

Relationship between Maternal Vitamin D Levels and Adverse Outcomes
 ,
,
Abstract
1. Introduction
2. Maternal Vitamin D Status and Adverse Pregnancy Outcomes
2.1. Gestational Diabetes Mellitus (GDM)
2.2. Pregnancy-Induced Hypertension
2.3. Spontaneous Abortion and Stillbirth
2.4. Preterm Birth (PTB)
2.5. Intrauterine Growth Restriction
3. Potential Mechanisms of Maternal VD Status during Pregnancy and Adverse Pregnancy
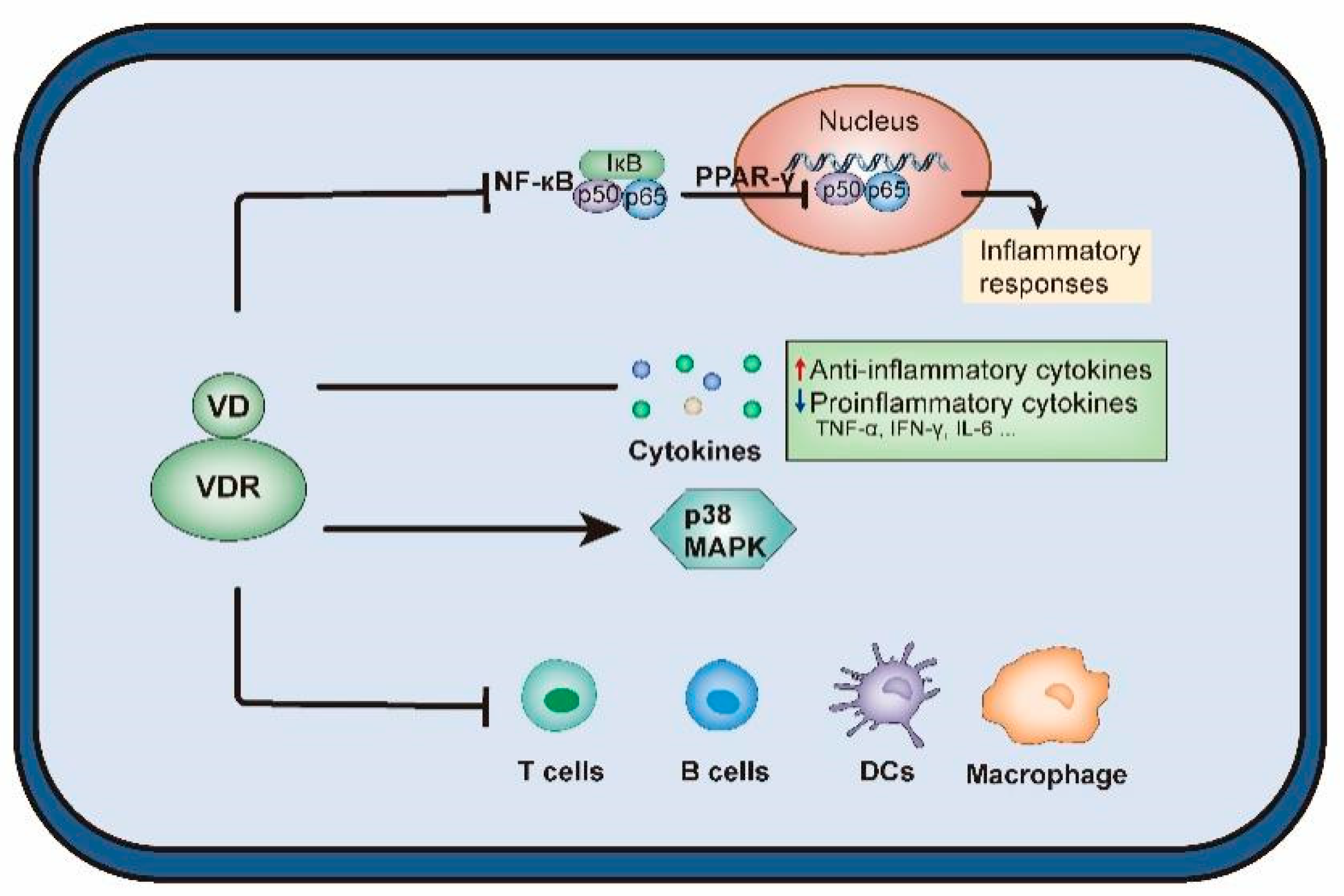
3.1. Regulation of Cytokine Pathways
3.2. Regulation of Immune System Processing
3.3. Regulation of Internal Secretion
3.4. Regulation of Placental Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Sizar, O.; Khare, S.; Goyal, A.; Bansal, P.; Givler, A. Vitamin D Deficiency. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Cashman, K.D. Vitamin D deficiency: Defining, prevalence, causes, and strategies of addressing. Calcif. Tissue Int. 2020, 106, 14–29. [Google Scholar] [CrossRef]
- Manaseki-Holland, S.; Maroof, Z.; Bruce, J.; Mughal, M.Z.; Masher, M.I.; A Bhutta, Z.; Walraven, G.; Chandramohan, D. Effect on the incidence of pneumonia of vitamin D supplementation by quarterly bolus dose to infants in Kabul: A randomised controlled superiority trial. Lancet 2012, 379, 1419–1427. [Google Scholar] [CrossRef]
- Denburg, M.R.; Hoofnagle, A.N.; Sayed, S.; Gupta, J.; de Boer, I.H.; Appel, L.J.; Durazo-Arvizu, R.; Whitehead, K.; I Feldman, H.; Leonard, M.B.; et al. Comparison of Two ELISA Methods and Mass Spectrometry for Measurement of Vitamin D-Binding Protein: Implications for the Assessment of Bioavailable Vitamin D Concentrations Across Genotypes. J. Bone Miner. Res. 2017, 31, 1128–1136. [Google Scholar] [CrossRef]
- Lontchi-Yimagou, E.; Kang, S.; Goyal, A.; Zhang, K.; You, J.Y.; Carey, M.; Jain, S.; Bhansali, S.; Kehlenbrink, S.; Guo, P.; et al. Insulin-sensitizing effects of vitamin D repletion mediated by adipocyte vitamin D receptor: Studies in humans and mice. Mol. Metab. 2020, 42, 101095. [Google Scholar] [CrossRef]
- Mulligan, M.L.; Felton, S.K.; Riek, A.E.; Bernal-Mizrachi, C. Implications of vitamin D deficiency in pregnancy and lactation. Am. J. Obstet. Gynecol. 2010, 202, 429.e421–429.e429. [Google Scholar] [CrossRef]
- Woon, F.C.; Chin, Y.S.; Ismail, I.H.; Batterham, M.; Latiff, A.H.A.; Gan, W.Y.; Appannah, G.; Hussien, S.H.M.; Edi, M.; Tan, M.L.; et al. Vitamin D deficiency during pregnancy and its associated factors among third trimester Malaysian pregnant women. PLoS ONE 2019, 14, e0216439. [Google Scholar] [CrossRef]
- Aji, A.S.; Yerizel, E.; Lipoeto, N.I. The association between lifestyle and maternal vitamin D during pregnancy in West Sumatra, Indonesia. Asia Pac. J. Clin. Nutr. 2018, 27, 1286–1293. [Google Scholar]
- Hanieh, S.; Ha, T.T.; Simpson, J.A.; Thuy, T.T.; Khuong, N.C.; Thoang, D.D.; Tran, T.; Tuan, T.; Fisher, J.; Biggs, B.-A. Maternal Vitamin D Status and Infant Outcomes in Rural Vietnam: A Prospective Cohort Study. PLoS ONE 2014, 9, e99005. [Google Scholar] [CrossRef]
- Pratumvinit, B.; Wongkrajang, P.; Wataganara, T.; Hanyongyuth, S.; Nimmannit, A.; Chatsiricharoenkul, S.; Manonukul, K.; Reesukumal, K. Maternal Vitamin D Status and Its Related Factors in Pregnant Women in Bangkok, Thailand. PLoS ONE 2015, 10, e0131126. [Google Scholar] [CrossRef]
- Chen, Y.-H.; Fu, L.; Hao, J.-H.; Wang, H.; Zhang, C.; Tao, F.-B.; Xu, D.-X. Influent factors of gestational vitamin D deficiency and its relation to an increased risk of preterm delivery in Chinese population. Sci. Rep. 2018, 8, 3608. [Google Scholar] [CrossRef]
- Halicioglu, O.; Aksit, S.; Koc, F.; Akman, S.A.; Albudak, E.; Yaprak, I.; Coker, I.; Colak, A.; Ozturk, C.; Gulec, E.S. Vitamin D deficiency in pregnant women and their neonates in spring time in western Turkey. Paediatr. Périnat. Epidemiol. 2012, 26, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Marwaha, R.K.; Tandon, N.; Chopra, S.; Agarwal, N.; Garg, M.K.; Sharma, B.; Kanwar, R.S.; Bhadra, K.; Singh, S.; Mani, K.; et al. Vitamin D status in pregnant Indian women across trimesters and different seasons and its correlation with neonatal serum 25-hydroxyvitamin D levels. Br. J. Nutr. 2011, 106, 1383–1389. [Google Scholar] [CrossRef]
- Maghbooli, Z.; Hossein-Nezhad, A.; Shafaei, A.R.; Karimi, F.; Madani, F.S.; Larijani, B. Vitamin D status in mothers and their newborns in Iran. BMC Pregnancy Childbirth 2007, 7, 1. [Google Scholar] [CrossRef]
- Ginde, A.A.; Sullivan, A.F.; Mansbach, J.M.; Camargo, C.A. Vitamin D insufficiency in pregnant and nonpregnant women of childbearing age in the United States. Am. J. Obstet. Gynecol. 2010, 202, 436. [Google Scholar] [CrossRef] [PubMed]
- Brembeck, P.; Winkvist, A.; Olausson, H. Determinants of vitamin D status in pregnant fair-skinned women in Sweden. Br. J. Nutr. 2013, 110, 856–864. [Google Scholar] [CrossRef] [PubMed]
- Nicolaidou, P.; Hatzistamatiou, Z.; Papadopoulou, A.; Kaleyias, J.; Floropoulou, E.; Lagona, E.; Tsagris, V.; Costalos, C.; Antsaklis, A. Low Vitamin D Status in Mother-Newborn Pairs in Greece. Calcif. Tissue Res. 2006, 78, 337–342. [Google Scholar] [CrossRef]
- Bowyer, L.; Catling-Paull, C.; Diamond, T.; Homer, C.; Davis, G.; Craig, M.E. Vitamin D, PTH and calcium levels in pregnant women and their neonates. Clin. Endocrinol. 2009, 70, 373–377. [Google Scholar] [CrossRef]
- Pereira-Santos, M.; Carvalho, G.Q.; Couto, R.D.; dos Santos, D.B.; Oliveira, A.M. Vitamin D deficiency and associated factors among pregnant women of a sunny city in Northeast of Brazil. Clin. Nutr. ESPEN 2018, 23, 240–244. [Google Scholar] [CrossRef]
- Toko, E.N.; Sumba, O.P.; Daud, I.I.; Ogolla, S.; Majiwa, M.; Krisher, J.T.; Ouma, C.; Dent, A.E.; Rochford, R.; Mehta, S. Maternal Vitamin D Status and Adverse Birth Outcomes in Children from Rural Western Kenya. Nutrients 2016, 8, 794. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.-X.; Pan, G.-T.; Guo, J.-F.; Li, B.-Y.; Qin, L.-Q.; Zhang, Z.-L. Vitamin D Deficiency Increases the Risk of Gestational Diabetes Mellitus: A Meta-Analysis of Observational Studies. Nutrients 2015, 7, 8366–8375. [Google Scholar] [CrossRef] [PubMed]
- Shibata, M.; Suzuki, A.; Sekiya, T.; Sekiguchi, S.; Asano, S.; Udagawa, Y.; Itoh, M. High prevalence of hypovitaminosis D in pregnant Japanese women with threatened premature delivery. J. Bone Miner. Metab. 2011, 29, 615–620. [Google Scholar] [CrossRef]
- Scholl, T.O.; Chen, X.; Stein, P. Maternal vitamin D status and delivery by cesarean. Nutrients 2012, 4, 319–330. [Google Scholar] [CrossRef]
- Bodnar, L.M.; Platt, R.W.; Simhan, H.N. Early-pregnancy vitamin D deficiency and risk of preterm birth subtypes. Obs. Gynecol 2015, 125, 439–447. [Google Scholar] [CrossRef]
- Pirdehghan, A.; Vakili, M.; Dehghan, R.; Zare, F. High Prevalence of Vitamin D Deficiency and Adverse Pregnancy Outcomes in Yazd, a Central Province of Iran. J. Reprod. Infertil. 2016, 17, 34–38. [Google Scholar] [PubMed]
- Pérez-López, F.R.; Pasupuleti, V.; Mezones-Holguin, E.; Benites-Zapata, V.A.; Thota, P.; Deshpande, A.; Hernandez, A.V. Effect of vitamin D supplementation during pregnancy on maternal and neonatal outcomes: A systematic review and meta-analysis of randomized controlled trials. Fertil. Steril. 2015, 103, 1278–1288. [Google Scholar] [CrossRef] [PubMed]
- Do, H.J.; Park, J.S.; Seo, J.-H.; Lee, E.S.; Park, C.-H.; Woo, H.-O.; Youn, H.-S. Neonatal Late-onset Hypocalcemia: Is There Any Relationship with Maternal Hypovitaminosis D? Pediatr. Gastroenterol. Hepatol. Nutr. 2014, 17, 47–51. [Google Scholar] [CrossRef]
- Damm, P.; Houshmand-Oeregaard, A.; Kelstrup, L.; Lauenborg, J.; Mathiesen, E.; Clausen, T.D. Gestational diabetes mellitus and long-term consequences for mother and offspring: A view from Denmark. Diabetologia 2016, 59, 1396–1399. [Google Scholar] [CrossRef]
- Olmos-Ortiz, A.; Avila, E.; Durand-Carbajal, M.; Díaz, L. Regulation of calcitriol biosynthesis and activity: Focus on gestational vitamin D deficiency and adverse pregnancy outcomes. Nutrients 2015, 7, 443–480. [Google Scholar] [CrossRef]
- Triunfo, S.; Lanzone, A.; Lindqvist, P. Low maternal circulating levels of vitamin D as potential determinant in the development of gestational diabetes mellitus. J. Endocrinol. Investig. 2017, 40, 1049–1059. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.; Xu, Y.; Lv, L.; Zhang, M. Association between vitamin D status and the risk of gestational diabetes mellitus: A meta-analysis. Arch. Gynecol. Obstet. 2016, 293, 959–966. [Google Scholar] [CrossRef]
- Yin, W.-J.; Tao, R.-X.; Hu, H.-L.; Zhang, Y.; Jiang, X.-M.; Zhang, M.-X.; Jin, D.; Yao, M.-N.; Tao, F.-B.; Zhu, P. The association of vitamin D status and supplementation during pregnancy with gestational diabetes mellitus: A Chinese prospective birth cohort study. Am. J. Clin. Nutr. 2020, 111, 122–130. [Google Scholar] [CrossRef]
- Yue, X.; Zhan, F.; Zhang, Q. Infuence of vitamin D on blood glucose and pregnancy outcome in normal body mass index patients with gestational diabetes mellitus. China Mod. Med. Chin. Mod. Med. 2019, 26, 99–102. [Google Scholar]
- Tabatabaei, N.; Rodd, C.J.; Kremer, R.; Weiler, H.A. High Vitamin D Status before Conception, but Not during Pregnancy, Is Inversely Associated with Maternal Gestational Diabetes Mellitus in Guinea Pigs. J. Nutr. 2014, 144, 1994–2001. [Google Scholar] [CrossRef] [PubMed]
- Pittas, A.G.; Dawson-Hughes, B. Vitamin D and diabetes. J. Steroid Biochem. Mol. Biol. 2010, 121, 425–429. [Google Scholar] [CrossRef]
- Sergeev, I.N.; Rhoten, W.B. 1,25-Dihydroxyvitamin D3 evokes oscillations of intracellular calcium in a pancreatic beta-cell line. Endocrinology 1995, 136, 2852–2861. [Google Scholar] [CrossRef]
- Jurutka, P.W.; Bartik, L.; Whitfield, G.K.; Mathern, D.R.; Barthel, T.K.; Gurevich, M.; Hsieh, J.-C.; Kaczmarska, M.; Haussler, C.A.; Haussler, M.R. Vitamin D Receptor: Key Roles in Bone Mineral Pathophysiology, Molecular Mechanism of Action, and Novel Nutritional Ligands. J. Bone Miner. Res. 2007, 22, V2–V10. [Google Scholar] [CrossRef]
- Ramos-Lopez, E.; Kahles, H.; Weber, S.; Kukic, A.; Penna-Martinez, M.; Badenhoop, K.; Louwen, F. Gestational diabetes mellitus and vitamin D deficiency: Genetic contribution of CYP27B1 and CYP2R1 polymorphisms. Diabetes, Obes. Metab. 2008, 10, 683–685. [Google Scholar] [CrossRef]
- World Health Organization. WHO Recommendations for Prevention and Treatment of Pre-Eclampsia and Eclampsia; World Health Organization: Geneva, Switzerland, 2011; Available online: https://apps.who.int/iris/bitstream/handle/10665/44703/?sequence=1 (accessed on 10 August 2022).
- Kintiraki, E.; Papakatsika, S.; Kotronis, G.; Goulis, D.G.; Kotsis, V. Pregnancy-Induced hypertension. Hormones (Athens Greece) 2015, 14, 211–223. [Google Scholar] [CrossRef]
- Guljit Kaur, S.P.; Preet, I. Prevalence of vitamin D deficiency in patients of pregnancy induced hypertension. Int. J. Reprod. Contracept. Obstet. Gynecol. 2018, 7, 3358–3362. [Google Scholar] [CrossRef]
- Alrb, M.T.G.; Hassan, M.M.; El-Den, H.A.B.; Ali, A.M.B.A.E. Vitamin D Level in Patients Suffering from Pregnancy Induced Hypertension. Minia J. Med. Res. 2019, 30, 42–45. [Google Scholar] [CrossRef]
- Osman, O.M.; Gaafar, T.; Eissa, T.S.; Abdella, R.; Ebrashy, A.; Ellithy, A. Prevalence of vitamin D deficiency in Egyptian patients with pregnancy-induced hypertension. J. Périnat. Med. 2020, 48, 583–588. [Google Scholar] [CrossRef]
- Díaz, L.; Arranz, C.; Avila, E.; Halhali, A.; Vilchis, F.; Larrea, F. Expression and Activity of 25-Hydroxyvitamin D-1?-Hydroxylase Are Restricted in Cultures of Human Syncytiotrophoblast Cells from Preeclamptic Pregnancies. J. Clin. Endocrinol. Metab. 2002, 87, 3876–3882. [Google Scholar] [CrossRef]
- Irani, R.A.; Xia, Y. Renin Angiotensin Signaling in Normal Pregnancy and Preeclampsia. Semin. Nephrol. 2011, 31, 47–58. [Google Scholar] [CrossRef]
- Dechend, R.; Gratze, P.; Wallukat, G.; Shagdarsuren, E.; Plehm, R.; Bräsen, J.-H.; Fiebeler, A.; Schneider, W.; Caluwaerts, S.; Vercruysse, L.; et al. Agonistic autoantibodies to the AT1 receptor in a transgenic rat model of preeclampsia. Hypertension 2005, 45, 742–746. [Google Scholar] [CrossRef] [PubMed]
- Shand, A.W.; Nassar, N.; Von Dadelszen, P.; Innis, S.M.; Green, T.J. Maternal vitamin D status in pregnancy and adverse pregnancy outcomes in a group at high risk for pre-eclampsia. BJOG Int. J. Obstet. Gynaecol. 2010, 117, 1593–1598. [Google Scholar] [CrossRef] [PubMed]
- Haugen, M.; Brantsæter, A.L.; Trogstad, L.; Alexander, J.; Roth, C.; Magnus, P.; Meltzer, H.M. Vitamin D Supplementation and Reduced Risk of Preeclampsia in Nulliparous Women. Epidemiology 2009, 20, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Robinson, C.J.; Alanis, M.C.; Wagner, C.L.; Hollis, B.W.; Johnson, D.D. Plasma 25-hydroxyvitamin D levels in early-onset severe preeclampsia. Am. J. Obstet. Gynecol. 2010, 203, 366.e1–366.e6. [Google Scholar] [CrossRef]
- Tabesh, M.; Salehi-Abargouei, A.; Tabesh, M.; Esmaillzadeh, A. Maternal Vitamin D Status and Risk of Pre-Eclampsia: A Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2013, 98, 3165–3173. [Google Scholar] [CrossRef]
- Christesen, H.T.; Falkenberg, T.; Lamont, R.F.; Jørgensen, J.S. The impact of vitamin D on pregnancy: A systematic review. Acta Obstet. Gynecol. Scand. 2012, 91, 1357–1367. [Google Scholar] [CrossRef]
- Aghajafari, F.; Nagulesapillai, T.; Ronksley, P.E.; Tough, S.C.; O’Beirne, M.; Rabi, D.M. Association between maternal serum 25-hydroxyvitamin D level and pregnancy and neonatal outcomes: Systematic review and meta-analysis of observational studies. Obstet. Anesth. Dig. 2014, 34, 115–116. [Google Scholar] [CrossRef]
- Mayrink, J.; Leite, D.F.; Nobrega, G.M.; Costa, M.L.; Cecatti, J.G. Prediction of pregnancy-related hypertensive disorders using metabolomics: A systematic review. BMJ Open 2022, 12, e054697. [Google Scholar] [CrossRef]
- Liu, N.Q.; Ouyang, Y.; Bulut, Y.; Lagishetty, V.; Chan, S.; Hollis, B.W.; Wagner, C.; Equils, O.; Hewison, M. Dietary Vitamin D Restriction in Pregnant Female Mice Is Associated With Maternal Hypertension and Altered Placental and Fetal Development. Endocrinology 2013, 154, 2270–2280. [Google Scholar] [CrossRef]
- Faulkner, J.L.; Cornelius, D.C.; Amaral, L.M.; Harmon, A.C.; Cunningham, M.W., Jr.; Darby, M.M.; Ibrahim, T.; Thomas, D.S.; Herse, F.; Wallukat, G.; et al. Vitamin D supplementation improves pathophysiology in a rat model of preeclampsia. Am. J. Physiol. Integr. Comp. Physiol. 2016, 310, R346–R354. [Google Scholar] [CrossRef]
- Al-Shaikh, G.K.; Ibrahim, G.H.; Fayed, A.A.; Al-Mandeel, H. Impact of vitamin D deficiency on maternal and birth outcomes in the Saudi population: A cross-sectional study. BMC Pregnancy Childbirth 2016, 16, 1–9. [Google Scholar] [CrossRef]
- Burris, H.H.; Rifas-Shiman, S.L.; Huh, S.Y.; Kleinman, K.; Litonjua, A.A.; Oken, E.; Rich-Edwards, J.W.; Camargo, C.A.; Gillman, M.W. Vitamin D status and hypertensive disorders in pregnancy. Ann. Epidemiol. 2014, 24, 399–403. [Google Scholar] [CrossRef]
- Bodnar, L.M.; Simhan, H.N.; Powers, R.W.; Frank, M.P.; Cooperstein, E.; Roberts, J.M. High Prevalence of Vitamin D Insufficiency in Black and White Pregnant Women Residing in the Northern United States and Their Neonates. J. Nutr. 2007, 137, 447–452. [Google Scholar] [CrossRef]
- Webb, A.R. Who, what, where and when—influences on cutaneous vitamin D synthesis. Prog. Biophys. Mol. Biol. 2006, 92, 17–25. [Google Scholar] [CrossRef]
- Bodnar, L.M.; Catov, J.M.; Simhan, H.N.; Holick, M.; Powers, R.W.; Roberts, J.M. Maternal Vitamin D Deficiency Increases the Risk of Preeclampsia. J. Clin. Endocrinol. Metab. 2007, 92, 3517–3522. [Google Scholar] [CrossRef]
- Lai, J.K.C.; Lucas, R.; Banks, E.; Ponsonby, A.-L. Ausimmune Investigator Group Variability in vitamin D assays impairs clinical assessment of vitamin D status. Intern. Med. J. 2012, 42, 43–50. [Google Scholar] [CrossRef]
- Roth, H.J.; Schmidt-Gayk, H.; Weber, H.; Niederau, C. Accuracy and clinical implications of seven 25-hydroxyvitamin D methods compared with liquid chromatography–tandem mass spectrometry as a reference. Ann. Clin. Biochem. Int. J. Lab. Med. 2008, 45, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.; McKenzie-McHarg, K.; Horsch, A. The impact of miscarriage and stillbirth on maternal–fetal relationships: An integrative review. J. Reprod. Infant Psychol. 2016, 35, 32–52. [Google Scholar] [CrossRef] [PubMed]
- Hou, W.; Yan, X.-T.; Bai, C.-M.; Zhang, X.-W.; Hui, L.-Y.; Yu, X.-W. Decreased serum vitamin D levels in early spontaneous pregnancy loss. Eur. J. Clin. Nutr. 2016, 70, 1004–1008. [Google Scholar] [CrossRef]
- Bärebring, L.; Bullarbo, M.; Glantz, A.; Hulthén, L.; Ellis, J.; Jagner, A.; Schoenmakers, I.; Winkvist, A.; Augustin, H. Trajectory of vitamin D status during pregnancy in relation to neonatal birth size and fetal survival: A prospective cohort study. BMC Pregnancy Childbirth 2018, 18, 1–7. [Google Scholar] [CrossRef]
- Andersen, L.B.; Jorgensen, J.S.; Jensen, T.K.; Dalgård, C.; Barington, T.; Nielsen, J.; Beck-Nielsen, S.S.; Husby, S.; Abrahamsen, B.; Lamont, R.F.; et al. Vitamin D insufficiency is associated with increased risk of first-trimester miscarriage in the Odense Child Cohort. Am. J. Clin. Nutr. 2015, 102, 633–638. [Google Scholar] [CrossRef]
- Zhou, J.; Su, L.; Liu, M.; Liu, Y.; Cao, X.; Wang, Z.; Xiao, H. Associations between 25-hydroxyvitamin D levels and pregnancy outcomes: A prospective observational study in southern China. Eur. J. Clin. Nutr. 2014, 68, 925–930. [Google Scholar] [CrossRef]
- Schneuer, F.; Roberts, C.L.; Guilbert, C.; Simpson, J.M.; Algert, C.; Khambalia, A.Z.; Tasevski, V.; Ashton, A.W.; Morris, J.M.; Nassar, N. Effects of maternal serum 25-hydroxyvitamin D concentrations in the first trimester on subsequent pregnancy outcomes in an Australian population. Am. J. Clin. Nutr. 2014, 99, 287–295. [Google Scholar] [CrossRef]
- Ghahfarokhi, M.S. Relationship between consanguineous marriage and spontaneous abortion and stillbirth. Payesh 2018, 17, 455–462. [Google Scholar]
- Magnus, M.C.; Hockey, R.L.; Håberg, S.E.; Mishra, G.D. Pre-pregnancy lifestyle characteristics and risk of miscarriage: The Australian Longitudinal Study on Women’s Health. BMC Pregnancy Childbirth 2022, 22, 1–10. [Google Scholar] [CrossRef]
- Ji, H.; Liang, H.; Yu, Y.; Wang, Z.; Yuan, W.; Qian, X.; Mikkelsen, E.M.; Laursen, A.S.D.; Fang, G.; Huang, G.; et al. Association of Maternal History of Spontaneous Abortion and Stillbirth with Risk of Congenital Heart Disease in Offspring of Women with vs without Type 2 Diabetes. JAMA Netw. Open 2021, 4, e2133805. [Google Scholar] [CrossRef]
- Yaya, S.; Bishwajit, G. Exposure to second-hand smoking as a predictor of fetal loss: Egypt Demographic and Health Survey 2014. Int. Health 2019, 11, 561–567. [Google Scholar] [CrossRef]
- Romero, R.; Dey, S.K.; Fisher, S.J. Preterm labor: One syndrome, many causes. Science 2014, 345, 760–765. [Google Scholar] [CrossRef]
- Perez-Ferre, N.; Torrejon, M.J.; Fuentes, M.; Fernandez, M.D.; Ramos, A.; Bordiu, E.; Del Valle, L.; Rubio, M.A.; Bedia, A.R.; Montañez, C.; et al. Association of Low Serum 25-Hydroxyvitamin D Levels in Pregnancy with Glucosehomeostasis and Obstetric And Newborn Outcomes. Endocr. Pract. 2012, 18, 676–684. [Google Scholar] [CrossRef]
- Wilson, R.L.; A Phillips, J.; Bianco-Miotto, T.; McAninch, D.; Goh, Z.; Anderson, P.H.; Roberts, C.T. Reduced Dietary Calcium and Vitamin D Results in Preterm Birth and Altered Placental Morphogenesis in Mice During Pregnancy. Reprod. Sci. 2020, 27, 1330–1339. [Google Scholar] [CrossRef]
- Yang, L.; Pan, S.; Zhou, Y.; Wang, X.; Qin, A.; Huang, Y.; Sun, S. The correlation between serum vitamin D deficiency and preterm birth. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2016, 22, 4401. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Thompson, J.M.; Irgens, L.M.; Rasmussen, S.; Daltveit, A.K. Secular trends in socio-economic status and the implications for preterm birth. Paediatr. Perinat. Epidemiol. 2006, 20, 182–187. [Google Scholar] [CrossRef]
- Perlman, J.M. Neurobehavioral deficits in premature graduates of intensive care--potential medical and neonatal environmental risk factors. Pediatrics 2001, 108, 1339–1348. [Google Scholar] [CrossRef]
- Gressens, P.; Rogido, M.; Paindaveine, B.; Sola, A. The impact of neonatal intensive care practices on the developing brain. J. Pediatr. 2002, 140, 646–653. [Google Scholar] [CrossRef]
- Mikolajczyk, R.T.; Zhang, J.; Betran, A.P.; Souza, J.P.; Mori, R.; Gülmezoglu, A.M.; Merialdi, M. A global reference for fetal-weight and birthweight percentiles. Lancet 2011, 377, 1855–1861. [Google Scholar] [CrossRef]
- Hoftiezer, L.; Hukkelhoven, C.W.P.M.; Hogeveen, M.; Straatman, H.M.P.M.; van Lingen, R.A. Defining small-for-gestational-age: Prescriptive versus descriptive birthweight standards. Eur. J. Pediatr. 2016, 175, 1047–1057. [Google Scholar] [CrossRef]
- Suhag, A.; Berghella, V. Intrauterine Growth Restriction (IUGR): Etiology and Diagnosis. Curr. Obstet. Gynecol. Rep. 2013, 2, 102–111. [Google Scholar] [CrossRef]
- De Bie, H.; Oostrom, K.; De Waal, H.D.-V. Brain Development, Intelligence and Cognitive Outcome in Children Born Small for Gestational Age. Horm. Res. Paediatr. 2010, 73, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Saenger, P.; Czernichow, P.; Hughes, I.; Reiter, E.O. Small for Gestational Age: Short Stature and Beyond. Endocr. Rev. 2007, 28, 219–251. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.H.; Chung, S. Small for gestational age and obesity related comorbidities. Ann. Pediatr. Endocrinol. Metab. 2018, 23, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Gortner, L.; Wauer, R.R.; Stock, G.J.; Reiter, H.L.; Reiss, I.; Jorch, G.; Hentschel, R.; Hieronimi, G. Neonatal outcome in small for gestational age infants: Do they really better? J. Périnat. Med. 1999, 27, 484–489. [Google Scholar] [CrossRef]
- Miliku, K.; Vinkhuyzen, A.; Blanken, L.M.E.; McGrath, J.; Eyles, D.; Burne, T.; Hofman, A.; Tiemeier, H.; Steegers, E.A.; Gaillard, R.; et al. Maternal vitamin D concentrations during pregnancy, fetal growth patterns, and risks of adverse birth outcomes. Am. J. Clin. Nutr. 2016, 103, 1514–1522. [Google Scholar] [CrossRef]
- Chen, Y.-H.; Fu, L.; Hao, J.-H.; Yu, Z.; Zhu, P.; Wang, H.; Xu, Y.-Y.; Zhang, C.; Tao, F.-B.; Xu, D.-X. Maternal Vitamin D Deficiency During Pregnancy Elevates the Risks of Small for Gestational Age and Low Birth Weight Infants in Chinese Population. J. Clin. Endocrinol. Metab. 2015, 100, 1912–1919. [Google Scholar] [CrossRef]
- Leffelaar, E.R.; Vrijkotte, T.G.M.; van Eijsden, M. Maternal early pregnancy vitamin D status in relation to fetal and neonatal growth: Results of the multi-ethnic Amsterdam Born Children and their Development cohort. Br. J. Nutr. 2010, 104, 108–117. [Google Scholar] [CrossRef]
- Burris, H.H.; Rifas-Shiman, S.L.; Camargo, C.A.; Litonjua, A.A.; Huh, S.Y.; Rich-Edwards, J.W.; Gillman, M.W. Plasma 25-hydroxyvitamin D during pregnancy and small-for-gestational age in black and white infants. Ann. Epidemiol. 2012, 22, 581–586. [Google Scholar] [CrossRef][Green Version]
- Chen, Y.H.; Liu, Z.B.; Ma, L.; Zhang, Z.C.; Fu, L.; Yu, Z.; Chen, W.; Song, Y.P.; Wang, P.; Wang, H.; et al. Gestational vitamin D deficiency causes placental insufficiency and fetal intrauterine growth restriction partially through inducing placental inflammation. J. Steroid Biochem. Mol. Biol. 2020, 203, 105733. [Google Scholar] [CrossRef]
- Francis, E.C.; Hinkle, S.N.; Song, Y.; Rawal, S.; Donnelly, S.R.; Zhu, Y.; Chen, L.; Zhang, C. Longitudinal Maternal Vitamin D Status during Pregnancy Is Associated with Neonatal Anthropometric Measures. Nutrients 2018, 10, 1631. [Google Scholar] [CrossRef] [PubMed]
- Hacker, A.N.; Fung, E.B.; King, J.C. Role of calcium during pregnancy: Maternal and fetal needs. Nutr. Rev. 2012, 70, 397–409. [Google Scholar] [CrossRef]
- Agarwal, S.; Kovilam, O.; Agrawal, D.K. Vitamin D and its impact on maternal-fetal outcomes in pregnancy: A critical review. Crit. Rev. Food Sci. Nutr. 2018, 58, 755–769. [Google Scholar] [CrossRef]
- Jha, R.K.; Kanyal, D.; Dhok, D.; Butola, L.K. NEED OF VITAMIN D BEYOND BONE: A CONSISE REVIEW. Eur. J. Mol. Clin. Med. 2021, 8, 1096–1109. [Google Scholar]
- Sultana, Z.; Maiti, K.; Aitken, J.; Morris, J.; Dedman, L.; Smith, R. Oxidative stress, placental ageing-related pathologies and adverse pregnancy outcomes. Am. J. Reprod. Immunol. 2017, 77, e12653. [Google Scholar] [CrossRef] [PubMed]
- Schröder-Heurich, B.; Springer, C.J.P.; Von Versen-Höynck, F. Vitamin D Effects on the Immune System from Periconception through Pregnancy. Nutrients 2020, 12, 1432. [Google Scholar] [CrossRef] [PubMed]
- Shirvani-Farsani, Z.; Behmanesh, M. RNAi-mediated knockdown of VDR surprisingly suppresses cell growth in Jurkat T and U87-MG cells. Heliyon 2019, 5, e02837. [Google Scholar] [CrossRef]
- Chen, Y.-H.; Yu, Z.; Fu, L.; Wang, H.; Chen, X.; Zhang, C.; Lv, Z.-M.; Xu, D.-X. Vitamin D3 inhibits lipopolysaccharide-induced placental inflammation through reinforcing interaction between vitamin D receptor and nuclear factor kappa B p65 subunit. Sci. Rep. 2015, 5, 1–14. [Google Scholar] [CrossRef]
- Zhang, Q.; Zhao, J.; Ni, M.; Shen, Q.; Zhou, W.; Liu, Z. Vitamin D3 reverses the transcriptional profile of offspring CD4+ T lymphocytes exposed to intrauterine inflammation. J. Steroid Biochem. Mol. Biol. 2022, 221. [Google Scholar] [CrossRef]
- Clark, D.A. Popular myths in reproductive immunology. J. Reprod. Immunol. 2014, 104–105, 54–62. [Google Scholar] [CrossRef]
- Gómez-Chávez, F.; Castro-Leyva, V.; Espejel-Núñez, A.; Zamora-Mendoza, R.G.; Rosas-Vargas, H.; Cancino-Díaz, J.C.; Cancino-Díaz, M.E.; Estrada-Gutierrez, G.; Rodríguez-Martínez, S. Galectin-1 reduced the effect of LPS on the IL-6 production in decidual cells by inhibiting LPS on the stimulation of IκBζ. J. Reprod. Immunol. 2015, 112, 46–52. [Google Scholar] [CrossRef]
- Liu, N.Q.; Kaplan, A.T.; Lagishetty, V.; Ouyang, Y.B.; Ouyang, Y.; Simmons, C.F.; Equils, O.; Hewison, M. Vitamin D and the Regulation of Placental Inflammation. J. Immunol. 2011, 186, 5968–5974. [Google Scholar] [CrossRef]
- Lambert, P.W.; Stern, P.H.; Avioli, R.C.; Brackett, N.C.; Turner, R.T.; Greene, A.; Fu, I.Y.; Bell, N.H. Evidence for extrarenal production of 1 alpha, 25-dihydroxyvitamin D in man. J. Clin. Investig. 1982, 69, 722–725. [Google Scholar] [CrossRef]
- Novakovic, B.; Galati, J.C.; Chen, A.; Morley, R.; Craig, J.M.; Saffery, R. Maternal vitamin D predominates over genetic factors in determining neonatal circulating vitamin D concentrations. Am. J. Clin. Nutr. 2012, 96, 188–195. [Google Scholar] [CrossRef]
- Gray, T.K.; Lester, G.E.; Lorenc, R.S. Evidence for extra-renal 1 α-hydroxylation of 25-hydroxyvitamin D3 in pregnancy. Science 1979, 204, 1311–1313. [Google Scholar] [CrossRef]
- Weisman, Y.; Harell, A.; Edelstein, S.; David, M.; Spirer, Z.; Golander, A. 1α, 25-Dihydroxyvitamin D3, and 24,25-dihydroxyvitamin D3 in vitro synthesis by human decidua and placenta. Nature 1979, 281, 317–319. [Google Scholar] [CrossRef]
- Evans, K.N.; Nguyen, L.; Chan, J.; Innes, B.A.; Bulmer, J.N.; Kilby, M.D.; Hewison, M. Effects of 25-Hydroxyvitamin D3 and 1,25-Dihydroxyvitamin D3 on Cytokine Production by Human Decidual Cells1. Biol. Reprod. 2006, 75, 816–822. [Google Scholar] [CrossRef]
- Liu, N.; Kaplan, A.; Low, J.; Nguyen, L.; Liu, G.; Equils, O.; Hewison, M. Vitamin D Induces Innate Antibacterial Responses in Human Trophoblasts via an Intracrine Pathway1. Biol. Reprod. 2009, 80, 398–406. [Google Scholar] [CrossRef]
- Díaz, L.; Noyola-Martínez, N.; Barrera, D.; Hernández, G.; Avila, E.; Halhali, A.; Larrea, F. Calcitriol inhibits TNF-α-induced inflammatory cytokines in human trophoblasts. J. Reprod. Immunol. 2009, 81, 17–24. [Google Scholar] [CrossRef]
- Ota, K.; Dambaeva, S.; Han, A.-R.; Beaman, K.; Gilman-Sachs, A.; Kwak-Kim, J. Vitamin D deficiency may be a risk factor for recurrent pregnancy losses by increasing cellular immunity and autoimmunity. Hum. Reprod. 2014, 29, 208–219. [Google Scholar] [CrossRef]
- Bouillon, R.; Lieben, L.; Mathieu, C.; Verstuyf, A.; Carmeliet, G. Vitamin D action: Lessons from VDR and Cyp27b1 null mice. Pediatric Endocrinol. Rev. PER 2013, 10, 354–366. [Google Scholar]
- Luderer, H.F.; Nazarian, R.M.; Zhu, E.D.; Demay, M.B. Ligand-dependent actions of the vitamin D receptor are required for activation of TGF-β signaling during the inflammatory response to cutaneous injury. Endocrinology 2013, 154, 16–24. [Google Scholar] [CrossRef]
- Halhali, A.; Acker, G.; Garabedian, M. 1, 25-Dihydroxyvitamin D3 induces in vivo the decidualization of rat endometrial cells. Reproduction 1991, 91, 59–64. [Google Scholar] [CrossRef]
- Cyprian, F.; Lefkou, E.; Varoudi, K.; Girardi, G. Immunomodulatory Effects of Vitamin D in Pregnancy and Beyond. Front. Immunol. 2019, 10, 2739. [Google Scholar] [CrossRef]
- Tavakoli, M.; Jeddi-Tehrani, M.; Salek-Moghaddam, A.; Rajaei, S.; Mohammadzadeh, A.; Sheikhhasani, S.; Kazemi-Sefat, G.-E.; Zarnani, A.H. Effects of 1,25(OH)2 vitamin D3 on cytokine production by endometrial cells of women with recurrent spontaneous abortion. Fertil. Steril. 2011, 96, 751–757. [Google Scholar] [CrossRef]
- Rajaei, S.; Mirahmadian, M.; Jeddi-Tehrani, M.; Tavakoli, M.; Zonoobi, M.; Dabbagh, A.; Zarnani, A.H. Effect of 1,25(OH)2vitamin D3on cytokine production by endometrial cells of women with repeated implantation failure. Gynecol. Endocrinol. 2012, 28, 906–911. [Google Scholar] [CrossRef]
- Penna, G.; Adorini, L. 1α, 25-dihydroxyvitamin D3 inhibits differentiation, maturation, activation, and survival of dendritic cells leading to impaired alloreactive T cell activation. J. Immunol. 2000, 164, 2405–2411. [Google Scholar] [CrossRef]
- Saito, S.; Nakashima, A.; Shima, T.; Ito, M. Th1/Th2/Th17 and regulatory T-cell paradigm in pregnancy. Am. J. Reprod. Immunol. 2010, 63, 601–610. [Google Scholar] [CrossRef]
- .Adorini, L.; Penna, G. Control of autoimmune diseases by the vitamin D endocrine system. Nat. Clin. Pr. Rheumatol. 2008, 4, 404–412. [Google Scholar] [CrossRef]
- Ganguly, A.; Tamblyn, J.A.; Finn-Sell, S.; Chan, S.-Y.; Westwood, M.; Gupta, J.; Kilby, M.D.; Gross, S.R.; Hewison, M. Vitamin D, the placenta and early pregnancy: Effects on trophoblast function. J. Endocrinol. 2018, 236, R93–R103. [Google Scholar] [CrossRef]
- Ikemoto, Y.; Kuroda, K.; Nakagawa, K.; Ochiai, A.; Ozaki, R.; Murakami, K.; Jinushi, M.; Matsumoto, A.; Sugiyama, R.; Takeda, S. Vitamin D Regulates Maternal T-Helper Cytokine Production in Infertile Women. Nutrients 2018, 10, 902. [Google Scholar] [CrossRef]
- Balogh, G.; De Boland, A.R.; Boland, R.; Barja, P. Effect of 1,25(OH)2-Vitamin D3 on the Activation of Natural Killer Cells: Role of Protein Kinase C and Extracellular Calcium. Exp. Mol. Pathol. 1999, 67, 63–74. [Google Scholar] [CrossRef]
- Mahon, P.; Harvey, N.; Crozier, S.; Inskip, H.; Robinson, S.; Arden, N.; Swaminathan, R.; Cooper, C.; Godfrey, K.; SWS Study Group. Low maternal vitamin D status and fetal bone development: Cohort study. J. Bone Miner. Res. 2010, 25, 14–19. [Google Scholar] [CrossRef]
- Marya, R. Calcium homeostasis during pregnancy and lactation: Role of vitamin D supplementation. Internet J. Med Updat. EJOURNAL 2018, 13. [Google Scholar] [CrossRef]
- Song, S.J.; Si, S.; Liu, J.; Chen, X.; Zhou, L.; Jia, G.; Liu, G.; Niu, Y.; Wu, J.; Zhang, W.; et al. Vitamin D status in Chinese pregnant women and their newborns in Beijing and their relationships to birth size. Public Heal. Nutr. 2013, 16, 687–692. [Google Scholar] [CrossRef]
- Randhawa, R.S. The insulin-like growth factor system and fetal growth restrictionn. Pediatric Endocrinol. Rev. PER 2008, 6, 235–240. [Google Scholar]
- Larqué, E.; Morales, E.; Leis, R.; Blanco-Carnero, J.E. Maternal and Foetal Health Implications of Vitamin D Status during Pregnancy. Ann. Nutr. Metab. 2018, 72, 179–192. [Google Scholar] [CrossRef]
- Haliloglu, B.; Ilter, E.; Aksungar, F.B.; Celik, A.; Coksuer, H.; Gunduz, T.; Yucel, E.; Ozekici, U. Bone turnover and maternal 25(OH) vitamin D3 levels during pregnancy and the postpartum period: Should routine vitamin D supplementation be increased in pregnant women? Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 158, 24–27. [Google Scholar] [CrossRef]
- Medici, M.; Korevaar, T.I.; Visser, W.E.; Visser, T.J.; Peeters, R.P. Thyroid function in pregnancy: What is normal? Clin. Chem. 2015, 61, 704–713. [Google Scholar] [CrossRef]
- Boogaard, E.V.D.; Vissenberg, R.; Land, J.A.; Van Wely, M.; Van Der Post, J.A.; Goddijn, M.; Bisschop, P.H. Significance of (sub)clinical thyroid dysfunction and thyroid autoimmunity before conception and in early pregnancy: A systematic review. Hum. Reprod. Updat. 2011, 17, 605–619. [Google Scholar] [CrossRef]
- Baker, A.M.; Haeri, S.; Camargo, C.A., Jr.; Espinola, J.A.; Stuebe, A.M. A nested case-control study of midgestation vitamin D deficiency and risk of severe preeclampsia. J. Clin. Endocrinol. Metab. 2010, 95, 5105–5109. [Google Scholar] [CrossRef]
- Robinson, C.J.; Wagner, C.L.; Hollis, B.W.; Baatz, J.E.; Johnson, D.D. Maternal vitamin D and fetal growth in early-onset severe preeclampsia. Am. J. Obstet. Gynecol. 2011, 204, 556.e1–556.e4. [Google Scholar] [CrossRef]
- Zhou, S.S.; Tao, Y.H.; Huang, K.; Zhu, B.B.; Tao, F.B. Vitamin D and risk of preterm birth: Up-to-date meta-analysis of randomized controlled trials and observational studies. J. Obstet. Gynaecol. Res. 2017, 43, 247–256. [Google Scholar] [CrossRef]
- Rostami, F.; Moghaddam-Benaem, L.; Ghasemi, N.; Hantoushzadeh, S. The relationship between Vitamin D deficiency and thyroid function in the first trimester of pregnancy. Arch. Pharm. Pract. 2020, 1, 131. [Google Scholar]
- Smallridge, R.C.; Glinoer, D.; Hollowell, J.G.; Brent, G. Thyroid function inside and outside of pregnancy: What do we know and what don’t we know? Thyroid 2005, 15, 54–59. [Google Scholar] [CrossRef]
- Tamer, G.; Arik, S.; Tamer, I.; Coksert, D. Relative vitamin D insufficiency in Hashimoto’s thyroiditis. Thyroid 2011, 21, 891–896. [Google Scholar] [CrossRef]
- Borzouei, S.; Goodarzi, M.T.; Biglari, M.; Nazari, F.; Shivapour, Z. The Prevalence of Thyroid Disorders in Pregnant Women of Hamadan. Avicenna J. Nurs. Midwifery Care 2019, 27, 11–17. [Google Scholar] [CrossRef]
- Chung, J.-Y.; Song, Y.; Wang, Y.; Magness, R.R.; Zheng, J. Differential Expression of Vascular Endothelial Growth Factor (VEGF), Endocrine Gland Derived-VEGF, and VEGF Receptors in Human Placentas from Normal and Preeclamptic Pregnancies. J. Clin. Endocrinol. Metab. 2004, 89, 2484–2490. [Google Scholar] [CrossRef]
- Garcia, L.A.; Ferrini, M.G.; Norris, K.C.; Artaza, J.N. 1, 25 (OH) 2vitamin D3 enhances myogenic differentiation by modulating the expression of key angiogenic growth factors and angiogenic inhibitors in C2C12 skeletal muscle cells. J. Steroid Biochem. Mol. Biol. 2013, 133, 1–11. [Google Scholar] [CrossRef]
- Stephanou, A.; Ross, R.; Handwerger, S. Regulation of human placental lactogen expression by 1,25-dihydroxyvitamin D3. Endocrinology 1994, 135, 2651–2656. [Google Scholar] [CrossRef]
- Barrera, D.; Avila, E.; Hernández, G.; Méndez, I.; González, L.; Halhali, A.; Larrea, F.; Morales, A.; Díaz, L. Calcitriol affects hCG gene transcription in cultured human syncytiotrophoblasts. Reprod. Biol. Endocrinol. 2008, 6, 1–8. [Google Scholar] [CrossRef]
- Barrera, D.; Avila, E.; Hernández, G.; Halhali, A.; Biruete, B.; Larrea, F.; Díaz, L. Estradiol and progesterone synthesis in human placenta is stimulated by calcitriol. J. Steroid Biochem. Mol. Biol. 2007, 103, 529–532. [Google Scholar] [CrossRef]
- Carter, A.M. Placental gas exchange and the oxygen supply to the fetus. Compr. Physiol. 2011, 5, 1381–1403. [Google Scholar]
- Jessel, R.H.; Rosario, F.J.; Chen, Y.-Y.; Erickson, K.; Teal, S.B.; Kramer, A.; Cotton, E.; Ryan, S.; Jansson, T.; Powell, T.L. Decreased placental folate transporter expression and activity in first and second trimester in obese mothers. J. Nutr. Biochem. 2019, 77, 108305. [Google Scholar] [CrossRef]
- Vaughan, O.; Rosario, F.; Powell, T.; Jansson, T. Regulation of Placental Amino Acid Transport and Fetal Growth. Prog. Mol. Biol. Transl. Sci. 2017, 145, 217–251. [Google Scholar] [CrossRef]
- Dłuski, D.; Mierzyński, R.; Poniedziałek-Czajkowska, E.; Leszczyńska-Gorzelak, B. Adverse pregnancy outcomes and inherited thrombophilia. J. Perinat. Med. 2018, 46, 411–417. [Google Scholar] [CrossRef]
- Dos Reis, H.L.B.; Boldrini, N.A.T.; Rangel, A.F.R.; Barros, V.F.; Merçon de Vargas, P.R.; Miranda, A.E. Placental growth disorders and perinatal adverse outcomes in Brazilian HIV-infected pregnant women. PLoS ONE 2020, 15, e0231938. [Google Scholar] [CrossRef]
- Fox, J.T.; Stover, P.J. Folate-mediated one-carbon metabolism. Vitam. Horm. 2008, 79, 1–44. [Google Scholar]
- Fleming, A.; Copp, A.J. Embryonic folate metabolism and mouse neural tube defects. Science 1998, 280, 2107–2109. [Google Scholar] [CrossRef]
- Chen, Y.-H.; Yu, Z.; Fu, L.; Xia, M.-Z.; Zhao, M.; Wang, H.; Zhang, C.; Hu, Y.-F.; Tao, F.-B.; Xu, D.-X. Supplementation With Vitamin D3 During Pregnancy Protects Against Lipopolysaccharide-Induced Neural Tube Defects Through Improving Placental Folate Transportation. Toxicol. Sci. 2015, 145, 90–97. [Google Scholar] [CrossRef]
- Harris, A.; Seckl, J. Glucocorticoids, prenatal stress and the programming of disease. Horm. Behav. 2011, 59, 279–289. [Google Scholar] [CrossRef]
- Tesic, D.; Hawes, J.E.; Zosky, G.R.; Wyrwoll, C.S. Vitamin D Deficiency in BALB/c Mouse Pregnancy Increases Placental Transfer of Glucocorticoids. Endocrinology 2015, 156, 3673–3679. [Google Scholar] [CrossRef]
- Cottrell, E.; Seckl, J.; Holmes, M.; Wyrwoll, C. Foetal and placental 11β-HSD 2: A hub for developmental programming. Acta Physiol. 2014, 210, 288–295. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Country | Survey Year(s) | N | Deficiency Definition and Incidence | Insufficiency Definition and Incidence | Gestation Age | Measurement Method |
|---|---|---|---|---|---|---|
| Malaysia [8] | 2016–2018 | 535 | <30 nmol/L 228 (42.6%) | 30–50 nmol/L 263 (49.2%) | Third trimester | Serum 25OHD concentration |
| Indonesia [9] | 2016 | 160 | <50 nmol/L 5 (3.1%) | 50–75 nmol/L 93 (58.1%) | Third trimester | Serum 25OHD concentration |
| Vietnam [10] | 2010–2012 | 960 | Deficiency < 37.5 nmol/L Insufficiency 37.5–75 nmol/L 582 (60%) < 75 nmol/L | Third trimester | Serum 25OHD concentration | |
| Thailand [11] | 2011–2012 | 147 | <50 nmol/L 50 (34.0%) | 50–75 nmol/L 61 (41.5%) | Third trimester (at delivery) | Plasma 25OHD concentration |
| China [12] | 2009 | 3598 | <50 nmol/L First trimester 519 (37.15%) Second trimester 878 (62.85%) | 50–75 nmol/L First trimester 444 (35.24%) Second trimester816 (64.76%) | First trimester Second trimester | Serum 25OHD concentration |
| Turkey [13] | 2008 | 258 | <50 nmol/L 233 (90.3%) | NA | Third trimester | Serum 25OHD concentration |
| India [14] | 2006–2007 | 541 | <50 nmol/L 521 (96.3%) | NA | All gestation age | Serum 25OHD concentration |
| Iran [15] | 2002 | 552 | <35 nmol/L 369 (66.8%) | NA | Third trimester (at delivery) | Serum 25OHD concentration |
| US [16] | 2001–2006 | 841 | <50 nmol/L First trimester 91 (46%) Second trimester 106 (32%) Third trimester 56 (18%) | 50–75 nmol/L First trimester 73 (37%) Second trimester 142 (43%) Third trimester 91 (29%) | First trimester Second trimester Third trimester | Serum 25OHDconcentration |
| Sweden [17] | 2008–2011 | 95 | <30 nmol/L 16 (17%) | 30–50 nmol/L 46 (48%) | Third trimester | Serum 25OHD concentration |
| Greece [18] | 2003–2004 | 123 | <25 nmol/L 24 (19.5%) | NA | Third trimester | Serum 25OHD concentration |
| Australia [19] | 2003–2004 | 971 | ≤25 nmol/L 144 (15%) | 26–50 nmol/L 317 (33%) | Third trimester | Serum 25OHD concentration |
| Brazil [20] | NA | 190 | <50 nmol/L First trimester 17 (23%) Second trimester 10 (9%) | 50–75 nmol/L First trimester 32 (43%) Second trimester 47 (41%) | First trimester Second trimester | Serum 25OHD concentration |
| Kenya [21] | 2011–2012 | 63 | <50 nmol/L 13 (20.6%) | 50–75 nmol/L 19 (30.2%) | Second trimester | Plasma 25OHD concentration |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, H.; Wang, S.; Tuo, L.; Zhai, Q.; Cui, J.; Chen, D.; Xu, D. Relationship between Maternal Vitamin D Levels and Adverse Outcomes. Nutrients 2022, 14, 4230. https://doi.org/10.3390/nu14204230
Zhang H, Wang S, Tuo L, Zhai Q, Cui J, Chen D, Xu D. Relationship between Maternal Vitamin D Levels and Adverse Outcomes. Nutrients. 2022; 14(20):4230. https://doi.org/10.3390/nu14204230
Chicago/Turabian StyleZhang, Heng, Shumin Wang, Lingjin Tuo, Qixiao Zhai, Jingjing Cui, Daozhen Chen, and Dexiang Xu. 2022. "Relationship between Maternal Vitamin D Levels and Adverse Outcomes" Nutrients 14, no. 20: 4230. https://doi.org/10.3390/nu14204230
APA StyleZhang, H., Wang, S., Tuo, L., Zhai, Q., Cui, J., Chen, D., & Xu, D. (2022). Relationship between Maternal Vitamin D Levels and Adverse Outcomes. Nutrients, 14(20), 4230. https://doi.org/10.3390/nu14204230