
Trends in Diet Quality by Race/Ethnicity among Adults in the United States for 2011–2018


Abstract
1. Introduction
2. Materials and Method
2.1. Study Population
2.2. Assessment of Dietary Intake
2.3. Assessments of Dietary Quality
2.4. Other Variables
2.5. Statistical Analysis
3. Results
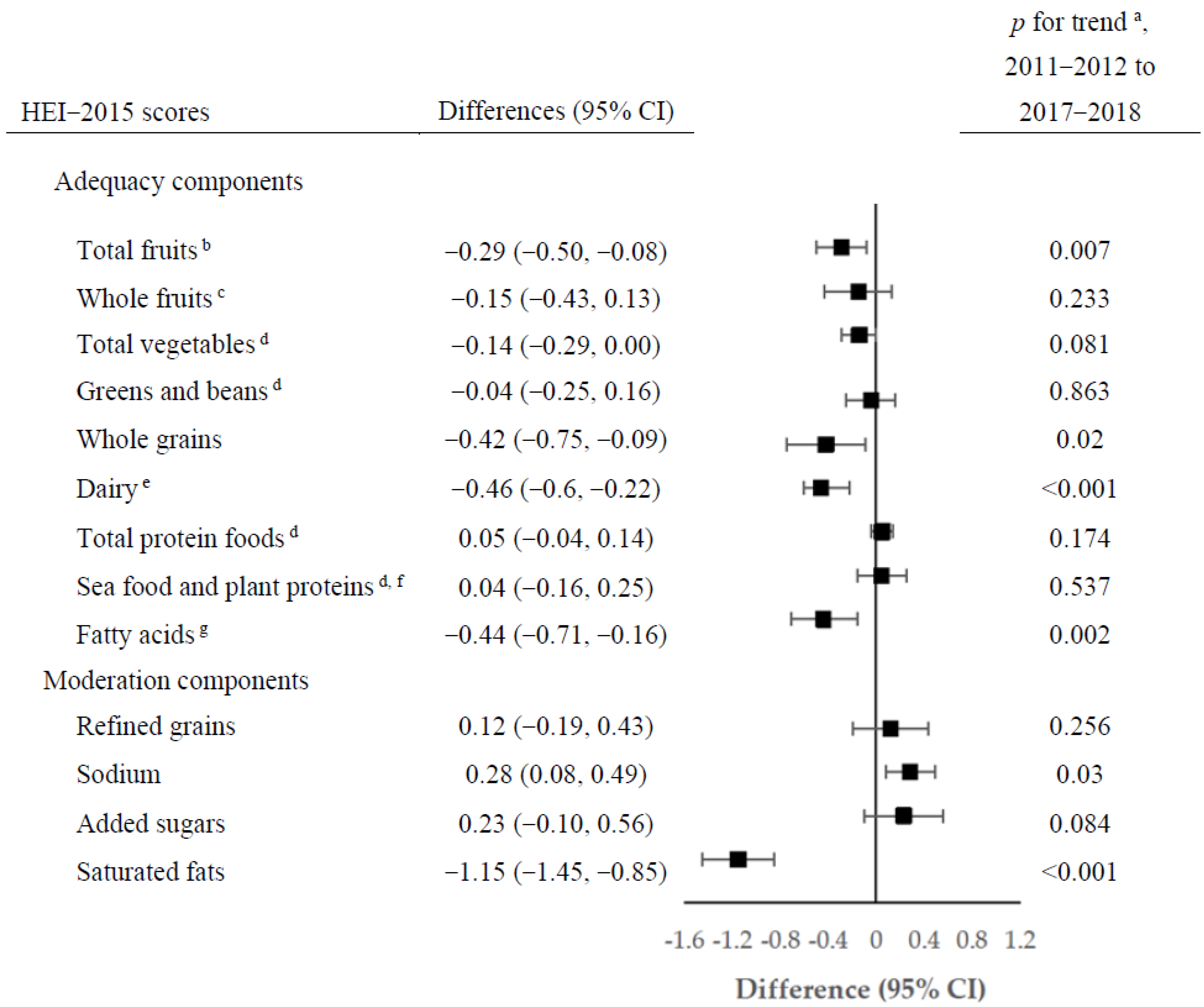
3.1. Healthy Eating Index 2015
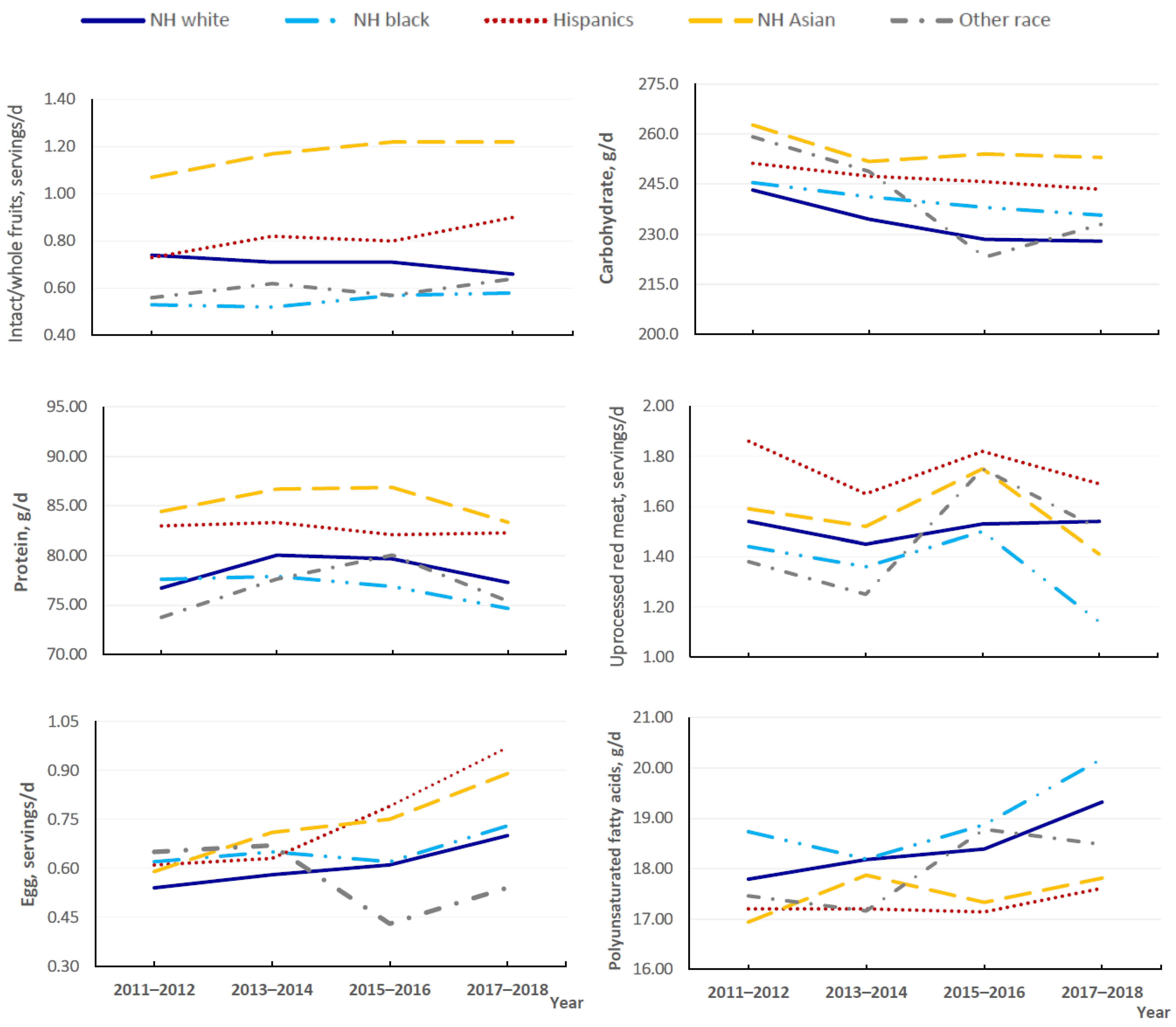
3.2. Trends in Specific Foods and Nutrients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD; 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar]
- Neuenschwander, M.; Ballon, A.; Weber, K.S.; Norat, T.; Aune, D.; Schwingshackl, L.; Schlesinger, S. Role of diet in type 2 diabetes incidence: Umbrella review of meta-analyses of prospective observation studies. BMJ 2019, 366, I2368. [Google Scholar] [CrossRef] [PubMed]
- Asghari, G.; Mirmiran, P.; Yuzbashian, E.; Azizi, F. A systematic review of diet quality indices in relation to obesity. Br. J. Nutr. 2017, 117, 1055–1065. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Hennein, R.; Liu, C.; Long, M.T.; Hoffmann, U.; Jacques, P.F.; Lichtenstein, A.H.; Hu, F.B.; Levy, D. Improved Diet Quality Associates with Reduction in Liver Fat, Particularly in Individuals with High Genetic Risk Scores for Nonalcoholic Fatty Liver Disease. Gastroenterology 2018, 155, 107–117. [Google Scholar] [CrossRef] [PubMed]
- US Department of Agriculture; US Department of Health and Human Services. Dietary Guidelines for Americans 2020–2025, 9th ed.; US Department of Agriculture: Washington, DC, USA, 2020.
- US Burden of Disease Collaborators; Mokdad, A.H.; Ballestros, K.; Echko, M.; Glenn, S.; Olsen, H.E.; Mullany, E.; Lee, A.; Khan, A.R.; Ahmadi, A.; et al. The State of US Health, 1990–2016: Burden of Diseases, Injuries, and Risk Factors Among US States. JAMA 2018, 319, 1444–1472. [Google Scholar] [PubMed]
- Han, S.; Wu, L.; Wang, W.; Li, N.; Wu, X. Trends in dietary nutrients by demographic characteristics and BMI among US adults, 2003–2016. Nutrients 2019, 11, 2617. [Google Scholar] [CrossRef]
- Shan, Z.; Rehm, C.D.; Rogers, G.; Ruan, M.; Wang, D.D.; Hu, F.B.; Mozaffarian, D.; Zhang, F.F.; Bhupathiraju, S.N. Trends in dietary carbohydrate, protein and fat intake and diet quality among US adults, 1999–2016. JAMA 2019, 322, 1178–1187. [Google Scholar] [CrossRef]
- Johnston, R.; Poti, J.M.; Popkin, B.M. Eating and aging: Trends in dietary intake among older Americans from 1977–2010. J. Nutr. Health Aging 2014, 18, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.D.; Wang, C.Y. Trends in intake of energy and macronutrients in adults from 1999–2000 through 2007–2008. NCHS Data Brief 2010, 49, 1–8. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Trends in intake of energy and macronutrients-United States, 1971–2000. MMWR Morb. Mortal. Wkly. Rep. 2004, 53, 80–82. [Google Scholar]
- Zeng, L.; Ruan, M.; Liu, J.; Wilde, P.; Naumova, E.N.; Mozaffarian, D.; Zhang, F.F. Trends in processed meat, unprocessed red meat, poultry, and fish consumption in the United States, 1999–2016. J. Acad. Nutr. Diet. 2019, 119, 1085–1098. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Rebholz, C.M.; Caulfield, L.E.; Ramsing, R.; Nachman, K.E. Trends in types of protein in US adults: Results from the National Health and Nutrition Examination Survey 1999–2010. Public Health Nutr. 2019, 22, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.F.; Liu, J.; Rehm, C.D.; Wilde, P.; Mande, J.R.; Mozaffarian, D. Trends and disparities in diet quality among US adults by Supplemental Nutrition Assistance Program participation status. JAMA Netw. Open 2018, 1, e180237. [Google Scholar] [CrossRef] [PubMed]
- Rehm, C.D.; Peñalvo, J.L.; Afshin, A.; Mozaffarian, D. Dietary intake among US adults, 1999–2012. JAMA 2016, 315, 2542–2553. [Google Scholar] [CrossRef]
- Wang, D.D.; Leung, C.W.; Li, Y.; Ding, E.L.; Chiuve, S.E.; Hu, F.B.; Willett, W.C. Trends in dietary quality among adults in the United States, 1999 through 2010. JAMA Intern. Med. 2014, 174, 1587–1595. [Google Scholar] [CrossRef] [PubMed]
- United States Census Bureau. Supplementary Tables on Race and Hispanic Origin: 2020 Census Redistricting Data; United States Census Bureau: Washington, DC, USA, 2020.
- Budiman, A.; Ruiz, N.G. Key Facts about Asian Americans, A Diverse and Growing Population; Pew Research Center: Washington, DC, USA, 2021. [Google Scholar]
- Liu, B.; Du, Y.; Wu, Y.; Snetselaar, L.G.; Wallace, R.B.; Bao, W. Trends in obesity and adiposity measures by race or ethnicity among adults in the United States 2011-18: Population based study. BMJ 2021, 372, n365. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.C.; Clark, J.; Riddles, M.K.; Mohadjer, L.K.; Fakhouri, T.H.I. National Health and Nutrition Examination Survey, 2015-2018: Sample Design and Estimation Procedures. Vital Health Stat. 2 2020, 184, 1–35. [Google Scholar]
- Johnson, C.L.; Dohrmann, S.M.; Burt, V.L.; Mohadjer, L.K. National health and nutrition examination survey: Sample design, 2011-2014. Vital Health Stat. 2 2014, 162, 1–33. [Google Scholar]
- Ahluwalia, N.; Dwyer, J.; Terry, A.; Moshfegh, A.; Johnson, C. Update on NHANES dietary data: Focus on collection, release, analytical considerations, and uses to inform public policy. Adv. Nutr. 2016, 7, 121–134. [Google Scholar] [CrossRef] [PubMed]
- Bowman, S.A.; Clemens, J.C.; Shimizu, M.; Friday, J.E.; Moshfegh, A.J. Food Patterns Equivalents Database 2015–2016: Methodology and User Guide. Food Surveys Research Group, Beltsville Human Nutrition Research Center, Agricultural Research Service, U.S. Department of Agriculture: Beltsville, MA, USA, 2018. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 26 April 2022).
- Bowman, S.A.; Clemens, J.C.; Friday, J.E.; Lynch, K.L.; Moshfegh, A.J. Food Patterns Equivalents Database 2013–2014: Methodology and User Guide. Food Surveys Research Group, Beltsville Human Nutrition Research Center, Agricultural Research Service, U.S. Department of Agriculture: Beltsville, MA, USA, 2017. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 26 April 2022).
- Bowman, S.A.; Clemens, J.C.; Friday, J.E.; Thoerig, R.C.; Moshfegh, A.J. Food Patterns Equivalents Database 2011–2012: Methodology and User Guide; Food Surveys Research Group, Beltsville Human Nutrition Research Center, Agricultural Research Service, U.S.; Department of Agriculture: Beltsville, MA, USA. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 26 April 2022).
- Haytowitz, D.B.; Ahuja, J.K.C.; Wu, X.; Somanchi, M.; Nickle, M.; Nguyen, Q.A.; Roseland, J.M.; Williams, J.R.; Patterson, K.Y.; Li, Y.; et al. USDA National Nutrient Database for Standard Reference, Legacy Release. Nutrient Data Laboratory, Beltsville Human Nutrition Research Center, ARS, USDA. 2019. Available online: https://data.nal.usda.gov/dataset/usda-national-nutrient-database-standard-reference-legacy-release (accessed on 26 April 2022).
- Krebs-Smith, S.M.; Pannucci, T.R.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef]
- National Cancer Institute. Division of Cancer Control and Population Sciences. Population Ratio Method. Available online: https://epi.grants.cancer.gov/hei/population-ratio-method.html (accessed on 15 June 2022).
- Tooze, J.A.; Kipnis, V.; Buchman, D.W.; Carroll, R.J.; Freedman, L.S.; Guenther, P.M.; Krebs-Smith, S.M.; Subar, A.F.; Dodd, K.W. A mixed-effects model approach for estimating the distribution of usual intake of nutrients: The NCI method. Stat. Med. 2010, 29, 2857–2868. [Google Scholar] [CrossRef] [PubMed]
- Ricciuto, L.; Fulgoni, V.L., 3rd; Gaine, P.C.; Scott, M.O.; DiFrancesco, L. Sources of added sugars intake among the US population: Analysis by selected sociodemographic factors using the National Health and Nutrition Examination Survey 2011–2018. Front. Nutr. 2021, 8, 687643. [Google Scholar] [CrossRef] [PubMed]
- Ricciuto, L.; Fulgoni, V.L.; Gaine, P.C.; Scott, M.O.; DiFrancesco, L. Trends in added sugars intake and sources among US children, adolescents, and teens using NHANES 2001–2018. J. Nutr. 2022, 152, 568–578. [Google Scholar] [CrossRef] [PubMed]
- Conrad, Z.; Johnson, L.K.; Roemmich, J.N.; Juan, W.Y.; Jahns, L. Time trends and patterns of reported egg consumption in the US by sociodemographic characteristics. Nutrients 2017, 9, 333. [Google Scholar] [CrossRef] [PubMed]
- McNamara, D.J. The Fifty Year Rehabilitation of the Egg. Nutrients 2015, 7, 8716–8722. [Google Scholar] [CrossRef]
- Powles, J.; Fahimi, S.; Micha, R.; Khatibzadeh, S.; Shi, P.; Ezzati, M.; Engell, R.E.; Lim, S.S.; Danaei, G.; Mozaffarian, D.; et al. Global, regional and national sodium intakes in 1990 and 2010: A systematic analysis of 24 h urinary sodium excretion and dietary surveys worldwide. BMJ Open 2013, 3, e003733. [Google Scholar] [CrossRef] [PubMed]
- Brown, I.J.; Tzoulaki, I.; Candeias, V.; Elliott, P. Salk intakes around the world: Implications for public health. Int. J. Epidemiol. 2009, 38, 791–813. [Google Scholar] [CrossRef] [PubMed]
- Firestone, M.J.; Beasley, J.M.; Kwon, S.C.; Ahn, J.; Trinh-Shevrin, C.; Yi, S.S. Asian American Dietary Sources of Sodium and Salt Behaviors Compared with Other Racial/ethnic Groups, NHANES, 2011–2012. Ethn. Dis. 2017, 27, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Murphy, S.P.; Sharma, S.; Kolonel, L.N. Dietary intakes and health-related behaviours of Korean American women born in the USA and Korea: The Multiethnic Cohort Study. Public Health Nutr. 2005, 8, 904–911. [Google Scholar] [CrossRef] [PubMed]
- Ma, G.X.; Zhu, L.; Shive, S.E.; Zhang, G.; Senter, Y.R.; Topete, P.; Seals, B.; Zhai, S.; Wang, M.; Tan, Y. The Evaluation of IDEAL-REACH Program to Improve Nutrition among Asian American Community Members in the Philadelphia Metropolitan Area. Int. J. Environ. Res. Public Health 2019, 16, 3054. [Google Scholar] [CrossRef] [PubMed]
- Dixit, A.A.; Azar, K.M.; Gardner, C.D.; Palaniappan, L.P. Incorporation of whole, ancient grains into a modern Asian Indian diet to reduce the burden of chronic disease. Nutr. Rev. 2011, 39, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Tseng, M.; Wright, D.J.; Fang, C.Y. Acculturation and dietary change among Chinese immigrant women in the United States. J. Immigr. Minor. Health 2015, 17, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Roark, R.A.; Niederhauser, V.P. Fruit and vegetable intake: Issues with definition and measurement. Public Health Nutr. 2013, 16, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Tooze, J.A.; Midthune, D.; Dodd, K.W.; Freedman, L.S.; Krebs-Smith, S.M.; Subar, A.F.; Guenther, P.M.; Carroll, R.J.; Kipnis, V.A. A new statistical method for estimating the usual intake of episodically consumed foods with application to their distribution. J. Am. Diet. Assoc. 2006, 106, 1575–1587. [Google Scholar] [CrossRef]
- Reedy, J.; Lerman, J.L.; Krebs-Smith, S.M.; Kirkpatrick, S.I.; Pannucci, T.E.; Wilson, M.M.; Subar, A.F.; Kahle, L.L.; Tooze, J.A. Evaluation of the Healthy Eating Index-2015. J. Acad. Nutr. Diet. 2018, 118, 1622–1633. [Google Scholar] [CrossRef]
- Herrick, K.A.; Rossen, L.M.; Parsons, R.; Dodd, K.W. Estimating usual dietary intake from National Health and Nutrition Examination Survey data using the National Cancer Institute method. Vital Health Stat. 2 2018, 178, 1–6. [Google Scholar]
- Bailey, R.L.; Dodd, K.W.; Goldman, J.A.; Gahche, J.J.; Dwyer, J.T.; Moshfegh, A.J.; Sempos, C.T.; Picciano, M.F. Estimation of total usual calcium and vitamin D intakes in the United States. J. Nutr. 2010, 140, 817–822. [Google Scholar] [CrossRef]
- National Cancer Institute. Usual Dietary Intakes: Details of the Method. Available online: https://epi.grants.cancer.gov/diet/usualintakes/details.html (accessed on 25 June 2022).




{kind=link}
{kind=link}
{kind=link}
| Total HEI-2015 Scores | Survey-Weighted Mean Score (95% CI) | |||||
|---|---|---|---|---|---|---|
| 2011–2012 (n = 4313) | 2013–2014 (n = 4559) | 2015–2016 (n = 4394) | 2017–2018 (n = 4058) | Differences 2017–2018 vs. 2011–2012 (95% CI) | p for Trend a | |
| Overall | 55.01 (54.09, 55.95) | 54.18 (53.46, 54.91) | 53.91 (52.46, 55.36) | 52.65 (51.12, 54.19) | −2.36 (−4.16, −0.57) | 0.011 |
| All participants | ||||||
| NH white | 55.36 (54.19, 56.53) | 54.03 (53.21, 54.86) | 54.15 (52.50, 55.80) | 52.14 (50.30, 53.98) | −3.22 (−5.40, −1.04) | 0.007 |
| NH black | 52.48 (50.27, 54.70) | 51.75 (50.57, 50.92) | 50.63 (48.67, 52.59) | 50.82 (49.04, 52.59) | −1.67 (−4.50, 1.17) | 0.176 |
| Hispanic | 54.06 (52.91, 55.21) | 54.58 (52.64, 56.52) | 52.75 (51.28, 54.21) | 54.04 (52.10, 55.99) | −0.02 (−2.28, 2.25) | 0.625 |
| NH Asian | 59.85 (58,09, 61.61) | 61.16 (59.54, 62.79) | 60.52 (58.89, 62.16) | 59.85 (57.36, 62.33) | −0.01 (−3.05, 3.04) | 0.855 |
| Other race b | 52.83 (48.68, 56.38) | 52.36 (48.10, 56.63) | 53.57 (50.12, 57.03) | 50.60 (46.84, 54.35) | −1.93 (−7.31, 3.44) | 0.498 |
| Male | ||||||
| NH white | 54.08 (53.14, 55.02) | 52.01 (51.01 53.02) | 53.40 (51.07, 55.73) | 50.46 (48.65, 52.27) | −3.62 (−5.66, −1.58) | 0.007 |
| NH black | 51.88 (49.27, 54.49) | 51.41 (50.40, 52.43) | 48.80 (46.99, 50.61) | 48.77 (46.89, 50.65) | −3.11 (−6.32, 0.11) | 0.020 |
| Hispanic | 52.64 (51.22, 54.07) | 53.17 (50.15, 56.20) | 50.61 (49.33, 51.89) | 52.30 (50.39, 54.22) | −0.34 (−2.73, 2.05) | 0.379 |
| NH Asian | 59.31 (57.01, 61.60) | 60.88 (58.06, 63.69) | 59.14 (56.91, 61.36) | 58.98 (55.76, 62.20) | −0.33 (−4.28, 3.63) | 0.643 |
| Other race b | 48.71 (44.42, 53.00) | 48.31 (44.15, 52.48) | 50.96 (47.57, 54.35) | 53.33 (47.55, 59.11) | 4.62 (−2.58, 11.82) | 0.137 |
| Female | ||||||
| NH white | 56.61 (54.88, 58.34) | 56.01 (55.11, 56.91) | 54.90 (52.91, 56.89) | 53.72 (51.61, 55.84) | −2.89 (−5.62, −0.15) | 0.025 |
| NH black | 52.95 (50.87, 55.02) | 52.01 (50.24, 53.78) | 52.23 (49.93, 54.53) | 51.73 (50.49, 54.97) | −0.22 (−3.27, 2.84) | 0.928 |
| Hispanic | 55.55 (54.24, 56.86) | 56.00 (54.41, 57.59) | 54.78 (52.46, 57.11) | 55.70 (53.49, 57.92) | 0.16 (−2.42, 2.73) | 0.869 |
| NH Asian | 60.38 (57.90, 62.86) | 61.45 (59.41, 63.49) | 61.89 (59.73, 64.05) | 60.64 (58.02, 63.26) | 0.26 (−3.35, 3.87) | 0.874 |
| Other race b | 56.28 (51.60, 60.95) | 57.14 (52.04, 62.23) | 55.89 (51.06, 60.71) | 47.55 (45.69, 49.41) | −8.73 (−13.76, −3.69) | <0.001 |
| Foods/Nutrients | Survey-Weighted Mean Score (95% CI) | |||||
|---|---|---|---|---|---|---|
| 2011–2012 (n = 4313) | 2013–2014 (n = 4559) | 2015–2016 (n = 4394) | 2017–2018 (n = 4058) | Differences 2017–2018 vs. 2011–2012 (95% CI) | p for Trend a | |
| Food density (per 2000 kcal per day) | ||||||
| Total fruits (servings) | 1.02 (0.93, 1.10) | 0.96 (0.89, 1.04) | 0.97 (0.89, 1.04) | 0.91 (0.83, 0.99) | −0.10 (−0.21, 0.001) | 0.005 |
| Intact/whole fruit | 0.73 (0.66, 0.79) | 0.72 (0.66, 0.79) | 0.74 (0.65, 0.82) | 0.72 (0.64, 0.79) | −0.01 (−0.10, 0.09) | 0.230 |
| 100% fruit juices | 0.30 (0.26, 0.34) | 0.26 (0.24, 0.28) | 0.26 (0.23, 0.28) | 0.21 (0.19, 0.23) | −0.09 (−0.14, −0.05) | <0.001 |
| Total vegetables (servings) | 1.65 (1.55, 1.75) | 1.56 (1.49, 1.64) | 1.64 (1.54, 1.73) | 1.60 (1.51, 1.70) | −0.05 (−0.18, 0.08) | 0.463 |
| Total grains (servings) | 6.28 (6.14, 6.43) | 6.21 (6.09, 6.34) | 6.07 (5.99, 6.15) | 6.13 (5.95, 6.31) | −0.15 (−0.36, 0.06) | 0.025 |
| Whole grains | 0.99 (0.88, 1.09) | 0.93 (0.87, 0.98) | 0.94 (0.87, 1.00) | 0.80 (0.70, 0.90) | −0.19 (−0.32, −0.05) | 0.008 |
| Refined grains | 5.31 (5.18, 5.45) | 5.30 (5.16, 5.43) | 5.14 (5.05, 5.23) | 5.32 (5.19, 5.45) | 0.01 (−0.16, 0.18) | 0.535 |
| Legumes (servings) | 0.12 (0.10, 0.14) | 0.11 (0.10, 0.12) | 0.12 (0.10, 0.13) | 0.11 (0.09, 0.13) | −0.01 (−0.04, 0.01) | 0.740 |
| Soy products (servings) | 0.07 (0.05, 0.09) | 0.08 (0.06, 0.10) | 0.12 (0.10, 0.15) | 0.11 (0.08, 0.15) | 0.04 (0.01, 0.08) | 0.004 |
| Total meat (servings) | 4.59 (4.41, 4.77) | 4.79 (4.54, 5.03) | 4.76 (4.53, 4.98) | 4.61 (4.42, 4.80) | 0.02 (−0.22, 0.26) | 0.726 |
| Unprocessed red meat | 1.57 (1.39, 1.75) | 1.47 (1.38, 1.56) | 1.59 (1.49, 1.68) | 1.50 (1.32, 1.69) | −0.07 (−0.30, 0.17) | 0.525 |
| Processed meat | 0.94 (0.87, 1.01) | 0.98 (0.88, 1.07) | 0.96 (0.89, 1.04) | 0.93 (0.85, 1.02) | −0.01 (−0.11, 0.10) | 0.276 |
| Poultry | 1.44 (1.29, 1.59) | 1.65 (1.51, 1.79) | 1.56 (1.39, 1.72) | 1.51 (1.37, 1.65) | 0.08 (−0.11, 0.27) | 0.116 |
| Fish/seafood | 0.63 (0.49, 0.87) | 0.69 (0.55, 0.84) | 0.61 (0.52, 0.69) | 0.63 (0.52, 0.73) | −0.002 (−0.16, 0.16) | 0.369 |
| Fish high in omega-3 fatty acids | 0.16 (0.11, 0.20) | 0.22 (0.17, 0.26) | 0.19 (0.15, 0.24) | 0.16 (0.12, 0.20) | 0.003 (−0.05, 0.06) | 0.510 |
| Fish low in omega-3 fatty acids | 0.46 (0.36, 0.56) | 0.48 (0.35, 0.62) | 0.42 (0.34, 0.51) | 0.48 (0.38, 0.57) | 0.02 (−0.11, 0.14) | 0.439 |
| Eggs (servings) | 0.56 (0.51, 0.61) | 0.60 (0.56, 0.65) | 0.64 (0.60, 0.69) | 0.75 (0.66, 0.83) | 0.18 (0.09, 0.28) | <0.001 |
| Total dairy (servings) | 1.50 (1.44, 1.55) | 1.50 (1.44, 1.57) | 1.41 (1.37, 1.46) | 1.35 (1.29, 1.40) | −0.15 (−0.22, −0.08) | <0.001 |
| Milk products (servings) | 0.73 (0.68, 0.78) | 0.68 (0.64, 0.71) | 0.62 (0.58, 0.65) | 0.59 (0.53, 0.64) | −0.14 (−0.21, −0.07) | <0.001 |
| Cheese (servings) | 0.68 (0.63, 0.72) | 0.72 (0.67, 0.77) | 0.67 (0.64, 0.71) | 0.68 (0.64, 0.73) | 0.01 (−0.05, 0.06) | 0.336 |
| Nuts and seeds (servings) | 0.72 (0.63, 0.80) | 0.72 (0.63, 0.81) | 0.73 (0.61, 0.86) | 0.76 (0.63, 0.89) | 0.04 (−0.10, 0.18) | 0.221 |
| Added sugars (tsp) | 16.35 (15.57, 17.12) | 15.95 (15.31, 16.59) | 15.11 (14.51, 15.70) | 15.53 (14.58, 16.48) | −0.81 (−1.93, 0.30) | 0.032 |
| Nutrients (per day) | ||||||
| Carbohydrate (g) | 246.02 (242.99, 249.05) | 238.47 (235.84, 241.10) | 233.38 (229.98, 236.79) | 232.94 (229.97, 235.91) | −13.09 (−16.97, −9.20) | <0.001 |
| Protein (g) | 78.03 (76.86, 79.20) | 80.55 (78.45, 82.65) | 80.14 (78.68, 81.60) | 78.02 (76.46, 79.58) | −0.01 (−1.79, 1.77) | 0.570 |
| Saturated fat (g) | 23.51 (22.91, 24.11) | 24.39 (24.04, 24.74) | 25.70 (25.20, 26.21) | 26.13 (25.57, 26.68) | 2.62 (1.87, 3.37) | <0.001 |
| Monounsaturated fat (g) | 26.26 (25.82, 26.71) | 26.41 (26.12, 26.70) | 27.80 (27.29, 28.31) | 27.46 (26.90, 28.03) | 1.20 (0.54, 1.86) | <0.001 |
| Polyunsaturated fat (g) | 17.76 (17.47, 18.06) | 17.99 (17.64, 18.35) | 18.21 (17.77, 18.65) | 19.02 (18.36, 19.69) | 1.26 (0.59, 1.92) | <0.001 |
| Omega-3 fatty acids (g) | 0.09 (0.08, 0.10) | 0.10 (0.08, 0.11) | 0.10 (0.09, 0.10) | 0.09 (0.08, 0.10) | 0.0002 (−0.01, 0.01) | 0.771 |
| Cholesterol (g) | 265.04 (258.25, 271.84) | 280.50 (273.96, 287.05) | 292.47 (282.91, 302.02) | 295.34 (281.75, 308.93) | 30.30 (16.38, 44.22) | <0.001 |
| Sodium (mg) | 3374.22 (3352.96, 3395.49) | 3393.99 (3346.66, 3441.32) | 3433.22 (3373.58, 3492.86) | 3372.48 (3286.77, 3459.19) | −1.74 (−83.73, 80.05) | 0.609 |
| Fiber (g) | 17.36 (16.69, 18.03) | 16.77 (16.20, 17.34) | 16.99 (16.34, 17.64) | 16.31 (15.70, 16.91) | −1.05 (−1.88, −0.22) | 0.016 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tao, M.-H.; Liu, J.-L.; Nguyen, U.-S.D.T. Trends in Diet Quality by Race/Ethnicity among Adults in the United States for 2011–2018. Nutrients 2022, 14, 4178. https://doi.org/10.3390/nu14194178
Tao M-H, Liu J-L, Nguyen U-SDT. Trends in Diet Quality by Race/Ethnicity among Adults in the United States for 2011–2018. Nutrients. 2022; 14(19):4178. https://doi.org/10.3390/nu14194178
Chicago/Turabian StyleTao, Meng-Hua, Jia-Liang Liu, and Uyen-Sa D. T. Nguyen. 2022. "Trends in Diet Quality by Race/Ethnicity among Adults in the United States for 2011–2018" Nutrients 14, no. 19: 4178. https://doi.org/10.3390/nu14194178
APA StyleTao, M.-H., Liu, J.-L., & Nguyen, U.-S. D. T. (2022). Trends in Diet Quality by Race/Ethnicity among Adults in the United States for 2011–2018. Nutrients, 14(19), 4178. https://doi.org/10.3390/nu14194178