The Interactive Role of Family Functioning among BMI Status, Physical Activity, and High-Fat Food in Adolescents: Evidence from Shanghai, China


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
2.2. Measures
2.2.1. Outcome Variables
2.2.2. Exposure Variables
2.2.3. Dietary Behaviours (DB)
2.2.4. Family Functioning (FF)
2.2.5. Adjusting Variables
2.3. Statistics
3. Results
3.1. Sample Characteristics and BMI Status
3.2. Multinomial Logistic Regression Analysis of BMI Status
3.3. The Multiplicative Interaction among PA, HF, and FF
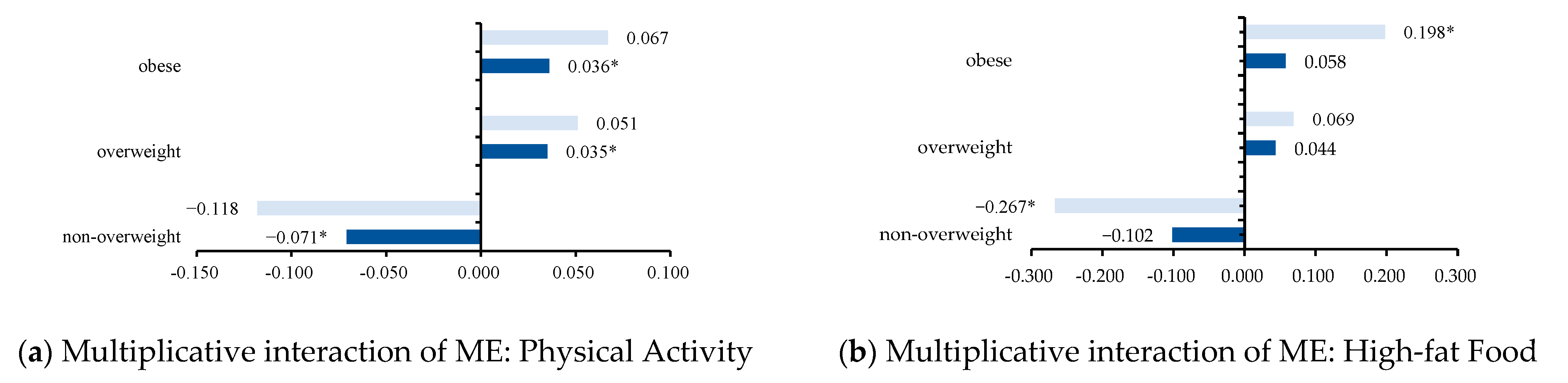
3.4. The Marginal Effects between FF and PA or HF
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| FF | family function |
| PA | physical activity |
| HF | high-fat food |
| DB | dietary behaviour |
| MI | multiplication interaction |
| ME | marginal effect |
References
- Sudore, R.L.; Yaffe, K.; Satterfield, S.; Harris, T.B.; Mehta, K.M.; Simonsick, E.M.; Newman, A.B.; Rosano, C.; Rooks, R.; Rubin, S.M.; et al. Limited literacy and mortality in the elderly: The heat, aging, and body composition study. J. Gen. Intern. Med. 2006, 21, 806–812. [Google Scholar] [CrossRef] [PubMed]
- Sabin, M.A.; Kiess, W. Childhood obesity: Current and novel approaches. Best Pract. Res. Clin. Endocrinol. Metab. 2015, 29, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Yoon, E.Y. Epidemic obesity in children and adolescents: Risk factors and prevention. Front. Med. 2018, 12, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Jin, S.W.; Henning-Smith, C.; Lee, J.; Lee, J. Role of Health Literacy in Health-Related Information-Seeking Behavior Online: Cross-sectional Study. J. Med. Internet Res. 2021, 1, e14088. [Google Scholar] [CrossRef]
- Mond, J.; van den Berg, P.; Boutelle, K.; Hannan, P.; Neumark-Sztainer, D. Obesity, body dissatisfaction, and emotional well-being in early and late adolescence: Findings from the project EAT study. J. Adolesc. Health 2011, 48, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Cooke, L. The impact of obesity on psychological well-being. Best Pract. Res. Clin. Endocrinol. Metab. 2005, 19, 421–440. [Google Scholar] [CrossRef]
- Wang, Y. Cross-national comparison of childhood obesity: The epidemic and the relationship between obesity and socioeconomic status. Int. J. Epidemiol. 2001, 30, 1129–1136. [Google Scholar] [CrossRef]
- Tas, D.; Tüzün, Z.; Düzçeker, Y.; Akgül, S.; Kanbur, N. The effects of parental and peer factors on psychiatric symptoms in adolescents with obesity. Eat Weight Disord. 2020, 25, 617–625. [Google Scholar] [CrossRef]
- Paxton, S.J.; Neumark-Sztainer, D.; Hannan, P.J.; Eisenberg, M.E. Body dissatisfaction prospectively predicts depressive mood and low self-esteem in adolescent girls and boys. J. Clin. Child. Adolesc. Psychol. 2006, 53, 539–549. [Google Scholar] [CrossRef]
- Witte, K.; Allen, M. A meta-analysis of fear appeals: Implications for effective public health campaigns. Health Educ. Behav. 2000, 27, 5. [Google Scholar] [CrossRef]
- Mond, J.M.; Baune, B.T. Overweight, medical comorbidity and health-related quality of life in a community sample of women and men. Obesity 2009, 17, 1627–1634. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.J.; Jackson, T.; Stice, E.; Chen, H. Effectiveness of an Internet Dissonance-Based Eating Disorder Prevention Intervention Among Body-Dissatisfied Young Chinese Women. Behav. Ther. 2021, 52, 221–233. [Google Scholar] [CrossRef] [PubMed]
- Weiland, A.; Nannette, L.K.; Zipfel, S.; Ehehalt, S.; Ziser, K.; Junne, F.; Mack, I. Predictors of Weight Loss and Weight Loss Maintenance in Children and Adolescents with Obesity after Behavioral Weight Loss Intervention. Front. Public Health 2022, 10, 813822. [Google Scholar] [CrossRef] [PubMed]
- Poorolajal, J.; Sahraei, F.; Mohamdadi, Y.; Doosti-Irani, A.; Moradi, L. Behavioral factors influencing childhood obesity: A systematic review and meta-analysis. Obes. Res. Clin. Pract. 2020, 14, 109–118. [Google Scholar] [CrossRef]
- Hosker, D.K.; Elkins, R.M.; Potter, M.P. Promoting Mental Health and Wellness in Youth Through Physical Activity, Nutrition, and Sleep. Child Adolesc. Psychiatr. Clin. N. Am. 2019, 28, 171–193. [Google Scholar] [CrossRef] [PubMed]
- Hills, A.P.; Andersen, L.B.; Byrne, N.M. Physical activity and obesity in children. Br. J. Sports Med. 2011, 45, 866–870. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.C.; Orenstein, M.R.; Richardson, M.J. Systematic review of active commuting to school and childrens physical activity and weight. J. Phys. Act. Health 2008, 5, 930–949. [Google Scholar] [CrossRef]
- Hargreaves, D.; Mates, E.; Menon, P.; Alderman, H.; Devakumar, D.; Fawzi, W.; Greenfield, G.; Hammoudeh, W.; He, S.; Lahiri, A.; et al. Strategies and interventions for healthy adolescent growth, nutrition, and development. Lancet 2022, 399, 198–210. [Google Scholar] [CrossRef]
- Hawkes, C.; Russell, S.; Isaacs, A.; Rutter, H.; Vinter, R. What Can Be Learned from the Amsterdam Healthy Weight Programme to Inform the Policy Response to Obesity in England? Obesity Policy Research Unit (OPRU): Rapid Response Briefing Paper. Available online: https://www.ucl.ac.uk/obesity-policy-research-unit/sites/obesity-policy-research-unit/files/what-learned-from-amsterdam-healthy-weight-programme-inform-policy-response-obesity-england.pdf (accessed on 8 July 2022).
- Tyson, N.; Frank, M. Childhood and adolescent obesity definitions as related to BMI, evaluation and management options. Best Pract. Res. Clin. Obs. Gynaecol. 2018, 48, 158–164. [Google Scholar] [CrossRef]
- Ha, A.; Bae, S.; Urrutia-Rojas, X.; Singh, K.P. Eating and physical activity practices in risk of overweight and overweight children: Compliance with US Department of Agriculture food guide pyramid and with National Association for Sport and Physical Activity guidelines for children. Nutr. Res. 2005, 25, 905–915. [Google Scholar] [CrossRef]
- Silveira, D.; Taddei, J.A.; Escrivão, M.A.; Oliveira, F.L.; Ancona-Lopez, F. Risk factors for overweight among Brazilian adolescents of low-income families: A case–control study. Public Health Nutr. 2006, 9, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Liberali, R.; Kupek, E.; Assis, M.A.A. Dietary Patterns and Childhood Obesity Risk: A Systematic Review. Child. Obes. 2020, 16, 70–85. [Google Scholar] [CrossRef] [PubMed]
- Qin, P.; Liu, D.; Wu, X.; Zeng, Y.; Sun, X.; Zhang, Y.; Li, Y.; Wu, Y.; Han, M.; Qie, R.; et al. Fried-food consumption and risk of overweight/obesity, type 2 diabetes mellitus, and hypertension in adults: A meta-analysis of observational studies. Crit. Rev. Food Sci. Nutr. 2021, 62, 6809–6820. [Google Scholar] [CrossRef] [PubMed]
- Zhen, S.; Ma, Y.; Zhao, Z.; Yang, X.; Wen, D. Dietary pattern is associated with obesity in Chinese children and adolescents: Data from China Health and Nutrition Survey (CHNS). Nutr. J. 2018, 17, 68. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Wang, Y.; Fries, L.R.; Li, Y.; Zhang, N.; Zhang, H.; Wei, H.; Jiang, X.; Shang, L. Infant and preschooler feeding behaviors in Chinese families: A systematic review. Appetite 2022, 168, 105768. [Google Scholar] [CrossRef] [PubMed]
- Okour, A.M.; Saadeh, R.A.; Hijazi, M.H.; Khalaileh, H.; Alfaqih, M.A. Socioeconomic status, perceptions and obesity among adolescents in Jordan. Pan. Afr. Med. J. 2019, 34, 148. [Google Scholar] [CrossRef]
- Scaglioni, S.; Arrizza, C.; Vecchi, F.; Tedeschi, S. Determinants of children’s eating behavior. Am. J. Clin. Nutr. 2011, 94 (Suppl. 6), 2006S–2011S. [Google Scholar] [CrossRef]
- Carbert, N.S.; Brussoni, M.; Geller, J.; Mâsse, L.C. Familial Environment and Overweight/Obese Adolescents’ Physical Activity. Int. J. Env. Res. Public Health 2019, 16, 2558. [Google Scholar] [CrossRef]
- Alderfer, M.A.; Fiese, B.H.; Gold, J.I.; Cutuli, J.J.; Holmbeck, G.N.; Goldbeck, L.; Chambers, C.T.; Abad, M.; Spetter, D.; Patterson, J. Evidence-based assessment in pediatric psychology: Family measures. J. Pediatr. Psychol. 2008, 33, 1046–1064. [Google Scholar] [CrossRef]
- Berge, J.M.; Wall, M.; Larson, N.; Loth, K.A.; Neumark-Sztainer, D. Family functioning: Associations with weight status, eating behaviors, and physical activity in adolescents. J. Adolesc. Health 2013, 52, 351–357. [Google Scholar] [CrossRef]
- Halliday, J.A.; Palma, C.L.; Mellor, D.; Green, J.; Renzaho, A.M. The relationship between family functioning and child and adolescent overweight and obesity: A systematic review. Int. J. Obes. 2014, 38, 480–493. [Google Scholar] [CrossRef] [PubMed]
- Haines, J.; Rifas-Shiman, S.L.; Horton, N.J.; Kleinman, K.; Bauer, K.W.; Davison, K.K.; Walton, K.; Austin, S.B.; Field, A.E.; Gillman, M.W. Family functioning and quality of parent-adolescent relationship: Cross-sectional associations with adolescent weight-related behaviors and weight status. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 68. [Google Scholar] [CrossRef]
- Pratt, K.J.; Skelton, J.A. Family Functioning and Childhood Obesity Treatment: A Family Systems Theory-Informed Approach. Acad. Pediatr. 2018, 18, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Lau, E.Y.; Barr-Anderson, D.J.; Dowda, M.; Forthofer, M.; Saunders, R.P.; Pate, R.R. Associations Between Home Environment and After-School Physical Activity and Sedentary Time Among 6th Grade Children. Pediatr. Exerc. Sci. 2015, 27, 226–233. [Google Scholar] [CrossRef]
- de Sousa, P.M. Body-image and obesity in adolescence: A comparative study of social-demographic, psychological, and behavioral aspects. Span. J. Psychol. 2008, 11, 551–563. [Google Scholar] [CrossRef] [PubMed]
- Kitzmann, K.M.; Dalton, W.T., III; Buscemi, J. Beyond Parenting Practices: Family Context and the Treatment of Pediatric Obesity. Fam. Relat. 2008, 57, 13–23. [Google Scholar] [CrossRef]
- Loth, K.; Wall, M.; Choi, C.W.; Bucchianeri, M.; Quick, V.; Larson, N.; Neumark-Sztainer, D. Family meals and disordered eating in adolescents: Are the benefits the same for everyone? Int. J. Eat Disord. 2015, 48, 100–110. [Google Scholar] [CrossRef]
- Niermann, C.Y.N.; Gerards, S.M.P.L.; Kremers, S.P.J. Conceptualizing Family Influences on Children’s Energy Balance-Related Behaviors: Levels of Interacting Family Environmental Subsystems (The LIFES Framework). Int. J. Environ. Res. Public Health 2018, 15, 2714. [Google Scholar] [CrossRef]
- Dallman, M.F.; Pecoraro, N.C.; la Fleur, S.E. Chronic stress and comfort foods: Self-medication and abdominal obesity. Brain Behav. Immun. 2005, 19, 275–280. [Google Scholar] [CrossRef]
- Warnick, J.L.; Stromberg, S.E.; Krietsch, K.M.; Janicke, D.M. Family functioning mediates the relationship between child behavior problems and parent feeding practices in youth with overweight or obesity. Transl. Behav. Med. 2019, 9, 431–439. [Google Scholar] [CrossRef]
- Ringle, J.F.; Hair, C.M.; Sarstedt, M. PLS-SEM: Indeed a Silver Bullet. J. Mark. Theory Pract. 2011, 19, 139–152. [Google Scholar] [CrossRef]
- Memon, M.; Ting, H.; Hwa, C.; Ramayah, T.; Chuah, F.; Cham, T.H. Sample Size for Survey Research: Review and Recommendations. J. Appl. Struct. Equ. Model. 2020, 4, i. [Google Scholar] [CrossRef]
- Jiang, Y.F.; Cole, T.; Pan, H.Q.; Ju, M.F.; Lin, Z.F.; Dong, X.Y.; Zhang, L. Body mass index percentile curves and cut off points for assessment of overweight and obesity in Shanghai children. World J. Pediatr. 2006, 1, 35–39. [Google Scholar]
- Centers for Disease Control, Youth Risk Behavior Survey. Available online: http://www.cdc.gov/yrbs/ (accessed on 5 July 2022).
- Central Health Education Unit Department of Health, A Qualitative Study on Dietary and Exercise Practices of People in Hong Kong. 2005. Available online: http://www.ssrc.hku.hk/files/reports/health/grp-pmpdb-focus_group_e.pdf (accessed on 5 July 2022).
- Fristad, M.A. A comparison of the McMaster and Circumplex family assessment instruments. J. Marital. Fam. Ther. 1989, 15, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Cong, C.W.; Tan, S.A.; Nainee, S.; Tan, C.S. Psychometric Qualities of the McMaster Family Assessment Device&ndash General Functioning Subscale for Malaysian Samples. Int. J. Environ. Res. Public Health 2022, 19, 2440. [Google Scholar] [CrossRef]
- Shanghai Municipal Government, Healthy Shanghai 2030 Planning Outline [EB/OL]. 2018. Available online: https://wsjkw.sh.gov.cn/sh1/20180525/0012-31275.html (accessed on 5 July 2022).
- Alexander, G.R.; Himes, J.H.; Kaufman, R.B.; Mor, J.; Kogan, M. A United States national reference for fetal growth. Obs. Gynecol. 1996, 87, 163–168. [Google Scholar] [CrossRef]
- Liao, Q.; Zheng, Z.; Xiu, S.; Chan, P. Waist circumference is a better predictor of risk for frailty than BMI in the community-dwelling elderly in Beijing. Aging Clin. Exp. Res. 2018, 30, 1319–1325. [Google Scholar] [CrossRef]
- Wang, S.; Dong, Y.H.; Wang, Z.H.; Zou, Z.Y.; Ma, J. Trends in overweight and obesity among Chinese children of 7-18 years old during 1985–2014. Zhonghua Yu Fang Yi Xue Za Zhi 2017, 51, 300–305. [Google Scholar] [CrossRef]
- Guo, Y.; Yin, X.; Wu, H.; Chai, X.; Yang, X. Trends in Overweight and Obesity Among Children and Adolescents in China from 1991 to 2015: A Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 4656. [Google Scholar] [CrossRef]
- Sun, H.; Ma, Y.; Han, D.; Pan, C.W.; Xu, Y. Prevalence and trends in obesity among China’s children and adolescents, 1985–2010. PLoS ONE 2014, 9, e105469. [Google Scholar] [CrossRef]
- Sagar, R.; Gupta, T. Psychological Aspects of Obesity in Children and Adolescents. Indian J. Pediatr. 2018, 85, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.F.; Wang, L.; Pan, A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021, 9, 373–392. [Google Scholar] [CrossRef]
- Ren, Y.; Campos, B.C.; Loy, J.P.; Brosig, S. Low-income and overweight in China: Evidence from a life-course utility model. J. Integr. Agric. 2019, 18, 1753–1767. [Google Scholar] [CrossRef]
- Mireku, M.O.; Rodriguez, A. Family Income Gradients in Adolescent Obesity, Overweight and Adiposity Persist in Extremely Deprived and Extremely Affluent Neighbourhoods but Not in Middle-Class Neighbourhoods: Evidence from the UK Millennium Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 418. [Google Scholar] [CrossRef] [PubMed]
- Dinsa, G.D.; Goryakin, Y.; Fumagalli, E.; Suhrcke, M. Obesity and socioeconomic status in developing countries: A systematic review. Obes. Rev. 2012, 13, 1067–1079. [Google Scholar] [CrossRef]
- Mazidi, M.; Banach, M.; Kengne, A.P. Prevalence of childhood and adolescent overweight and obesity in Asian countries: A systematic review and meta-analysis. Arch. Med. Sci. 2018, 14, 1185–1203. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Ouidir, M.; Tekola-Ayele, F. Pleiotropic genetic influence on birth weight and childhood obesity. Sci. Rep. 2021, 11, 48. [Google Scholar] [CrossRef]
- Chen, J.; Luo, S.; Liang, X.; Luo, Y.; Li, R. The relationship between socioeconomic status and childhood overweight/obesity is linked through paternal obesity and dietary intake: A cross-sectional study in Chongqing, China. Environ. Health Prev. Med. 2021, 26, 56. [Google Scholar] [CrossRef]
- Gruber, K.J.; Haldeman, L.A. Using the family to combat childhood and adult obesity. Prev. Chronic. Dis. 2009, 6, A106. [Google Scholar]
- Brown, T.; Moore, T.H.; Hooper, L.; Gao, Y.; Zayegh, A.; Ijaz, S.; Elwenspoek, M.; Foxen, S.C.; Magee, L.; O’Malley, C.; et al. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2019, 7, Cd001871. [Google Scholar] [CrossRef]
- Eichen, D.M.; Matheson, B.E.; Liang, J.; Strong, D.R.; Rhee, K.; Boutelle, K.N. The relationship between executive functioning and weight loss and maintenance in children and parents participating in family-based treatment for childhood obesity. Behav. Res. Ther. 2018, 105, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Blissett, J.; Haycraft, E.; Farrow, C. Inducing preschool children’s emotional eating: Relations with parental feeding practices. Am. J. Clin. Nutr. 2010, 92, 359–365. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| BMI Status | n | % | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|---|---|
| Non-overweight | 593 | 63.29 | 18.27 | 1.98 | 13.39 | 22.75 |
| Overweight | 207 | 22.09 | 23.20 | 1.49 | 19.17 | 27.17 |
| Obese | 137 | 14.62 | 28.16 | 2.91 | 23.97 | 42.64 |
| Characteristics | Total | Non-Overweight | Overweight | Obesity | X2 | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |||
| Sex | 56.552 | <0.001 | ||||||||
| Male | 512 | 54.64 | 272 | 45.87 | 133 | 64.25 | 107 | 78.10 | ||
| Female | 425 | 45.36 | 321 | 54.13 | 74 | 35.75 | 30 | 21.90 | ||
| Grade | ||||||||||
| 6th | 362 | 38.63 | 231 | 38.95 | 77 | 37.20 | 54 | 39.42 | 1.494 | 0.828 |
| 7th | 290 | 30.95 | 187 | 31.53 | 60 | 20.69 | 43 | 31.39 | ||
| 8th | 285 | 30.42 | 175 | 29.51 | 70 | 33.82 | 40 | 29.20 | ||
| Age (years) | ||||||||||
| ≤11 | 215 | 22.95 | 132 | 22.26 | 52 | 25.12 | 31 | 22.63 | 0.748 | 0.945 |
| 12 | 279 | 29.78 | 179 | 30.19 | 59 | 28.50 | 41 | 29.93 | ||
| ≥13 | 443 | 47.28 | 282 | 47.55 | 96 | 46.38 | 65 | 47.45 | ||
| Length of stay (years) | ||||||||||
| ≤5 | 50 | 5.34 | 33 | 5.56 | 13 | 6.28 | 4 | 2.92 | 11.014 | 0.026 |
| 5–10 | 779 | 83.14 | 478 | 80.61 | 177 | 85.51 | 124 | 90.51 | ||
| ≥10 | 108 | 11.53 | 82 | 13.83 | 17 | 8.21 | 9 | 6.57 | ||
| Birth weight (kg) | ||||||||||
| ≤2.5 | 22 | 2.35 | 20 | 3.38 | 0 | 0.00 | 2 | 1.46 | 11.239 | 0.024 |
| 2.5–4 | 863 | 92.10 | 544 | 91.74 | 196 | 94.69 | 123 | 89.78 | ||
| ≥4 | 52 | 5.55 | 29 | 4.89 | 11 | 5.31 | 12 | 8.76 | ||
| Primary caretakers | ||||||||||
| Parents | 799 | 89.27 | 514 | 90.18 | 178 | 88.56 | 107 | 86.29 | 7.904 | 0.245 |
| Parental grandparents | 50 | 5.59 | 30 | 5.26 | 9 | 4.48 | 11 | 8.87 | ||
| Maternal grandparents | 39 | 4.436 | 20 | 3.51 | 13 | 6.47 | 6 | 4.84 | ||
| Others | 7 | 0.78 | 6 | 1.05 | 1 | 0.50 | 0 | 0.0 | ||
| Monthly family income (* CNY) | ||||||||||
| ≤3000 | 49 | 5.63 | 27 | 4.84 | 12 | 6.25 | 10 | 8.26 | 19.204 | 0.014 |
| 3001~6000 | 187 | 21.47 | 140 | 25.09 | 31 | 16.15 | 16 | 13.22 | ||
| 6001~9000 | 197 | 22.62 | 120 | 21.51 | 54 | 28.13 | 23 | 19.01 | ||
| 9001~12,000 | 134 | 15.38 | 88 | 15.77 | 26 | 13.54 | 20 | 16.53 | ||
| ≥12,000 | 304 | 34.90 | 183 | 32.8 | 69 | 35.9 | 52 | 43.0 | ||
| Father’s BMI status | ||||||||||
| Non-overweight | 434 | 46.32 | 303 | 51.10 | 89 | 43.00 | 42 | 30.66 | 20.727 | <0.001 |
| Overweight | 402 | 42.90 | 234 | 39.46 | 95 | 45.89 | 73 | 53.28 | ||
| Obese | 101 | 10.78 | 56 | 9.44 | 23 | 11.11 | 22 | 16.06 | ||
| Mother’s BMI status | ||||||||||
| Non-overweight | 711 | 75.88 | 463 | 78.08 | 149 | 71.98 | 99 | 72.26 | 6.335 | 0.175 |
| Overweight | 167 | 17.82 | 92 | 55.09 | 44 | 26.35 | 31 | 18.56 | ||
| Obese | 59 | 6.30 | 38 | 6.41 | 14 | 6.76 | 7 | 5.11 | ||
| Physical activity | ||||||||||
| Active | 253 | 27.00 | 172 | 29.01 | 58 | 28.02 | 23 | 16.79 | 8.567 | 0.014 |
| Not/less active | 684 | 73.00 | 421 | 70.99 | 149 | 71.98 | 114 | 83.21 | ||
| Fruit and vegetable | ||||||||||
| Unhealthy | 208 | 77.80 | 453 | 76.39 | 166 | 80.19 | 110 | 80.29 | 1.861 | 0.394 |
| Healthy | 729 | 22.20 | 140 | 23.61 | 41 | 19.81 | 27 | 19.71 | ||
| Protein and dairy | ||||||||||
| Unhealthy | 276 | 29.46 | 172 | 29.01 | 65 | 31.40 | 39 | 28.47 | 0.499 | 0.779 |
| Healthy | 661 | 70.54 | 421 | 70.99 | 142 | 68.60 | 98 | 71.53 | ||
| High-fat food consumption | ||||||||||
| Unhealthy | 93 | 9.93 | 48 | 8.09 | 23 | 11.11 | 22 | 16.06 | 8.313 | 0.016 |
| Healthy | 844 | 90.07 | 545 | 91.91 | 31 | 88.89 | 26 | 83.94 | ||
| Dietary habits | ||||||||||
| Unhealthy | 184 | 19.64 | 118 | 19.90 | 39 | 18.84 | 27 | 19.71 | 0.109 | 0.947 |
| healthy | 753 | 80.36 | 475 | 80.10 | 168 | 81.16 | 110 | 80.29 | ||
| Family functioning | ||||||||||
| Healthy | 803 | 85.70 | 513 | 86.51 | 182 | 87.92 | 108 | 78.83 | 6.424 | 0.040 |
| Unhealthy | 134 | 14.30 | 80 | 13.49 | 25 | 12.08 | 29 | 21.17 | ||
| Non-Overweight (Reference: Obesity) | Overweight (Reference: Obesity) | |||||||
|---|---|---|---|---|---|---|---|---|
| OR | 95%CI | p | OR | 95%CI | p | |||
| Lower | Upper | Lower | Upper | |||||
| Sex | ||||||||
| Male | 0.229 | 0.142 | 0.369 | <0.001 | 0.538 | 0.316 | 0.915 | 0.022 |
| Female | 1 | reference | - | 1 | reference | - | ||
| Length of stay (years) | ||||||||
| ≤5 | 0.722 | 0.195 | 2.667 | 0.625 | 1.661 | 0.400 | 6.900 | 0.485 |
| 5–10 | 0.535 | 0.248 | 1.150 | 0.109 | 0.997 | 0.414 | 2.401 | 0.995 |
| ≥10 | 1 | reference | - | 1 | reference | - | ||
| Birth weight (kg) | ||||||||
| ≤2.5 | 3.755 | 0.690 | 20.417 | 0.126 | <0.001 | <0.001 | <0.001 | 0.981 |
| 2.5–4 | 2.503 | 1.149 | 5.452 | 0.021 | 2.672 | 1.075 | 6.641 | 0.034 |
| ≥4 | 1 | reference | - | 1 | reference | - | ||
| Monthly family income (* CNY) | ||||||||
| ≤3000 | 0.802 | 0.347 | 1.855 | 0.607 | 0.870 | 0.339 | 2.234 | 0.772 |
| 3001~6000 | 2.432 | 1.289 | 4.589 | 0.006 | 1.324 | 0.645 | 2.721 | 0.444 |
| 6001~9000 | 1.402 | 0.786 | 2.504 | 0.253 | 1.582 | 0.844 | 2.965 | 0.152 |
| 9001~12,000 | 1.509 | 0.811 | 2.809 | 0.194 | 1.007 | 0.495 | 2.047 | 0.985 |
| ≥12,000 | 1 | reference | - | 1 | reference | - | ||
| Father’s BMI status | ||||||||
| Non-overweight | 2.873 | 1.496 | 5.517 | 0.002 | 1.817 | 0.875 | 3.773 | 0.485 |
| Overweight | 1.381 | 0.729 | 2.617 | 0.322 | 1.407 | 0.689 | 2.873 | 0.995 |
| Obese | 1 | reference | - | 1 | reference | - | ||
| Physical Activity | ||||||||
| Active | 2.260 | 1.318 | 3.874 | 0.003 | 2.096 | 1.167 | 3.766 | 0.013 |
| Inactive | 1 | reference | - | 1 | reference | - | ||
| High-fat food consumption | ||||||||
| Healthy | 2.048 | 1.105 | 3.796 | 0.023 | 1.476 | 0.748 | 2.909 | 0.261 |
| Unhealthy | 1 | reference | - | 1 | reference | - | ||
| Family Functioning | ||||||||
| Healthy | 1.336 | 0.785 | 2.272 | 0.285 | 2.084 | 1.099 | 3.952 | 0.025 |
| Unhealthy | 1 | reference | - | 1 | reference | - | ||
| Multiplicative Interaction | Non-Overweight (Reference: Obesity) | Overweight (Reference: Obesity) | |||||
|---|---|---|---|---|---|---|---|
| Family Function | Physical Activity | OR | 95%CI | p | OR | 95%CI | p |
| Healthy | Active | 3.440 | (1.760, 6.722) | <0.001 | 3.870 | (1.719, 8.713) | 0.001 |
| Healthy | Inactive | 1.794 | (1.062, 3.030) | 0.029 | 2.181 | (1.114, 4.272) | 0.023 |
| Unhealthy | Active | 2.522 | (0.790, 8.055) | 0.118 | 2.941 | (0.763, 11.336) | 0.117 |
| Unhealthy | Inactive | 1 | - | 1 | - | ||
| Family function | High-fat food consumption | ||||||
| Healthy | Healthy | 4.989 | (1.930, 12.899) | 0.001 | 5.116 | (1.352, 19.362) | 0.016 |
| Healthy | Unhealthy | 3.000 | (0.982, 9.167) | 0.054 | 4.615 | (1.049, 20.306) | 0.043 |
| Unhealthy | Healthy | 3.550 | (1.244, 10.132) | 0.018 | 3.300 | (0.782, 13.930) | 0.104 |
| Unhealthy | Unhealthy | 1 | - | 1 | - | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, M.; Yin, W.; Sung-Chan, P.; Wang, Z.; Shi, J. The Interactive Role of Family Functioning among BMI Status, Physical Activity, and High-Fat Food in Adolescents: Evidence from Shanghai, China. Nutrients 2022, 14, 4053. https://doi.org/10.3390/nu14194053
Chen M, Yin W, Sung-Chan P, Wang Z, Shi J. The Interactive Role of Family Functioning among BMI Status, Physical Activity, and High-Fat Food in Adolescents: Evidence from Shanghai, China. Nutrients. 2022; 14(19):4053. https://doi.org/10.3390/nu14194053
Chicago/Turabian StyleChen, Mingyue, Wei Yin, Pauline Sung-Chan, Zhaoxin Wang, and Jianwei Shi. 2022. "The Interactive Role of Family Functioning among BMI Status, Physical Activity, and High-Fat Food in Adolescents: Evidence from Shanghai, China" Nutrients 14, no. 19: 4053. https://doi.org/10.3390/nu14194053
APA StyleChen, M., Yin, W., Sung-Chan, P., Wang, Z., & Shi, J. (2022). The Interactive Role of Family Functioning among BMI Status, Physical Activity, and High-Fat Food in Adolescents: Evidence from Shanghai, China. Nutrients, 14(19), 4053. https://doi.org/10.3390/nu14194053