
Lupins and Health Outcomes: A Systematic Literature Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility and Exclusion Criteria
2.2. Search Strategy
2.3. Study Selection, Data Extraction, and Quality Assessment
3. Results
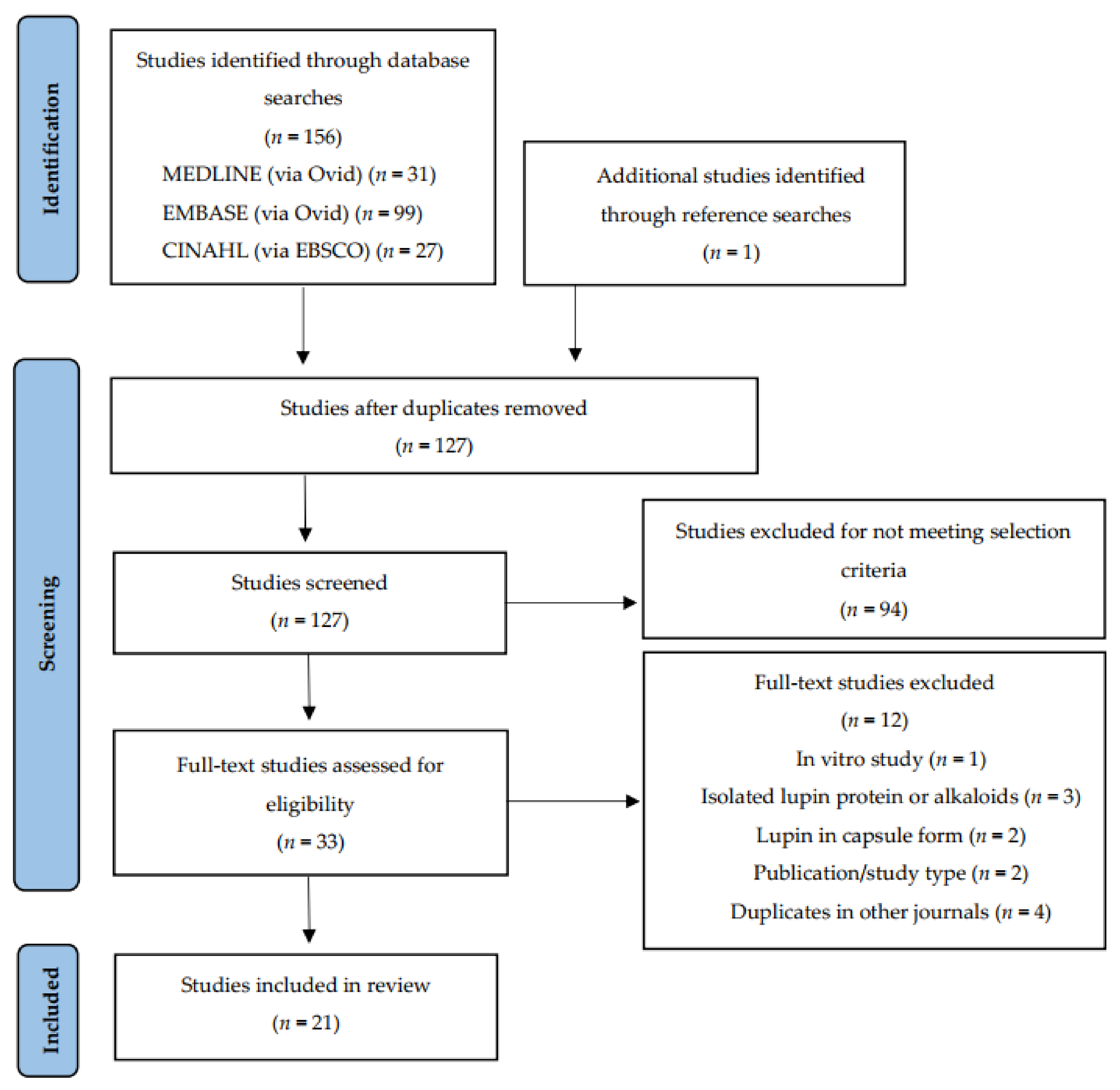
3.1. Search Results and Study Selection
3.2. Study Characteristics
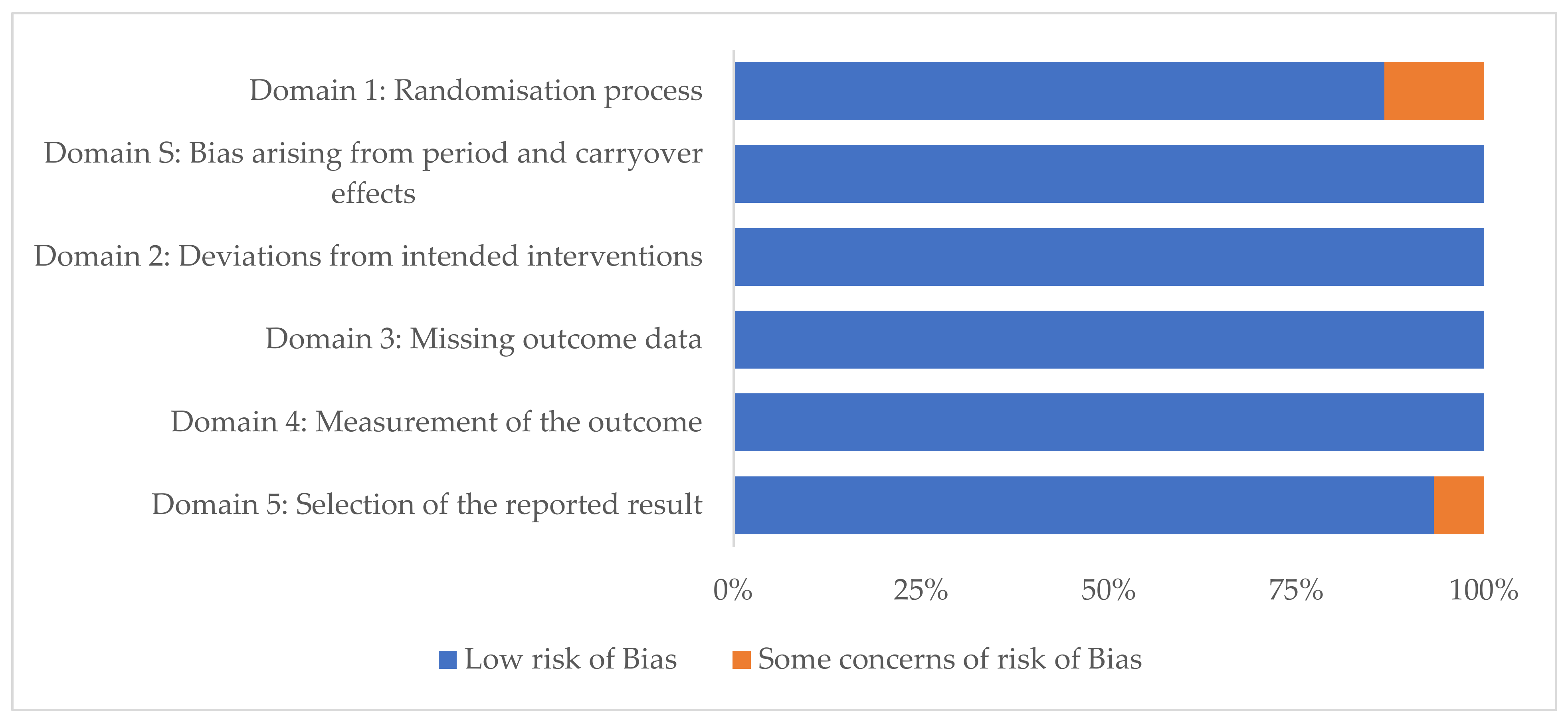
3.3. Risk of Bias
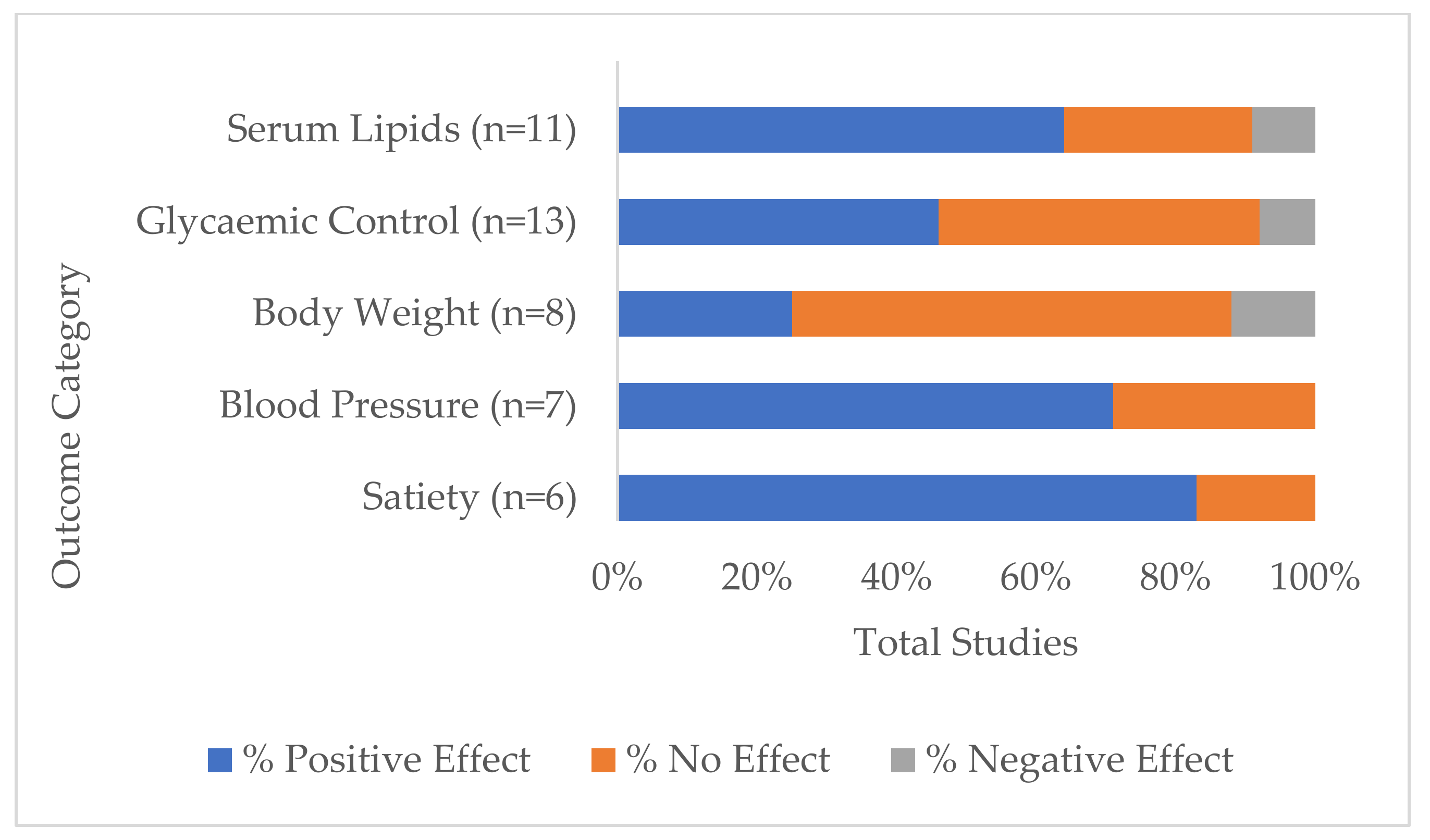
3.4. Range of Investigated Health Measurements and Their Outcomes
3.5. Range of Health Outcomes by Lupin Treatment Category
3.5.1. Whole Lupin
3.5.2. Lupin Protein
3.5.3. Lupin Fibre
4. Discussion
4.1. Whole Lupin
4.2. Lupin Protein and Fibre Components
4.3. Dose Response
4.4. Healthy vs. Unhealthy Participants Health Outcomes
4.5. Progression of Lupin and Health Outcomes Knowledge
4.6. Strengths and Limitations
4.7. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Grains & Legumes Nutrition Council (G.L.N.C). Lupins. Available online: https://www.glnc.org.au/legumes/types-of-legumes/lupins/ (accessed on 23 August 2021).
- NSW Government Industry & Investment. Lupin Growth & Development. Available online: https://www.dpi.nsw.gov.au/__data/assets/pdf_file/0006/516183/Procrop-lupin-growth-and-development.pdf (accessed on 23 August 2021).
- Foyer, C.H.; Lam, H.-M.; Nguyen, H.T.; Siddique, K.H.M.; Varshney, R.K.; Colmer, T.D.; Cowling, W.; Bramley, H.; Mori, T.A.; Hodgson, J.M.; et al. Neglecting legumes has compromised human health and sustainable food production. Nat. Plants 2016, 2, 16112. [Google Scholar] [CrossRef] [PubMed]
- Food Standards Australia New Zealand (FSANZ). Australian Sweet Lupin. Available online: https://www.foodstandards.gov.au/science/monitoringnutrients/afcd/Documents/Industry%20Report%20-%20Australian%20Sweet%20Lupin.pdf (accessed on 23 August 2021).
- Grains & Legumes Nutrition Council (G.L.N.C). Consumption of Attitudes Study Results: 2017. Available online: https://www.glnc.org.au/wp-content/uploads/2018/09/GLNC-Consumption-Study-Summary-5.pdf (accessed on 23 August 2021).
- Figueira, N.; Curtain, F.; Beck, E.; Grafenauer, S. Consumer understanding and culinary use of legumes in Australia. Nutrients 2019, 11, 1575. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council (NHMRC). A Modelling System to Inform the Revision of the Australian Guide to Healthy Eating; Department of Health and Ageing: Canberra, Australia, 2011; Volume 66. [Google Scholar]
- Kouris-Blazos, A.; Belski, R. Health benefits of legumes and pulses with a focus on Australian sweet lupins. Asia Pac. J. Clin. Nutr. 2016, 25, 1–17. [Google Scholar] [PubMed]
- Food Standards Australia New Zealand (FSANZ). Allergen Labelling. Available online: https://www.foodstandards.gov.au/consumer/labelling/Pages/Allergen-labelling.aspx (accessed on 12 November 2021).
- Allergy and Anaphylaxis Australia. Lupin. Available online: https://allergyfacts.org.au/allergy-anaphylaxis/food-allergens/lupin (accessed on 25 November 2021).
- Janusz, P. White lupin (Lupinus albus L.)—Nutritional and health values in human nutrition—A review. Czech J. Food Sci. 2017, 35, 95–105. [Google Scholar] [CrossRef]
- Bielefeld, D.; Grafenauer, S.; Rangan, A. The effects of legume consumption on markers of glycaemic control in individuals with and without diabetes mellitus: A systematic literature review of randomised controlled trials. Nutrients 2020, 12, 2123. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Heng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, 14898. [Google Scholar] [CrossRef]
- Schopen, K.; Ewald, A.C.; Johannes, B.W.; Bloch, W.; Rittweger, J.; Frings-Meuthen, P. Short-term effects of lupin vs. Whey supplementation on glucose and insulin responses to a standardized meal in a randomized cross-over trial. Front. Physiol. 2017, 8, 198. [Google Scholar] [CrossRef]
- Lee, Y.P.; Mori, T.A.; Sipsas, S.; Barden, A.; Puddey, I.B.; Burke, V.; Hall, R.S.; Hodgson, J.M. Lupin-enriched bread increases satiety and reduces energy intake acutely. Am. J. Clin. Nutr. 2006, 84, 975–980. [Google Scholar] [CrossRef]
- Keogh, J.; Atkinson, F.; Eisenhauer, B.; Inamdar, A.; Brand-Miller, J. Food intake, postprandial glucose, insulin and subjective satiety responses to three different bread-based test meals. Appetite 2011, 57, 707–710. [Google Scholar] [CrossRef]
- Hall, R.S.; Thomas, S.J.; Johnson, S.K. Australian sweet lupin flour addition reduces the glycaemic index of a white bread breakfast without affecting palatability in healthy human volunteers. Asia Pac. J. Clin. Nutr. 2005, 14, 91–97. [Google Scholar]
- Fechner, A.; Fenske, K.; Jahreis, G. Effects of legume kernel fibres and citrus fibre on putative risk factors for colorectal cancer: A randomised, double-blind, crossover human intervention trial. Nutr. J. 2013, 12, 101. [Google Scholar] [CrossRef]
- Smith, S.C.; Choy, R.; Johnson, S.K.; Hall, R.S.; Wildeboer-Veloo, A.C.; Welling, G.W. Lupin kernel fiber consumption modifies fecal microbiota in healthy men as determined by rRNA gene fluorescent in situ hybridization. Eur. J. Nutr. 2006, 45, 335–341. [Google Scholar] [CrossRef]
- Johnson, S.K.; Chua, V.; Hall, R.S.; Baxter, A.L. Lupin kernel fibre foods improve bowel function and beneficially modify some putative faecal risk factors for colon cancer in men. Br. J. Nutr. 2006, 95, 372–378. [Google Scholar] [CrossRef]
- Hall, R.S.; Johnson, S.K.; Baxter, A.L.; Ball, M.J. Lupin kernel fibre-enriched foods beneficially modify serum lipids in men. Eur. J. Clin. Nutr. 2005, 59, 325–333. [Google Scholar] [CrossRef]
- Ward, N.C.; Mori, T.A.; Beilin, L.J.; Johnson, S.; Williams, C.; Gan, S.K.; Puddey, I.B.; Woodman, R.; Phillips, M.; Connolly, E.; et al. The effect of regular consumption of lupin-containing foods on glycaemic control and blood pressure in people with type 2 diabetes mellitus. Food Funct. 2020, 11, 741–747. [Google Scholar] [CrossRef]
- Skalkos, S.; Moschonis, G.; Thomas, C.J.; McMillan, J.; Kouris-Blazos, A. Effect of lupin-enriched biscuits as substitute mid-meal snacks on post-prandial interstitial glucose excursions in post-surgical hospital patients with type 2 diabetes. Nutrients 2020, 12, 1239. [Google Scholar] [CrossRef]
- Fornasini Salvador, M.V.; Abril-Ulloa, S.V.; Beltran Carreno, J.P.; Villacres, E.; Cuadrado-Merino, L.; Robalino, F.; Sanchez, R.; Ricaurte Ortiz, P.S.; Munoz, E.B.; Benitez Loza, N.B.; et al. Efficacy of a Lupinus mutabilis Sweet snack as complement to conventional type 2 diabetes mellitus treatment. Nutr. Hosp. 2019, 36, 905–911. [Google Scholar] [CrossRef]
- Dove, E.R.; Mori, T.A.; Chew, G.T.; Barden, A.E.; Woodman, R.J.; Puddey, I.B.; Sipsas, S.; Hodgson, J.M. Lupin and soya reduce glycaemia acutely in type 2 diabetes. Br. J. Nutr. 2011, 106, 1045–1051. [Google Scholar] [CrossRef]
- Weisse, K.; Brandsch, C.; Zernsdorf, B.; Nkengfack Nembongwe, G.S.; Hofmann, K.; Eder, K.; Stangl, G.I. Lupin protein compared to casein lowers the LDL cholesterol:HDL cholesterol-ratio of hypercholesterolemic adults. Eur. J. Nutr. 2010, 49, 65–71. [Google Scholar] [CrossRef]
- Sirtori, C.R.; Triolo, M.; Bosisio, R.; Bondioli, A.; Calabresi, L.; De Vergori, V.; Gomaraschi, M.; Mombelli, G.; Pazzucconi, F.; Zacherl, C.; et al. Hypocholesterolaemic effects of lupin protein and pea protein/fibre combinations in moderately hypercholesterolaemic individuals. Br. J. Nutr. 2012, 107, 1176–1183. [Google Scholar] [CrossRef]
- Fechner, A.; Kiehntopf, M.; Jahreis, G. The formation of short-chain fatty acids is positively associated with the blood lipid-lowering effect of lupin kernel fiber in moderately hypercholesterolemic adults. J. Nutr. 2014, 144, 599–607. [Google Scholar] [CrossRef]
- Bahr, M.; Fechner, A.; Kramer, J.; Kiehntopf, M.; Jahreis, G. Lupin protein positively affects plasma LDL cholesterol and LDL:HDL cholesterol ratio in hypercholesterolemic adults after four weeks of supplementation: A randomized, controlled crossover study. Nutr. J. 2013, 12, 107. [Google Scholar] [CrossRef]
- Bahr, M.; Fechner, A.; Kiehntopf, M.; Jahreis, G. Consuming a mixed diet enriched with lupin protein beneficially affects plasma lipids in hypercholesterolemic subjects: A randomized controlled trial. Clin. Nutr. 2015, 34, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Croft, K.D.; Lee, Y.P.; Mori, T.A.; Puddey, I.B.; Sipsas, S.; Barden, A.; Swinny, E.; Hodgson, J.M. The effects of a lupin-enriched diet on oxidative stress and factors influencing vascular function in overweight subjects. Antioxid. Redox Signal. 2010, 13, 1517–1524. [Google Scholar] [CrossRef]
- Lee, Y.P.; Mori, T.A.; Puddey, I.B.; Sipsas, S.; Ackland, T.R.; Beilin, L.J.; Hodgson, J.M. Effects of lupin kernel flour-enriched bread on blood pressure: A controlled intervention study. Am. J. Clin. Nutr. 2009, 89, 766–772. [Google Scholar] [CrossRef]
- Hodgson, J.M.; Lee, Y.P.; Puddey, I.B.; Sipsas, S.; Ackland, T.R.; Beilin, L.J.; Belski, R.; Mori, T.A. Effects of increasing dietary protein and fibre intake with lupin on body weight and composition and blood lipids in overweight men and women. Int. J. Obes. 2010, 34, 1086–1094. [Google Scholar] [CrossRef]
- Belski, R.; Mori, T.A.; Puddey, I.B.; Sipsas, S.; Woodman, R.J.; Ackland, T.R.; Beilin, L.J.; Dove, E.R.; Carlyon, N.B.; Jayaseena, V.; et al. Effects of lupin-enriched foods on body composition and cardiovascular disease risk factors: A 12-month randomized controlled weight loss trial. Int. J. Obes. 2011, 35, 810–819. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G.; Iqbal, K.; Schwedhelm, C.; Boeing, H. Food groups and intermediate disease markers: A systematic review and network meta-analysis of randomized trials. Am. J. Clin. Nutr. 2018, 108, 576–586. [Google Scholar] [CrossRef] [PubMed]
- Melse-Boonstra, A. Bioavailability of micronutrients from nutrient-dense whole foods: Zooming in on dairy, vegetables, and fruits. Front. Nutr. 2020, 7, 101. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Reference | Lupin Species/Common Name (NS = Not Stated) | Whole Seed (W), Protein Isolate (PI) or Fibre Isolate (FI) |
|---|---|---|---|
| Australia | Hall et al., 2005 [18] | L. angustifolius | W |
| Hall et al., 2005 [22] | L. angustifolius | FI | |
| Smith et al., 2006 [20] | L. angustifolius | FI | |
| Johnson et al., 2006 [21] | L. angustifolius | FI | |
| Lee et al., 2006 [16] | NS | W | |
| Lee et al., 2009 [33] | NS | W | |
| Yang et al., 2010 [32] | NS | W | |
| Hodgson et al., 2010 [34] | L. angustifolius | W | |
| Dove et al., 2011 [26] | L. angustifolius | W | |
| Keogh et al., 2011 [17] | NS | W | |
| Belski et al., 2011 [35] | L. angustifolius | W | |
| Skalkos et al., 2020 [24] | Australian Sweet Lupin | W | |
| Ward et al., 2020 [23] | L. angustifolius | W | |
| Germany | Weiße et al., 2010 [27] | L. angustifolius | PI |
| Bähr et al., 2013 [30] | L. angustifolius | PI | |
| Fechner et al., 2013 [19] | L. angustifolius and L. albus | FI | |
| Fechner et al., 2014 [29] | L. angustifolius | FI | |
| Bähr et al., 2015 [31] | L. angustifolius | PI | |
| Schopen et al., 2017 [15] | L. albus | W | |
| Italy | Sirtori et al., 2012 [28] | L. angustifolius | PI |
| Ecuador | Fornasini et al., 2019 [25] | L. mutabilis | W |
| Reference | Study Type | Subjects (n) and Characteristics | Intervention | Control/Comparator | Energy Balance | Main Health Markers | Main Outcomes |
|---|---|---|---|---|---|---|---|
| Hall et al., 2005 [18] | RCT single blind cross-over Post-meal study | n = 11 Healthy men (n = 9) and women (n = 2). Mean age 31.6 years, range 25–45 years | Breakfast including lupin bread with 10% wheat flour replaced with Australian sweet lupin kernel flour | Breakfast including standard recipe white bread | 95kJ difference in lupin breakfast (1338 kJ) and control breakfast (1243 kJ) | 120 min SG, SI 180 min satiety response. Glycaemic index (GI), insulinaemic index (II) and satiety index (WB = 100). Energy intake from ad libitum buffet and during remainder of day. | ↓ GI (p = 0.022) ↑ II (p = 0.046) Trend to lower SG at 30 min. Peak satiety at 10 min WB and 25 min lupin. Below baseline at 160 min for WB. Lupin did not reach zero within 180 min. No difference in SI, satiety response, satiety index, energy intake at ad libitum buffet, or energy intake during remainder of day. |
| Lee et al., 2006 [16] | RCT cross-over Study 1: 4 treatments 1 week apart | Study 1: n = 16 healthy men (n = 8) and women (n = 8). Mean age 58.6 ± 7.2 years. Mean BMI 31.3 ± 4.5 kg/m2 | Lupin bread 40% total flour (24% final weight of bread) in 4 treatments: WB-WB/WB-lupin/lupin-WB/lupin-lupin | White bread breakfast and lunch | Isocaloric at breakfast, ad libitum lunch | Post breakfast 180 min satiety response. Total energy intake after ad libitum lunch. | ↑ Satiety at breakfast for satisfaction and prospective consumption (p < 0.001, p < 0.001). ↑ Satiety at 180 min for fullness (p < 0.001), satisfaction (p < 0.001) and prospective consumption (p < 0.001). ↓ Energy intake at lunch after lupin breakfast (−488; 95% CI: −798, −178 kJ). ↓ Intrameal energy intake when lupin consumed at lunch(−1028; 95% CI: −1338, −727 kJ). |
| Study 2: 2 treatments 1 week apart | Study 2: n = 17 healthy men (n = 11) and women (n = 6). Mean age 61.0 ± 5.6 years. Mean BMI 27.2 ± 4.3 kg/m2 | Lupin bread 40% wheat flour replaced with lupin kernel flour | White bread | Isocaloric | Post breakfast 180 min plasma ghrelin, SG and SI | Altered ghrelin response (p = 0.04) ↓ 180 min plasma ghrelin (p = 0.009). Altered glucose response (p = 0.01) ↓ glucose AUC (p = 0.006) ↓ insulin AUC (p = 0.002). | |
| Lee et al., 2009 * [33] | RCT parallel study 16 weeks 2 cohorts | n = 74 Overweight and obese men (n = 26) and women (n = 48) Mean age 59.0 ± 7.4/56.8 ± 8.5 years. Mean BMI 30.6 ± 3.6/30.5 ± 3.4 kg/m2. | Lupin bread 40% wheat flour replaced with lupin kernel flour (24% final weight bread) to replace usual carbohydrate-rich foods to ~15–20% usual energy intake. | White bread to replace normal bread intake and other carbo-hydrate-rich foods to ~15–20% usual energy intake | Isocaloric | 24-h SBP, DBP, pulse pressure and heart rate | ↓ 24-h SBP (p = 0.03) ↓ pulse pressure (p < 0.001). No difference in DBP, heart rate |
| Yang et al., 2010 * [32] | Paper refers to the Lee et al., 2009 study above | As above | As above | As above | As above | Plasma and urinary F2-isoprostanes, plasma 20-HETE, plasma and urinary nitrite and nitrate concentrates | No difference between groups |
| Hodgson et al., 2010 * [34] | Paper refers to the Lee et al., 2009 study above | As above | As above | As above | As above | BW every 2 weeks Body composition at 16 weeks TC, HDL, TG, LDL, SG, SI, HOMA-IR, plasma leptin and adiponectin, hs-CRP | No difference between groups |
| Dove et al., 2011 [26] | RCT cross-over study of 3 test sessions, 7–14 days apart | n = 24 type 2 diabetic men (n = 19) and women (n = 5). Mean age: 57 ± 6.6 years, range 44–66 years. Mean BMI: 30.9 ± 4.8 kg/m2 | Beverage of 50 g glucose and 50 g lupin kernel flour | Beverage of 50% glucose (control), beverage of 50% glucose + soya protein and fibre isolates (comparator) | All beverages matched for total volume, carbohydrates and fat content lupin and soya matched for energy, protein and fibre | 240 min SG, SI and C-peptide response | ↓ 240 min SG response (p < 0.001), ↑ 240 min SI and C-peptide responses (p < 0.001) ↓ SI response compared with soya (p = 0.013). No difference in SG and C-peptide responses between lupin and soya |
| Keogh et al., 2011 [17] | RCT cross-over study | n = 20 Healthy men (n = 10) and women (n = 10) Mean age 29.4 years Range: 20.1–44.8 years BMI 21.8 kg/m2 Range: 18.4–24.8 kg/m2 | Lupin Bread breakfast | White bread breakfast (control), wholemeal and seeds bread breakfast (comparator) | Isocaloric breakfast, ad libitum standardised food and beverage tray 120 min post breakfast | 120 min satiety, PG and insulin response. Food and beverage weight, energy and macronutrient content 120 min post meal | ↑ Fullness response for lupin (p < 0.01) and WSB (p < 0.05) ↓ glucose AUC for lupin and WSB (p < 0.001) ↓ insulin AUC for lupin and WSB (p < 0.001) ↓ weight of food and beverage for lupin and WSB (p < 0.05) ↓ energy and total fat consumed after WSB (p < 0.05). No difference in energy and macronutrient intake post lupin meal. |
| Belski et al., 2011 [35] | RCT double blind parallel study 12 months 2 cohorts | n = 131 n = 93 at 12 months Overweight and obese men (n = 68) and women (n = 63) Mean age 46.5 ± 10.1/46.7 ± 9.4. Mean BMI 31.3 ± 2.7/31.4 ± 2.8 kg/m2 | Lupin kernel flour in bread, biscuits and pasta | Standard food products without lupin (matched for colour, taste, texture) | Isocaloric | 4 and 12 month BW, body composition SBP, DBP, TC, HDL, LDL, TG, SG and SI, HOMA-IR and hs-CRP. | ↓ 24-h SBP and DBP at 12 months (p < 0.05) ↓ HDL (p < 0.05) ↓ SI and HOMA-IR at 4 and 12 months (p < 0.05) No difference in TC, LDL, TG, SG, hs-CRP BW or body composition at 4 or 12 months. No difference in maintenance of body weight loss during weight maintenance period (4–12 months) |
| Schopen et al., 2017 [15] | RCT single blind cross-over study 3 test visits 24 h apart | n = 12 healthy men (n = 5) and women (n = 7). Mean age men 28 ± 3.67 years, women 26.86 ± 3.44 years. Mean BMI men 24.72 ± 2.3 kg/m2, women 20.92 ± 1.63 kg/m2 | Sweet lupin flour in lunch meal of pasta and meat sauce (0.94 g lupin flour per kg of participant body weight) | Pasta and meat sauce lunch (reference meal), pasta and meat sauce lunch with whey protein (0.42 g per kg of participant BW) | Standardised breakfast, standardised test lunch. Lupin and whey meals matched for protein. Reference meal ~22% less kJ and ~50% less protein per kg of participant BW. All test meals similar in carbohydrate | 180 min SG 180 min SI Post test meal | ↓ SG AUC 0–60 min (p < 0.001) ↓ SG AUC 0–180 min (p = 0.030). No difference in SI |
| Fornasini et al., 2019 [25] | Controlled non-randomised single blind cross-over study (28 weeks) (One-group pretest-posttest design with double pretest) | n = 5 type 2 diabetic men (n = 19) and women (n = 32) under conventional non-insulin medication. Mean age 64.1 ± 11.1 years. Mean BMI 30.3 ± 4.5 kg/m2 | Whole Lupinus mutabilis 10 g dehydrated lupin snack. One dose per day 7 weeks (following initial 14-week medication only period). 2 doses per day next 7 weeks | Usual diet and medication | N/A | At 14 and 28 weeks BW, SBP, DBP, SG, SI, HbA1c, TC, LDL, HDL, Uric acid, CRP | ↑ SG and SI 0–28 weeks (p ≤ 0.05) ↑ HDL 0–28 weeks (p ≤ 0.05) ↓ BW (p = 0.015) and BMI (p = 0.009) 0–28 weeks ↓ SBP and DBP 0–28 and 14–28 weeks (p ≤0.05). No difference in HbA1c, TC, LDL, uric acid, CRP |
| Skalkos et al., 2020 [24] | Controlled non-randomised cross-over study 3 consecutive days, 1 treatment per day | n = 20 Post-surgical hospital patient men (n = 12) and women (n = 8) with type 2 diabetes. Mean age 74.3 ± 11.7 years. Mean BMI 30.7 ± 4.5 kg/m2 | 4 × lupin biscuit containing 20% lupin flour (2 at morning tea and 2 at afternoon tea) on day 1 | 4 × wholemeal spelt biscuit day 2 4 × Arnott’s Marie biscuit (standard hospital option) day 3 | Lupin and spelt biscuits isocaloric (1590 kJ/100 g) and lower than Marie biscuit (1850 kJ/100 g). Higher protein, fat and fibre in lupin and spelt, and lower carbohydrate and sugar than Marie biscuit | CGM interstitial glucose pre- and 5 timepoints post-meal, bowel function (Bristol Stool Chart), hunger and fullness rating | ↓ glucose after dinner following lupin biscuit (p < 0.001) No difference in 0–90 min glucose at breakfast, morning tea, lunch, and afternoon tea for all 3 treatments. More patients felt fuller between afternoon tea-dinner following lupin biscuit (p = 0.018). No difference in bowel function |
| Ward et al., 2020 [23] | RCT double blind cross-over study 1-week run-in period, 2 × 8-week treatment with 8-week washout period | n = 22 n = 17 completed, men (n = 14) and women (n = 8) with moderate-to-well controlled type 2 diabetes (HbA1c < 9%) Mean age 58 ± 6.6 years. Mean BMI 29.9 ± 3.5 kg/m2 | Lupin-enriched foods replacing 20% of daily energy intake. Consumed every breakfast, lunch and at least 3 dinners per week. Average daily intake ~45 g lupin per day (12 g/d protein 10 g/d fibre) | Wheat-based control foods | Isocaloric | SG (at waking, 1 h post breakfast, immediately pre-lunch and 1 h post-lunch), SI, HOMA-IR, BW, BP, TC, LDL, TG, HDL, C-peptide | No difference between treatments. Borderline significant decrease in TG with lupin |
| Reference | Study Type | Subjects (n) and Characteristics | Intervention | Control/Comparator | Energy Balance | Main Health Markers | Main Outcomes |
|---|---|---|---|---|---|---|---|
| Weiße et al., 2010 [27] | RCT double blind parallel study 10-day run-in, 6-week treatment | n = 56 n = 43 completed, moderately hypercholesterol-aemic (5.7–7.9 mmol/L) men (n = 25) and women (n = 31). Mean age 43.9 ± 11.8 years. Mean BMI 25.9 ± 4.5 kg/m2 | Blue lupin protein isolate, 35 g in 2 snack bars per day | Casein protein (CP), 35 g protein in snack bars per day | Isocaloric | LDL:HDL, TC, LDL, HDL, TG, PG, mRNA SREBP-2, LDL receptor and HMG-CoA reductase | ↓ LDL:HDL for lupin compared to CP (p < 0.05) ↓ 0–6 week TC and LDL in lupin group ↓ 0–6 week TC, HDL, and TG for CP group (all p < 0.05) No difference between groups. ↓ alanine and glycine after CP ↓ methionine after Lupin, and ↓ than CP (p < 0.05) ↑ SREBP-2 in Lupin group, but not CP ↑ LDL receptor and ↓ HMG-CoA reductase in both groups (p < 0.05) No difference between groups for all 3 mRNA outcomes |
| Sirtori et al., 2012 [28] | RCT double blind, parallel study 4-week run-in, 4-week treatment | n = 193 n = 175 completed, moderately hypercholesterol-aemic (TC > 2200 mg/L) men (n = 82) and women (n = 93). Mean age range 52.7 ± 12.4–55.3 ± 14.6 years. Mean BMI range 24.0 ± 2.0–25.6 ± 3.2 kg/m2 | Blue lupin protein isolate/cellulose fibre combination added to 2 snack bars per day | Control: casein/cellulose. Comparators: lupin/cellulose; pea protein/cellulose; casein/oat fibre; casein/apple pectin; pea protein/oat fibre; pea protein/apple pectin | Isocaloric | TC, LDL, HDL, TG, SG, SI, HOMA-IR, BW, adiponectin, sICAM-1, IL-6, hs-CRP | ↓ TC lupin/cellulose (p < 0.05) (Greatest reduction in TC (p = 0.0098) and LDL (p = 0.004) in pea/apple pectin treatment). No difference lupin/cellulose for LDL, HDL, TG, SG, SI or HOMA-IR (casein/cellulose, casein/apple pectin and pea/oat fibre all decreased SI and HOMA-IR (p < 0.05). Pea/oat fibre also decreased SG (p < 0.05)). No difference in adiponectin or inflammatory markers |
| Bähr et al., 2013 [30] | RCT double-blind cross-over study 8-week treatment, 4-week washout | n = 33 hypercholesterol-aemic (TC ≥ 5.2 mmol/L) men (n = 33) and women (n = 18). Mean age range 49.4 ± 13.9–49.7 ± 12.8 years. Mean BMI range 27.3 ± 5.4–28.8 ± 6.5 kg/m2 | Blue lupin protein isolate (LPI) protein drinks, 25 g LPI per day | Milk protein isolate (MPI) protein drinks, 25 g MPI per day | Isocaloric | TC, LDL, HDL, LDL:HDL, TG, 4 and 8week BW, SBP, DBP, resting pulse, urea, hs-CR | ↑ HDL at week 4 for LPI compared to MPI (p = 0.036) No difference between treatments for lipids ↓ LDL for both treatments at 4 weeks but not at 8 weeks (p ≤ 0.008) ↓ LDL:HDL for LPI (p = 0.022) Both treatments slight ↑ BW and body fat from 0–8 weeks (p ≤ 0.045) No difference between treatments ↓ SBP for both (p ≤ 0.014) ↓ DBP and resting pulse for LPI (p ≤ 0.044) No difference between treatments. No difference between treatments in hs-CRP and urea 0–4 or 0–8 weeks, ↑ urea 0–4 weeks for both treatments (p ≤ 0.001) with smaller increases 0–8 weeks (p ≤ 0.022) |
| Bähr et al., 2015 [31] | RCT double blind, cross-over 3-phase study 28 days treatment 6-week washout | n = 72 n = 68 completed, hypercholesterol-aemic (TC ≥ 5.2 mmol/L) men (n = 28) and women (n = 40). Mean age range 50.4 ± 19.2–59.8. ± 9.3 years. Mean BMI range 24.9 ± 5.0–27.6 ± 4.4 kg/m2 | Blue lupin protein isolate, 25 g consumed daily in 4 food products. | Milk protein (MP) 25 g in 4 food products; MP foods plus 2.5 g/d arginine in capsule form (MPA). Placebo capsules added to LP and MP diets for blindness | Isocaloric | TC, LDL, HDL, LDL:HDL, oxidised LDL, TG, SBP, DBP hs-CRP, urea, uric acid, homocysteine | ↓ LDL after Lupin compared with MP (p = 0.044) ↓ 0–28 d TC (p < 0.001), LDL (p < 0.01) and HDL (p < 0.001) after lupin and MPA ↓ TG (p < 0.05) after Lupin Increases in urea were smaller for Lupin (p = 0.004) and MP (p = 0.001) compared with MPA ↓ Uric acid (p < 0.01) after lupin ↓ homocysteine after lupin compared with MP (p = 0.001) and MPA (p = 0.004) |
| Reference | Study Type | Subject (n) and Characteristics | Intervention | Control/Comparator | Energy Balance | Main Health Markers | Main Outcomes |
|---|---|---|---|---|---|---|---|
| Hall et al., 2005 * [22] | RCT single blind cross-over study 28 days of treatment 28 days washout period | n = 44 n = 38 completed, healthy men. Mean age 41.0 ± 1.9 years. Mean BMI 26.7 ± 0.5 kg/m2 | Australian sweet lupin kernel fibre in foods within prescribed diet. 55 g dietary fibre/day for diets >9 MJ/day, 35 g dietary fibre/day for diets ≤9 MJ/day | Prescribed control diet without added lupin fibre. 25 g dietary fibre/day for diets >9 MJ/day, 18 g dietary fibre/day for diets ≤9 MJ/day | Isocaloric | TC, HDL, TG, PG and insulin, HOMA-IR, satiety perception, BW | ↓ TC, LDL, TC:HDL and LDL:HDL for both treatments (p < 0.05) ↓ TC (p = 0.001), LDL (p = 0.001) TC:LDL (p = 0.006 ) and LDL:HDL (p = 0.003) for lupin relative to control. No difference in HDL and TG. No difference in PG for lupin (↓ PG in control (p = 0.001)) No difference in PG, insulin, HOMA-IR or satiety perception between treatments. No difference in BW for either treatment |
| Smith et al., 2006 * [20] | Paper refers to the Hall 2005 study above | n = 18 (randomly selected from above study) | As above | As above | As above | Measures of (i) total cells, (ii) total bacteria, (iii) E. rectale-C. coccoides, (iv) Bacteriodes-Prevotella, (v) Enterobacteriaceae, (vi) C. histolyticum/C. lituseburense group, (vii) Lactobacillus-Enterococci, (viii) Bifidobacterium, (ix) C. ramosum, C. spiroforme and C. cocleatum group | ↑ Bifidobacteria (p = 0.001) ↓ C. ramosum, C. spiroforme and C. cocleatum group (p = 0.039) in lupin diet. No difference between treatments in total cells, total bacteria or populations of other species. Strong trend (p = 0.53) towards decreased Bacteroides-Prevotella in lupin diet |
| Johnson et al., 2006 * [21] | Paper refers to the Hall 2005 study above | n = 38 healthy men. Mean age 41.0 ± 1.9 years. Mean BMI 26.7 ± 0.5 kg/m2 | As above | As above | As above | Frequency and ease of bowel motion, flatulence level, Bristol Stool Form, frequency (events), output, transit time, pH, faecal moisture content SCFA (total, acetate, propionate, isobutyrate, butyrate, isovalerate, valerate) | ↑ Frequency (p = 0.047), ↑ faecal output (p = 0.020), ↓ transit time (p = 0.012), ↑ perception of flatulence level (p < 0.001), ↓ faecal pH (p < 0.001), ↑ faecal moisture content (p = 0.027), ↑ total SCFA concentration (p = 0.001) and ↑ daily output (p < 0.001), ↑ acetate concentration (p < 0.001) and ↑ daily output (p < 0.001) ↑ butyrate concentration (p = 0.006) and output (p = 0.002) ↑ valerate output (p = 0.030) with no difference in concentration. No difference in proprionate, isobutyrate or isovalerate. |
| Fechner et al., 2013 [19] | RCT double blind cross-over study 4 periods of 2 weeks each: run-in, 2 treatments and washout | n = 76 healthy men (n = 21) and women (n = 55). Mean age 24.4 ± 3.2 years. Mean BMI 21.7 ± 2.4 kg/m2 | Blue lupin kernel fibre and white lupin kernel fibre. Total dietary fibre per treatment 25 g/d in beverages | Citrus fibre as active comparator for 2 lupin and 1 soya fibre treatments | Isocaloric | TC, HDL, LDL, TG, faecal pH, transit time, Bristol Stool Form, faecal SCFAs and bile acids | No change in serum lipids for all treatments, ↓ faecal pH for blue lupin (p < 0.01), no difference relative to citrus. ↓ Transit time, ↑ Bristol Stool Form score for blue lupin (p ≤ 0.05) ↑ Total SCFA, acetate, propionate and n-butyrate excretion for blue lupin (p ≤ 0.05). ↑ Primary bile acid excretion (p = 0.02) for blue lupin, ↓ total bile acid excretion for blue lupin relative to citrus. ↓ Total bile acid excretion for white lupin from run-in. ↓ Secondary bile acid excretion for blue and white lupin from run-in (p ≤ 0.05). |
| Fechner et al., 2014 [29] | RCT double blind cross-over study 3 intervention periods of 4 weeks each, run-in and 2 washout periods of 2 weeks each | n = 52 moderately hypercholesterol-aemic (TC >5.2 mmol/L) men (n = 20) and women (n = 32). Mean age: 46.9 ± 3.2 years. Mean BMI: 26.5 ± 5.9 kg/m2 | Blue lupin kernel fibre 25 g/d | Citrus fibre 25 g/d as active comparator; control diet (CD) with no added fibre | Isocaloric | General excretion markers, faecal concentration or excretion of neutral sterols, bile acids and SCFAs. BW, body composition, BP, TC, HDL, LDL, TG LDL:HDL hs-CRP, satiety score | ↓ Faecal pH from baseline (p ≤ 0.01) and against CD (p ≤ 0.001), ↓ transit time against CD (p ≤ 0.05), no difference in neutral sterols. ↑ Primary bile acids from baseline (p ≤ 0.05), no difference in total or secondary bile acids. ↑ Formation of total SCFA from baseline (p ≤ 0.001) and against CD (p ≤ 0.01), ↑ acetate from baseline and against CD (p ≤ 0.001), ↑ propionate from baseline (p ≤ 0.001) and against control (p ≤ 0.05), ↑ butyrate from baseline (p ≤ 0.01) and against control (p ≤ 0.05). ↓ BW, BMI, and WC from baseline (p ≤ 0.001) and against control (p ≤ 0.01). ↓ TC (9%), LDL (12%) and TG (10%) for lupin compared with citrus (p ≤ 0.02), ↓ hs-CRP (p = 0.02), SBP (p = 0.01) for lupin compared to baseline. ↑ Perception of satiety (p ≤ 0.001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bryant, L.; Rangan, A.; Grafenauer, S. Lupins and Health Outcomes: A Systematic Literature Review. Nutrients 2022, 14, 327. https://doi.org/10.3390/nu14020327
Bryant L, Rangan A, Grafenauer S. Lupins and Health Outcomes: A Systematic Literature Review. Nutrients. 2022; 14(2):327. https://doi.org/10.3390/nu14020327
Chicago/Turabian StyleBryant, Lesley, Anna Rangan, and Sara Grafenauer. 2022. "Lupins and Health Outcomes: A Systematic Literature Review" Nutrients 14, no. 2: 327. https://doi.org/10.3390/nu14020327
APA StyleBryant, L., Rangan, A., & Grafenauer, S. (2022). Lupins and Health Outcomes: A Systematic Literature Review. Nutrients, 14(2), 327. https://doi.org/10.3390/nu14020327