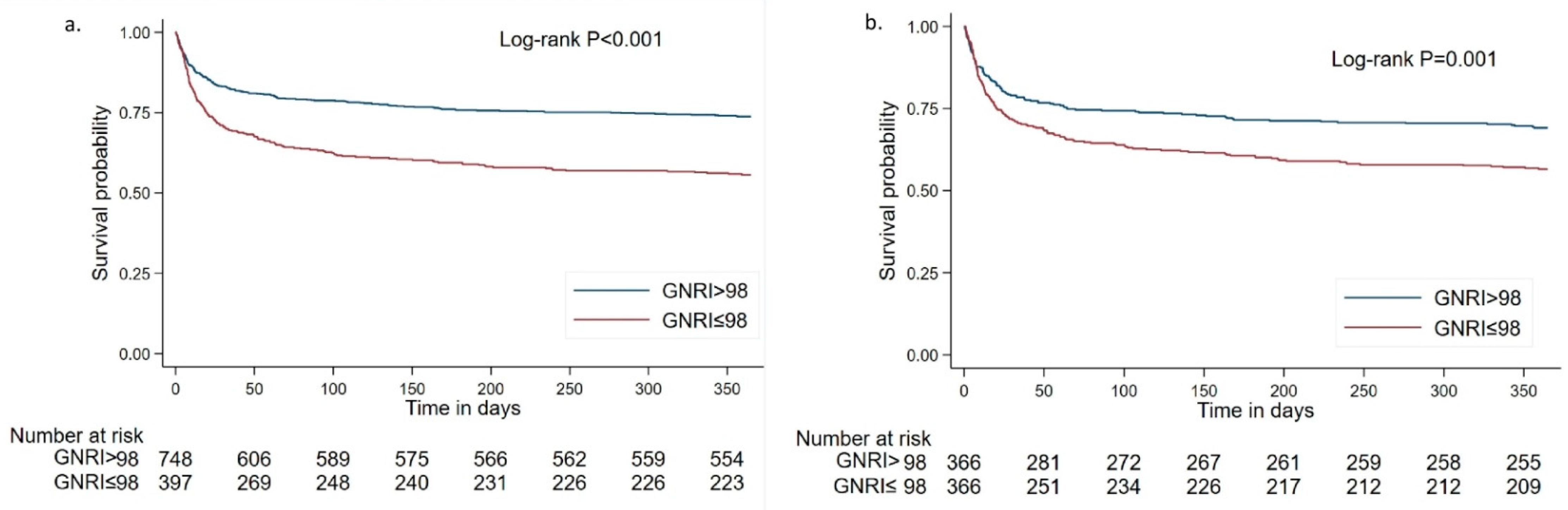
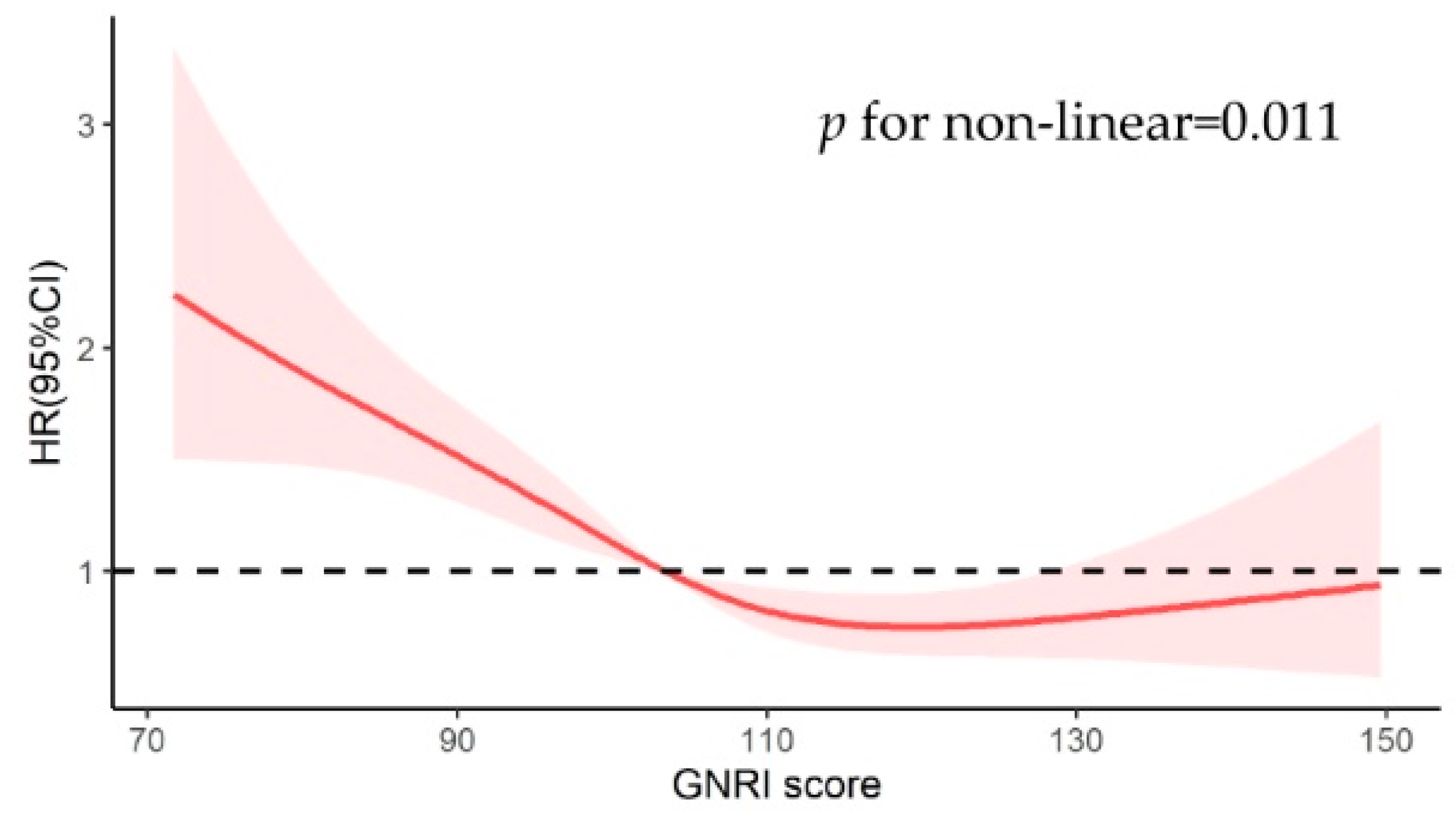
3.2. Association between Different GNRI Groups and Mortality
3.3. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maigeng, Z.; Haidong, W.; Xinying, Z.; Peng, Y.; Jun, Z.; Wanqing, C.; Xiaohong, L.; Lijun, W.; Limin, W.; Yunning, L. Mortality, Morbidity, and Risk Factors in China and Its Provinces, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2019, 394, 1145–1158. [Google Scholar]
- GBD 2019 Stroke Collaborators. Global, Regional, and National Burden of Stroke and Its Risk Factors, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2021 Update: A Report From the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef] [PubMed]
- Sweid, A.; Hammoud, B.; Ramesh, S.; Wong, D.; Alexander, T.D.; Weinberg, J.H.; Deprince, M.; Dougherty, J.; Maamari, D.J.; Tjoumakaris, S.; et al. Acute Ischaemic Stroke Interventions: Large Vessel Occlusion and Beyond. Stroke Vasc. Neurol. 2020, 5, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Zhang, J.; Jiang, X.; Wang, L.; Yin, Z.; Hall, M.; Wang, Y.; Lai, L. Is Endovascular Treatment Still Good for Ischemic Stroke in Real World?: A Meta-Analysis of Randomized Control Trial and Observational Study in the Last Decade. Stroke 2020, 51, 3250–3263. [Google Scholar] [CrossRef]
- Broderick, J.P.; Palesch, Y.Y.; Demchuk, A.M.; Yeatts, S.D.; Khatri, P.; Hill, M.D.; Jauch, E.C.; Jovin, T.G.; Yan, B.; Silver, F.L. Endovascular Therapy after Intravenous T-PA versus t-PA Alone for Stroke. N. Engl. J. Med. 2013, 368, 893–903. [Google Scholar] [CrossRef]
- Correia, M.I.; Waitzberg, D.L. The Impact of Malnutrition on Morbidity, Mortality, Length of Hospital Stay and Costs Evaluated through a Multivariate Model Analysis. Clin. Nutr. 2003, 22, 235–239. [Google Scholar] [CrossRef]
- Raposeiras, R.S.; Abu, A.E.; Cespon, F.M.; Barreiro, P.C.; Lizancos, C.A.; Parada, J.A.; Perez, D.D.; Blanco, P.S.; Rossello, X.; Ibanez, B.; et al. Prevalence and Prognostic Significance of Malnutrition in Patients With Acute Coronary Syndrome. J. Am. Coll. Cardiol. 2020, 76, 828–840. [Google Scholar] [CrossRef]
- Sze, S.; Pellicori, P.; Kazmi, S.; Rigby, A.; Cleland, J.; Wong, K.; Clark, A.L. Prevalence and Prognostic Significance of Malnutrition Using 3 Scoring Systems Among Outpatients With Heart Failure: A Comparison With Body Mass Index. JACC Heart Fail 2018, 6, 476–486. [Google Scholar] [CrossRef]
- Naito, H.; Hosomi, N.; Nezu, T.; Kuzume, D.; Aoki, S.; Morimoto, Y.; Yoshida, T.; Shiga, Y.; Kinoshita, N.; Ueno, H.; et al. Prognostic Role of the Controlling Nutritional Status Score in Acute Ischemic Stroke among Stroke Subtypes. J. Neurol. Sci. 2020, 416, 116984. [Google Scholar] [CrossRef]
- Chen, N.; Li, Y.; Fang, J.; Lu, Q.; He, L. Risk Factors for Malnutrition in Stroke Patients: A Meta-Analysis. Clin. Nutr. 2019, 38, 127–135. [Google Scholar] [CrossRef]
- Lamb, C.A.; Parr, J.; Lamb, E.I.M.; Warren, M.D. Adult Malnutrition Screening, Prevalence and Management in a United Kingdom Hospital: Cross-Sectional Study. Br. J. Nutr. 2009, 102, 571. [Google Scholar] [CrossRef]
- Yuan, K.; Zhu, S.; Wang, H.; Chen, J.; Zhang, X.; Xu, P.; Xie, Y.; Zhu, X.; Zhu, W.; Sun, W.; et al. Association between Malnutrition and Long-Term Mortality in Older Adults with Ischemic Stroke. Clin. Nutr. 2021, 40, 2535–2542. [Google Scholar] [CrossRef]
- Sabbouh, T.; Torbey, M.T. Malnutrition in Stroke Patients: Risk Factors, Assessment, and Management. Neurocrit. Care 2018, 29, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Yuan, F.; Song, C.; Yin, R.; Chang, M.; Zhang, W.; Zhang, B.; Yu, L.; Jia, Y.; Ma, Y.; et al. Safety and Efficacy of Three Enteral Feeding Strategies in Patients with Severe Stroke in China (OPENS): A Multicentre, Prospective, Randomised, Open-Label, Blinded-Endpoint Trial. Lancet Neurol. 2022, 21, 319–328. [Google Scholar] [CrossRef]
- Johnson, A.E.; Pollard, T.J.; Shen, L.; Lehman, L.W.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Celi, L.A.; Mark, R.G. MIMIC-III, a Freely Accessible Critical Care Database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A New Index for Evaluating at-Risk Elderly Medical Patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Riveros, C.; Jazayeri, S.B.; Chalfant, V.; Ahmed, F.; Bandyk, M.; Balaji, K.C. The Geriatric Nutritional Risk Index Predicts Postoperative Outcomes in Bladder Cancer: A Propensity Score-Matched Analysis. J. Urol. 2022, 207, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.M.; Li, S.; Claytor, L.; Partridge, J.; Goates, S. Prevalence and Predictors of Malnutrition in Elderly Chinese Adults: Results from the China Health and Retirement Longitudinal Study. Public Health Nutr. 2018, 21, 3129–3134. [Google Scholar] [CrossRef]
- Unosson, M.; Ek, A.C.; Bjurulf, P.; von Schenck, H.; Larsson, J. Feeding Dependence and Nutritional Status after Acute Stroke. Stroke 1994, 25, 366–371. [Google Scholar] [CrossRef]
- Foley, N.C.; Salter, K.L.; Robertson, J.; Teasell, R.W.; Woodbury, M.G. Which Reported Estimate of the Prevalence of Malnutrition after Stroke Is Valid? Stroke 2009, 40, e66–e74. [Google Scholar] [CrossRef]
- Haukoos, J.S.; Lewis, R.J. The Propensity Score. JAMA 2015, 314, 1637–1638. [Google Scholar] [CrossRef] [PubMed]
- Fanali, G.; di Masi, A.; Trezza, V.; Marino, M.; Fasano, M.; Ascenzi, P. Human Serum Albumin: From Bench to Bedside. Mol. Asp. Med. 2012, 33, 209–290. [Google Scholar]
- Geovanini, G.R.; Libby, P. Atherosclerosis and Inflammation: Overview and Updates. Clin. Sci. 2018, 132, 1243–1252. [Google Scholar] [CrossRef] [PubMed]
- Gimbrone, M.J.; Garcia-Cardena, G. Endothelial Cell Dysfunction and the Pathobiology of Atherosclerosis. Circ. Res. 2016, 118, 620–636. [Google Scholar] [CrossRef]
- Folsom, A.R.; Lutsey, P.L.; Heckbert, S.R.; Cushman, M. Serum Albumin and Risk of Venous Thromboembolism. Thromb. Haemost. 2010, 104, 100–104. [Google Scholar]
- Zhou, H.; Wang, A.; Meng, X.; Lin, J.; Jiang, Y.; Jing, J.; Zuo, Y.; Wang, Y.; Zhao, X.; Li, H.; et al. Low Serum Albumin Levels Predict Poor Outcome in Patients with Acute Ischaemic Stroke or Transient Ischaemic Attack. Stroke Vasc. Neurol. 2021, 6, 458–466. [Google Scholar] [CrossRef]
- Xu, W.H.; Dong, C.; Rundek, T.; Elkind, M.S.; Sacco, R.L. Serum Albumin Levels Are Associated with Cardioembolic and Cryptogenic Ischemic Strokes: Northern Manhattan Study. Stroke 2014, 45, 973–978. [Google Scholar] [CrossRef]
- Rodriguez-Castro, E.; Rodriguez-Yanez, M.; Arias-Rivas, S.; Santamaria-Cadavid, M.; Lopez-Dequidt, I.; Hervella, P.; Lopez, M.; Campos, F.; Sobrino, T.; Castillo, J. Obesity Paradox in Ischemic Stroke: Clinical and Molecular Insights. Transl. Stroke Res. 2019, 10, 639–649. [Google Scholar] [CrossRef]
- Liu, Z.; Sanossian, N.; Starkman, S.; Avila-Rinek, G.; Eckstein, M.; Sharma, L.K.; Liebeskind, D.; Conwit, R.; Hamilton, S.; Saver, J.L. Adiposity and Outcome After Ischemic Stroke: Obesity Paradox for Mortality and Obesity Parabola for Favorable Functional Outcomes. Stroke 2021, 52, 144–151. [Google Scholar] [CrossRef]
- Kondrup, J.; Rasmussen, H.H.; Hamberg, O.; Stanga, Z. Nutritional Risk Screening (NRS 2002): A New Method Based on an Analysis of Controlled Clinical Trials. Clin. Nutr. 2003, 22, 321–336. [Google Scholar] [CrossRef]
- Heyland, D.K.; Dhaliwal, R.; Jiang, X.; Day, A.G. Identifying Critically Ill Patients Who Benefit the Most from Nutrition Therapy: The Development and Initial Validation of a Novel Risk Assessment Tool. Crit. Care 2011, 15, R268. [Google Scholar] [CrossRef] [PubMed]
- Sharma, K.; Mogensen, K.M.; Robinson, M.K. Pathophysiology of Critical Illness and Role of Nutrition. Nutr. Clin. Pract. 2019, 34, 12–22. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Non-Matched Cohort | Matched Cohort | |||||
|---|---|---|---|---|---|---|
| Characteristics | High GNRI Group (≥98) | Low GNRI Group (<98) | p | High GNRI Group (≥98) | Low GNRI Group (<98) | p |
| n | 748 | 397 | NA | 366 | 366 | NA |
| Age, years | 65.17 ± 15.12 | 69.51 ± 15.29 | <0.001 | 69.63 ± 13.18 | 69.12 ± 15.42 | 0.49 |
| Male | 427 (57.1%) | 215 (54.2%) | 0.34 | 201 (54.9%) | 198 (54.1%) | 0.82 |
| Weight, kg | 87.55 ± 21.05 | 66.56 ± 13.59 | <0.001 | 86.03 ± 21.40 | 66.80 ± 13.66 | <0.001 |
| BMI | 30.34 ± 6.45 | 23.27 ± 3.57 | <0.001 | 31.11 ± 6.45 | 23.32 ± 3.59 | <0.001 |
| SAPS score | 18.69 ± 4.9 | 20.65 ± 5.06 | <0.001 | 20.27 ± 4.68 | 20.23 ± 4.81 | 0.13 |
| SOFA score | 4 (2–6) | 5 (3–7) | <0.001 | 4 (2–7) | 4 (3–7) | 0.38 |
| GNRI score | 112.57 ± 11.77 | 88.39 ± 7.42 | <0.001 | 111.46 ± 11.51 | 88.49 ± 7.31 | <0.001 |
| Types of stroke | ||||||
| Ischemic stroke | 413 (64%) | 228 (36%) | NA | 207 (48%) | 221 (52%) | NA |
| Hemorrhagic stroke | 335 (66%) | 169 (34%) | NA | 159 (52%) | 145 (48%) | NA |
| Comorbidities | ||||||
| CHF | 170 (22.7%) | 115 (29.0%) | 0.02 | 94 (25.7%) | 106 (29.0%) | 0.32 |
| Renal | 68 (9.1%) | 51 (12.9%) | 0.05 | 36 (9.8%) | 44 (12.0%) | 0.34 |
| AFIB | 241 (33.2%) | 127 (32.0%) | 0.94 | 123 (33.6%) | 118 (32.2%) | 0.69 |
| Liver | 18 (2.4%) | 15 (3.8%) | 0.19 | 12 (3.3%) | 11 (3.0%) | 0.83 |
| COPD | 57 (7.6%) | 55 (13.9%) | 0.001 | 46 (12.6%) | 40 (10.9%) | 0.49 |
| CHD | 247 (33.0%) | 103 (25.9%) | 0.01 | 118 (32.2%) | 92 (25.1%) | 0.03 |
| Malignancy | 100 (13.4%) | 66 (16.6%) | 0.14 | 52 (14.2%) | 52 (14.2) | 1.00 |
| AIDS | 0 (0%) | 5 (1.3%) | 0.005 | 0 (0%) | 4 (1.1%) | 0.045 |
| Diabetes | 237 (31.68%) | 92 (23.2%) | 0.002 | 93 (25.4%) | 89 (24.3%) | 0.73 |
| Sepsis | 51 (6.8%) | 52 (13.1%) | <0.001 | 37 (10.1%) | 40 (10.9%) | 0.72 |
| Vital signs | ||||||
| Heart rate | 82.64 ± 17.77 | 86.47 ± 19.82 | <0.001 | 84.83 ± 19.40 | 85.01 ± 18.99 | 0.75 |
| MAP | 87.12 ± 19.64 | 86.54 ± 19.68 | 0.63 | 87.54 ± 21.42 | 86.89 ± 19.44 | 0.33 |
| Temperature (°C) | 36.6 (36.0–37.1) | 36.6 (35.9–37.1) | 0.42 | 36.6 (35.9–37.0) | 36.6 (35.9–37.1) | 0.69 |
| Lab tests | ||||||
| Serum albumin, g/dL | 3.7 (3.4–4.0) | 3.0 (2.6–3.4) | <0.001 | 3.7 (3.3–4.0) | 3.0 (2.6–3.4) | <0.001 |
| WBC | 11.35 (8.50–14.50) | 11.30 (8.20–15.40) | 0.86 | 11.80 (9.00–15.05) | 11.05 (8.10–15.20) | 0.07 |
| Hb | 11.70 (9.80–13.10) | 10.50 (9.30–12.08) | <0.001 | 11.45 (9.28–12.90) | 10.60 (9.40–12.03) | 0.003 |
| Platelet | 200.00 (149.00–262.00) | 206.00 (147.00–268.00) | 0.70 | 197.00 (151.75–260.00) | 203.50 (146.25–269.00) | 0.56 |
| Sodium | 138.00 (136.00–141.00) | 139.00 (135.00–142.00) | 0.46 | 138.00 (136.00–141.00) | 139 (135.00–142.00) | 0.51 |
| Potassium | 4.00 (3.60–4.40) | 3.90 (3.60–4.40) | 0.17 | 4.00 (3.60–4.50) | 3.90 (3.60–4.40) | 0.08 |
| Bicarbonate | 24.00 (22.00–26.00) | 23.00 (21.00–26.00) | 0.008 | 23.00 (21.00–26.00) | 23.00 (21.00–25.00) | 0.18 |
| Chloride | 106.00 (102.00–108.00) | 106.00 (102.00–110.00) | 0.015 | 106.00 (102.00–109.00) | 107.00 (102.00–110.00) | 0.07 |
| BUN | 16.00 (12.00–24.00) | 18.00 (13.00–29.50) | <0.001 | 18.00 (13.00–27.00) | 18.00 (13.00–28.00) | 0.93 |
| Creatinine | 0.90 (0.70–1.20) | 0.90 (0.70–1.40) | 0.258 | 0.90 (0.70–1.30) | 0.90 (0.70–1.40) | 0.41 |
| Interventions | ||||||
| Sedative use | 452 (60.4%) | 241 (60.7%) | 0.93 | 243 (66.4%) | 222 (60.7%) | 0.11 |
| Infusion of thrombolytic agent | 49 (6.6%) | 19 (4.8%) | 0.23 | 20 (5.5%) | 18 (4.9%) | 0.21 |
| Endovascular removal of obstruction | 18 (2.4%) | 14 (3.5%) | 0.27 | 11 (3.0%) | 14 (3.8%) | 0.20 |
| Clinical Outcomes | ||||||
| Mortality_ 28-day | 125 (16.7%) | 114 (28.7%) | <0.001 | 76 (20.8%) | 102 (27.9%) | 0.025 |
| Mortality_ 90-day | 159 (21.3%) | 145 (36.5%) | <0.001 | 94 (25.7%) | 130 (35.5%) | 0.004 |
| Mortality_ 1-year | 196 (26.2%) | 176 (44.3%) | <0.001 | 113 (30.9%) | 159 (43.4%) | <0.001 |
| ICU LOS(d) | 8.23 ± 8.72 | 9.77 ± 9.70 | 0.006 | 8.32 ± 0.46 | 9.86 ± 0.51 | 0.024 |
| Outcomes | Hazard Ratio (95% CI) | p Value |
|---|---|---|
| 28-day mortality | 1.38 (1.03–1.86) | 0.03 |
| 90-day mortality | 1.45 (1.11–1.89) | 0.006 |
| 1-year mortality | 1.51 (1.19–1.92) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Yang, X.; Zhu, Y.; Zhang, X.; Ni, J.; Li, Y. Malnutrition Defined by Geriatric Nutritional Risk Index Predicts Outcomes in Severe Stroke Patients: A Propensity Score-Matched Analysis. Nutrients 2022, 14, 4786. https://doi.org/10.3390/nu14224786
Chen Y, Yang X, Zhu Y, Zhang X, Ni J, Li Y. Malnutrition Defined by Geriatric Nutritional Risk Index Predicts Outcomes in Severe Stroke Patients: A Propensity Score-Matched Analysis. Nutrients. 2022; 14(22):4786. https://doi.org/10.3390/nu14224786
Chicago/Turabian StyleChen, Ying, Xinguang Yang, Yingying Zhu, Xiaoni Zhang, Jingxian Ni, and Yi Li. 2022. "Malnutrition Defined by Geriatric Nutritional Risk Index Predicts Outcomes in Severe Stroke Patients: A Propensity Score-Matched Analysis" Nutrients 14, no. 22: 4786. https://doi.org/10.3390/nu14224786
APA StyleChen, Y., Yang, X., Zhu, Y., Zhang, X., Ni, J., & Li, Y. (2022). Malnutrition Defined by Geriatric Nutritional Risk Index Predicts Outcomes in Severe Stroke Patients: A Propensity Score-Matched Analysis. Nutrients, 14(22), 4786. https://doi.org/10.3390/nu14224786