Awareness, Knowledge and Attitude towards ‘Superfood’ Kale and Its Health Benefits among Arab Adults

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Questionnaire
- The first section asked about the participants’ socio-demographic information, which included age, sex, marital status, family income, educational qualification, etc.
- In the second section, 13 questions, which determined the kale nutritional value knowledge among Saudi adults, were asked to the study participants. The questions included information about kale being a food with high calorie content, with high nutritional value, with immune boosting properties, rich in fiber, rich in vitamin C, and low in fats. This section also included questions about benefits of kale consumption in health conditions such as constipation, digestive problems, cancer, inflammation, oxidative stress, and chronic diseases. The study participants were also asked whether or not cooking kale decreases its nutritional and health benefits.
- In the final portion, research participants were asked if they had ever consumed kale previously, and if so, what positive or negative health impacts they experienced. The questions included information about how many times a week the participants were consuming kale and if there were any health effects, such as weight loss, decrease in appetite, improved bowel movements, etc., felt by the participants during this time, or if they experienced any side effects, such as constipation, bloating, bowel irritability, etc. Additionally, the mode of consumption of kale was also asked in this section, such as consumed fresh, cooked, as supplements, or as the commercially available powdered form.
2.3. Data Analysis
3. Results
3.1. Characteristics of the Study Participants
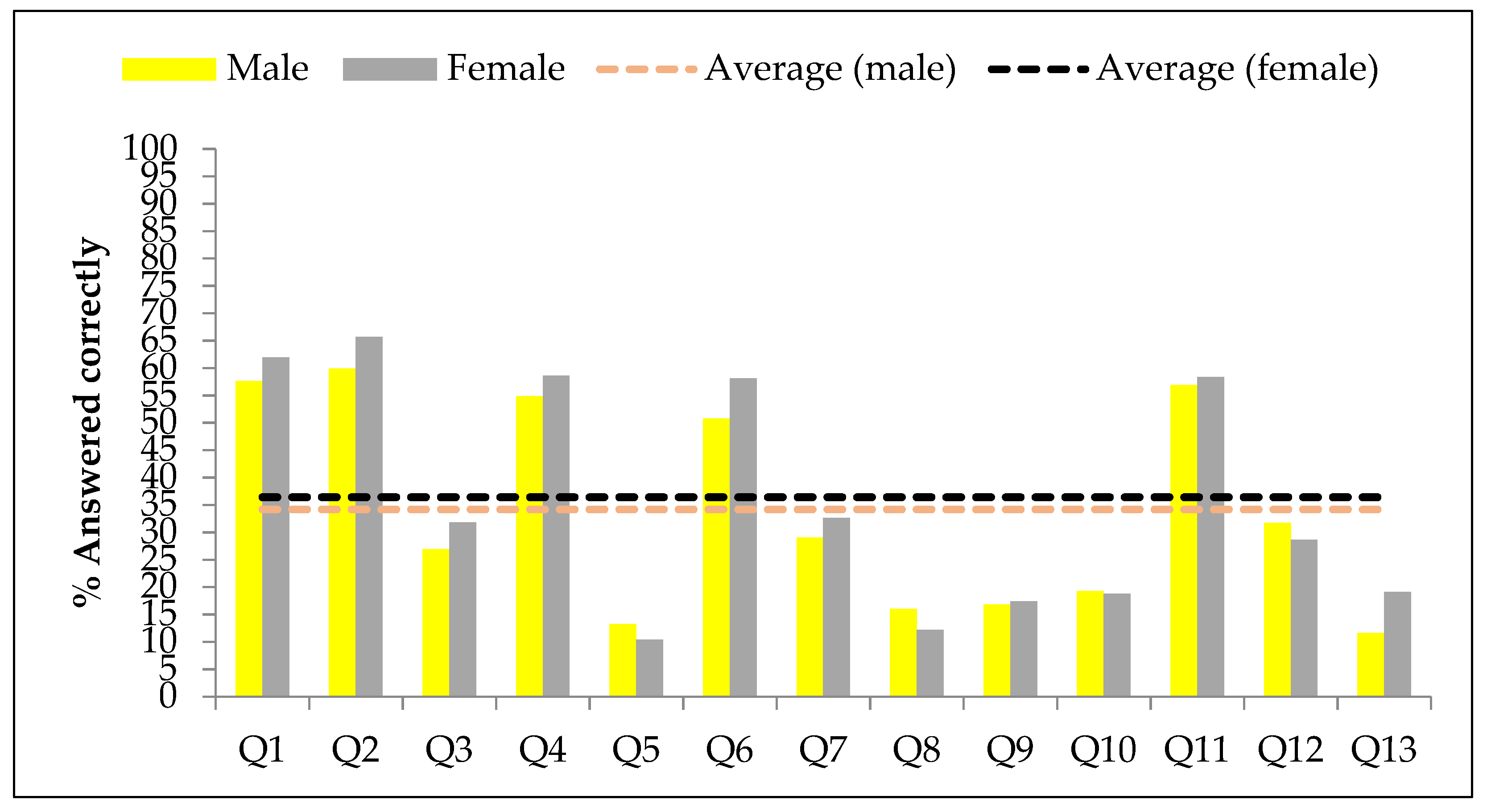
3.2. Knowledge about Benefits of Kale Consumption in the Study Participants
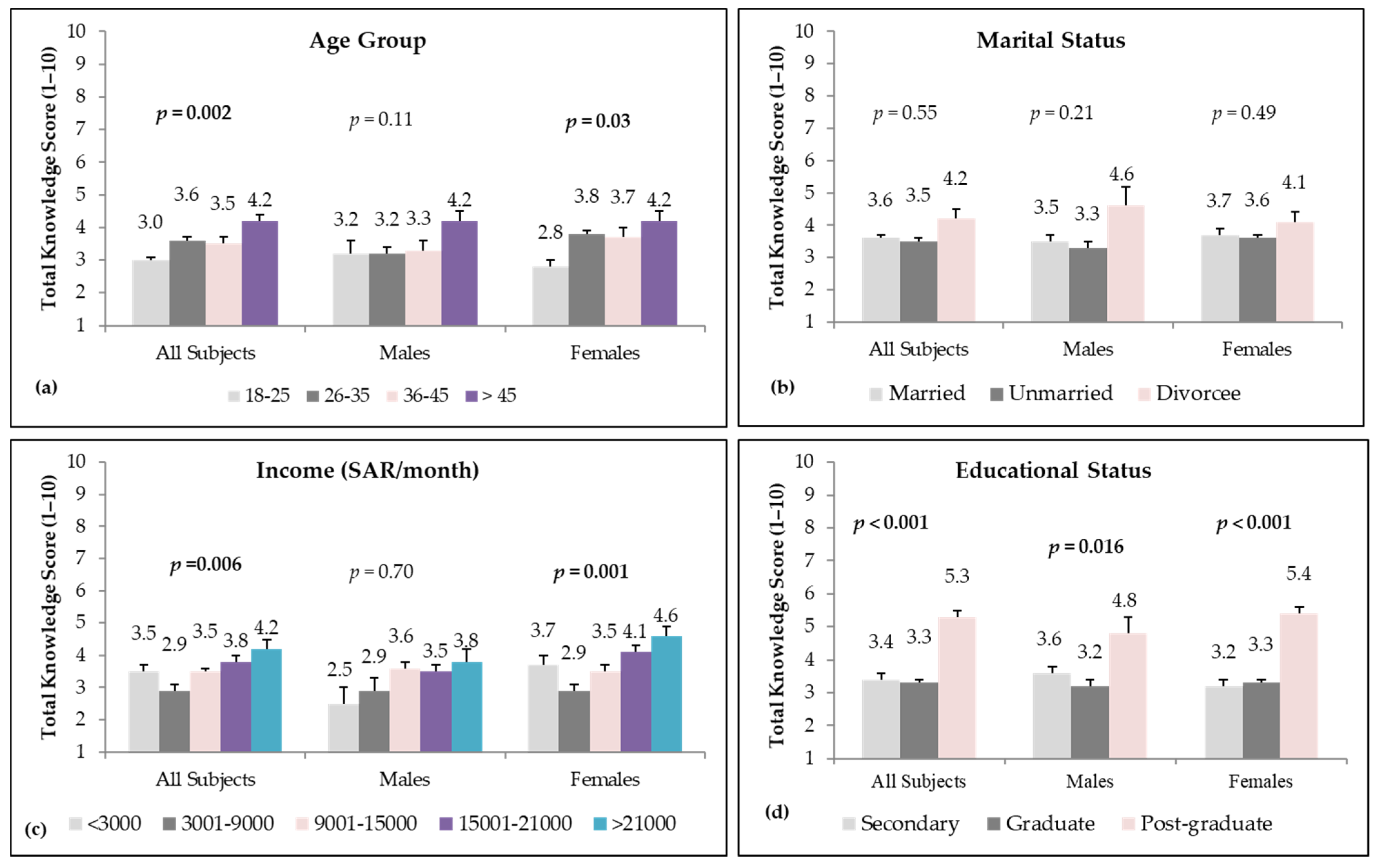
3.3. Kale Knowledge Score in Study Participants Divided as Per Socio-Demographic Variables
3.4. Consumption of Kale in Study Participants and Its Health Effects
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Overweight and Obesity 2020. Available online: https://www.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-asia-pacific-2020_a47d0cd2-en (accessed on 25 May 2021).
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [Green Version]
- Malhotra, A.; Noakes, T.; Phinney, S. It is time to bust the myth of physical inactivity and obesity: You cannot outrun a bad diet. Br. J. Sports Med. 2015, 49, 967–968. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.-C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The un decade of nutrition, the nova food classification and the trouble with ultra-processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronto, R.; Wu, J.H.; Singh, G.M. The global nutrition transition: Trends, disease burdens and policy interventions. Public Health Nutr. 2018, 21, 2267–2270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habib, S.H.; Saha, S. Burden of non-communicable disease: Global overview. Diabetes Metab. Syndr. Clin. Res. Rev. 2010, 4, 41–47. [Google Scholar] [CrossRef]
- Martinez, R.; Lloyd-Sherlock, P.; Soliz, P.; Ebrahim, S.; Vega, E.; Ordunez, P.; McKee, M. Trends in premature avertable mortality from non-communicable diseases for 195 countries and territories, 1990–2017: A population-based study. Lancet Glob. Health 2020, 8, e511–e523. [Google Scholar] [CrossRef] [Green Version]
- Al-Daghri, N.M.; Alkharfy, K.M.; Al-Othman, A.; Yakout, S.M.; Al-Saleh, Y.; Fouda, M.; Sabico, S. Effect of non-pharmacologic vitamin D status correction on circulating bone markers in healthy overweight and obese Saudis. Molecules 2013, 18, 10671–10680. [Google Scholar] [CrossRef] [Green Version]
- Al-Daghri, N.M.; Kumar, S.; Chrousos, G.; Alkharfy, K.; Al-Saleh, Y.; Al-Attas, O.; Alokail, M.; El-Kholie, E.; Yousef, M.; Al-Othman, A.M.; et al. Vitamin d supplementation is recommended during summer season in the gulf region: The counterintuitive seasonal effect in vitamin d levels of adult, overweight middle-eastern residents. Clin. Endocrinol. 2012, 76, 346–350. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Alkharfy, K.M.; Al-Saleh, Y.; Al-Attas, O.S.; Alokail, M.S.; Al-Othman, A.; Moharram, O.; El-Kholie, E.; Sabico, S.; Kumar, S. Modest reversal of metabolic syndrome manifestations with vitamin d status correction: A 12-month prospective study. Metabolism 2012, 61, 661–666. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Alfawaz, H.; Aljohani, N.J.; Al-Saleh, Y.; Wani, K.; Alnaami, A.M.; Alharbi, M.; Kumar, S. A 6-month “self-monitoring” lifestyle modification with increased sunlight exposure modestly improves vitamin d status, lipid profile and glycemic status in overweight and obese saudi adults with varying glycemic levels. Lipids Health Dis. 2014, 13, 87. [Google Scholar] [CrossRef] [Green Version]
- Alfawaz, H.A.; Wani, K.; Alnaami, A.M.; Al-Saleh, Y.; Aljohani, N.J.; Al-Attas, O.S.; Alokail, M.S.; Kumar, S.; Al-Daghri, N.M. Effects of different dietary and lifestyle modification therapies on metabolic syndrome in prediabetic Arab patients: A 12-month longitudinal study. Nutrients 2018, 10, 383. [Google Scholar] [CrossRef] [Green Version]
- Wani, K.; Alfawaz, H.; Alnaami, A.M.; Sabico, S.; Khattak, M.N.K.; Al-Attas, O.; Alokail, M.S.; Alharbi, M.; Chrousos, G.; Kumar, S.; et al. Effects of a 12-month intensive lifestyle monitoring program in predominantly overweight/obese arab adults with prediabetes. Nutrients 2020, 12, 464. [Google Scholar] [CrossRef] [Green Version]
- Naeem, Z. Increasing trend of junk food use in saudi arabia and health implications. Int. J. Health Sci. (Qassim) 2012, 6, V–VI. [Google Scholar] [CrossRef]
- Benajiba, N. Fast food intake among saudi population: Alarming fact. Am. J. Food Nutr. 2016, 6, 44–48. [Google Scholar]
- Khan, M.U.K. Hidden hunger, a global health problem. Community Based Med. J. 2015, 4, 1–2. [Google Scholar] [CrossRef]
- Burchi, F.; Fanzo, J.; Frison, E. The role of food and nutrition system approaches in tackling hidden hunger. Int. J. Environ. Res. Public Health 2011, 8, 358–373. [Google Scholar] [CrossRef] [PubMed]
- Alfawaz, H.; Naeef, A.F.; Wani, K.; Khattak, M.N.K.; Sabico, S.; Alnaami, A.M.; Al-Daghri, N.M. Improvements in glycemic, micronutrient, and mineral indices in arab adults with pre-diabetes post-lifestyle modification program. Nutrients 2019, 11, 2775. [Google Scholar] [CrossRef] [Green Version]
- Caballero, B.; Trugo, L.C.; Finglas, P.M. Encyclopedia of Food Sciences and Nutrition, Food and Agriculture Organizationof the United Nations, Academic 2003. Available online: https://agris.fao.org/agris-search/search.do?recordID=US201300082710 (accessed on 25 June 2021).
- Maggioni, L.; von Bothmer, R.; Poulsen, G.; Branca, F. Origin and domestication of cole crops (Brassica oleracea L.): Linguistic and literary considerations 1. Econ. Bot. 2010, 64, 109–123. [Google Scholar] [CrossRef]
- Cernansky, R. Super vegetables: Long overlooked in parts of africa, indigenous greens are now capturing attention for their nutritional and environmental benefits. Nature 2015, 522, 149–152. [Google Scholar]
- Aires, A. Brassica composition and food processing. In Processing and Impact on Active Components in Food; Elsevier: Amsterdam, The Netherlands, 2015; pp. 17–25. [Google Scholar]
- Kim, M.J.; Chiu, Y.-C.; Ku, K.-M. Glucosinolates, carotenoids, and vitamins e and k variation from selected kale and collard cultivars. J. Food Qual. 2017, 2017. [Google Scholar] [CrossRef] [Green Version]
- Bowden, J. The 150 Healthiest Foods on Earth, Revised Edition: The Surprising, Unbiased Truth about what You Should Eat and Why; Fair Winds Press: Beverly, MA, USA , 2017. [Google Scholar]
- Awuchi, C.G.; Igwe, V.S.; Amagwula, I.O. Nutritional diseases and nutrient toxicities: A systematic review of the diets and nutrition for prevention and treatment. Int. J. Adv. Acad. Res. 2020, 6, 1–46. [Google Scholar] [CrossRef]
- Lee, H.-J.; Han, J.-H.; Park, Y.K.; Kang, M.-H. Effects of glutathione s-transferase (gst) m1 and t1 polymorphisms on antioxidant vitamins and oxidative stress-related parameters in korean subclinical hypertensive subjects after kale juice (Brassica oleracea acephala) supplementation. Nutr. Res. Pract. 2018, 12, 118–128. [Google Scholar] [CrossRef] [Green Version]
- Charron, C.S.; Novotny, J.A.; Jeffery, E.H.; Kramer, M.; Ross, S.A.; Seifried, H.E. Consumption of baby kale increased cytochrome p450 1a2 (cyp1a2) activity and influenced bilirubin metabolism in a randomized clinical trial. J. Funct. Foods 2020, 64, 103624. [Google Scholar] [CrossRef]
- Thavarajah, P.; Abare, A.; Basnagala, S.; Lacher, C.; Smith, P.; Combs, G.F., Jr. Mineral micronutrient and prebiotic carbohydrate profiles of USA-grown kale (Brassica oleracea L. Var. Acephala). J. Food Compos. Anal. 2016, 52, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Al-Daghri, N.M.; Al-Attas, O.S.; Alokail, M.; Alkharfy, K.; Wani, K.; Amer, O.E.; Ul Haq, S.; Rahman, S.; Alnaami, A.M.; Livadas, S.; et al. Does visceral adiposity index signify early metabolic risk in children and adolescents?: Association with insulin resistance, adipokines, and subclinical inflammation. Pediatr Res. 2014, 75, 459–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Daghri, N.M.; Al-Attas, O.S.; Alokail, M.S.; Alkharfy, K.M.; Yousef, M.; Sabico, S.L.; Chrousos, G.P. Diabetes mellitus type 2 and other chronic non-communicable diseases in the central region, saudi arabia (riyadh cohort 2): A decade of an epidemic. BMC Med. 2011, 9, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Daghri, N.M.; Khan, N.; Alkharfy, K.M.; Al-Attas, O.S.; Alokail, M.S.; Alfawaz, H.A.; Alothman, A.; Vanhoutte, P.M. Selected dietary nutrients and the prevalence of metabolic syndrome in adult males and females in saudi arabia: A pilot study. Nutrients 2013, 5, 4587–4604. [Google Scholar] [CrossRef] [Green Version]
- Hwalla, N.; Al Dhaheri, A.S.; Radwan, H.; Alfawaz, H.A.; Fouda, M.A.; Al-Daghri, N.M.; Zaghloul, S.; Blumberg, J.B. The prevalence of micronutrient deficiencies and inadequacies in the middle east and approaches to interventions. Nutrients 2017, 9, 229. [Google Scholar] [CrossRef]
- Reda, T.; Thavarajah, P.; Polomski, R.; Bridges, W.; Shipe, E.; Thavarajah, D. Reaching the highest shelf: A review of organic production, nutritional quality, and shelf life of kale (Brassica oleracea var. Acephala). Plants People Planet 2021, 3, 308–318. [Google Scholar] [CrossRef]
- Food Survey Research Group. Food and Nutrient Database for Dietary Studies, United States Department of Agriculture. Available online: https://ndb.nal.usda.gov/ndb/ (accessed on 6 September 2021).
- Wibowo, S.; Afuape, A.L.; De Man, S.; Bernaert, N.; Van Droogenbroeck, B.; Grauwet, T.; Van Loey, A.; Hendrickx, M. Thermal processing of kale purée: The impact of process intensity and storage on different quality related aspects. Innov. Food Sci. Emerg. Technol. 2019, 58, 102213. [Google Scholar] [CrossRef]
- Deng, M.; Qian, H.; Chen, L.; Sun, B.; Chang, J.; Miao, H.; Cai, C.; Wang, Q. Influence of pre-harvest red light irradiation on main phytochemicals and antioxidant activity of chinese kale sprouts. Food Chem. 2017, 222, 1–5. [Google Scholar] [CrossRef]
- Alpers, D.H. Subclinical micronutrient deficiency: A problem in recognition. Curr. Opin. Gastroenterol. 2012, 28, 135–138. [Google Scholar] [CrossRef]
- Gödecke, T.; Stein, A.J.; Qaim, M. The global burden of chronic and hidden hunger: Trends and determinants. Glob. Food Secur. 2018, 17, 21–29. [Google Scholar] [CrossRef]
- Šamec, D.; Urlić, B.; Salopek-Sondi, B. Kale (Brassica oleracea var. Acephala) as a superfood: Review of the scientific evidence behind the statement. Crit. Rev. Food Sci. Nutr. 2019, 59, 2411–2422. [Google Scholar] [CrossRef]
- Ayaz, F.A.; Glew, R.H.; Millson, M.; Huang, H.; Chuang, L.; Sanz, C.; Hayırlıoglu-Ayaz, S. Nutrient contents of kale (Brassica oleraceae l. Var. Acephala dc.). Food Chem. 2006, 96, 572–579. [Google Scholar] [CrossRef]
- Jahangir, M.; Kim, H.K.; Choi, Y.H.; Verpoorte, R. Health-affecting compounds in brassicaceae. Compr. Rev. Food Sci. Food Saf. 2009, 8, 31–43. [Google Scholar] [CrossRef]
- Korus, A.; Lisiewska, Z. Effect of preliminary processing and method of preservation on the content of selected antioxidative compounds in kale (Brassica oleracea l. Var. Acephala) leaves. Food Chem. 2011, 129, 149–154. [Google Scholar] [CrossRef]
- Becerra-Moreno, A.; Alanís-Garza, P.A.; Mora-Nieves, J.L.; Mora-Mora, J.P.; Jacobo-Velázquez, D.A. Kale: An excellent source of vitamin c, pro-vitamin a, lutein and glucosinolates. CyTA-J. Food 2014, 12, 298–303. [Google Scholar] [CrossRef]
- Prakash, D.; Gupta, C. Glucosinolates: The phytochemicals of nutraceutical importance. J. Complement. Integr. Med. 2012, 9. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, Á.L.M.; Lemos, M.; Niero, R.; de Andrade, S.F.; Maistro, E.L. Evaluation of the genotoxic and antigenotoxic potential of Brassica oleracea l. Var. Acephala dc in different cells of mice. J. Ethnopharmacol. 2012, 143, 740–745. [Google Scholar] [CrossRef]
- Olsen, H.; Grimmer, S.; Aaby, K.; Saha, S.; Borge, G.I.A. Antiproliferative effects of fresh and thermal processed green and red cultivars of curly kale (Brassica oleracea L. Convar. Acephala var. Sabellica). J. Agric. Food Chem. 2012, 60, 7375–7383. [Google Scholar] [CrossRef]
- Fahey, J.W.; Stephenson, K.K.; Wade, K.L.; Talalay, P. Urease from helicobacter pylori is inactivated by sulforaphane and other isothiocyanates. Biochem. Biophys. Res. Commun. 2013, 435, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Walker, A.W.; Ince, J.; Duncan, S.H.; Webster, L.M.; Holtrop, G.; Ze, X.; Brown, D.; Stares, M.D.; Scott, P.; Bergerat, A. Dominant and diet-responsive groups of bacteria within the human colonic microbiota. ISME J. 2011, 5, 220–230. [Google Scholar] [CrossRef]
- Mandoura, N.; Al-Raddadi, R.; Abdulrashid, O.; Shah, H.B.U.; Kassar, S.M.; Hawari, A.R.A.; Jahhaf, J.M. Factors associated with consuming junk food among saudi adults in jeddah city. Cureus 2017, 9, e2008. [Google Scholar] [CrossRef] [Green Version]
- ALFaris, N.A.; Al-Tamimi, J.Z.; Al-Jobair, M.O.; Al-Shwaiyat, N.M. Trends of fast food consumption among adolescent and young adult saudi girls living in riyadh. Food Nutr. Res. 2015, 59, 26488. [Google Scholar] [CrossRef] [Green Version]
- Moradi-Lakeh, M.; El Bcheraoui, C.; Afshin, A.; Daoud, F.; AlMazroa, M.A.; Al Saeedi, M.; Basulaiman, M.; Memish, Z.A.; Al Rabeeah, A.A.; Mokdad, A.H. Diet in saudi arabia: Findings from a nationally representative survey. Public Health Nutr. 2017, 20, 1075–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, L.; Alicandro, G.; Bertuccio, P.; La Vecchia, C. Educational inequality in the dietary approach to stop hypertension (dash) diet in the uk: Evaluating the mediating role of income. Br. J. Nutr. 2021, 126, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Konttinen, H.; Sarlio-Lähteenkorva, S.; Silventoinen, K.; Männistö, S.; Haukkala, A. Socio-economic disparities in the consumption of vegetables, fruit and energy-dense foods: The role of motive priorities. Public Health Nutr. 2013, 16, 873–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amer, O.E.; Sabico, S.; Alfawaz, H.A.; Aljohani, N.; Hussain, S.D.; Alnaami, A.M.; Wani, K.; Al-Daghri, N.M. Reversal of Prediabetes in Saudi Adults: Results from an 18 Month Lifestyle Intervention. Nutrients 2020, 12, 804. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Parameters | All | Males | Females |
|---|---|---|---|
| N | 1200 | 476 | 724 |
| Age Group (Years) | |||
| 18–25 | 174 (14.5) | 61 (12.8) | 113 (15.6) |
| 26–35 | 644 (53.7) | 217 (45.6) | 427 (59) |
| 36–45 | 200 (16.6) | 105 (22.1) | 95 (13.1) |
| >45 | 182 (15.2) | 93 (19.5) | 89 (12.3) |
| Marital Status | |||
| Married | 445 (37.1) | 175 (36.8) | 270 (37.3) |
| Unmarried | 657 (54.8) | 271 (56.9) | 386 (53.3) |
| Divorced | 98 (8.2) | 30 (6.3) | 68 (9.4) |
| Family Income (SAR/Month) | |||
| <3000 | 138 (11.5) | 22 (4.6) | 116 (16) |
| 3001–9000 | 161 (13.4) | 57 (12) | 104 (14.4) |
| 9001–15,000 | 464 (38.7) | 186 (39.1) | 278 (38.4) |
| 15,001–21,000 | 315 (26.3) | 153 (32.1) | 162 (22.4) |
| >21,000 | 122 (10.2) | 58 (12.2) | 64 (8.8) |
| Educational Status | |||
| Secondary | 345 (28.8) | 180 (37.8) | 165 (22.8) |
| Graduate | 691 (57.6) | 262 (55) | 429 (59.3) |
| Post-graduate | 164 (13.7) | 34 (7.1) | 130 (18) |
| Kale Knowledge Questionnaire | All (1200) | Male (476) | Female (724) | p |
|---|---|---|---|---|
| Is kale considered a high calorie food? | 60.2 | 57.6 | 61.9 | 0.15 |
| Is kale considered a high nutritional value food? | 63.4 | 59.9 | 65.7 | 0.11 |
| Is kale considered a food with antioxidant properties? | 29.8 | 26.9 | 31.8 | 0.07 |
| Is kale considered a food with immune boosting properties? | 57.1 | 54.8 | 58.6 | 0.31 |
| Does excessive eating of kale cause constipation? | 11.5 | 13.2 | 10.4 | 0.06 |
| Is kale considered a food rich in fibers? | 55.3 | 50.8 | 58.1 | 0.02 |
| Is kale considered a food rich in vitamin C? | 31.2 | 29.0 | 32.6 | 0.37 |
| Is kale consumption considered bad for people suffering from digestive problems? | 13.7 | 16.0 | 12.2 | 0.05 |
| Is kale considered a food with anti-carcinogenic properties? | 17.2 | 16.8 | 17.4 | 0.88 |
| Is kale considered a food with anti-inflammatory properties? | 19.0 | 19.3 | 18.8 | 0.92 |
| Is kale considered a food high in fats? | 57.8 | 56.9 | 58.3 | 0.19 |
| Does kale play a role in controlling chronic diseases? | 29.8 | 31.7 | 28.6 | 0.47 |
| Does the nutritional value of kale increase after cooking? | 16.1 | 11.6 | 19.1 | <0.01 |
| Total Knowledge Score | 3.6 ± 0.1 | 3.5 ± 0.1 | 3.7 ± 0.1 | 0.12 |
| Parameters | All Subjects (1200) | ||||
|---|---|---|---|---|---|
| Tertile 1 (400) | Tertile 2 (400) | Tertile 3 (400) | Tertile3 vs. Tertile1 | ||
| Total Knowledge Score | 0.5 ± 0.0 | 3.5 ± 0.1 | 6.8 ± 0.1 | OR (95% CI) | p-value |
| Age Group (Years) | |||||
| 18–25 (174) | 43.1 | 32.8 | 24.1 | Reference | 0.002 |
| 26–35 (644) | 32.1 | 35.4 | 32.5 | 1.80 (1.2, 2.8) ** | |
| 36–45 (200) | 35.5 | 29 | 35.5 | 1.79 (1.1, 2.9) * | |
| >45 (182) | 25.8 | 31.3 | 42.9 | 2.96 (1.8, 5.0) ** | |
| Marital Status | |||||
| Married (445) | 33.7 | 33 | 33.3 | Reference | 0.55 |
| Unmarried (657) | 33.9 | 33.8 | 32.3 | 0.96 (0.7, 1.3) | |
| Divorced (98) | 27.6 | 31.6 | 40.8 | 1.50 (0.9, 2.6) | |
| Family Income (SAR/Month) | |||||
| <3000 (138) | 39.1 | 31.2 | 29.7 | 0.80 (0.5, 1.3) | 0.006 |
| 3001–9000 (161) | 41 | 34.8 | 24.2 | 0.63 (0.4, 0.9) * | |
| 9001–15,000 (464) | 35.1 | 31.7 | 33.2 | Reference | |
| 15,001–21,000 (315) | 28.3 | 35.9 | 35.9 | 1.34 (0.9, 1.9) | |
| >21,000 (122) | 23 | 33.6 | 43.4 | 2.00 (1.2, 3.3) ** | |
| Education Level | |||||
| Secondary (345) | 34.8 | 34.2 | 31 | Reference | <0.001 |
| Graduate (691) | 37.2 | 34 | 28.8 | 0.87 (0.6, 1.2) | |
| Post-graduate (164) | 14 | 28.7 | 57.3 | 4.58 (2.7, 7.7) ** | |
| Parameters | Males (476) | ||||
| Tertile 1 (159) | Tertile 2 (158) | Tertile 3 (159) | Tertile 3 vs. Tertile 1 | ||
| Total Knowledge Score | 0.2 ± 0.0 | 2.8 ± 0.1 | 6.6 ± 0.1 | OR (95% C.I.) | p-value |
| Age Group (Years) | |||||
| 18–25 (61) | 36.1 | 34.4 | 29.5 | Reference | 0.11 |
| 26–35 (217) | 33.6 | 37.3 | 29 | 1.05 (0.5, 2.1) | |
| 36–45 (105) | 38.1 | 27.6 | 34.3 | 1.10 (0.5, 2.3) | |
| >45 (93) | 25.8 | 29 | 45.2 | 2.14 (0.9, 4.7) | |
| Marital Status | |||||
| Married (175) | 33.1 | 33.7 | 33.1 | Reference | 0.21 |
| Unmarried (271) | 34.3 | 34.3 | 31.4 | 0.91 (0.6, 1.5) | |
| Divorced (30) | 26.7 | 20 | 53.3 | 2.00 (0.8, 5.0) | |
| Family Income (SAR/Month) | |||||
| <3000 (22) | 45.5 | 31.8 | 22.7 | 0.45 (0.1, 1.4) | 0.70 |
| 3001–9000 (57) | 38.6 | 36.8 | 24.6 | 0.59 (0.3, 1.3) | |
| 9001–15,000 (186) | 31.7 | 33.3 | 34.9 | Reference | |
| 15,001–21,000 (153) | 32 | 34 | 34 | 0.96 (0.6, 1.6) | |
| >21,000 (58) | 32.8 | 27.6 | 39.7 | 1.10 (0.5, 2.2) | |
| Education Level | |||||
| Secondary (180) | 32.2 | 31.1 | 36.7 | Reference | 0.016 |
| Graduate (262) | 35.9 | 35.5 | 28.6 | 0.72 (0.5, 1.1) | |
| Post-graduate (34) | 20.6 | 26.5 | 52.9 | 2.66 (1.1, 7.0) * | |
| Parameters | Females (724) | ||||
| Tertile 1 (241) | Tertile 2 (241) | Tertile 3 (242) | Tertile 3 vs. Tertile 1 | ||
| Total Knowledge score | 0.7 ± 0.1 | 3.9 ± 0.1 | 6.9 ± 0.1 | OR (95% CI) | p-value |
| Age Group (Years) | |||||
| 18–25 (113) | 46 | 31 | 23 | Reference | 0.03 |
| 26–35 (427) | 30.9 | 35.4 | 33.7 | 2.18 (1.3, 3.7) ** | |
| 36–45 (95) | 33.7 | 29.5 | 36.8 | 2.19 (1.1, 4.3) * | |
| >45 (89) | 28.1 | 30.3 | 41.6 | 2.96 (1.5, 5.9) ** | |
| Marital Status | |||||
| Married (270) | 35.2 | 30.4 | 34.4 | Reference | 0.49 |
| Unmarried (386) | 32.9 | 35.5 | 31.6 | 0.98 (0.7, 1.4) | |
| Divorced (68) | 27.9 | 32.4 | 39.7 | 1.45 (0.8, 2.8) | |
| Family Income (SAR/Month) | |||||
| <3000 (116) | 37.1 | 25.9 | 37.1 | 1.18 (0.7, 1.9) | 0.001 |
| 3001–9000 (104) | 42.3 | 31.7 | 26 | 0.73 (0.4, 1.3) | |
| 9001–15,000 (278) | 37.1 | 31.7 | 31.3 | Reference | |
| 15,001–21,000 (162) | 26.5 | 37.7 | 35.8 | 1.59 (0.9, 2.6) | |
| >21,000 (64) | 12.5 | 45.3 | 42.2 | 3.99 (1.7, 9.2) ** | |
| Education Level | |||||
| Secondary (165) | 40.6 | 34.5 | 24.8 | Reference | <0.001 |
| Graduate (429) | 36.8 | 34 | 29.1 | 1.29 (0.8, 2.0) | |
| Post-graduate (130) | 12.3 | 29.2 | 58.5 | 7.76 (3.9, 15.1) ** | |
| All | Male | Female | p-Value | |
|---|---|---|---|---|
| N | 1200 | 476 | 724 | |
| Have You Ever Heard about Kale? | ||||
| Yes | 585 (48.8) | 201 (42.2) | 384 (53) | <0.001 |
| No | 615 (51.3) | 275 (57.8) | 340 (47) | |
| Have You Consumed Kale Before? | ||||
| Yes | 276 (23) | 87 (18.3) | 189 (26.1) | 0.002 |
| No | 924 (77) | 389 (81.7) | 535 (73.9) | |
| How Many Times a Week Were You Consuming Kale? | ||||
| Once | 199 (72.1) | 48 (55.2) | 151 (79.9) | <0.001 |
| 2–3 times | 61 (22.1) | 33 (37.9) | 28 (14.8) | |
| >3 times | 16 (5.8) | 6 (6.9) | 10 (5.3) | |
| Have You Noticed Any Positive Effects on Health? | ||||
| Yes | 178 (64.5) | 62 (71.3) | 115 (60.8) | 0.11 |
| No | 98 (35.5) | 25 (28.7) | 74 (39.2) | |
| If Yes, Mention the Positive Effects? | ||||
| Weight Loss | 91 (51.1) | 28 (45.2) | 63 (54.8) | 0.14 |
| Decrease in appetite | 36 (20.2) | 18 (29) | 18 (15.7) | |
| Improved bowel movement | 30 (16.9) | 11 (17.7) | 19 (16.5) | |
| Energy boost | 21 (11.8) | 5 (8.1) | 15 (13) | |
| Any Side Effects? | ||||
| Yes | 49 (17.8) | 17 (19.5) | 32 (16.9) | 0.74 |
| No | 227 (82.2) | 70 (80.5) | 157 (83.1) | |
| If Yes, Mention the Side Effects? | ||||
| Constipation | 25 (51) | 10 (58.8) | 15 (46.9) | 0.69 |
| Bloating | 12 (24.5) | 4 (23.5) | 8 (25) | |
| Bowel irritability | 10 (20.4) | 2 (11.8) | 8 (25) | |
| Others | 2 (4.1) | 1 (5.9) | 1 (3.1) | |
| Mode of Consumption? | ||||
| Fresh | 158 (57.2) | 46 (52.9) | 112 (59.3) | 0.69 |
| Cooked | 53 (19.2) | 17 (19.5) | 36 (19) | |
| Supplement | 47 (17) | 18 (20.7) | 29 (15.3) | |
| Powder | 18 (6.5) | 6 (6.9) | 12 (6.3) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfawaz, H.A.; Wani, K.; Alrakayan, H.; Alnaami, A.M.; Al-Daghri, N.M. Awareness, Knowledge and Attitude towards ‘Superfood’ Kale and Its Health Benefits among Arab Adults. Nutrients 2022, 14, 245. https://doi.org/10.3390/nu14020245
Alfawaz HA, Wani K, Alrakayan H, Alnaami AM, Al-Daghri NM. Awareness, Knowledge and Attitude towards ‘Superfood’ Kale and Its Health Benefits among Arab Adults. Nutrients. 2022; 14(2):245. https://doi.org/10.3390/nu14020245
Chicago/Turabian StyleAlfawaz, Hanan A., Kaiser Wani, Haya Alrakayan, Abdullah M. Alnaami, and Nasser M. Al-Daghri. 2022. "Awareness, Knowledge and Attitude towards ‘Superfood’ Kale and Its Health Benefits among Arab Adults" Nutrients 14, no. 2: 245. https://doi.org/10.3390/nu14020245
APA StyleAlfawaz, H. A., Wani, K., Alrakayan, H., Alnaami, A. M., & Al-Daghri, N. M. (2022). Awareness, Knowledge and Attitude towards ‘Superfood’ Kale and Its Health Benefits among Arab Adults. Nutrients, 14(2), 245. https://doi.org/10.3390/nu14020245