

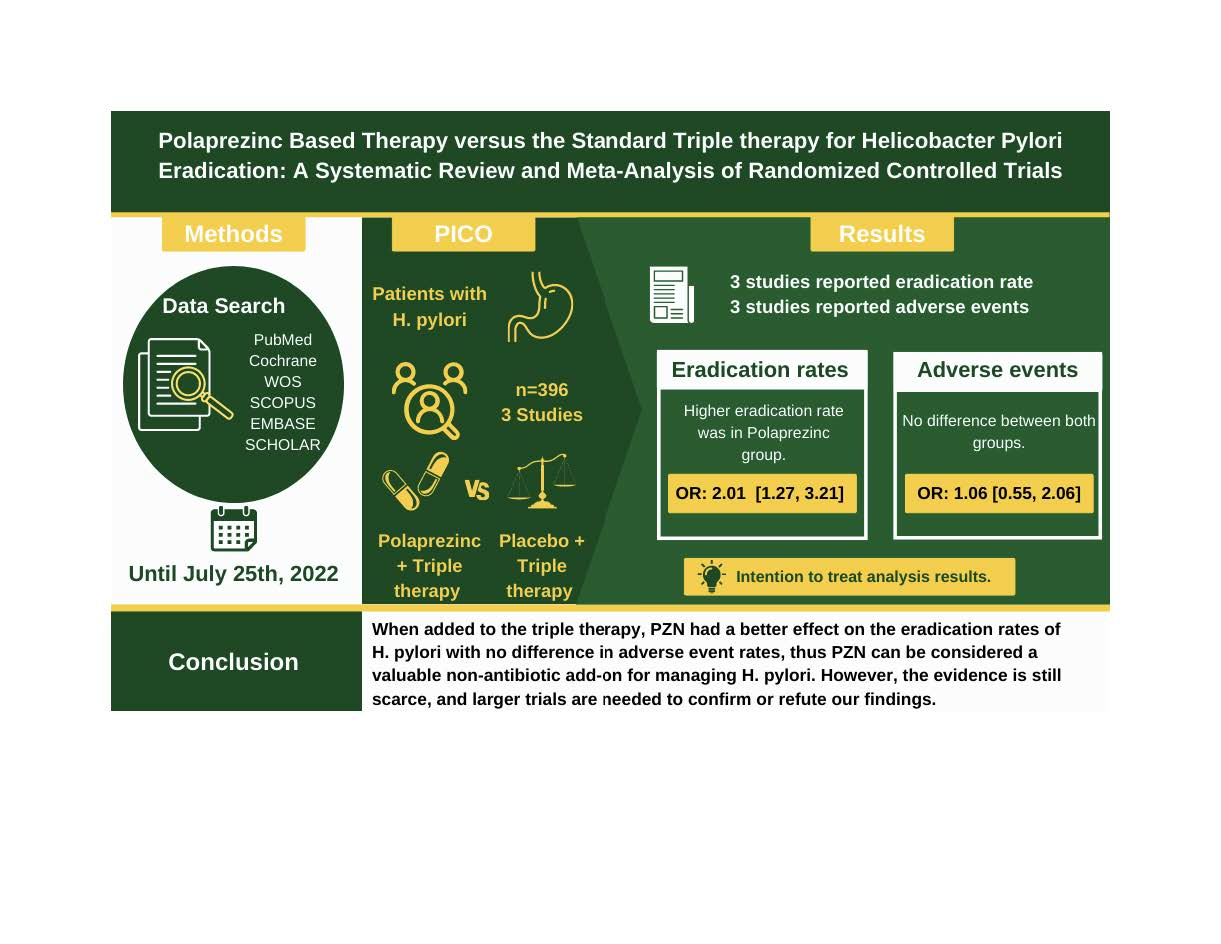
Efficacy and Safety of Polaprezinc-Based Therapy versus the Standard Triple Therapy for Helicobacter pylori Eradication: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 ,
,  and
and 
Abstract

1. Introduction
2. Materials and Methods
2.1. Protocol Registration
2.2. Data Sources and Search Strategy
2.3. Eligibility Criteria
2.4. Study Selection
2.5. Data Extraction
2.6. Risk of Bias and Quality Assessment
2.7. Statistical Analysis
3. Results
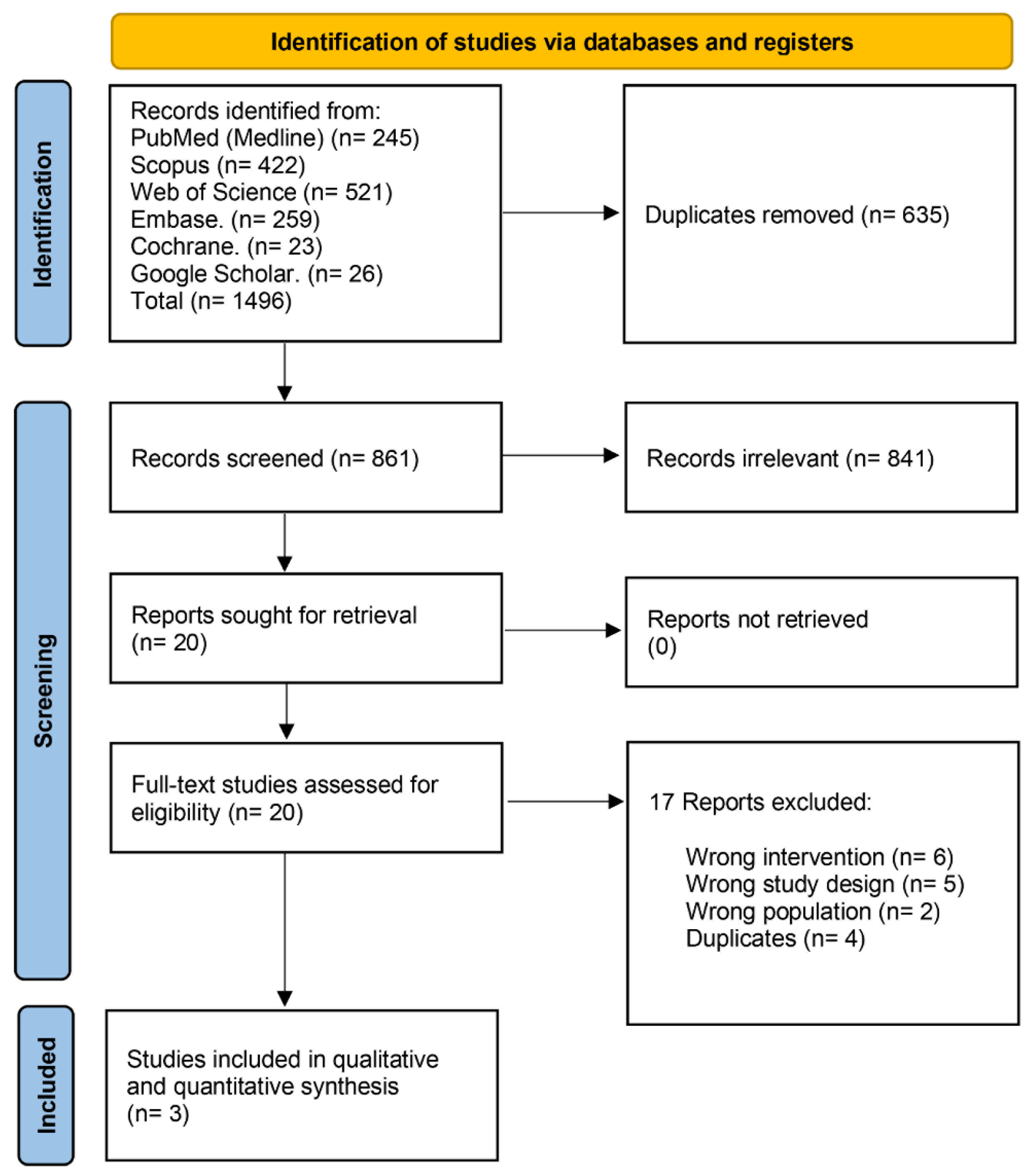
3.1. Search Results and Study Selection
3.2. Characteristics of Included Studies
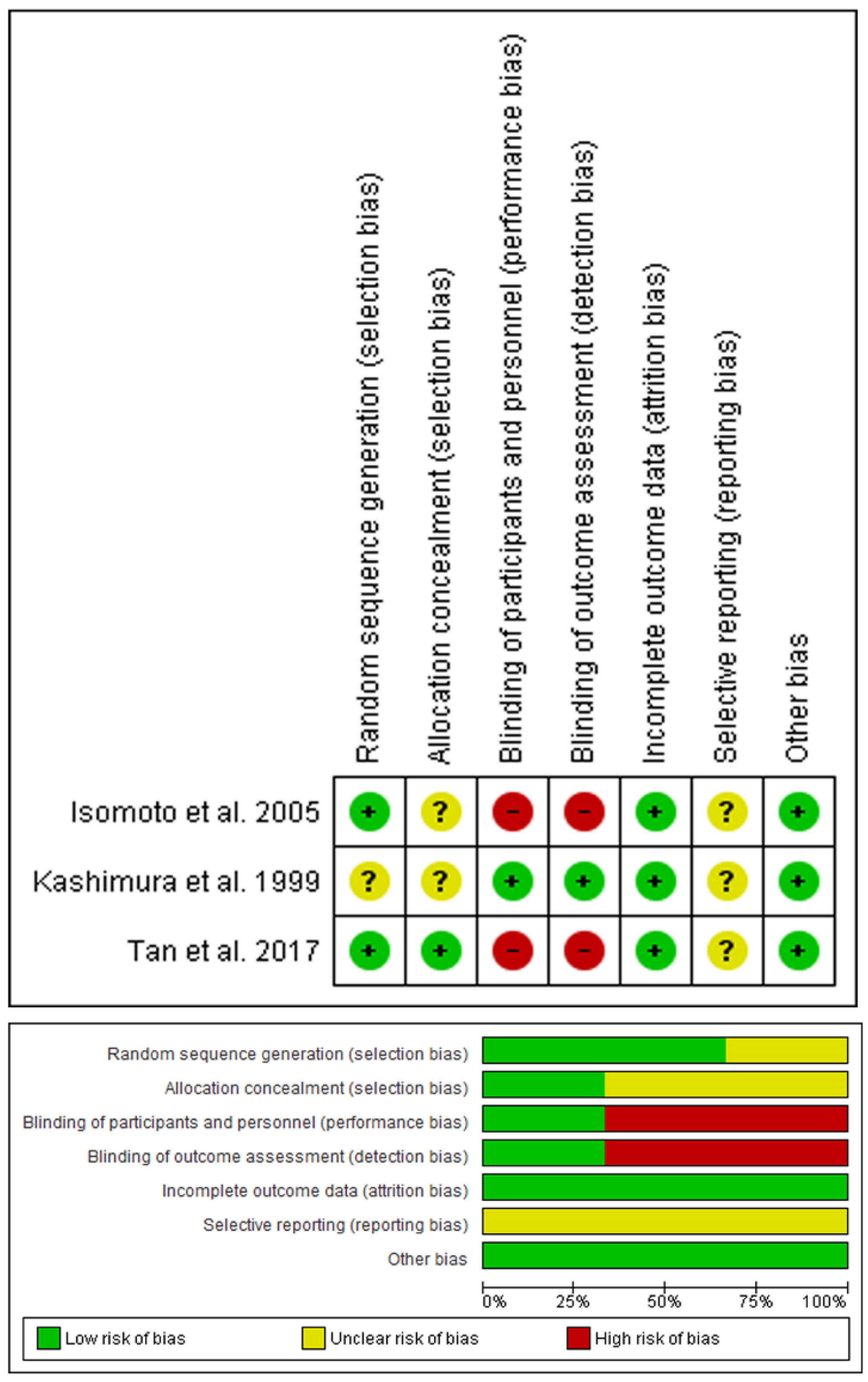
3.3. Risk of Bias and Quality of Evidence
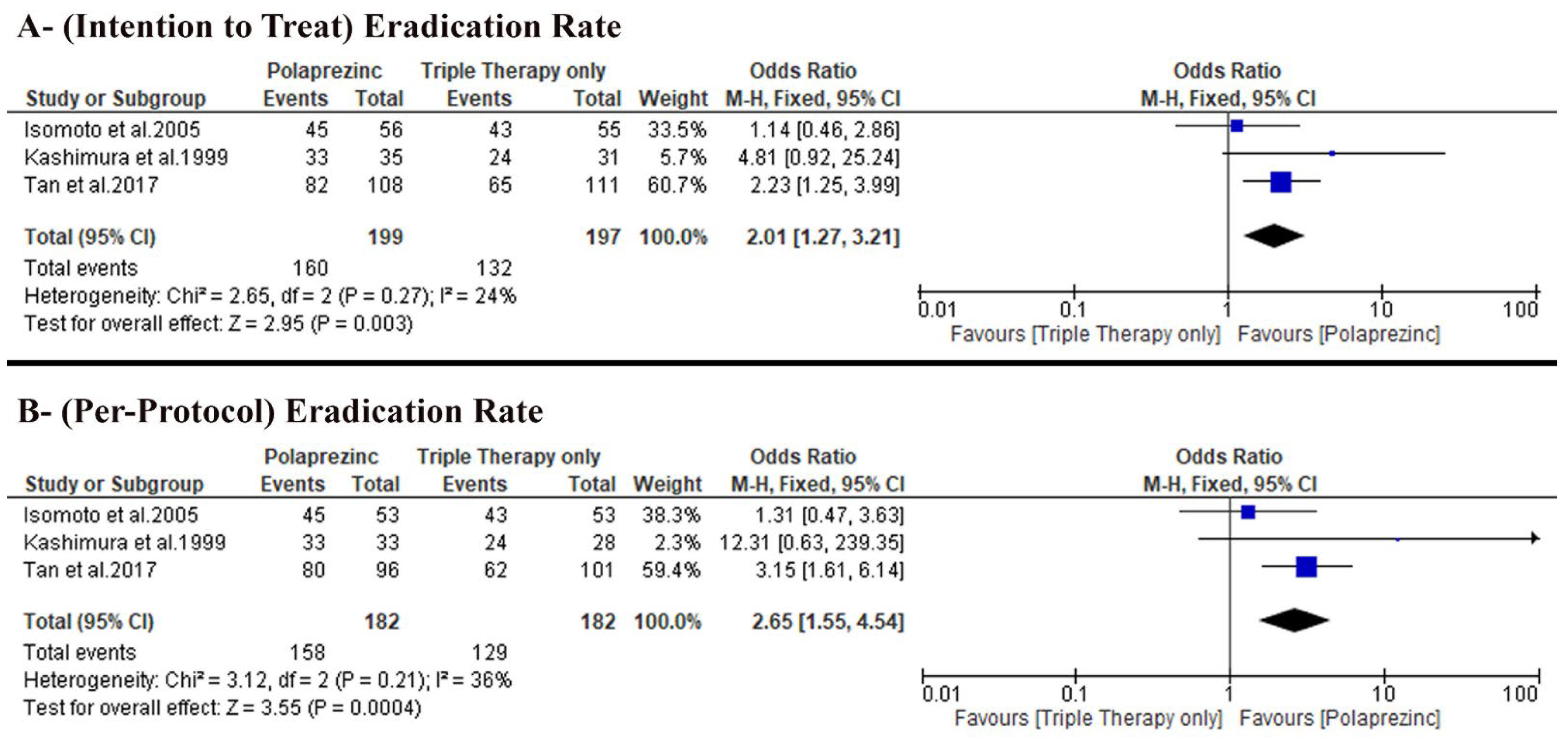
3.4. Primary Outcomes
3.4.1. H. pylori Eradication Rates Based on Intention to Treat Analysis
3.4.2. H. pylori Eradication Rates Based on per Protocol Analysis
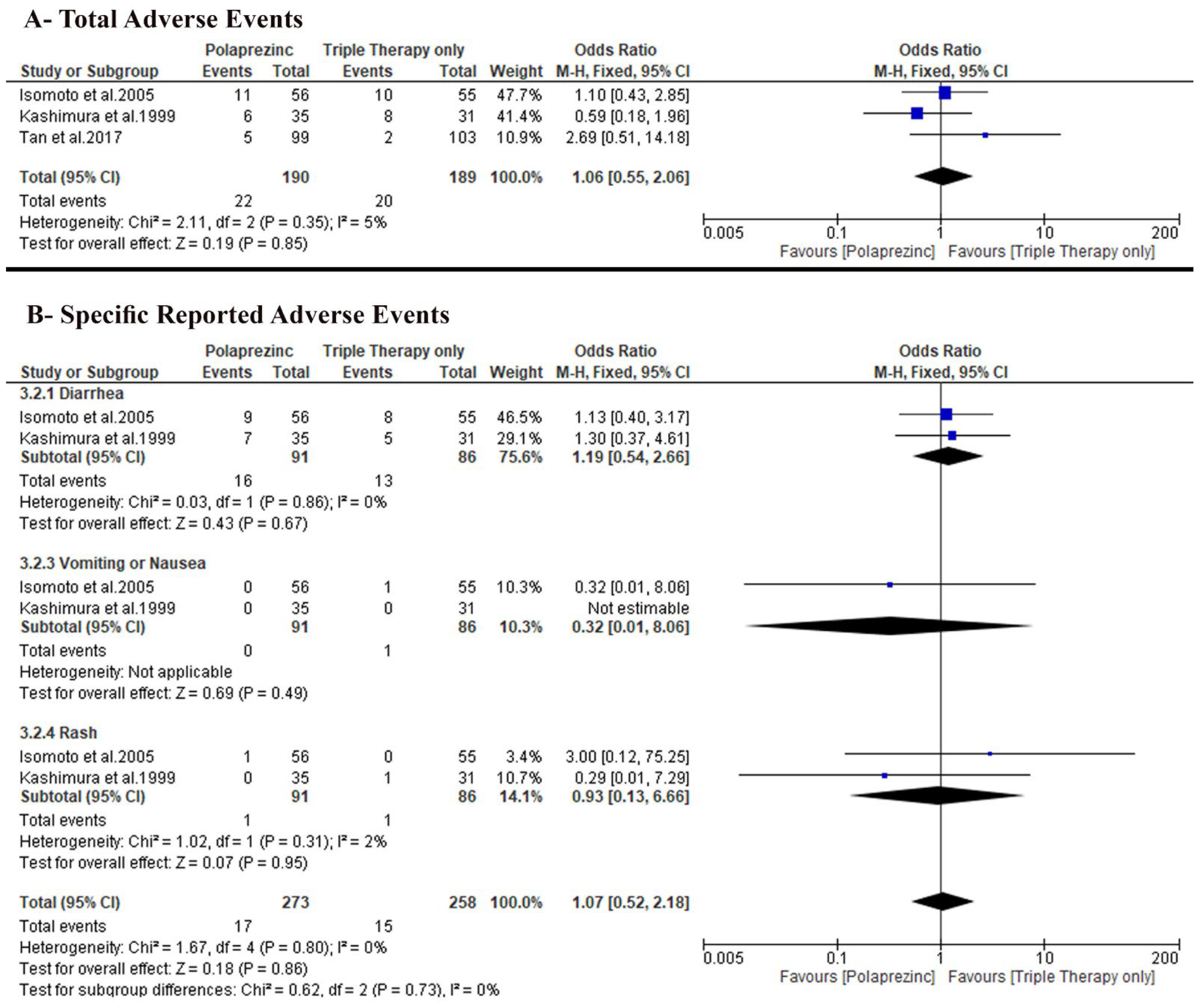
3.5. Secondary Outcomes
3.5.1. Total Patients with Adverse Events
3.5.2. Specific Adverse Events
4. Discussion
4.1. Strengths
4.2. Limitations
4.3. Implications for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CI | Confidence interval, the lower and upper limits of significance |
| TT | Triple therapy |
| H. pylori | Helicobacter pylori |
| MD | Mean difference |
| N/A | Not available |
| p | Probability |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses [42,43] |
| PZN | Polaprezinc |
| RCT | Randomized controlled trial |
| SD | Standard deviation |
| WOS | Web of Science |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section and Topic | Item # | Checklist Item | Location Where Item Is Reported |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | Page 1 |
| ABSTRACT | |||
| Abstract | 2 | See the PRISMA 2020 for Abstracts checklist. | Page 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | Page 2 |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | page 2 |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | Page 3 Section 2.3 |
| Information sources | 6 | Specify all databases, registers, websites, organisations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | Page 3 Section 2.2 |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | Page 2, 3, Table 1 |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process. | Page 3 Section 2.4 |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and if applicable, details of automation tools used in the process. | Page 3 Section 2.4 |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses), and if not, the methods used to decide which results to collect. | Page 3 Section 2.5 |
| 10b | List and define all other variables for which data were sought (e.g., participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | Page 3 Section 2.5 | |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process. | Page 3 Section 2.6 |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results. | Page 4 Section 2.7 |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g., tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | Page 4 Section 2.7 |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions. | Page 4 Section 2.7 | |
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | Page 4 Section 2.7 | |
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used. | Page 4 Section 2.7 | |
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results (e.g., subgroup analysis, meta-regression). | Not applicable | |
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | Not applicable | |
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | Page 3 Section 2.6 |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | Page 4 Section 2.7 |
| RESULTS | |||
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | Page 4, Section 3.1 |
| 16b | Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded. | Not applicable | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | Page 5, Section 3.2 |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | Page 5, Section 3.3 |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | Pages 9, 10 Section 3.4 and 3.5 |
| Results of syntheses | 20a | For each synthesis, briefly summarise the characteristics and risk of bias among contributing studies. | Page 5 Section 3.2 and 3.3 |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | Pages 9, 10 Section 3.4 and 3.5 | |
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | Not applicable | |
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | Not applicable | |
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | Page 5, Section 3.3 |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | Page 9, 10 |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | Page 10, 11 |
| 23b | Discuss any limitations of the evidence included in the review. | Page 12 | |
| 23c | Discuss any limitations of the review processes used. | Page 12 | |
| 23d | Discuss implications of the results for practice, policy, and future research. | Page 12 | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | Page 2 Section 2.1 |
| 24b | Indicate where the review protocol can be accessed, or state that a protocol was not prepared. | Page 2 Section 2.1 | |
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | Page 2 Section 2.1 | |
| Support | 25 | Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review. | Page 12 |
| Competing interests | 26 | Declare any competing interests of review authors. | Page 12 |
| Availability of data, code and other materials | 27 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review. | Page 12 |
Appendix B
| Study ID | Domain | Judgment |
|---|---|---|
| Isomoto et al. [26] 2005 | Allocation concealment (selection bias) | Unclear risk “no enough information’’ |
| Blinding of participants and personnel (performance bias) | High risk “The present study was open label trial” | |
| Blinding of outcome assessment (detection bias) | High Risk “The study was open-label” | |
| Selective reporting (reporting bias) | Unclear risk “no protocol was able to be retrieved” | |
| Kashimura et al. [27] 1999 | Random sequence generation (selection bias) | Unclear risk “did not mention the method of randomization” |
| Allocation concealment (selection bias) | Unclear risk “did not mention the method of allocation” | |
| Selective reporting (reporting bias) | Unclear risk “no protocol was able to be retrieved” | |
| Tan et al. [28] 2017 | Blinding of participants and personnel (performance bias) | High risk “This was an open-label clinical study.” |
| Blinding of outcome assessment (detection bias) | High risk “This was an open-label clinical study.” |
References
- Hooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong., V.W.S.; Wu., J.Y.; et al. Global prevalence of Helicobacter pylori infection: Systematic review and meta-analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef]
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2017: A systematic analysis for the global burden of disease study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [CrossRef]
- Wang, Z.; Liu, Y.; Peng, Y.; Peng, L. Helicobacter pylori Infection—A risk factor for irritable bowel syndrome? An updated systematic review and meta-analysis. Medicina 2022, 58, 1035. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Lu, H.; Graham, D.Y. An update on Helicobacter pylori as the cause of gastric cancer. Gastrointest. Tumors 2014, 1, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Holtmann, G.J.; Ford, A.C.; Talley, N.J. Pathophysiology of irritable bowel syndrome. Lancet Gastroenterol. Hepatol. 2016, 1, 133–146. [Google Scholar] [CrossRef]
- Saha, L. Irritable bowel syndrome: Pathogenesis, diagnosis, treatment, and evidence-based medicine. World J. Gastroenterol. 2014, 20, 6759–6773. [Google Scholar] [CrossRef]
- Graham, D.Y.; Yamaoka, Y. H. pylori and cagA: Relationships with gastric cancer, duodenal ulcer, and reflux esophagitis and its complications. Helicobacter 1998, 3, 145–151. [Google Scholar] [CrossRef]
- Tsay, F.-W.; Hsu, P.-I. H. pylori infection and extra-gastroduodenal diseases. J. Biomed. Sci. 2018, 25, 65. [Google Scholar] [CrossRef]
- Fang, Y.; Fan, C.; Xie, H. Effect of Helicobacter pylori infection on the risk of acute coronary syndrome: A systematic review and meta-analysis. Medicine 2019, 98, e18348. [Google Scholar] [CrossRef]
- Szwed, P.; Gąsecka, A.; Zawadka, M.; Eyileten, C.; Postuła, M.; Mazurek, T.; Szarpak, Ł.; Filipiak, K.J. Infections as novel risk factors of atherosclerotic cardiovascular diseases: Pathophysiological links and therapeutic implications. J. Clin. Med. 2021, 10, 2539. [Google Scholar] [CrossRef]
- Doheim, M.F.; Altaweel, A.A.; Elgendy, M.G.; Elshanbary, A.A.; Dibas, M.; Ali, A.; Dahy, T.M.; Sharaf, A.K.; Hassan, A.E. Association between Helicobacter pylori infection and stroke: A meta-analysis of 273, 135 patients. J. Neurol. 2021, 268, 3238–3248. [Google Scholar] [CrossRef]
- Doulberis, M.; Kotronis, G.; Gialamprinou, D.; Polyzos, S.A.; Papaefthymiou, A.; Katsinelos, P.; Kountouras, J. Alzheimer’s disease and gastrointestinal microbiota; impact of Helicobacter pylori infection involvement. Int. J. Neurosci. 2021, 131, 289–301. [Google Scholar] [CrossRef]
- Fu, P.; Gao, M.; Yung, K.K.L. Association of intestinal disorders with Parkinson’s disease and Alzheimer’s disease: A systematic review and meta-analysis. ACS Chem. Neurosci. 2020, 11, 395–405. [Google Scholar] [CrossRef]
- de Brito, B.B.; da Silva, F.A.F.; Soares, A.S.; Pereira, V.A.; Santos, M.L.C.; Sampaio, M.M.; Neves, P.H.M.; de Melo, F.F. Pathogenesis and clinical management of Helicobacter pylori gastric infection. World J. Gastroenterol. 2019, 25, 5578–5589. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; Rokkas, T.; Gisbert, J.P.; Liou, J.M.; Schulz, C.; Gasbarrini, A.; Hunt, R.H.; Leja, M.; O’Morain, C.; et al. Management of Helicobacter pylori infection-the Maastricht VI/Florence consensus report. Gut 2022, 71, 1724–1762. [Google Scholar] [CrossRef]
- Rokkas, T.; Gisbert, J.P.; Malfertheiner, P.; Niv, Y.; Gasbarrini, A.; Leja, M.; Megraud, F.; O’Morain, C.; Graham, D.Y. Comparative effectiveness of multiple different first-line treatment regimens for Helicobacter pylori infection: A network meta-analysis. Gastroenterology 2021, 161, 495–507.e4. [Google Scholar] [CrossRef]
- Aslam, B.; Wang, W.; Arshad, M.I.; Khurshid, M.; Muzammil, S.; Rasool, M.H.; Nisar, M.A.; Alvi, R.F.; Aslam, M.A.; Qamar, M.U.; et al. Antibiotic resistance: A rundown of a global crisis. Infect. Drug Resist. 2018, 11, 1645–1658. [Google Scholar] [CrossRef]
- Bujanda, L.; Nyssen, O.P.; Vaira, D.; Saracino, I.M.; Fiorini, G.; Lerang, F.; Georgopoulos, S.; Tepes, B.; Heluwaert, F.; Gasbarrini, A.; et al. Antibiotic resistance prevalence and trends in patients infected with Helicobacter pylori in the period 2013–2020: Results of the European Registry on H. pylori Management (Hp-EuReg). Antibiotics 2021, 10, 1058. [Google Scholar] [CrossRef]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of antibiotic resistance in Helicobacter pylori: A systematic review and meta-analysis in World Health Organization regions. Gastroenterology 2018, 155, 1372–1382.e17. [Google Scholar] [CrossRef]
- Andreev, D.N.; Maev, I.V.; Dicheva, D.T. Efficiency of the inclusion of rebamipide in the eradication therapy for Helicobacter pylori infection: Meta-analysis of randomized controlled studies. J. Clin. Med. 2019, 8, 1498. [Google Scholar] [CrossRef]
- Higuchi, K.; Watanabe, T.; Tanigawa, T.; Tominaga, K.; Fujiwara, Y.; Arakawa, T. Sofalcone, a gastroprotective drug, promotes gastric ulcer healing following eradication therapy for Helicobacter pylori: A randomized controlled comparative trial with cimetidine, an H2-receptor antagonist. J. Gastroenterol. Hepatol. 2010, 25 (Suppl. 1), S155–S160. [Google Scholar] [CrossRef]
- Teng, G.; Liu, Y.; Wu, T.; Wang, W.; Wang, H.; Hu, F. Efficacy of sucralfate-combined quadruple therapy on gastric mucosal injury induced by Helicobacter pylori and its effect on gastrointestinal flora. BioMed Res. Int. 2020, 2020, 4936318. [Google Scholar] [CrossRef]
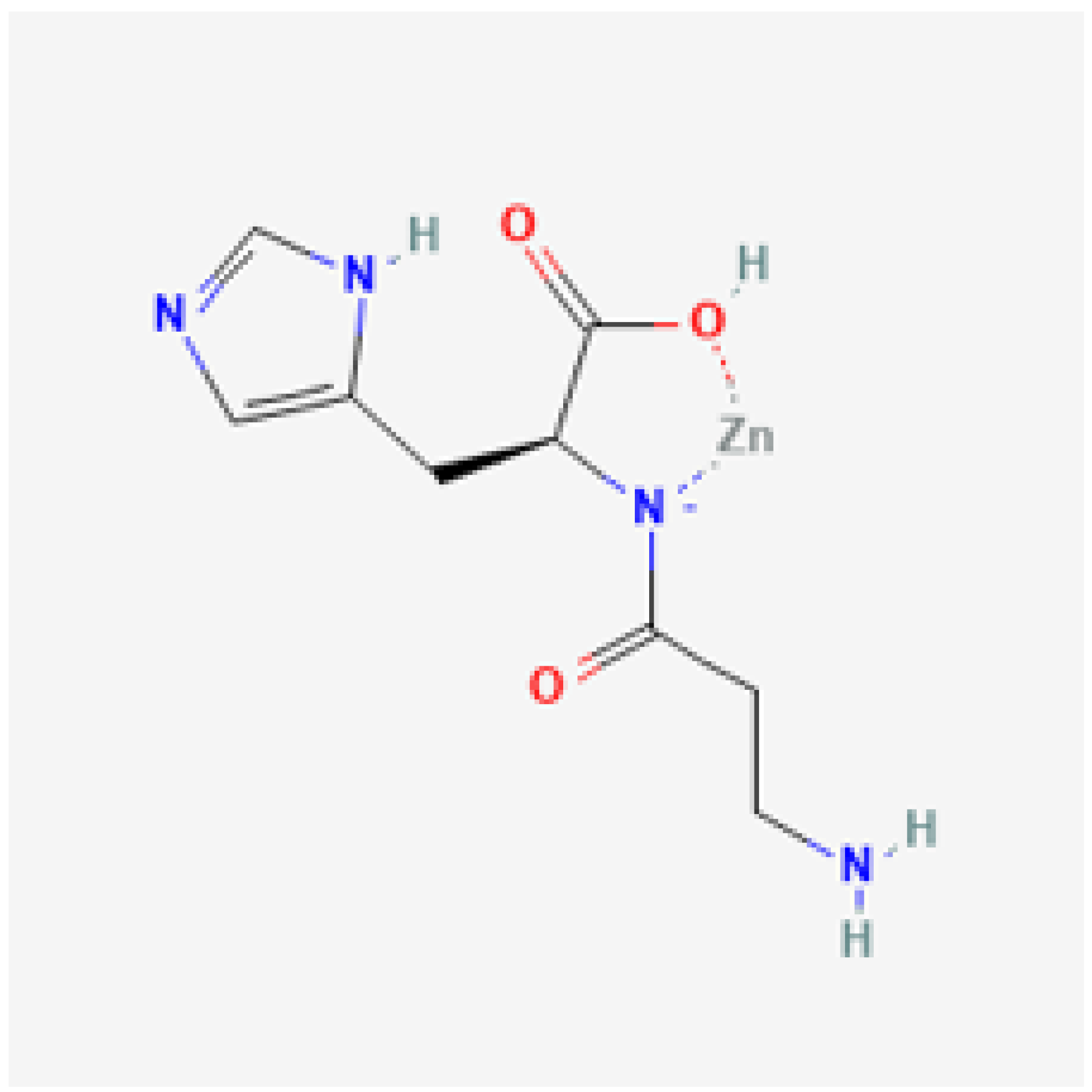
- National Center for Biotechnology Information. PubChem Compound Summary for CID 51051629, Polaprezinc. 2022. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/51051629 (accessed on 3 October 2022).
- Ibrahim, N.; El Said, H.; Choukair, A. Zinc carnosine-based modified bismuth quadruple therapy vs standard triple therapy for Helicobacter pylori eradication: A randomized controlled study. World J. Clin. Cases 2022, 10, 227–235. [Google Scholar] [CrossRef]
- Ishihara, R.; Iishi, H.; Sakai, N.; Yano, H.; Uedo, N.; Narahara, H.; Iseki, K.; Mikuni, T.; Ishiguro, S.; Tatsuta, M. Polaprezinc attenuates Helicobacter pylori-associated gastritis in Mongolian gerbils. Helicobacter 2002, 7, 384–389. [Google Scholar] [CrossRef]
- Isomoto, H.; Furusu, H.; Ohnita, K.; Wen, C.Y.; Inoue, K.; Kohno, S. Sofalcone, a mucoprotective agent, increases the cure rate of Helicobacter pylori infection when combined with rabeprazole, amoxicillin and clarithromycin. World J. Gastroenterol. 2005, 11, 1629–1633. [Google Scholar] [CrossRef]
- Kashimura, H.; Suzuki, K.; Hassan, M.; Ikezawa, K.; Sawahata, T.; Watanabe, T.; Nakahara, A.; Mutoh, H.; Tanaka, N. Polaprezinc, a mucosal protective agent, in combination with lansoprazole, amoxycillin and clarithromycin increases the cure rate of Helicobacter pylori infection. Aliment. Pharmacol. Ther. 1999, 13, 483–487. [Google Scholar] [CrossRef]
- Tan, B.; Luo, H.-Q.; Xu, H.; Lv, N.-H.; Shi, R.-H.; Luo, H.-S.; Li, J.-S.; Ren, J.-L.; Zou, Y.-Y.; Li, Y.-Q.; et al. Polaprezinc combined with clarithromycin-based triple therapy for Helicobacter pylori-associated gastritis: A prospective, multicenter, randomized clinical trial. PLoS ONE 2017, 12, e0175625. [Google Scholar] [CrossRef]
- Hewlings, S.; Kalman, C. A review of zinc-L-carnosine and its positive effects on oral mucositis, taste disorders, and gastrointestinal disorders. Nutirents 2020, 12, 665. [Google Scholar] [CrossRef]
- Kobayashi, H.; Abe, M.; Okada, K.; Tei, R.; Maruyama, N.; Kikuchi, F.; Higuchi, T.; Soma, M. Oral zinc supplementation reduces the erythropoietin responsiveness index in patients on hemodialysis. Nutrients 2015, 7, 3782–3895. [Google Scholar] [CrossRef]
- Kawahara, M.; Tanaka, K.-i.; Kato-Negishi, M. Zinc, carnosine, and neurodegenerative diseases. Nutrients 2018, 10, 147. [Google Scholar] [CrossRef]
- Furihata, K.; Tsuchikawa, M.; Miwa, T.; Naito, Y.; Oba, K.; Sakagami, M. Efficacy and safety of polaprezinc (zinc compound) on zinc deficiency: A systematic review and dose-response meta-analysis of randomized clinical trials using individual patient data. Nutrients 2020, 12, 1128. [Google Scholar] [CrossRef] [PubMed]
- Handa, O.; Yoshida, N.; Tanaka, Y.; Ueda, M.; Ishikawa, T.; Takagi, T.; Matsumoto, N.; Naito, Y.; Yoshikawa, T. Inhibitory effect of polaprezinc on the inflammatory response to Helicobacter pylori. Can. J. Gastroenterol. 2002, 16, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Matsuu-Matsuyama, M.; Shichijo, K.; Okaichi, K.; Nakayama, T.; Nakashima, M.; Uemura, T.; Niino, D.; Sekine, I. Protection by polaprezinc against radiation-induced apoptosis in rat jejunal crypt cells. J. Radiat. Res. 2008, 49, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Omatsu, T.; Naito, Y.; Handa, O.; Mizushima, K.; Hayashi, N.I.; Qin, Y.; Harusato, A.; Hirata, I.; Kishimoto, E.; Okada, H.; et al. Reactive oxygen species-quenching and anti-apoptotic effect of polaprezinc on indomethacin-induced small intestinal epithelial cell injury. J. Gastroenterol. 2010, 45, 692–702. [Google Scholar] [CrossRef] [PubMed]
- Fujii, Y.; Matsura, T.; Kai, M.; Kawasaki, H.; Yamada, K. Protection by polaprezinc, an anti-ulcer drug, against indomethacin-induced apoptosis in rat gastric mucosal cells. Jpn. J. Pharmacol. 2000, 84, 63–70. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zhang, B.; Guo, Y. Supplemental zinc reduced intestinal permeability by enhancing occludin and zonula occludens protein-1 (ZO-1) expression in weaning piglets. Br. J. Nutr. 2009, 102, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Finamore, A.; Massimi, M.; Conti Devirgiliis, L.; Mengheri, E. Zinc deficiency induces membrane barrier damage and increases neutrophil transmigration in Caco-2 cells. J. Nutr. 2008, 138, 1664–1670. [Google Scholar] [CrossRef]
- Mahmood, A.; FitzGerald, A.J.; Marchbank, T.; Ntatsaki, E.; Murray, D.; Ghosh, S.; Playford, R.J. Zinc carnosine, a health food supplement that stabilises small bowel integrity and stimulates gut repair processes. Gut 2007, 56, 168–175. [Google Scholar] [CrossRef]
- Kato, S.; Tanaka, A.; Ogawa, Y.; Kanatsu, K.; Seto, K.; Yoneda, T.; Takeuchi, K. Effect of polaprezinc on impaired healing of chronic gastric ulcers in adjuvant-induced arthritic rats: Role of insulin-like growth factors (IGF)-1. Med. Sci. Monit. 2001, 7, 20–25. [Google Scholar]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, Ed000142. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Wiley: Chichester, UK, 2019; pp. 1–694. [Google Scholar]
- Covidence. Available online: http://www.covidence.org/ (accessed on 5 September 2022).
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Cochrane Bias Methods Group; Cochrane Statistical Methods Group; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Vist, G.E.; Falck-Ytter, Y.; Schünemann, H.J.; GRADE Working Group. What is “quality of evidence” and why is it important to clinicians? BMJ 2008, 336, 995–998. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Hultcrantz, M.; Rind, D.; Akl, E.A.; Treweek, S.; Mustafa, R.A.; Iorio, A.; Alper, B.S.; Meerpohl, J.J.; Murad, M.H.; Ansari, M.T.; et al. The GRADE Working Group clarifies the construct of certainty of evidence. J. Clin. Epidemiol. 2017, 87, 4–13. [Google Scholar] [CrossRef]
- RevMan. Available online: https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman (accessed on 5 September 2022).
- Leja, M.; Grinberga-Derica, I.; Bilgilier, C.; Steininger, C. Review: Epidemiology of Helicobacter pylori infection. Helicobacter 2019, 24 (Suppl. 1), e12635. [Google Scholar] [CrossRef]
- Dunn, B.E.; Cohen, H.; Blaser, M.J. Helicobacter pylori. Clin. Microbiol. Rev. 1997, 10, 720–741. [Google Scholar] [CrossRef]
- Peek, R.M., Jr.; Crabtree, J.E. Helicobacter infection and gastric neoplasia. J. Pathol. 2006, 208, 233–248. [Google Scholar] [CrossRef]
- Matsukura, T.; Tanaka, H. Applicability of zinc complex of L-carnosine for medical use. Biochemistry 2000, 65, 817–823. [Google Scholar]
- Yakoob, J.; Abbas, Z.; Jafri, W.; Usman, M.W.; Awan, S. Zinc chloride inhibits Helicobacter pylori growth and reduces expression of interleukin-1beta by gastric epithelial cells. Br. J. Biomed. Sci. 2014, 71, 43–45. [Google Scholar] [CrossRef]
- Amin, M.; Iqbal, M.S.; Hughes, R.W.; Khan, S.A.; Reynolds, P.A.; Enne, V.I.; Rahman, S.-U.; Mirza, A.S. Mechanochemical synthesis and in vitro anti-Helicobacter pylori and uresase inhibitory activities of novel zinc(II)–famotidine complex. J. Enzyme Inhib. Med. Chem. 2010, 25, 383–390. [Google Scholar] [CrossRef]
- Fan, D.; Gong, Y.; Sun, L.; Zhang, Y.; Zhang, J. Comparative transcriptome analysis to investigate the mechanism of anti-Helicobacter pylori activity of zinc. Microb. Pathog. 2022, 168, 105611. [Google Scholar] [CrossRef]
- Raetz, C.R.H.; Whitfield, C. Lipopolysaccharide endotoxins. Annu. Rev. Biochem. 2003, 71, 635–700. [Google Scholar] [CrossRef]
- Sakae, K.; Yanagisawa, H. Oral treatment of pressure ulcers with polaprezinc (zinc L-carnosine complex): 8-week open-label trial. Biol. Trace Elem. Res. 2014, 158, 280–288. [Google Scholar] [CrossRef]
- Chinese Study Group on Helicobacter pylori; Liu, W.Z.; Xie, Y.; Cheng, H.; Lu, N.H.; Hu, F.L.; Zhang, W.D.; Zhou, L.Y.; Chen, Y.; Zeng, Z.R.; et al. Fourth Chinese National Consensus Report on the management of Helicobacter pylori infection. J. Dig. Dis. 2013, 14, 211–221. [Google Scholar] [CrossRef]
- Graham, D.Y. Hp-normogram (normo-graham) for assessing the outcome of H. pylori therapy: Effect of resistance, curation, and CYP2C19 genotype. Helicobacter 2016, 21, 85–90. [Google Scholar] [CrossRef]





| Database | Search Terms | Search Field | Search Results |
|---|---|---|---|
| PubMed | (polaprezinc OR zinc OR zn OR carnosine OR “zinc carnosine”) AND ((Helicobacter pylori) OR (H. pylori)) | All Field | 245 |
| Cochrane | (polaprezinc OR zinc OR zn OR carnosine OR “zinc carnosine”) AND ((Helicobacter pylori) OR (H. pylori)) | All Field | 23 |
| WOS | (polaprezinc OR zinc OR zn OR carnosine OR “zinc carnosine”) AND ((Helicobacter pylori) OR (H. pylori)) | All Field | 521 |
| SCOPUS | (polaprezinc OR zinc OR zn OR carnosine OR “zinc carnosine”) AND ((Helicobacter pylori) OR (H. pylori)) | Title, Abstract, | 422 |
| EMBASE | #3. 1 AND #2 #2.‘Helicobacter pylori’: ti,ab,kw OR ‘H. pylori’: ti,ab,kw #1.zinc: ti,ab,kw OR carnosine: ti,ab,kw OR polaprezinc: ti,ab,kw | All Field | 259 |
| Google Scholar | Allintitle: polaprezinc pylori | Allintitle | 26 |
| Study ID | Study Design | Country | Total Participants | Dose and Frequency of Administration | Method of H. pylori Diagnosis | |
|---|---|---|---|---|---|---|
| TT | PZN | |||||
| Isomoto et al. [26] 2005 | RCT | Single center in China | 111 | Rabeprazole (10 mg twice daily), clarithromycin (200 mg twice daily) and amoxicillin (750 mg twice daily). | PZN 150 mg twice daily for 7 days | Serology (anti-H. pylori immunoglobulin G antibody and histology (Giemsa staining) using two biopsy specimens obtained during endoscopy from each antrum) |
| Kashimura et al. [27] 1999 | RCT | Single center in Japan | 66 | Lansoprazole 30 mg twice, amoxicillin 500 twice, clarithromycin 400 mg twice for 7 days | PZN 150 mg twice daily for 7 days | Rapid urease test, histology, and culture |
| Tan et al. [28] 2017 | RCT | Single center in China | 219 | Omeprazole 20 mg, amoxicillin 1 g, and clarithromycin 500 mg, each twice daily | PZN 150 mg twice daily for 14 days | 13C or 14C urea breath test and esophagogastroduodenoscopy (EGD) |
| Study ID | Number of Patients | Age (Year) Mean (Range) Mean ± SD | Gender (Male) N. (%) | Gastric Ulcer N. (%) | Duodenal Ulcer N. (%) | Gastroduodenal Ulcers N. (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PZN | TT | PZN | TT | PZN | TT | PZN | TT | PZN | TT | PZN | TT | |
| Isomoto et al. [26] 2005 | 56 | 55 | 45.6 (21–71) | 45.3 (21–73) | 42 (75%) | 41 (74.5%) | 36 (64.3%) | 34 (61.8%) | 19 (33.9%) | 19 (34.5) | 1 (1.8%) | 2 (3.6%) |
| Kashimura et al. [27] 1999 | 35 | 31 | 53.7 (25–70) | 55.3 (22–72) | 22 (62.8%) | 25 (80.6%) | 4 (11.4%) | 4 (12.9%) | 7 (20%) | 9 (31%) | 2 (2.71%) | 2 (6.45%) |
| Tan et al. [28] 2017 | 108 | 111 | 40.5 ± 13.6 | 41.0 ± 11.8 | 58 (53.7) | 58 (52.3) | N/A | N/A | N/A | N/A | N/A | N/A |
| Certainty assessment | № of Patients | Effect | Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Primary Outcome | Placebo | Relative (95% CI) | Absolute (95% CI) | ||
| Intention to treat H. pylori eradication rate | ||||||||||||
| 3 | RCTs | Very serious a | Not serious | Not serious | Serious b | None | 160/199 (80.4%) | 132/197 (67.0%) | OR 2.01 (1.27 to 3.21) | 133 more per 1000 (from 51 more to 197 more) | ⨁◯◯◯ Very low | CRITICAL |
| Per-protocol H. pylori eradication rate | ||||||||||||
| 3 | RCTs | Very serious a | Not serious | Not serious | Seriousb | None | 158/182 (86.8%) | 129/182 (70.9%) | OR 2.65 (1.55 to 4.54) | 157 more per 1000 (from 82 more to 208 more) | ⨁◯◯◯ Very low | CRITICAL |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahmoud, A.; Abuelazm, M.; Ahmed, A.A.S.; Abdalshafy, H.; Abdelazeem, B.; Brašić, J.R. Efficacy and Safety of Polaprezinc-Based Therapy versus the Standard Triple Therapy for Helicobacter pylori Eradication: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2022, 14, 4126. https://doi.org/10.3390/nu14194126
Mahmoud A, Abuelazm M, Ahmed AAS, Abdalshafy H, Abdelazeem B, Brašić JR. Efficacy and Safety of Polaprezinc-Based Therapy versus the Standard Triple Therapy for Helicobacter pylori Eradication: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. 2022; 14(19):4126. https://doi.org/10.3390/nu14194126
Chicago/Turabian StyleMahmoud, Abdelrahman, Mohamed Abuelazm, Ali Ashraf Salah Ahmed, Hassan Abdalshafy, Basel Abdelazeem, and James Robert Brašić. 2022. "Efficacy and Safety of Polaprezinc-Based Therapy versus the Standard Triple Therapy for Helicobacter pylori Eradication: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Nutrients 14, no. 19: 4126. https://doi.org/10.3390/nu14194126
APA StyleMahmoud, A., Abuelazm, M., Ahmed, A. A. S., Abdalshafy, H., Abdelazeem, B., & Brašić, J. R. (2022). Efficacy and Safety of Polaprezinc-Based Therapy versus the Standard Triple Therapy for Helicobacter pylori Eradication: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients, 14(19), 4126. https://doi.org/10.3390/nu14194126