
The Relationship between Body Composition, Dietary Intake, Physical Activity, and Pulmonary Status in Adolescents and Adults with Cystic Fibrosis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Eligibility Criteria
2.2. Clinical Assessments
2.3. Dietary Intake and Physical Activity Assessments
2.4. Assessment of Body Composition
2.5. Statistical Analyses
3. Results
3.1. Clinical Characteristics
3.2. Body Composition and Dietary Intake in Participants with CF and Healthy Volunteers
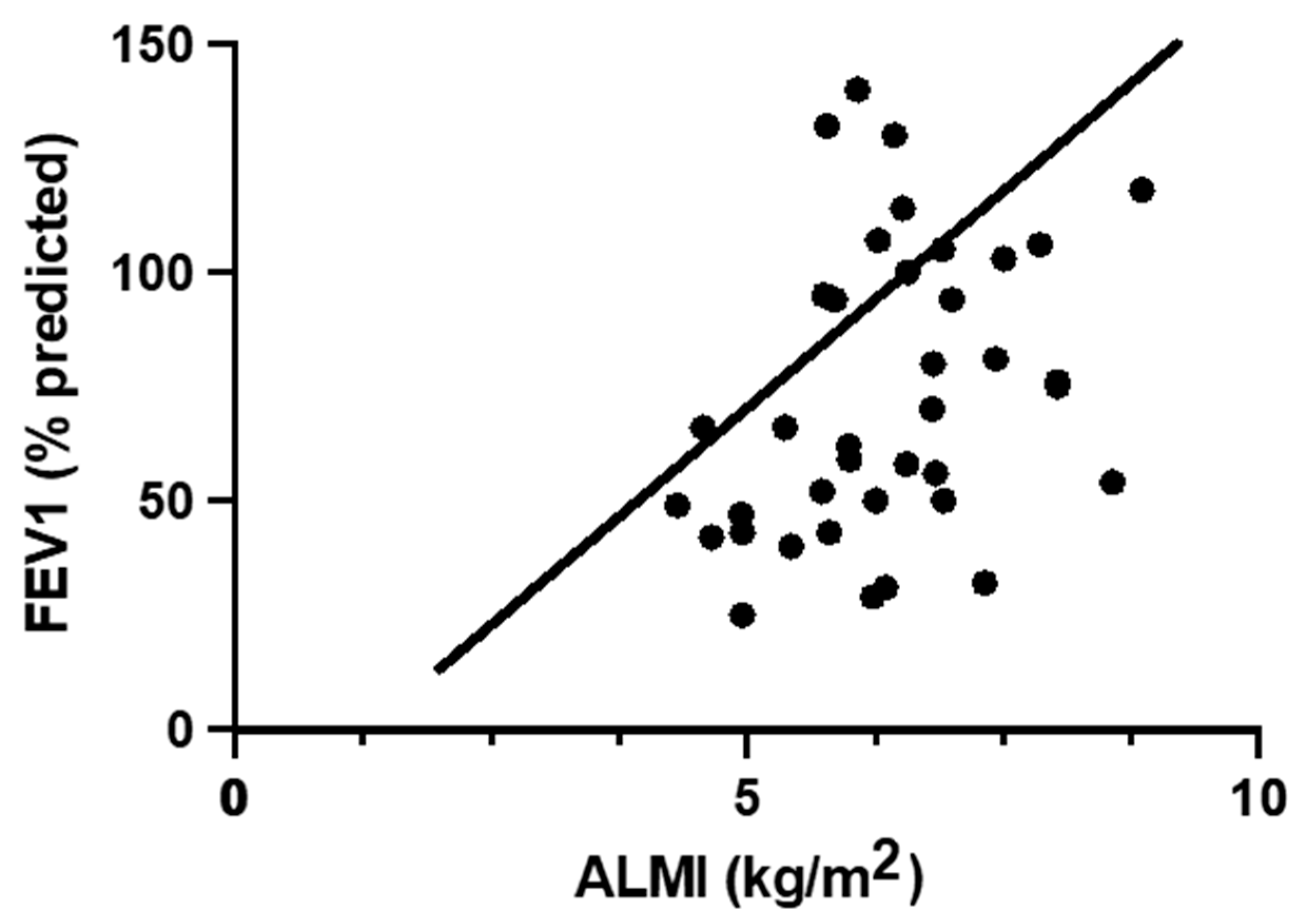
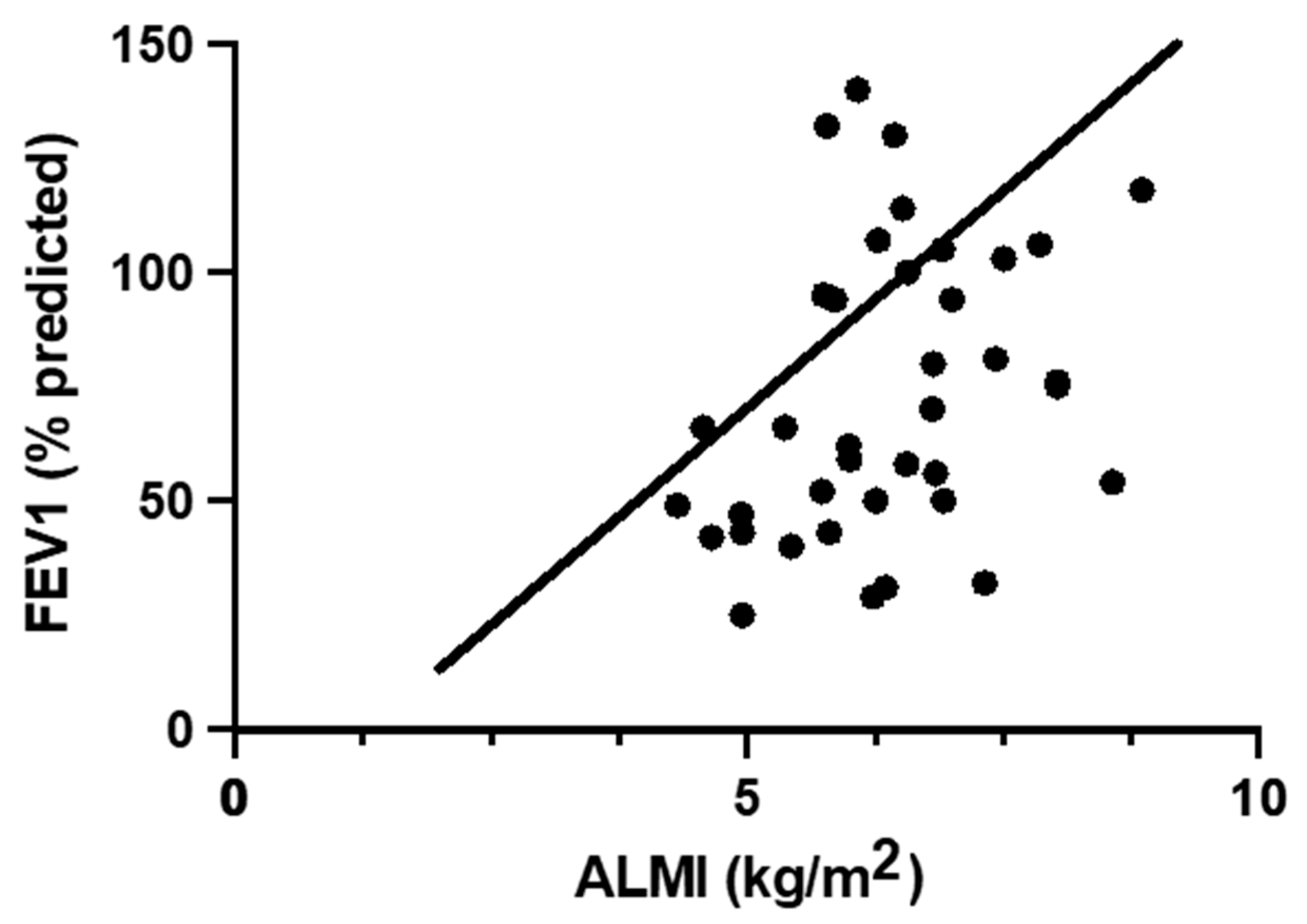
3.3. Relationship between Body Composition and Pulmonary Function in Participants with CF
3.4. Relationship of Body Composition with Dietary Intake and Physical Activity in Participants with CF
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moran, A.; Brunzell, C.; Cohen, R.C.; Katz, M.; Marshall, B.C.; Onady, G.; Robinson, K.A.; Sabadosa, K.A.; Stecenko, A.; Slovis, B.; et al. Clinical care guidelines for cystic fibrosis-related diabetes: A position statement of the American Diabetes Association and a clinical practice guideline of the Cystic Fibrosis Foundation, endorsed by the Pediatric Endocrine Society. Diabetes Care 2010, 33, 2697–2708. [Google Scholar] [CrossRef] [Green Version]
- Yen, E.H.; Quinton, H.; Borowitz, D. Better nutritional status in early childhood is associated with improved clinical outcomes and survival in patients with cystic fibrosis. J. Pediatr. 2013, 162, 530–535.e1. [Google Scholar] [CrossRef]
- Borowitz, D.; Baker, R.D.; Stallings, V. Consensus report on nutrition for pediatric patients with cystic fibrosis. J. Pediatr. Gastroenterol. Nutr. 2002, 35, 246–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morton, A.M. Symposium 6: Young people, artificial nutrition and transitional care the nutritional challenges of the young adult with cystic fibrosis: Transition. Proc. Nutr. Soc. 2009, 68, 430–440. [Google Scholar] [CrossRef] [Green Version]
- Calella, P.; Valerio, G.; Thomas, M.; McCabe, H.; Taylor, J.; Brodlie, M.; Siervo, M. Association between body composition and pulmonary function in children and young people with cystic fibrosis. Nutrition 2018, 48, 73–76. [Google Scholar] [CrossRef] [PubMed]
- McDonald, C.M.; Alvarez, J.A.; Bailey, J.; Bowser, E.K.; Farnham, K.; Mangus, M.; Padula, L.; Porco, K.; Rozga, M. Academy of Nutrition and Dietetics: 2020 Cystic Fibrosis Evidence Analysis Center Evidence-Based Nutrition Practice Guideline. J. Acad. Nutr. Diet. 2021, 121, 1591–1636.e3. [Google Scholar] [CrossRef] [PubMed]
- Culhane, S.; George, C.; Pearo, B.; Spoede, E. Malnutrition in cystic fibrosis: A review. Nutr. Clin. Pract. 2013, 28, 676–683. [Google Scholar] [CrossRef] [PubMed]
- Engelen, M.P.K.J.; Com, G.; Deutz, N.E.P. Protein is an important but undervalued macronutrient in the nutritional care of patients with cystic fibrosis. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 515–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellissimo, M.P.; Zhang, I.; Ivie, E.A.; Tran, P.H.; Tangpricha, V.; Hunt, W.R.; Stecenko, A.A.; Ziegler, T.R.; Alvarez, J.A. Visceral adipose tissue is associated with poor diet quality and higher fasting glucose in adults with cystic fibrosis. J. Cyst. Fibros. 2019, 18, 430–435. [Google Scholar] [CrossRef]
- Sutherland, R.; Katz, T.; Liu, V.; Quintano, J.; Brunner, R.; Tong, C.W.; Collins, C.E.; Ooi, C.Y. Dietary intake of energy-dense, nutrient-poor and nutrient-dense food sources in children with cystic fibrosis. J. Cyst. Fibros. 2018, 17, 804–810. [Google Scholar] [CrossRef]
- Calvo-Lerma, J.; Boon, M.; Hulst, J.; Colombo, C.; Asseiceira, I.; Garriga, M.; Masip, E.; Claes, I.; Bulfamante, A.; Janssens, H.M.; et al. Change in Nutrient and Dietary Intake in European Children with Cystic Fibrosis after a 6-Month Intervention with a Self-Management mHealth Tool. Nutrients 2021, 13, 1801. [Google Scholar] [CrossRef] [PubMed]
- Woestenenk, J.W.; Castelijns, S.J.A.M.; van der Ent, C.K.; Houwen, R.H.J. Dietary intake in children and adolescents with cystic fibrosis. Clin. Nutr. 2014, 33, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Panagopoulou, P.; Fotoulaki, M.; Nikolaou, A.; Nousia-Arvanitakis, S. Prevalence of malnutrition and obesity among cystic fibrosis patients. Pediatr. Int. 2014, 56, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Hanna, R.M.; Weiner, D.J. Overweight and obesity in patients with cystic fibrosis: A center-based analysis. Pediatr. Pulmonol. 2015, 50, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, A.L.; Mannik, L.A.; Walsh, S.; Brotherwood, M.; Robert, R.; Darling, P.B.; Nisenbaum, R.; Moerman, J.; Stanojevic, S. Longitudinal trends in nutritional status and the relation between lung function and BMI in cystic fibrosis: A population-based cohort study. Am. J. Clin. Nutr. 2013, 97, 872–877. [Google Scholar] [CrossRef] [Green Version]
- Harindhanavudhi, T.; Wang, Q.; Dunitz, J.; Moran, A.; Moheet, A. Prevalence and factors associated with overweight and obesity in adults with cystic fibrosis: A single-center analysis. J. Cyst. Fibros. 2020, 19, 139–145. [Google Scholar] [CrossRef] [Green Version]
- Guimbellot, J.S.; Baines, A.; Paynter, A.; Heltshe, S.L.; VanDalfsen, J.; Jain, M.; Rowe, S.M.; Sagel, S.D. Long term clinical effectiveness of ivacaftor in people with the G551D CFTR mutation. J. Cyst. Fibros. 2021, 20, 213–219. [Google Scholar] [CrossRef]
- Cystic Fibrosis Foundation. 2019 Patient Registry Annual Data Report; Cystic Fibrosis Foundation: Bethesda, MD, USA, 2019. [Google Scholar]
- Moran, A.; Pekow, P.; Grover, P.; Zorn, M.; Slovis, B.; Pilewski, J.; Tullis, E.; Liou, T.G.; Allen, H. Cystic Fibrosis Related Diabetes Therapy Study Group. Insulin therapy to improve BMI in cystic fibrosis-related diabetes without fasting hyperglycemia: Results of the cystic fibrosis related diabetes therapy trial. Diabetes Care 2009, 32, 1783–1788. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, J.A.; Ziegler, T.R.; Millson, E.C.; Stecenko, A.A. Body composition and lung function in cystic fibrosis and their association with adiposity and normal-weight obesity. Nutrition 2016, 32, 447–452. [Google Scholar] [CrossRef] [Green Version]
- Ritchie, H.; Nahikian-Nelms, M.; Roberts, K.; Gemma, S.; Shaikhkhalil, A. The prevalence of aberrations in body composition in pediatric cystic fibrosis patients and relationships with pulmonary function, bone mineral density, and hospitalizations. J. Cyst. Fibros. 2021, 20, 837–842. [Google Scholar] [CrossRef]
- Nevill, A.M.; Stewart, A.D.; Olds, T.; Holder, R. Relationship between adiposity and body size reveals limitations of BMI. Am. J. Phys. Anthropol. 2006, 129, 151–156. [Google Scholar] [CrossRef] [Green Version]
- King, S.J.; Nyulasi, I.B.; Strauss, B.J.G.; Kotsimbos, T.; Bailey, M.; Wilson, J.W. Fat-free mass depletion in cystic fibrosis: Associated with lung disease severity but poorly detected by body mass index. Nutrition 2010, 26, 753–759. [Google Scholar] [CrossRef]
- Sheikh, S.; Zemel, B.S.; Stallings, V.A.; Rubenstein, R.C.; Kelly, A. Body composition and pulmonary function in cystic fibrosis. Front. Pediatr. 2014, 2, 33. [Google Scholar] [CrossRef] [Green Version]
- Baker, J.F.; Putman, M.S.; Herlyn, K.; Tillotson, A.P.; Finkelstein, J.S.; Merkel, P.A. Body composition, lung function, and prevalent and progressive bone deficits among adults with cystic fibrosis. Jt. Bone Spine 2016, 83, 207–211. [Google Scholar] [CrossRef]
- King, S.J.; Tierney, A.C.; Edgeworth, D.; Keating, D.; Williams, E.; Kotsimbos, T.; Button, B.M.; Wilson, J.W. Body composition and weight changes after ivacaftor treatment in adults with cystic fibrosis carrying the G551 D cystic fibrosis transmembrane conductance regulator mutation: A double-blind, placebo-controlled, randomized, crossover study with open-label extension. Nutrition 2021, 85, 111124. [Google Scholar]
- Putman, M.S.; Greenblatt, L.B.; Bruce, M.; Joseph, T.; Lee, H.; Sawicki, G.; Uluer, A.; Sicilian, L.; Neuringer, I.; Gordon, C.M.; et al. The Effects of Ivacaftor on Bone Density and Microarchitecture in Children and Adults with Cystic Fibrosis. J. Clin. Endocrinol. Metab. 2021, 106, E1248–E1261. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Augustin, L.S.A.; Kendall, C.W.C.; Jenkins, D.J.A.; Willett, W.C.; Astrup, A.; Barclay, A.W.; Björck, I.; Brand-Miller, J.C.; Brighenti, F.; Buyken, A.E.; et al. Glycemic index, glycemic load and glycemic response: An International Scientific Consensus Summit from the International Carbohydrate Quality Consortium (ICQC). Nutr. Metab. Cardiovasc. Dis. 2015, 25, 795–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sievert, Y.A.; Schakel, S.F.; Buzzard, I.M. Maintenance of a nutrient database for clinical trials. Control. Clin. Trials 1989, 10, 416–425. [Google Scholar] [CrossRef]
- Kriska, A.M.; Bennett, P.H. An epidemiological perspective of the relationship between physical activity and NIDDM: From activity assessment to intervention. Diabetes. Metab. Rev. 1992, 8, 355–372. [Google Scholar] [CrossRef]
- Madeira, F.B.; Silva, A.A.; Veloso, H.F.; Goldani, M.Z.; Kac, G.; Cardoso, V.C.; Bettiol, H.; Barbieri, M.A. Normal weight obesity is associated with metabolic syndrome and insulin resistance in young adults from a middle-income country. PLoS ONE 2013, 8, e60673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunout, D.; de la Maza, M.P.; Barrera, G.; Leiva, L.; Hirsch, S. Association between sarcopenia and mortality in healthy older people. Australas. J. Ageing 2011, 30, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Alicandro, G.; Bisogno, A.; Battezzati, A.; Bianchi, M.L.; Corti, F.; Colombo, C. Recurrent pulmonary exacerbations are associated with low fat free mass and low bone mineral density in young adults with cystic fibrosis. J. Cyst. Fibros. 2014, 13, 328–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaisman, N.; Pencharz, P.B.; Corey, M.; Canny, G.J.; Hahn, E. Energy expenditure of patients with cystic fibrosis. J. Pediatr. 1987, 111, 496–500. [Google Scholar] [CrossRef]
- Turck, D.; Braegger, C.P.; Colombo, C.; Declercq, D.; Morton, A.; Pancheva, R.; Robberecht, E.; Stern, M.; Strandvik, B.; Wolfe, S.; et al. ESPEN-ESPGHAN-ECFS guidelines on nutrition care for infants, children, and adults with cystic fibrosis. Clin. Nutr. 2016, 35, 557–577. [Google Scholar] [CrossRef] [Green Version]
- Matel, J.L. Nutritional Management of Cystic Fibrosis. J. Parenter. Enter. Nutr. 2012, 36 (Suppl. 1), 60S–67S. [Google Scholar] [CrossRef]
- Gaskin, K.J. Nutritional care in children with cystic fibrosis: Are our patients becoming better? Eur. J. Clin. Nutr. 2013, 67, 558–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prévotat, A.; Godin, J.; Bernard, H.; Perez, T.; Le Rouzic, O.; Wallaert, B. Improvement in body composition following a supervised exercise-training program of adult patients with cystic fibrosis. Respir. Med. Res. 2019, 75, 5–9. [Google Scholar] [CrossRef]
- Papalexopoulou, N.; Dassios, T.G.; Lunt, A.; Bartlett, F.; Perrin, F.; Bossley, C.J.; Wyatt, H.A.; Greenough, A. Nutritional status and pulmonary outcome in children and young people with cystic fibrosis. Respir. Med. 2018, 142, 60–65. [Google Scholar] [CrossRef]
- Fielding, J.; Brantley, L.; Seigler, N.; McKie, K.T.; Davison, G.W.; Harris, R.A. Oxygen uptake kinetics and exercise capacity in children with cystic fibrosis. Pediatr. Pulmonol. 2015, 50, 647–654. [Google Scholar] [CrossRef]

{kind=link}
| CF (n = 38) | Healthy Volunteers (n = 19) | p-Value | |
|---|---|---|---|
| Age (years) | 27.9 ± 2.0 | 28.8 ± 2.7 | 0.796 |
| Female, n (%) | 20 (52.6%) | 10 (52.6%) | |
| Race, n (%) | |||
| White | 38 (100%) | 19 (100%) | |
| Black | |||
| Asian | |||
| Native Haqaiian or Pacific Islander | |||
| American Indian or Alaskan Native | |||
| Ethnicity, n (%) | |||
| Hispanic | 0 (0%) | 0 (0%) | |
| Non-Hispanic | 38 (100%) | 38 (100%) | |
| Height (cm) | 166.9 ± 1.5 | 170.3 ± 1.9 | 0.185 |
| Weight (kg) | 59.6 ± 1.9 | 64.4 ± 2.6 | 0.154 |
| BMI (kg/m2) | 21.4 ± 0.6 | 22.1 ± 0.5 | 0.447 |
| HOMA-IR | 1.2 ± 0.1 | 1.0 ± 0.1 | 0.455 |
| Physical Activity Score | 22.3 ± 2.8 | 16.4 ± 2.6 | 0.311 |
| Genotype, n (%) | |||
| F508del homozygous | 7 (18.4%) | ||
| F508del heterozygous | 20 (52.6%) | ||
| Other | 11 (28.9%) | ||
| Pancreatic insufficiency, n (%) | 30 (78.9%) | ||
| FEV1 (% predicted) | 73 ± 5 | ||
| CFRD, n (%) | 5 (13.2%) | ||
| CF Exacerbations in the past prior year (Y/N) | 25 (65.8%) | ||
| Number of CF Exacerbations in the prior year | 1.5 ± 0.25 | ||
| Glucocorticoid Use in the prior year | 15 (39.5%) | ||
| Ivacaftor Use, n (%) | 10 (26.3%) |
| CF (n = 38) | Healthy Volunteers (n = 19) | p-Value | |
|---|---|---|---|
| Body Composition | |||
| Fat mass (g) | 15,740 ± 1119 | 16,687 ± 898 | 0.097 |
| Lean mass (g) | 42,438 ± 1301 | 46,109 ± 2593 | 0.352 |
| Total mass (g) | 60,274 ± 1940 | 65,163 ± 2611 | 0.07 |
| % fat | 25.6 ± 1.2 | 26.2 ± 1.7 | 0.778 |
| Trunk fat mass (g) | 7051 ± 646 | 6709 ± 426 | 0.294 |
| Trunk total mass (g) | 30,267 ± 1111 | 30,330 ± 1299 | 0.618 |
| Trunk % fat | 22.3 ± 1.3 | 22.4 ± 1.3 | 0.52 |
| Fat mass/height2 (kg/m2) | 5.8 ± 0.4 | 5.9 ± 0.4 | 0.275 |
| Lean/height2 (kg/m2) | 15.9 ± 0.4 | 16.4 ± 0.6 | 0.481 |
| Appen lean/height2 (kg/m2) | 6.4 ± 0.2 | 7.2 ± 0.4 | 0.029 |
| Dietary intake | |||
| Energy (kcal) | 2880 ± 258 | 2203 ± 196 | 0.137 |
| Total Fat (g) | 118.8 ± 11.7 | 74.8 ± 8 | 0.016 |
| Total Carb (g) | 362.6 ± 34.4 | 292 ± 22.3 | 0.418 |
| Total Protein (g) | 104 ± 10.2 | 96.5 ± 11.4 | 0.667 |
| Cholesterol (mg) | 313.9 ± 42.9 | 248.3 ± 26.9 | 0.569 |
| % Calories from Fat | 36.5 ± 1.6 | 29.3 ± 1.3 | 0.002 |
| % Calories from Carbohydrates | 48.5 ± 1.8 | 52.8 ± 1.4 | 0.092 |
| % Calories from Protein | 14.9 ± 0.8 | 17.2 ± 0.8 | 0.015 |
| Added Sugar (g) | 120.6 ± 17.5 | 66.7 ± 6.2 | 0.142 |
| Glycemic Index | 61.4 ± 1.2 | 57.7 ± 1.1 | 0.036 |
| Glycemic Load | 213.1 ± 22 | 154.1 ± 11.6 | 0.131 |
| % Predicted FEV1 | ||||||
|---|---|---|---|---|---|---|
| r | p-Value | Model 1 Beta Coefficient | p-Value | Model 2 Beta Coefficient | p-Value | |
| Fat mass (g) | 0.174 | 0.296 | 0.0004 ± 0.0009 | 0.656 | −0.003 ± 0.002 | 0.051 |
| Lean mass (g) | 0.194 | 0.243 | 0.003 ± 0.001 | 0.001 | 0.003 ± 0.001 | 0.003 |
| % fat | 0.065 | 0.7 | −1.12 ± 0.992 | 0.263 | −4.066 ± 0.1.121 | 0.001 |
| Trunk fat mass (g) | 0.157 | 0.348 | 0.001 ± 0.002 | 0.513 | −0.005 ± 0.003 | 0.111 |
| Trunk total mass (g) | 0.265 | 0.108 | 0.002 ± 0.001 | 0.072 | 0.001 ± 0.002 | 0.451 |
| Trunk % fat | 0.081 | 0.629 | −0.259 ± 0.87 | 0.768 | −3.206 ± 1.184 | 0.011 |
| FMI (kg/m2) | 0.171 | 0.305 | −0.141 ± 2.35 | 0.953 | −14.684 ± 3.931 | 0.001 |
| LMI (kg/m2) | 0.264 | 0.11 | 5.242 ± 2.325 | 0.031 | 4.839 ± 3.459 | 0.171 |
| ALMI (kg/m2) | 0.332 | 0.042 | 15.021 ± 4.45 | 0.002 | 18.972 ± 6.542 | 0.007 |
| BMI (kg/m2) | 0.405 | 0.012 | 2.574 ± 1.505 | 0.096 | ||
| Energy (kcal) | Total Fat (g) | Total Carb (g) | Total Protein (g) | % Cal Fat | % Cal Carb | % Cal Protein | Added Sugars (g) | GI (Glucose) | GL (Glucose) | Physical Activity | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Fat mass (g) | −0.533 (0.002) | −0.498 (0.004) | −0.445 (0.012) | −0.508 (0.004) | 0.091 (0.626) | −0.104 (0.576) | 0.096 (0.608) | −0.354 (0.051) | −0.036 (0.846) | −0.445 (0.012) | −0.469 (0.003) |
| Lean mass (g) | 0.181 (0.331) | 0.194 (0.296) | 0.073 (0.696) | 0.277 (0.131) | 0.248 (0.179) | −0.26 (0.158) | 0.161 (0.389) | 0.005 (0.979) | −0.024 (0.9) | 0.072 (0.70) | 0.304 (0.068) |
| % fat | −0.679 (<0.0001) | −0.621 (0.0002) | −0.512 (0.003) | −0.705 (<0.0001) | −0.041 (0.827) | 0.084 (0.653) | 0.015 (0.936) | −0.409 (0.022) | −0.024 (0.898) | −0.481 (0.006) | −0.55 (0.0004) |
| Trunk fat mass (g) | −0.54 (0.002) | −0.504 (0.004) | −0.443 (0.013) | −0.536 (0.002) | 0.084 (0.655) | −0.08 (0.668) | 0.017 (0.928) | −0.334 (0.066) | −0.057 (0.763) | −0.451 (0.011) | −0.457 (0.005) |
| Trunk % fat | −0.65 (0.0001) | −0.618 (0.0002) | −0.512 (0.003) | −0.684 (<0.0001) | 0.016 (0.931) | −0.009 (0.962) | −0.02 (0.916) | −0.349 (0.054) | −0.035 (0.853) | −0.508 (0.004) | −0.532 (0.0007) |
| FMI (kg/m2) | −0.626 (0.0002) | −0.567 (0.0009) | −0.525 (0.002) | −0.623 (0.0002) | 0.097 (0.605) | −0.097 (0.604) | 0.049 (0.794) | −0.409 (0.022) | −0.051 (0.784) | −0.517 (0.003) | −0.51 (0.001) |
| LMI (kg/m2) | −0.135 (0.469) | −0.099 (0.595) | −0.223 (0.228) | 0.012 (0.949) | 0.192 (0.301) | −0.271 (0.14) | 0.259 (0.159) | −0.196 (0.292) | −0.156 (0.403) | −0.228 (0.219) | 0.225 (0.181) |
| ALMI (kg/m2) | 0.004 (0.984) | 0.063 (0.737) | −0.029 (0.878) | 0.153 (0.41) | 0.206 (0.266) | −0.288 (0.116) | 0.232 (0.209) | −0.062 (0.742) | −0.113 (0.546) | −0.043 (0.819) | 0.367 (0.025) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scully, K.J.; Jay, L.T.; Freedman, S.; Sawicki, G.S.; Uluer, A.; Finkelstein, J.S.; Putman, M.S. The Relationship between Body Composition, Dietary Intake, Physical Activity, and Pulmonary Status in Adolescents and Adults with Cystic Fibrosis. Nutrients 2022, 14, 310. https://doi.org/10.3390/nu14020310
Scully KJ, Jay LT, Freedman S, Sawicki GS, Uluer A, Finkelstein JS, Putman MS. The Relationship between Body Composition, Dietary Intake, Physical Activity, and Pulmonary Status in Adolescents and Adults with Cystic Fibrosis. Nutrients. 2022; 14(2):310. https://doi.org/10.3390/nu14020310
Chicago/Turabian StyleScully, Kevin J., Laura T. Jay, Steven Freedman, Gregory S. Sawicki, Ahmet Uluer, Joel S. Finkelstein, and Melissa S. Putman. 2022. "The Relationship between Body Composition, Dietary Intake, Physical Activity, and Pulmonary Status in Adolescents and Adults with Cystic Fibrosis" Nutrients 14, no. 2: 310. https://doi.org/10.3390/nu14020310
APA StyleScully, K. J., Jay, L. T., Freedman, S., Sawicki, G. S., Uluer, A., Finkelstein, J. S., & Putman, M. S. (2022). The Relationship between Body Composition, Dietary Intake, Physical Activity, and Pulmonary Status in Adolescents and Adults with Cystic Fibrosis. Nutrients, 14(2), 310. https://doi.org/10.3390/nu14020310