Is Adolescents’ Free Sugar Intake Associated with the Free Sugar Intake of Their Parents?




Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Study Design and Sampling
2.3. Questionnaire Survey
- Demographic information: parent–student kinship, gender, age, Body Mass Index (BMI), and ethnicity; parent education, average monthly household income, and student pocket money.
- Free sugar intake of parents and students: free sugar intake of parents or students in the past month was collected by semi-quantitative FFQ. The semi-quantitative FFQ in our study was developed based on two previous studies conducted by the Chinese Center for Disease Control and Prevention (CDC) [33,34]. The options of intake frequency were set as never eat/drink, monthly frequency, weekly frequency, and daily frequency. To assess the total daily free sugar intake of individuals, the frequency of intake was all converted to daily frequency of intake, converting 1 time per week to 0.14 times/day, 2–3 times per week to 0.36 times/day, etc. In this study’s questionnaire, free sugar types included SSBs (carbonated beverages, tea drinks, fruit and vegetable juice drinks, plant protein drinks, functional drinks, milk tea, and flavored sour milk) and sugary foods (sugary snacks, candy, dried fruit, and honey).
- Parental free sugar KAP [35]: parents’ knowledge of free sugar, parents’ attitude toward controlling adolescents’ free sugar intake, parents’ behavior regarding the intake of sugary foods, purchase and storage behavior of beverages and desserts, and parents’ guidance behavior toward adolescents were considered.
- Classification of KAP: we divided the respondents into two categories based on the 75th percentile of their knowledge, attitude, and practice scores. Values less than P75 were defined as low levels of free sugar knowledge, negative attitudes, and poor behavior. On the contrary, others were defined as high levels of free sugar knowledge, positive attitudes, and better behaviors.
2.4. Free Sugar Intake Assessment
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Sample
3.2. Parental Free Sugar Intake Characteristics
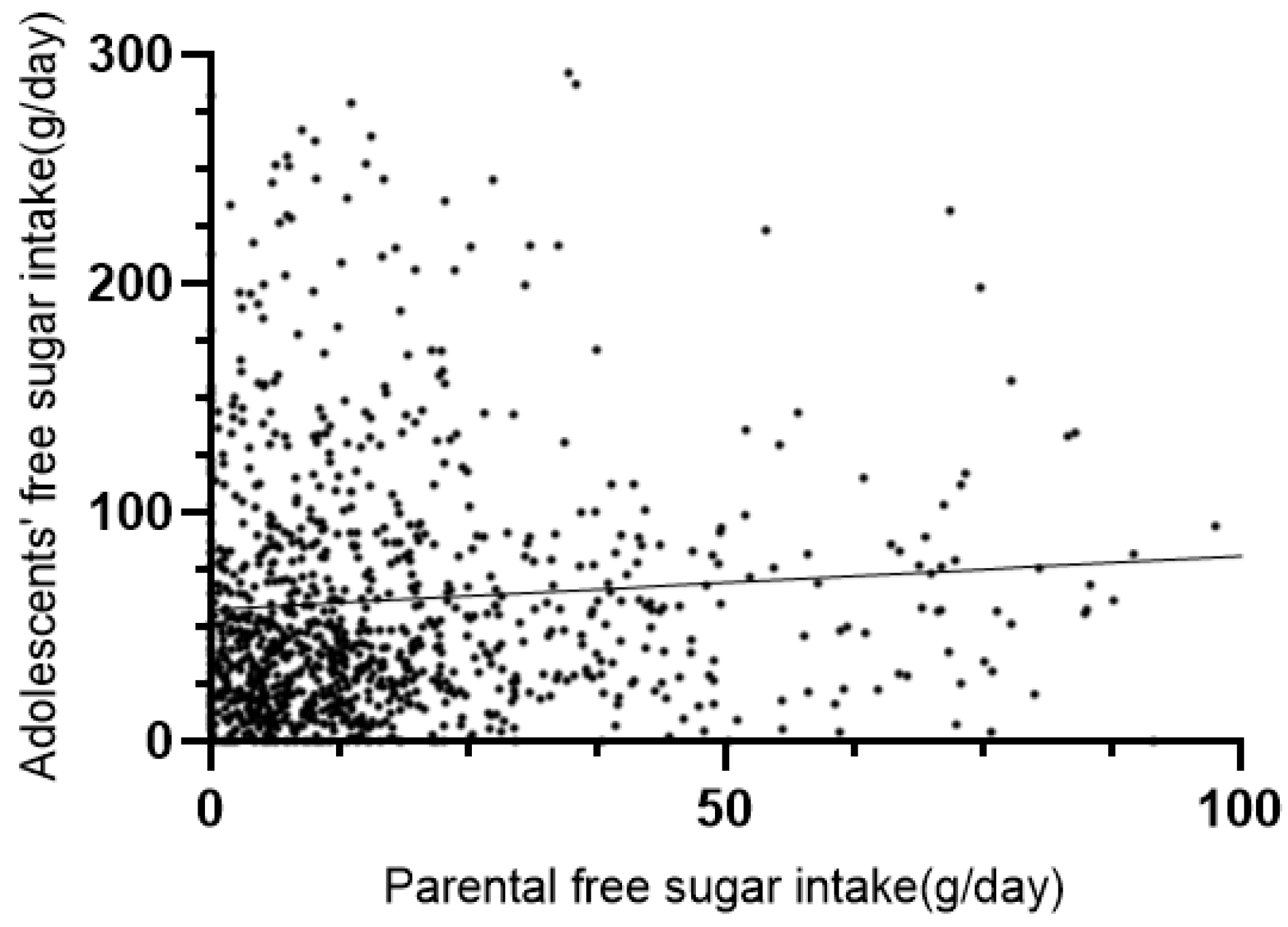
3.3. Association between Parental Free Sugar Intake and Adolescents’ Free Sugar Intake
3.4. Correlation between Parental Free Sugar KAP Levels and Adolescents’ Free Sugar Intake
3.5. Adolescents’ Free Sugar Intake in Terms of Parental Free Sugar Intake in Ordinal Logistic Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vartanian, L.R.; Schwartz, M.B.; Brownell, K.D. Effects of soft drink consumption on nutrition and health: A systematic review and meta-analysis. Am. J. Public Health 2007, 97, 667–675. [Google Scholar]
- Phipps, D.J.; Hagger, M.S.; Hamilton, K. Predicting limiting ‘free sugar’ consumption using an integrated model of health behavior. Appetite 2020, 150, 104668. [Google Scholar]
- Prinz, P. The role of dietary sugars in health: Molecular composition or just calories? Eur. J. Clin. Nutr. 2019, 73, 1216–1223. [Google Scholar]
- Moynihan, P. Sugars and Dental Caries: Evidence for Setting a Recommended Threshold for Intake. Adv. Nutr. 2016, 7, 149–156. [Google Scholar]
- Macdonald, I.A. Free sugars. Proc. Nutr. Soc. 2020, 79, 56–60. [Google Scholar]
- Ha, D.H.; Spencer, A.J.; Moynihan, P.; Thomson, W.M.; Do, L.G. Excess Risk of Dental Caries from Higher Free Sugars Intake Combined with Low Exposure to Water Fluoridation. J. Dent. Res. 2021, 100, 1243–1250. [Google Scholar]
- Yang, Q.; Xi, Y.; Liu, H.; Luo, J.; Ouyang, Y.; Sun, M.; Yong, C.; Xiang, C.; Lin, Q. Free Sugars Intake among Chinese Adolescents and Its Association with Dental Caries: A Cross-Sectional Study. Nutrients 2021, 13, 765. [Google Scholar]
- Xi, Y.; Lin, Q.; Yang, Q.; Li, F.; Liu, H.; Luo, J.; Ouyang, Y.; Sun, M.; Yong, C.; Xiang, C.; et al. Association between Free Sugars Intake and Excessive Daytime Sleepiness among Chinese Adolescents. Nutrients 2021, 13, 3959. [Google Scholar]
- Li, F.; Lin, Q.; Yang, Q.; Xi, Y.; Liu, H.; Luo, J.; Ouyang, Y.; Sun, M.; Yong, C.; Xiang, C.; et al. The Association between Free Sugars Consumption and Laryngopharyngeal Reflux: A Cross-Sectional Study among Chinese Adolescents. Nutrients 2021, 13, 3012. [Google Scholar]
- Te, M.L.; Howatson, A.J.; Jones, R.M.; Mann, J. Dietary sugars and cardiometabolic risk: Systematic review and meta-analyses of randomized controlled trials of the effects on blood pressure and lipids. Am. J. Clin. Nutr. 2014, 100, 65–79. [Google Scholar]
- Malik, V.S.; Hu, F.B. Sugar-Sweetened Beverages and Cardiometabolic Health: An Update of the Evidence. Nutrients 2019, 11, 1840. [Google Scholar]
- World Health Organization. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015. Available online: https://www.ncbi.nlm.nih.gov/books/NBK285537/ (accessed on 1 October 2022).
- Mela, D.J.; Woolner, E.M. Perspective: Total, Added, or Free? What Kind of Sugars Should We Be Talking About? Adv. Nutr. 2018, 9, 63–69. [Google Scholar]
- Mok, A.; Ahmad, R.; Rangan, A.; Louie, J. Intake of free sugars and micronutrient dilution in Australian adults. Am. J. Clin. Nutr. 2018, 107, 94–104. [Google Scholar]
- Paglia, L. The sweet danger of added sugars. Eur. J. Paediatr. Dent. 2019, 20, 89. [Google Scholar]
- Ma, Y.; He, F.J.; Yin, Y.; Hashem, K.M.; MacGregor, G.A. Gradual reduction of sugar in soft drinks without substitution as a strategy to reduce overweight, obesity, and type 2 diabetes: A modelling study. Lancet Diabetes Endocrinol. 2016, 4, 105–114. [Google Scholar]
- Rana, H.; Mallet, M.C.; Gonzalez, A.; Verreault, M.F.; St-Pierre, S. Free Sugars Consumption in Canada. Nutrients 2021, 13, 1471. [Google Scholar]
- Flieh, S.M.; Moreno, L.A.; Miguel-Berges, M.L.; Stehle, P.; Marcos, A.; Molnar, D.; Widhalm, K.; Beghin, L.; De Henauw, S.; Kafatos, A.; et al. Free Sugar Consumption and Obesity in European Adolescents: The HELENA Study. Nutrients 2020, 12, 3747. [Google Scholar]
- Liu, Y.; Shi, M.; Pan, F.; Li, G.; Luan, D.; Liu, A.; Li, N.; Li, J. The content of total free sugars in commercial sugary beverages in China. Chin. J. Food Hyg. 2021, 33, 93–96. [Google Scholar]
- Pan, F.; Luan, D.; Zhang, T.; Mao, W.; Liang, D.; Liu, A.; Li, J. Assessment of sugar-sweetened beverages consumption and free sugar intake among urban residents aged 3 years and above in China. Chin. J. Food Hyg. 2022, 34, 126–130. [Google Scholar]
- Zhuang, X.; Liu, Y.; Gittelsohn, J.; Lewis, E.; Song, S.; Ma, Y.; Wen, D. Sugar-Sweetened Beverages Consumption and Associated Factors among Northeastern Chinese Children. Nutrients 2021, 13, 2233. [Google Scholar]
- Park, S.; Blanck, H.M.; Sherry, B.; Brener, N.; O’Toole, T. Factors associated with sugar-sweetened beverage intake among United States high school students. J. Nutr. 2012, 142, 306–312. [Google Scholar]
- Rippe, J.M.; Angelopoulos, T.J. Relationship between Added Sugars Consumption and Chronic Disease Risk Factors: Current Understanding. Nutrients 2016, 8, 697. [Google Scholar]
- Vos, M.B.; Kaar, J.L.; Welsh, J.A.; Van Horn, L.V.; Feig, D.I.; Anderson, C.; Patel, M.J.; Cruz, M.J.; Krebs, N.F.; Xanthakos, S.A.; et al. Added Sugars and Cardiovascular Disease Risk in Children: A Scientific Statement from the American Heart Association. Circulation 2017, 135, e1017–e1034. [Google Scholar]
- Lei, L.; Rangan, A.; Flood, V.M.; Louie, J.C. Dietary intake and food sources of added sugar in the Australian population. Br. J. Nutr. 2016, 115, 868–877. [Google Scholar]
- Azais-Braesco, V.; Sluik, D.; Maillot, M.; Kok, F.; Moreno, L.A. A review of total & added sugar intakes and dietary sources in Europe. Nutr. J. 2017, 16, 6. [Google Scholar]
- Hoffman, A.C.; Salgado, R.V.; Dresler, C.; Faller, R.W.; Bartlett, C. Flavour preferences in youth versus adults: A review. Tob. Control. 2016, 25, i32–i39. [Google Scholar]
- Van der Horst, K.; Oenema, A.; Ferreira, I.; Wendel-Vos, W.; Giskes, K.; van Lenthe, F.; Brug, J. A systematic review of environmental correlates of obesity-related dietary behaviors in youth. Health Educ. Res. 2007, 22, 203–226. [Google Scholar]
- Bjelland, M.; Lien, N.; Grydeland, M.; Bergh, I.H.; Anderssen, S.A.; Ommundsen, Y.; Klepp, K.I.; Andersen, L.F. Intakes and perceived home availability of sugar-sweetened beverages, fruit and vegetables as reported by mothers, fathers and adolescents in the HEIA (HEalth in Adolescents) study. Public Health Nutr. 2011, 14, 2156–2165. [Google Scholar]
- Bogart, L.M.; Cowgill, B.O.; Sharma, A.J.; Uyeda, K.; Sticklor, L.A.; Alijewicz, K.E.; Schuster, M.A. Parental and home environmental facilitators of sugar-sweetened beverage consumption among overweight and obese Latino youth. Acad. Pediatr. 2013, 13, 348–355. [Google Scholar]
- Yuhas, M.; Porter, K.J.; Hedrick, V.; Zoellner, J.M. Using a Socioecological Approach to Identify Factors Associated with Adolescent Sugar-Sweetened Beverage Intake. J. Acad. Nutr. Diet. 2020, 120, 1557–1567. [Google Scholar]
- Mumena, W.A. Maternal Knowledge, Attitude and Practices toward Free Sugar and the Associations with Free Sugar Intake in Children. Nutrients 2021, 13, 4403. [Google Scholar]
- Liu, S. The Status and Change of Sugary Food Consumption and Its Relationship with Overweight and Obesity in Chinese Residents during 2002–2012; Chinese Center for Disease Control and Prevention: Beijing, China, 2016. [Google Scholar]
- Hou, L. Analysis of Sugar Content in Prepackaged Foods and Its Application in Population Sugar Intake Assessment in China; Chinese Center for Disease Control and Prevention: Beijing, China, 2017. [Google Scholar]
- Tang, Q.; Lin, Q.; Yang, Q.; Sun, M.; Liu, H.; Yang, L. Knowledge, Attitude, and Practice of Adolescent Parents on Free Sugar and Influencing Factors about Recognition. Int. J. Environ. Res. Public Health 2020, 17, 4003. [Google Scholar]
- The Chinese Nutrition Society. Dietary Guidelines for Chinese Residents—2022; The Chinese Nutrition Society: Beijing, China, 2022. [Google Scholar]
- Walton, J.; Bell, H.; Re, R.; Nugent, A.P. Current perspectives on global sugar consumption: Definitions, recommendations, population intakes, challenges and future direction. Nutr. Res. Rev. 2021, 1–22. [Google Scholar] [CrossRef]
- Bjelland, M.; Hausken, S.E.; Sleddens, E.F.; Andersen, L.F.; Lie, H.C.; Finset, A.; Maes, L.; Melbye, E.L.; Glavin, K.; Hanssen-Bauer, M.W.; et al. Development of family and dietary habits questionnaires: The assessment of family processes, dietary habits and adolescents’ impulsiveness in Norwegian adolescents and their parents. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 130. [Google Scholar]
- Vandeweghe, L.; Moens, E.; Braet, C.; Van Lippevelde, W.; Vervoort, L.; Verbeken, S. Perceived effective and feasible strategies to promote healthy eating in young children: Focus groups with parents, family child care providers and daycare assistants. BMC Public Health 2016, 16, 1045. [Google Scholar]
- Hanson, N.I.; Neumark-Sztainer, D.; Eisenberg, M.E.; Story, M.; Wall, M. Associations between parental report of the home food environment and adolescent intakes of fruits, vegetables and dairy foods. Public Health Nutr. 2005, 8, 77–85. [Google Scholar]
- Arredondo, E.M.; Elder, J.P.; Ayala, G.X.; Campbell, N.; Baquero, B.; Duerksen, S. Is parenting style related to children’s healthy eating and physical activity in Latino families? Health Educ. Res. 2006, 21, 862–871. [Google Scholar]
- Patrick, H.; Nicklas, T.A.; Hughes, S.O.; Morales, M. The benefits of authoritative feeding style: Caregiver feeding styles and children’s food consumption patterns. Appetite 2005, 44, 243–249. [Google Scholar]
- Schwimmer, J.B.; Ugalde-Nicalo, P.; Welsh, J.A.; Angeles, J.E.; Cordero, M.; Harlow, K.E.; Alazraki, A.; Durelle, J.; Knight-Scott, J.; Newton, K.P.; et al. Effect of a Low Free Sugar Diet vs Usual Diet on Nonalcoholic Fatty Liver Disease in Adolescent Boys: A Randomized Clinical Trial. JAMA J. Am. Med. Assoc. 2019, 321, 256–265. [Google Scholar]
- Elfhag, K.; Tholin, S.; Rasmussen, F. Consumption of fruit, vegetables, sweets and soft drinks are associated with psychological dimensions of eating behaviour in parents and their 12-year-old children. Public Health Nutr. 2008, 11, 914–923. [Google Scholar]
- Imoisili, O.E.; Park, S.; Lundeen, E.A.; Yaroch, A.L.; Blanck, H.M. Daily Adolescent Sugar-Sweetened Beverage Intake Is Associated with Select Adolescent, Not Parent, Attitudes about Limiting Sugary Drink and Junk Food Intake. Am. J. Health Promot. 2020, 34, 76–82. [Google Scholar]
- Fulkerson, J.A.; Friend, S.; Horning, M.; Flattum, C.; Draxten, M.; Neumark-Sztainer, D.; Gurvich, O.; Garwick, A.; Story, M.; Kubik, M.Y. Family Home Food Environment and Nutrition-Related Parent and Child Personal and Behavioral Outcomes of the Healthy Home Offerings via the Mealtime Environment (HOME) Plus Program: A Randomized Controlled Trial. J. Acad. Nutr. Diet. 2018, 118, 240–251. [Google Scholar]
- Shier, V.; Nicosia, N.; Datar, A. Neighborhood and home food environment and children’s diet and obesity: Evidence from military personnel’s installation assignment. Soc. Sci. Med. 2016, 158, 122–131. [Google Scholar]
- Bogart, L.M.; Elliott, M.N.; Ober, A.J.; Klein, D.J.; Hawes-Dawson, J.; Cowgill, B.O.; Uyeda, K.; Schuster, M.A. Home Sweet Home: Parent and Home Environmental Factors in Adolescent Consumption of Sugar-Sweetened Beverages. Acad. Pediatr. 2017, 17, 529–536. [Google Scholar]
- Zahid, A.; Davey, C.; Reicks, M. Beverage Intake among Children: Associations with Parent and Home-Related Factors. Int. J. Environ. Res. Public Health 2017, 14, 929. [Google Scholar]
- Hock, K.; Acton, R.B.; Jauregui, A.; Vanderlee, L.; White, C.M.; Hammond, D. Experimental study of front-of-package nutrition labels’ efficacy on perceived healthfulness of sugar-sweetened beverages among youth in six countries. Prev. Med. Rep. 2021, 24, 101577. [Google Scholar]
- National Health Commission of the People’s Republic of China. Notification on the issuance of the national healthy lifestyle action program (2017–2025). Gaz. Natl. Health Fam. Plan. Comm. People’s Repub. China 2017, 4, 61–64. [Google Scholar]
- Orehek, E.; Ferrer, R. Parent Instrumentality for Adolescent Eating and Activity. Ann. Behav. Med. 2019, 53, 652–664. [Google Scholar]


{kind=link}
| Characteristics | Parents | Adolescents | ||
|---|---|---|---|---|
| Sample Size (n) | Percentage (%) | Sample Size (n) | Percentage (%) | |
| Gender | ||||
| Male | 326 | 29.9 | 569 | 52.2 |
| Female | 764 | 70.1 | 521 | 47.8 |
| Parental role | ||||
| Father | 315 | 28.9 | - | - |
| Mother | 757 | 69.4 | - | - |
| Grandparents | 18 | 1.7 | - | - |
| Age # | 1090 | 41.85 ± 5.28 | 1090 | 13.54 ± 0.64 |
| Ethnicity | ||||
| Hans | 1051 | 96.4 | 1051 | 96.4 |
| Minorities | 39 | 3.6 | 39 | 3.6 |
| Parental education | ||||
| ≤Primary school | 25 | 2.3 | - | - |
| Middle school | 261 | 23.9 | - | - |
| (Vocational) high school | 465 | 42.7 | - | - |
| ≥College | 339 | 31.1 | - | - |
| Family monthly income | ||||
| CNY ≤ 1000 | 20 | 1.8 | - | - |
| CNY 1001–3000 | 193 | 17.7 | - | - |
| CNY 3001–5000 | 299 | 27.4 | - | - |
| CNY 5001–7000 | 223 | 20.5 | - | - |
| CNY ≥7001 | 355 | 32.6 | - | - |
| Student pocket money | ||||
| Low | - | - | 1026 | 94.1 |
| Medium | - | - | 27 | 2.5 |
| High | - | - | 32 | 2.9 |
| BMI | ||||
| Wasting | 62 | 5.7 | 42 | 3.9 |
| Normal | 735 | 67.4 | 755 | 69.3 |
| Overweight | 249 | 22.8 | 130 | 11.9 |
| Obese | 44 | 4.0 | 163 | 15.0 |
| Characteristics | Parental Free Sugar Intake Level (n, %) | p-Value | ||
|---|---|---|---|---|
| Low (<25 g) | Middle (25~50 g) | High (>50 g) | ||
| Total | 861 (79.0) | 147 (13.5) | 82 (7.5) | |
| Gender | ||||
| Male | 267 (81.9) | 35 (10.7) | 24 (7.4) | 0.152 |
| Female | 594 (77.7) | 112 (14.7) | 58 (7.6) | |
| Ages | ||||
| ≤40 year | 372 (74.4) | 82 (16.4) | 46 (9.2) | 0.003 ** |
| 41–50 year | 449 (82.7) | 62 (11.4) | 32 (5.9) | |
| ≥51 year | 40 (85.1) | 3 (6.4) | 4 (8.5) | |
| Ethnicity | ||||
| Hans | 827 (78.7) | 143 (23.6) | 81 (7.7) | 0.182 |
| Minorities | 34 (87.2) | 4 (10.3) | 1 (2.6) | |
| Parental education | ||||
| ≤Primary school | 17 (68.0) | 6 (24.0) | 2 (8.0) | 0.094 |
| Middle school | 199 (76.2) | 35 (13.4) | 27 (10.3) | |
| (Vocational) high school | 365 (78.5) | 62 (13.3) | 38 (8.2) | |
| ≥College | 280 (82.6) | 44 (13.0) | 15 (4.4) | |
| Family monthly income | ||||
| CNY ≤ 1000 | 18 (90.0) | 0 (0.0) | 2 (10.0) | 0.668 |
| CNY 1001–3000 | 148 (76.7) | 28 (14.5) | 17 (8.8) | |
| CNY 3001–5000 | 234 (78.3) | 50 (16.7) | 15 (5.0) | |
| CNY 5001–7000 | 175 (78.5) | 26 (11.7) | 22 (9.9) | |
| CNY ≥7001 | 286 (80.6) | 43 (12.1) | 26 (7.3) | |
| BMI | ||||
| Wasting | 49 (79.0) | 9 (14.5) | 4 (6.5) | 0.364 |
| Normal | 584 (79.5) | 95 (12.9) | 56 (7.6) | |
| Overweight | 198 (79.5) | 34 (13.7) | 17 (6.8) | |
| Obese | 30 (68.2) | 9 (20.5) | 5 (11.4) | |
| Free sugar knowledge level (K) | ||||
| Poor | 648 (78.3) | 116 (14.0) | 64 (7.7) | 0.304 |
| Better | 213 (81.3) | 31 (11.8) | 18 (6.9) | |
| Parental attitude (A) | ||||
| Poor | 424 (76.1) | 84 (15.1) | 49 (8.8) | 0.016 * |
| Better | 437 (82.0) | 63 (11.8) | 33 (6.2) | |
| Parental practice (P) | ||||
| Poor | 611 (73.5) | 141 (17.0) | 79 (9.5) | <0.001 *** |
| Better | 250 (96.5) | 6 (2.3) | 3 (1.2) | |
| Intake behavior | ||||
| Poor | 263 (31.1) | 217 (25.7) | 366 (43.3) | <0.001 *** |
| Better | 88 (36.1) | 69 (28.3) | 87 (35.7) | |
| Purchase and storage behavior | ||||
| Poor | 278 (33.5) | 219 (26.4) | 334 (40.2) | 0.807 |
| Better | 73 (28.2) | 67 (25.9) | 119 (45.9) | |
| Guidance behavior | ||||
| Poor | 270 (30.8) | 225 (25.6) | 383 (43.6) | 0.002 ** |
| Better | 81 (38.2) | 61 (28.8) | 70 (33.0) | |
| Parental Free Sugar Intake | Adolescents’ Free Sugar Intake (n, %) | Total | rs | p-Value | ||
|---|---|---|---|---|---|---|
| Low (<25 g) | Middle (25~50 g) | High (>50 g) | ||||
| Low (<25 g) | 307 (35.7) | 226 (26.2) | 328 (38.1) | 861 | 0.159 | p < 0.001 |
| Middle (25~50 g) | 29 (19.7) | 43 (29.3) | 75 (51.0) | 147 | ||
| High (>50 g) | 15 (18.3) | 17 (20.7) | 50 (61.0) | 82 | ||
| Total | 351 (32.2) | 286 (26.2) | 453 (41.6) | 1090 | ||
| Parental Free Sugar KAP | Adolescents’ Free Sugar Intake (n, %) | rs | p-Value | ||
|---|---|---|---|---|---|
| Low (<25 g) | Middle (25~50 g) | High (>50 g) | |||
| Free sugar knowledge level (K) | |||||
| Poor | 251 (30.3) | 214 (25.8) | 363 (43.8) | −0.087 | 0.004 ** |
| Better | 100 (38.2) | 72 (27.5) | 90 (34.4) | ||
| Parental attitude (A) | |||||
| Poor | 174 (31.2) | 153 (27.5) | 230 (41.3) | −0.007 | 0.812 |
| Better | 177 (33.2) | 133 (25.0) | 223 (41.8) | ||
| Parental practice (P) | |||||
| Poor | 251 (30.2) | 212 (25.5) | 368 (44.3) | −0.100 | 0.001 ** |
| Better | 100 (38.6) | 74 (28.6) | 85 (32.8) | ||
| Intake behavior | |||||
| Poor | 263 (31.1) | 217 (25.7) | 366 (43.3) | −0.062 | 0.040 * |
| Better | 88 (36.1) | 69 (28.3) | 87 (35.7) | ||
| Purchase and storage behavior | |||||
| Poor | 278 (33.5) | 219 (26.4) | 334 (40.2) | 0.055 | 0.070 |
| Better | 73 (28.2) | 67 (25.9) | 119 (45.9) | ||
| Guidance behavior | |||||
| Poor | 270 (30.8) | 225 (25.6) | 383 (43.6) | −0.085 | 0.005 ** |
| Better | 81 (38.2) | 61 (28.8) | 70 (33.0) | ||
| Variable | Model 1 a (OR, 95% CI) | Model 2 b (OR, 95% CI) | Model 3 c (OR, 95% CI) |
|---|---|---|---|
| Parental free sugar KAP (Poor = ref) | |||
| Better knowledge level | 0.720 (0.555, 0.934) * | 0.717 (0.551, 0.934) * | 0.726 (0.557, 0.946) * |
| Better attitude | 1.065 (0.851, 1.333) | 1.058 (0.842, 1.329) | 1.080 (0.859, 1.359) |
| Better practice | 0.710 (0.467, 1.080) | 0.710 (0.465, 1.085) | 0.718 (0.469, 1.101) |
| Better intake behavior | 1.203 (0.795, 1.822) | 1.203 (0.790, 1.832) | 1.138 (0.744, 1.740) |
| Better purchase and storage behavior | 1.246 (0.956, 1.625) | 1.257 (0.960, 1.647) | 1.238 (0.944, 1.623) |
| Better guidance behavior | 0.829 (0.613, 1.121) | 0.837 (0.617, 1.134) | 0.861 (0.634, 1.168) |
| Parental free sugar intake (Low = ref) | |||
| Middle (25~50 g) | 1.760 (1.256, 2.465) ** | 1.697 (1.208, 2.386) ** | 1.706 (1.212, 2.401) ** |
| High (>50 g) | 2.369 (1.500, 3.744) ** | 2.371 (1.493, 3.763) ** | 2.372 (1.492, 3.773) ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, R.; Yang, Q.; Tang, Q.; Xi, Y.; Lin, Q.; Yang, L. Is Adolescents’ Free Sugar Intake Associated with the Free Sugar Intake of Their Parents? Nutrients 2022, 14, 4741. https://doi.org/10.3390/nu14224741
Zhang R, Yang Q, Tang Q, Xi Y, Lin Q, Yang L. Is Adolescents’ Free Sugar Intake Associated with the Free Sugar Intake of Their Parents? Nutrients. 2022; 14(22):4741. https://doi.org/10.3390/nu14224741
Chicago/Turabian StyleZhang, Rou, Qiping Yang, Qiong Tang, Yue Xi, Qian Lin, and Lina Yang. 2022. "Is Adolescents’ Free Sugar Intake Associated with the Free Sugar Intake of Their Parents?" Nutrients 14, no. 22: 4741. https://doi.org/10.3390/nu14224741
APA StyleZhang, R., Yang, Q., Tang, Q., Xi, Y., Lin, Q., & Yang, L. (2022). Is Adolescents’ Free Sugar Intake Associated with the Free Sugar Intake of Their Parents? Nutrients, 14(22), 4741. https://doi.org/10.3390/nu14224741