
What Do People Know about Food, Nutrition and Health?—General Nutrition Knowledge in the Austrian Population


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Questionnaire
2.3. Data Analysis
3. Results
3.1. Nutrition Knowledge of the General Population
3.1.1. Selected Results for Single Questions in the General Population
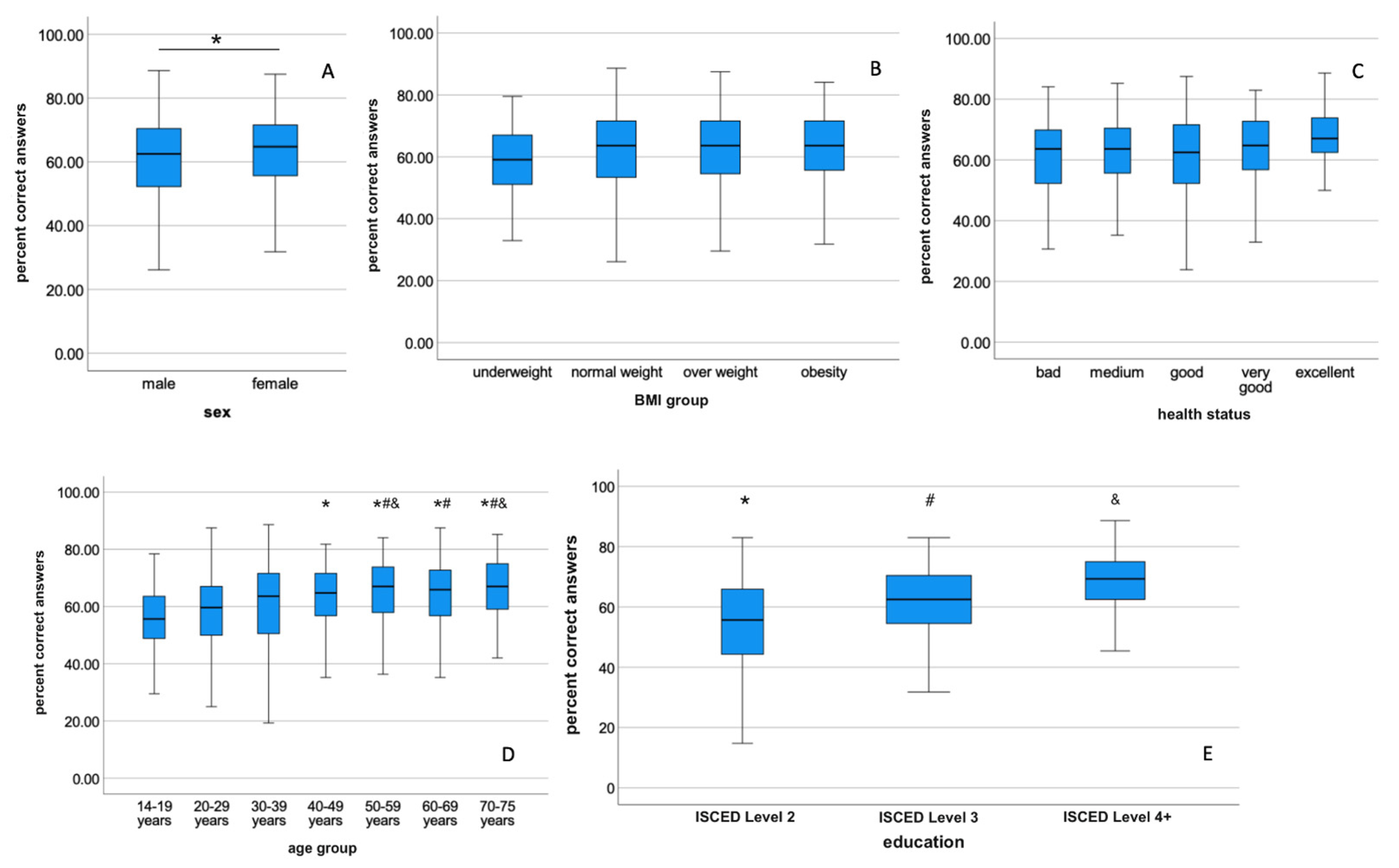
3.1.2. Factors of Influence on Nutrition Knowledge of the General Population
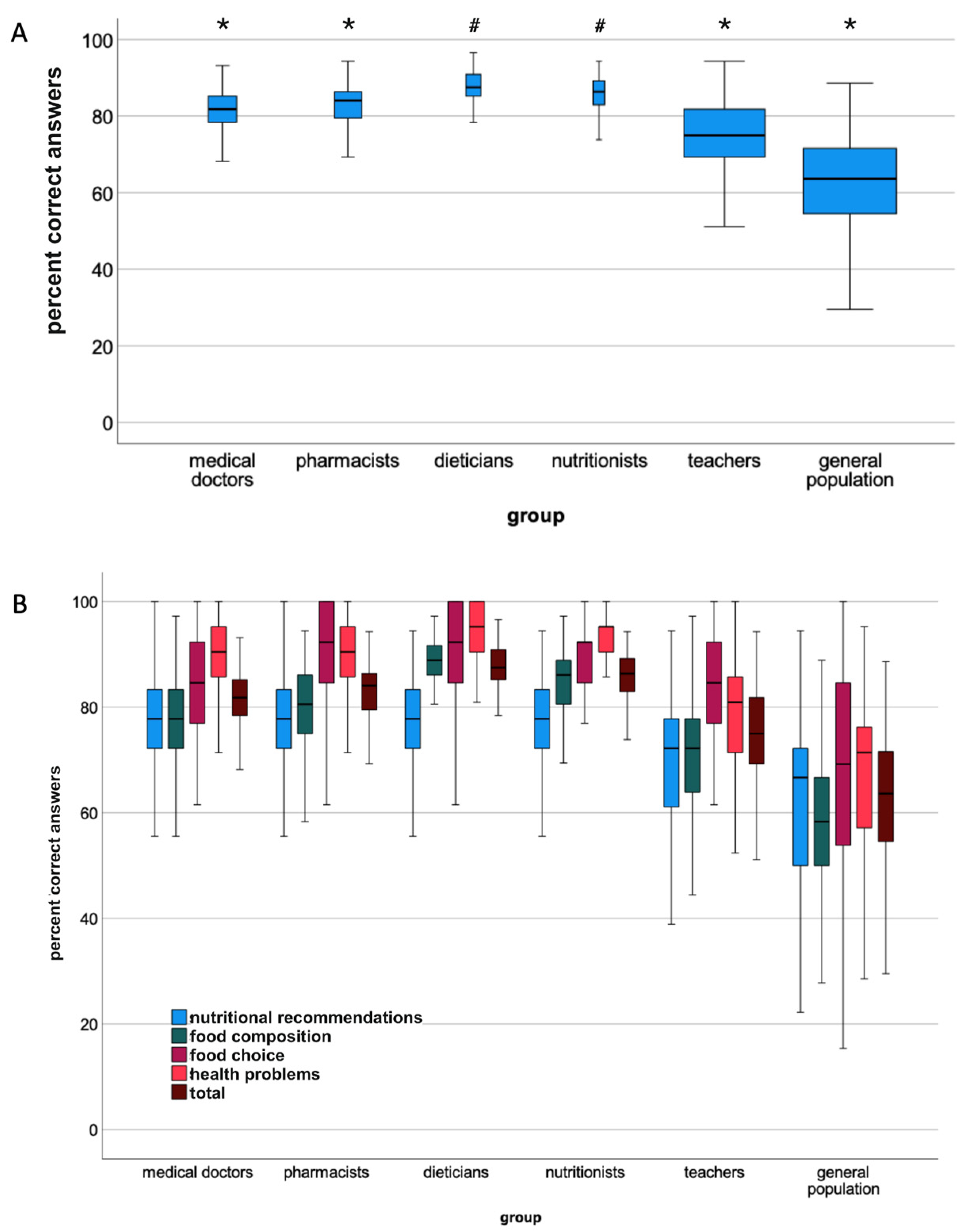
3.2. Nutritional Knowledge of Health Professionals and School Teachers
Health Status
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Diet, nutrition and the prevention of chronic diseases. World Health Organ. Tech. Rep. Ser. 2003, 916, 1–149. [Google Scholar]
- Rust, P.; Hasenegger, V.; König, J. Österreichischer Ernährungsbericht 2017; Bundesministerium für Gesundheit und Frauen: Vienna, Austria, 2017. [Google Scholar]
- Statistik Austria. Todeszrsachen. Available online: https://www.statistik.at/statistiken/bevoelkerung-und-soziales/bevoelkerung/gestorbene/todesursachen (accessed on 24 August 2022).
- Haghighian Roudsari, A.; Vedadhir, A.; Amiri, P.; Kalantari, N.; Omidvar, N.; Eini-Zinab, H.; Hani Sadati, S.M. Psycho-Socio-Cultural Determinants of Food Choice: A Qualitative Study on Adults in Social and Cultural Context of Iran. Iran. J. Psychiatry 2017, 12, 241–250. [Google Scholar] [PubMed]
- Leng, G.; Adan, R.A.H.; Belot, M.; Brunstrom, J.M.; de Graaf, K.; Dickson, S.L.; Hare, T.; Maier, S.; Menzies, J.; Preissl, H.; et al. The determinants of food choice. Proc. Nutr. Soc. 2017, 76, 316–327. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Mistretta, A.; Turconi, G.; Cena, H.; Roggi, C.; Galvano, F. Nutrition knowledge and other determinants of food intake and lifestyle habits in children and young adolescents living in a rural area of Sicily, South Italy. Public Health Nutr. 2013, 16, 1827–1836. [Google Scholar] [CrossRef]
- Worsley, A. Nutrition knowledge and food consumption: Can nutrition knowledge change food behaviour? Asia Pac. J. Clin. Nutr. 2002, 11, S579–S585. [Google Scholar] [CrossRef]
- Parmenter, K.; Waller, J.; Wardle, J. Demographic variation in nutrition knowledge in England. Health Educ. Res. 2000, 15, 163–174. [Google Scholar] [CrossRef]
- Pillai, K.G.; Liang, Y.S.; Thwaites, D.; Sharma, P.; Goldsmith, R. Regulatory focus, nutrition involvement, and nutrition knowledge. Appetite 2019, 137, 267–273. [Google Scholar] [CrossRef]
- Yahia, N.; Brown, C.A.; Rapley, M.; Chung, M. Level of nutrition knowledge and its association with fat consumption among college students. BMC Public Health 2016, 16, 1047. [Google Scholar] [CrossRef]
- Cavelaars, A.E.; Kunst, A.E.; Geurts, J.J.; Crialesi, R.; Grotvedt, L.; Helmert, U.; Lahelma, E.; Lundberg, O.; Matheson, J.; Mielck, A.; et al. Educational differences in smoking: International comparison. BMJ 2000, 320, 1102–1107. [Google Scholar] [CrossRef]
- Kari, J.T.; Viinikainen, J.; Bockerman, P.; Tammelin, T.H.; Pitkanen, N.; Lehtimaki, T.; Pahkala, K.; Hirvensalo, M.; Raitakari, O.T.; Pehkonen, J. Education leads to a more physically active lifestyle: Evidence based on Mendelian randomization. Scand. J. Med. Sci. Sports 2020, 30, 1194–1204. [Google Scholar] [CrossRef]
- Tracey, M.L.; Fitzgerald, S.; Geaney, F.; Perry, I.J.; Greiner, B. Socioeconomic inequalities of cardiovascular risk factors among manufacturing employees in the Republic of Ireland: A cross-sectional study. Prev. Med. Rep. 2015, 2, 699–703. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Belogianni, K.; Ooms, A.; Lykou, A.; Moir, H.J. Nutrition knowledge among university students in the UK: A cross-sectional study. Public Health Nutrition 2022, 25, 2834–2841. [Google Scholar] [CrossRef] [PubMed]
- Grunert, K.G.; Wills, J.; Celemin, L.F.; Lahteenmaki, L.; Scholderer, J.; Bonsmann, S.S.G. Socio-demographic and attitudinal determinants of nutrition knowledge of food shoppers in six European countries. Food Qual. Prefer. 2012, 26, 166–177. [Google Scholar] [CrossRef]
- Parmenter, K.; Wardle, J. Development of a general nutrition knowledge questionnaire for adults. Eur. J. Clin. Nutr. 1999, 53, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.; Vidgen, H.A.; Gallegos, D.; Hannan-Jones, M. Validation of a revised General Nutrition Knowledge Questionnaire for Australia. Public Health Nutr. 2021, 24, 1608–1618. [Google Scholar] [CrossRef]
- Kliemann, N.; Wardle, J.; Johnson, F.; Croker, H. Reliability and validity of a revised version of the General Nutrition Knowledge Questionnaire. Eur. J. Clin. Nutr. 2016, 70, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Alkhaldy, A.; Alshehri, B.; Albalawi, N.; Alsaady, F.; Alfarshooti, R.; Jamal, W.; Altaf, A.; Maghrabi, A.A. General and Postbariatric Nutritional Knowledge among Patients Undergoing Bariatric Surgery. J. Nutr. Metab. 2019, 2019, 6549476. [Google Scholar] [CrossRef] [PubMed]
- Bataineh, M.F.; Attlee, A. Reliability and validity of Arabic version of revised general nutrition knowledge questionnaire on university students. Public Health Nutr. 2021, 24, 851–860. [Google Scholar] [CrossRef]
- de Ellery, T.H.P. Adaptação Transcultural e Avaliação Psicométrica da Versão Brasileira do General Nutrition Knowledge Questionnaire-Revised. Ph.D. Thesis, University of São Paulo, São Paulo, Brazil, 2019. [Google Scholar]
- Husain, W.; Ashkanani, F.; Al Dwairji, M.A. Nutrition Knowledge among College of Basic Education Students in Kuwait: A Cross-Sectional Study. J. Nutr. Metab. 2021, 2021, 5560714. [Google Scholar] [CrossRef]
- Putnoky, S.; Banu, A.M.; Moleriu, L.C.; Putnoky, S.; Serban, D.M.; Niculescu, M.D.; Serban, C.L. Reliability and validity of a General Nutrition Knowledge Questionnaire for adults in a Romanian population. Eur. J. Clin. Nutr. 2020, 74, 1576–1584. [Google Scholar] [CrossRef]
- Teasdale, S.B.; Burrows, T.L.; Hayes, T.; Hsia, C.Y.; Watkins, A.; Curtis, J.; Ward, P.B. Dietary intake, food addiction and nutrition knowledge in young people with mental illness. Nutr. Diet. 2020, 77, 315–322. [Google Scholar] [CrossRef]
- Vidgen, H.A.; Gallegos, D. Defining food literacy and its components. Appetite 2014, 76, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Truman, E.; Lane, D.; Elliott, C. Defining food literacy: A scoping review. Appetite 2017, 116, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Parmenter, K.; Waller, J. Nutrition knowledge and food intake. Appetite 2000, 34, 269–275. [Google Scholar] [CrossRef] [PubMed]
- De Vriendt, T.; Matthys, C.; Verbeke, W.; Pynaert, I.; De Henauw, S. Determinants of nutrition knowledge in young and middle-aged Belgian women and the association with their dietary behaviour. Appetite 2009, 52, 788–792. [Google Scholar] [CrossRef] [PubMed]
- Contento, I.R. Nutrition education: Linking research, theory, and practice. Asia Pac. J. Clin. Nutr. 2008, 17 (Suppl. 1), 176–179. [Google Scholar]
- Kolpatzik, K.; Zaunbrecher, R. Ernährungskompetenz in Deutschland; KomPart: Berlin, Germany, 2020. [Google Scholar]
- Balani, R.; Herrington, H.; Bryant, E.; Lucas, C.; Kim, S.C. Nutrition knowledge, attitudes, and self-regulation as predictors of overweight and obesity. J. Am. Assoc. Nurse Pract. 2019, 31, 502–510. [Google Scholar] [CrossRef]
- Van Horn, L.; Lenders, C.M.; Pratt, C.A.; Beech, B.; Carney, P.A.; Dietz, W.; DiMaria-Ghalili, R.; Harlan, T.; Hash, R.; Kohlmeier, M.; et al. Advancing Nutrition Education, Training, and Research for Medical Students, Residents, Fellows, Attending Physicians, and Other Clinicians: Building Competencies and Interdisciplinary Coordination. Adv. Nutr. 2019, 10, 1181–1200. [Google Scholar] [CrossRef]
- Hendrie, G.A.; Cox, D.N.; Coveney, J. Validation of the general nutrition knowledge questionnaire in an Australian community sample. Nutr. Diet. 2008, 65, 72–77. [Google Scholar] [CrossRef]
- Cotton, W.; Dudley, D.; Peralta, L.; Werkhoven, T. The effect of teacher-delivered nutrition education programs on elementary-aged students: An updated systematic review and meta-analysis. Prev. Med. Rep. 2020, 20, 101178. [Google Scholar] [CrossRef]
- University of Vienna. Studierende und Studienzulassungen nach Studienprogrammleitung und Studienrichtung. Available online: https://studieren.univie.ac.at/fileadmin/user_upload/p_studieren/Studienwahl-Angebot/Statistiken/STUDSTAT_72_2019W.pdf (accessed on 7 September 2022).
- NÖ Forschungs-und Bildungsges.m.b.H. (NFB). Hoschschulstatistik NÖ. Available online: https://www.martschin.com/wp-content/uploads/2018/06/Hochschulstatistik_NÖ_NFB_Broschuere.pdf (accessed on 7 September 2022).
- Österreichische Apothekerkammer. Apotheke in Zahlen. Available online: https://www.apothekerkammer.at/fileadmin/Kommunikation/ApothekeinZahlen2020.pdf (accessed on 7 September 2022).
- Bundesministerium für Bildung und Forschung. Lehrer/innen—Österreich 2018/19. Available online: https://www.bmbwf.gv.at/Themen/schule/schulsystem/gd/lehrstat_oester.html (accessed on 7 September 2022).
- Österreichische Ärztekammer. Ärztestatistik für Österreich. Available online: https://www.aerztekammer.at/documents/261766/986618/ÖÄK_Ärztestatistik_2020.pdf/8d3a4002-2ba2-4e44-6550-6cf190e0fb6b (accessed on 7 September 2022).




{kind=link}
{kind=link}
{kind=link}
| Study Group | General Population | Health Professionals | School Teachers | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Medical Doctors | Pharmacists | Dieticians | Nutritionists | |||||||||||||||
| total | m | f | total | m | f | total | m | f | total | m | f | total | m | f | total | m | f | |
| n | 1000 | 502 | 498 | 307 | 78 | 227 | 295 | 44 | 251 | 160 | 4 | 156 | 124 | 22 | 102 | 873 | 137 | 735 |
| Age group | ||||||||||||||||||
| 14–19 | 77 | 39 | 38 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 20–29 | 162 | 83 | 79 | 21 | 5 | 15 | 39 | 4 | 35 | 69 | 1 | 68 | 93 | 19 | 74 | 113 | 13 | 100 |
| 30–39 | 176 | 89 | 87 | 58 | 11 | 47 | 110 | 18 | 92 | 44 | 0 | 44 | 23 | 2 | 21 | 160 | 17 | 143 |
| 40–49 | 166 | 86 | 80 | 85 | 16 | 69 | 68 | 9 | 59 | 27 | 2 | 25 | 6 | 1 | 5 | 207 | 32 | 175 |
| 50–59 | 201 | 101 | 100 | 77 | 15 | 62 | 60 | 8 | 52 | 20 | 1 | 19 | 2 | 0 | 2 | 321 | 58 | 262 |
| 60–69 | 148 | 71 | 77 | 58 | 27 | 31 | 15 | 3 | 12 | 0 | 0 | 0 | 0 | 0 | 0 | 72 | 17 | 55 |
| 70–75 | 70 | 33 | 37 | 4 | 2 | 2 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| >75 | 0 | 0 | 0 | 4 | 2 | 2 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| BMI group | ||||||||||||||||||
| <18.5 | 34 | 10 | 24 | 9 | 0 | 9 | 18 | 0 | 18 | 6 | 0 | 6 | 7 | 0 | 7 | 16 | 0 | 16 |
| 18.5–24.9 | 425 | 190 | 235 | 219 | 47 | 172 | 213 | 24 | 189 | 128 | 0 | 128 | 104 | 19 | 85 | 548 | 63 | 485 |
| 25.0–29.9 | 323 | 193 | 130 | 54 | 20 | 34 | 52 | 19 | 33 | 21 | 4 | 17 | 11 | 2 | 9 | 222 | 58 | 164 |
| ≥30.0 | 217 | 109 | 108 | 25 | 11 | 14 | 12 | 1 | 11 | 5 | 0 | 5 | 2 | 1 | 1 | 87 | 16 | 71 |
| Subjective health status | ||||||||||||||||||
| Poor | 44 | 20 | 24 | 3 | 2 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 9 | 2 | 7 |
| Fair | 252 | 129 | 123 | 33 | 12 | 21 | 13 | 1 | 12 | 8 | 0 | 8 | 11 | 2 | 9 | 86 | 18 | 68 |
| Good | 453 | 217 | 236 | 107 | 23 | 84 | 84 | 14 | 70 | 42 | 1 | 41 | 29 | 6 | 23 | 358 | 52 | 306 |
| Very good | 216 | 115 | 101 | 125 | 29 | 96 | 159 | 24 | 135 | 86 | 3 | 83 | 61 | 12 | 49 | 335 | 50 | 285 |
| Excellent | 35 | 21 | 14 | 39 | 12 | 27 | 39 | 5 | 34 | 24 | 0 | 24 | 23 | 2 | 21 | 85 | 15 | 70 |
| Subsample | Section 1 (Nutritional Recommendations) | Section 2 (Food Composition) | Section 3 (Food Choice) | Section 4 (Health Problems) | Total Score | |
|---|---|---|---|---|---|---|
| Medical Doctors (n = 307) | M | 75.73 | 78.05 | 86.32 | 88.49 | 81.29 |
| Md | 77.78 | 77.78 | 84.62 | 90.48 | 81.82 | |
| SD | 10.45 | 8.04 | 10.54 | 7.33 | 5.65 | |
| Min | 38.89 | 50.00 | 53.85 | 57.14 | 60.23 | |
| Max | 100.00 | 97.22 | 100.00 | 100.00 | 93.18 | |
| Pharmacists (n = 295) | M | 76.53 | 80.45 | 89.93 | 88.28 | 82.92 |
| Md | 77.78 | 80.56 | 92.31 | 90.48 | 84.09 | |
| SD | 9.95 | 8.06 | 8.73 | 7.23 | 5.38 | |
| Min | 38.89 | 41.67 | 61.54 | 57.14 | 64.77 | |
| Max | 100.00 | 94.44 | 100.00 | 100.00 | 94.32 | |
| Dieticians (n = 160) | M | 75.28 | 88.33 | 90.91 | 94.55 | 87.53 |
| Md | 77.78 | 88.89 | 92.31 | 95.24 | 87.50 | |
| SD | 10.98 | 5.41 | 8.66 | 4.71 | 3.72 | |
| Min | 33.33 | 72.22 | 61.54 | 80.95 | 78.41 | |
| Max | 94.44 | 100.00 | 100.00 | 100.00 | 96.59 | |
| Nutritionists (n =124) | M | 77.96 | 84.25 | 88.77 | 92.36 | 85.57 |
| Md | 77.78 | 86.11 | 92.31 | 95.24 | 86.36 | |
| SD | 9.21 | 8.38 | 10.63 | 7.23 | 6.29 | |
| Min | 44.44 | 36.11 | 46.15 | 42.86 | 40.91 | |
| Max | 94.44 | 97.22 | 100.00 | 100.00 | 94.32 | |
| School teachers (n = 873) | M | 70.71 | 70.66 | 83.19 | 78.99 | 74.51 |
| Md | 72.22 | 72.22 | 84.62 | 80.95 | 75.00 | |
| SD | 13.04 | 11.49 | 12.99 | 12.75 | 9.51 | |
| Min | 11.11 | 8.33 | 0.00 | 0.00 | 9.09 | |
| Max | 94.44 | 97.22 | 100.00 | 100.00 | 94.32 | |
| General population (n = 1000) | M | 61.12 | 57.42 | 65.38 | 66.04 | 61.41 |
| Md | 66.67 | 58.33 | 69.23 | 71.43 | 63.64 | |
| SD | 16.97 | 15.10 | 21.21 | 16.87 | 14.11 | |
| Min | 0.00 | 0.00 | 7.69 | 4.76 | 2.27 | |
| Max | 94.44 | 88.89 | 100.00 | 95.24 | 88.64 | |
| Analysis of Covariance with age and sex as covariants | F (5;2750) = 108.934 p < 0.001 | F (5;2750) = 361.568 p < 0.001 | F (5;2750) = 197.777 p < 0.001 | F (5;2750) = 307.705 p < 0.001 | F (5;2750) = 392.103 p < 0.001 | |
| Bonferroni-corrected post-hoc analysis. p < 0.05 | Nutritionists > dieticians = pharmacists = medical doctors > school teachers > general population | Dieticians > nutritionists > pharmacists > medical doctors > school teachers > general population | Dieticians = pharmacists = Nutritionists > medical doctors > school teachers > general population | Dieticians = nutritionists > pharmacists = medical doctors > school teachers > general population | Dieticians = nutritionists > pharmacists > medical doctors > school teachers > general population |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gruber, M.; Iwuchukwu, C.G.; Sperr, E.; König, J. What Do People Know about Food, Nutrition and Health?—General Nutrition Knowledge in the Austrian Population. Nutrients 2022, 14, 4729. https://doi.org/10.3390/nu14224729
Gruber M, Iwuchukwu CG, Sperr E, König J. What Do People Know about Food, Nutrition and Health?—General Nutrition Knowledge in the Austrian Population. Nutrients. 2022; 14(22):4729. https://doi.org/10.3390/nu14224729
Chicago/Turabian StyleGruber, Marlies, Chinyere Gina Iwuchukwu, Elisabeth Sperr, and Jürgen König. 2022. "What Do People Know about Food, Nutrition and Health?—General Nutrition Knowledge in the Austrian Population" Nutrients 14, no. 22: 4729. https://doi.org/10.3390/nu14224729
APA StyleGruber, M., Iwuchukwu, C. G., Sperr, E., & König, J. (2022). What Do People Know about Food, Nutrition and Health?—General Nutrition Knowledge in the Austrian Population. Nutrients, 14(22), 4729. https://doi.org/10.3390/nu14224729