
The Role of Infant Formulas in the Primary Prevention of Allergies in Non-Breastfed Infants at Risk of Developing Allergies—Recommendations from a Multidisciplinary Group of Experts

 ,
,
Abstract
1. Introduction
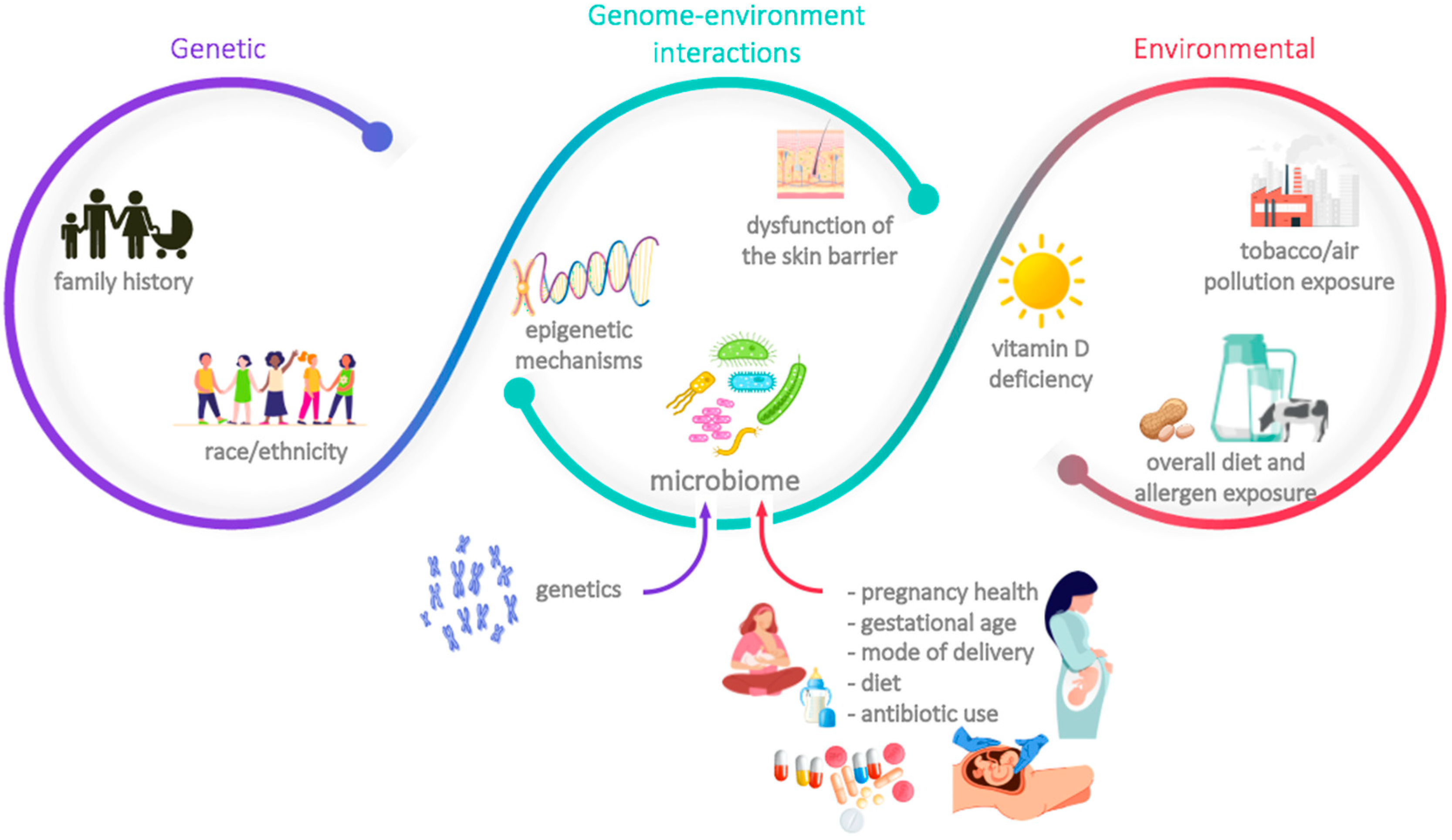
2. Risk Factors for Infant Allergies
2.1. Family History of Atopic Disease
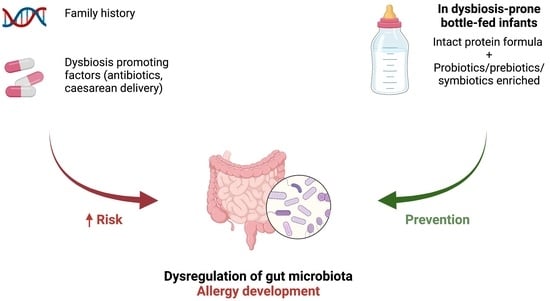
2.2. Dysregulation of the Microbiota
3. The Role of Infant Formulas in Allergy Prevention
3.1. Partially and Extensively Hydrolysed Formulas vs. Intact Protein Formulas
3.2. Synbiotics-Enriched Formulas
4. International Guidelines and Regulatory Authorities
5. Expert Comment
- -
- Allergy-related familial history and the presence of dysbiosis-promoting factors (namely pre-, peri-, or post-partum antibiotic exposure and caesarean delivery) should be evaluated during the infant’s initial medical appointments in order to ascertain the risk of allergy.
- -
- When exclusive breastfeeding is not an option, intact protein cow’s milk-based formula should be used to feed or supplement healthy infants, irrespective of their allergy risk *.
- -
- Without disregarding the previous point, the short-term bottle feeding of otherwise breastfed babies up to 1 week of age should be avoided (as breastmilk is usually sufficient); however, and when needed, adequate supplementary options include donor breast milk, eHF, or AAF, although it should be acknowledged that these options are expensive *.
- -
- A probiotic-, prebiotic-, or synbiotic-enriched formula should be considered in non-breastfed infants who are at risk of developing allergies *.
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yang, L.; Fu, J.; Zhou, Y. Research Progress in Atopic March. Front. Immunol. 2020, 11, 1907. [Google Scholar] [CrossRef] [PubMed]
- Warren, C.M.; Jiang, J.; Gupta, R.S. Epidemiology and Burden of Food Allergy. Curr. Allergy Asthma Rep. 2020, 20, 6. [Google Scholar] [CrossRef] [PubMed]
- Sicherer, S.H.; Sampson, H.A. Food Allergy: A Review and Update on Epidemiology, Pathogenesis, Diagnosis, Prevention, and Management. J. Allergy Clin. Immunol. 2018, 141, 41–58. [Google Scholar] [CrossRef] [PubMed]
- D’Auria, E.; Salvatore, S.; Pozzi, E.; Mantegazza, C.; Sartorio, M.U.A.; Pensabene, L.; Baldassarre, M.E.; Agosti, M.; Vandenplas, Y.; Zuccotti, G. Cow’s Milk Allergy: Immunomodulation by Dietary Intervention. Nutrients 2019, 11, 1399. [Google Scholar] [CrossRef] [PubMed]
- Flom, J.D.; Sicherer, S.H. Epidemiology of Cow’s Milk Allergy. Nutrients 2019, 11, 1051. [Google Scholar] [CrossRef] [PubMed]
- Langan, S.M.; Irvine, A.D.; Weidinger, S. Atopic Dermatitis. Lancet 2020, 396, 345–360. [Google Scholar] [CrossRef]
- Stern, J.; Pier, J.; Litonjua, A.A. Asthma Epidemiology and Risk Factors. Semin. Immunopathol. 2020, 42, 5–15. [Google Scholar] [CrossRef]
- Bylund, S.; Kobyletzki, L.B.; Svalstedt, M.; Svensson, Å. Prevalence and Incidence of Atopic Dermatitis: A Systematic Review. Acta Derm. Venereol. 2020, 100, adv00160. [Google Scholar] [CrossRef]
- Kuruvilla, M.E.; Vanijcharoenkarn, K.; Shih, J.A.; Lee, F.E.-H. Epidemiology and Risk Factors for Asthma. Respir. Med. 2019, 149, 16–22. [Google Scholar] [CrossRef]
- World Health Organization; UNICEF. Global Strategy for Infant and Young Child Feeding; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Dipasquale, V.; Serra, G.; Corsello, G.; Romano, C. Standard and Specialized Infant Formulas in Europe: Making, Marketing, and Health Outcomes. Nutr. Clin. Pract. 2020, 35, 273–281. [Google Scholar] [CrossRef]
- Salminen, S.J.; Szajewska, H.; Knol, J. (Eds.) The Biotics Family in Early Life; Wiley: West Sussex, UK, 2019. [Google Scholar]
- Renz, H.; Skevaki, C. Early Life Microbial Exposures and Allergy Risks: Opportunities for Prevention. Nat. Rev. Immunol. 2021, 21, 177–191. [Google Scholar] [CrossRef] [PubMed]
- Cukrowska, B.; Bierła, J.B.; Zakrzewska, M.; Klukowski, M.; Maciorkowska, E. The Relationship between the Infant Gut Microbiota and Allergy. The Role of Bifidobacterium Breve and Prebiotic Oligosaccharides in the Activation of Anti-Allergic Mechanisms in Early Life. Nutrients 2020, 12, 946. [Google Scholar] [CrossRef] [PubMed]
- Kumar, H.; Collado, M.C.; Wopereis, H.; Salminen, S.; Knol, J.; Roeselers, G. The Bifidogenic Effect Revisited-Ecology and Health Perspectives of Bifidobacterial Colonization in Early Life. Microorganisms 2020, 8, 1855. [Google Scholar] [CrossRef]
- Vandenplas, Y.; Carnielli, V.P.; Ksiazyk, J.; Luna, M.S.; Migacheva, N.; Mosselmans, J.M.; Picaud, J.C.; Possner, M.; Singhal, A.; Wabitsch, M. Factors Affecting Early-Life Intestinal Microbiota Development. Nutrition 2020, 78, 110812. [Google Scholar] [CrossRef] [PubMed]
- Shu, S.-A.; Yuen, A.W.T.; Woo, E.; Chu, K.-H.; Kwan, H.-S.; Yang, G.-X.; Yang, Y.; Leung, P.S.C. Microbiota and Food Allergy. Clin. Rev. Allergy Immunol. 2019, 57, 83–97. [Google Scholar] [CrossRef]
- Zhao, W.; Ho, H.-E.; Bunyavanich, S. The Gut Microbiome in Food Allergy. Ann. Allergy Asthma Immunol. 2019, 122, 276–282. [Google Scholar] [CrossRef]
- Wypych, T.P.; Marsland, B.J. Antibiotics as Instigators of Microbial Dysbiosis: Implications for Asthma and Allergy. Trends Immunol. 2018, 39, 697–711. [Google Scholar] [CrossRef]
- Iweala, O.I.; Nagler, C.R. The Microbiome and Food Allergy. Annu. Rev. Immunol. 2019, 37, 377–403. [Google Scholar] [CrossRef]
- Stephen-Victor, E.; Crestani, E.; Chatila, T.A. Dietary and Microbial Determinants in Food Allergy. Immunity 2020, 53, 277–289. [Google Scholar] [CrossRef]
- De Filippis, F.; Paparo, L.; Nocerino, R.; Della Gatta, G.; Carucci, L.; Russo, R.; Pasolli, E.; Ercolini, D.; Berni Canani, R. Specific Gut Microbiome Signatures and the Associated Pro-Inflamatory Functions Are Linked to Pediatric Allergy and Acquisition of Immune Tolerance. Nat. Commun. 2021, 12, 5958. [Google Scholar] [CrossRef]
- Huang, Y.J.; Marsland, B.J.; Bunyavanich, S.; O’Mahony, L.; Leung, D.Y.M.; Muraro, A.; Fleisher, T.A. The Microbiome in Allergic Disease: Current Understanding and Future Opportunities-2017 PRACTALL Document of the American Academy of Allergy, Asthma & Immunology and the European Academy of Allergy and Clinical Immunology. J. Allergy Clin. Immunol. 2017, 139, 1099–1110. [Google Scholar] [CrossRef] [PubMed]
- Bunyavanich, S.; Berin, M.C. Food Allergy and the Microbiome: Current Understandings and Future Directions. J. Allergy Clin. Immunol. 2019, 144, 1468–1477. [Google Scholar] [CrossRef]
- Aguilera, A.C.; Dagher, I.A.; Kloepfer, K.M. Role of the Microbiome in Allergic Disease Development. Curr. Allergy Asthma Rep. 2020, 20, 44. [Google Scholar] [CrossRef] [PubMed]
- Wopereis, H.; Oozeer, R.; Knipping, K.; Belzer, C.; Knol, J. The First Thousand Days-Intestinal Microbiology of Early Life: Establishing a Symbiosis. Pediatr. Allergy Immunol. 2014, 25, 428–438. [Google Scholar] [CrossRef] [PubMed]
- Berni Canani, R.; Paparo, L.; Nocerino, R.; Di Scala, C.; Della Gatta, G.; Maddalena, Y.; Buono, A.; Bruno, C.; Voto, L.; Ercolini, D. Gut Microbiome as Target for Innovative Strategies Against Food Allergy. Front. Immunol. 2019, 10, 191. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies. Scientific Opinion on the Essential Composition of Infant and Follow-on Formulae. EFSA J. 2014, 12, 3760. [Google Scholar] [CrossRef]
- Cabana, M.D. The Role of Hydrolyzed Formula in Allergy Prevention. Ann. Nutr. Metab. 2017, 70 (Suppl. 2), 38–45. [Google Scholar] [CrossRef]
- Hays, T.; Wood, R.A. A Systematic Review of the Role of Hydrolyzed Infant Formulas in Allergy Prevention. Arch. Pediatr. Adolesc. Med. 2005, 159, 810–816. [Google Scholar] [CrossRef]
- de Silva, D.; Geromi, M.; Halken, S.; Host, A.; Panesar, S.S.; Muraro, A.; Werfel, T.; Hoffmann-Sommergruber, K.; Roberts, G.; Cardona, V.; et al. Primary Prevention of Food Allergy in Children and Adults: Systematic Review. Allergy 2014, 69, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Committee on Nutrition. Hypoallergenic Infant Formulas. Pediatrics 2000, 106, 346–349. [Google Scholar] [CrossRef]
- Fleischer, D.M.; Spergel, J.M.; Assa’ad, A.H.; Pongracic, J.A. Primary Prevention of Allergic Disease through Nutritional Interventions. J. Allergy Clin. Immunol. Pract. 2013, 1, 29–36. [Google Scholar] [CrossRef]
- Høst, A.; Koletzko, B.; Dreborg, S.; Muraro, A.; Wahn, U.; Aggett, P.; Bresson, J.L.; Hernell, O.; Lafeber, H.; Michaelsen, K.F.; et al. Dietary Products Used in Infants for Treatment and Prevention of Food Allergy. Joint Statement of the European Society for Paediatric Allergology and Clinical Immunology (ESPACI) Committee on Hypoallergenic Formulas and the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) Committee on Nutrition. Arch. Dis. Child. 1999, 81, 80–84. [Google Scholar] [CrossRef]
- Muraro, A.; Halken, S.; Arshad, S.H.; Beyer, K.; Dubois, A.E.J.; Du Toit, G.; Eigenmann, P.A.; Grimshaw, K.E.C.; Hoest, A.; Lack, G.; et al. EAACI Food Allergy and Anaphylaxis Guidelines. Primary Prevention of Food Allergy. Allergy 2014, 69, 590–601. [Google Scholar] [CrossRef] [PubMed]
- Boyle, R.J.; Ierodiakonou, D.; Khan, T.; Chivinge, J.; Robinson, Z.; Geoghegan, N.; Jarrold, K.; Afxentiou, T.; Reeves, T.; Cunha, S.; et al. Hydrolysed Formula and Risk of Allergic or Autoimmune Disease: Systematic Review and Meta-Analysis. BMJ 2016, 352, i974. [Google Scholar] [CrossRef]
- Burke, M.; Chan, E.S.; Abrams, E.M. Should We Continue to Counsel Families to Use Hydrolyzed Formulas as a Means of Allergy Prevention in High-Risk Infants? Paediatr. Child Health 2020, 25, 79–81. [Google Scholar] [CrossRef] [PubMed]
- Lodge, C.J.; Allen, K.J.; Lowe, A.J.; Dharmage, S.C. Overview of Evidence in Prevention and Aetiology of Food Allergy: A Review of Systematic Reviews. Int. J. Environ. Res. Public Health 2013, 10, 5781–5806. [Google Scholar] [CrossRef] [PubMed]
- Golpanian, R.S.; Aickara, D.J.; Bellodi Schmidt, F.; Smith, P.K.; Yosipovitch, G. Hydrolysed Formula, Delayed Food Introduction and Fatty Acids for Atopic Dermatitis Prevention in Infancy. Acta Paediatr. 2021, 110, 1784–1787. [Google Scholar] [CrossRef]
- Vandenplas, Y.; Meyer, R.; Chouraqui, J.-P.; Dupont, C.; Fiocchi, A.; Salvatore, S.; Shamir, R.; Szajewska, H.; Thapar, N.; Venter, C.; et al. The Role of Milk Feeds and Other Dietary Supplementary Interventions in Preventing Allergic Disease in Infants: Fact or Fiction? Clin. Nutr. 2021, 40, 358–371. [Google Scholar] [CrossRef]
- Osborn, D.A.; Sinn, J.K.; Jones, L.J. Infant Formulas Containing Hydrolysed Protein for Prevention of Allergic Disease. Cochrane Database Syst. Rev. 2018, 10, CD003664. [Google Scholar] [CrossRef]
- Urashima, M.; Mezawa, H.; Okuyama, M.; Urashima, T.; Hirano, D.; Gocho, N.; Tachimoto, H. Primary Prevention of Cow’s Milk Sensitization and Food Allergy by Avoiding Supplementation With Cow’s Milk Formula at Birth: A Randomized Clinical Trial. JAMA Pediatr. 2019, 173, 1137–1145. [Google Scholar] [CrossRef]
- Davisse-Paturet, C.; Raherison, C.; Adel-Patient, K.; Divaret-Chauveau, A.; Bois, C.; Dufourg, M.-N.; Lioret, S.; Charles, M.-A.; de Lauzon-Guillain, B. Use of Partially Hydrolysed Formula in Infancy and Incidence of Eczema, Respiratory Symptoms or Food Allergies in Toddlers from the ELFE Cohort. Pediatr. Allergy Immunol. 2019, 30, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Katz, Y.; Rajuan, N.; Goldberg, M.R.; Eisenberg, E.; Heyman, E.; Cohen, A.; Leshno, M. Early Exposure to Cow’s Milk Protein Is Protective against IgE-Mediated Cow’s Milk Protein Allergy. J. Allergy Clin. Immunol. 2010, 126, 77–82.e1. [Google Scholar] [CrossRef]
- Onizawa, Y.; Noguchi, E.; Okada, M.; Sumazaki, R.; Hayashi, D. The Association of the Delayed Introduction of Cow’s Milk with IgE-Mediated Cow’s Milk Allergies. J. Allergy Clin. Immunol. Pract. 2016, 4, 481–488.e2. [Google Scholar] [CrossRef] [PubMed]
- Peters, R.L.; Koplin, J.J.; Dharmage, S.C.; Tang, M.L.K.; McWilliam, V.L.; Gurrin, L.C.; Neeland, M.R.; Lowe, A.J.; Ponsonby, A.-L.; Allen, K.J. Early Exposure to Cow’s Milk Protein Is Associated with a Reduced Risk of Cow’s Milk Allergic Outcomes. J. Allergy Clin. Immunol. Pract. 2019, 7, 462–470.e1. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.R.; Ling, P.-R.; Blackburn, G.L. Review of Infant Feeding: Key Features of Breast Milk and Infant Formula. Nutrients 2016, 8, 279. [Google Scholar] [CrossRef]
- Gibson, G.R.; Hutkins, R.; Sanders, M.E.; Prescott, S.L.; Reimer, R.A.; Salminen, S.J.; Scott, K.; Stanton, C.; Swanson, K.S.; Cani, P.D.; et al. Expert Consensus Document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) Consensus Statement on the Definition and Scope of Prebiotics. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 491–502. [Google Scholar] [CrossRef]
- Report of a Joint FAO/WHO Expert Consultation on Evaluation of Health and Nutritional Properties of Probiotics in Food Including Powder Milk with Live Lactic Acid Bacteria, Cordoba, Argentina, 1–4 October 2001; FAO/WHO: Rome, Italy, 2006.
- World Gastroenterology Organisation. WGO Global Guidelines: Probiotics and Prebiotics; WGO: Milwaukee, WI, USA, 2017. [Google Scholar]
- Halken, S.; Muraro, A.; de Silva, D.; Khaleva, E.; Angier, E.; Arasi, S.; Arshad, H.; Bahnson, H.T.; Beyer, K.; Boyle, R.; et al. EAACI Guideline: Preventing the Development of Food Allergy in Infants and Young Children (2020 Update). Pediatr. Allergy Immunol. 2021, 32, 843–858. [Google Scholar] [CrossRef]
- Joshi, P.A.; Smith, J.; Vale, S.; Campbell, D.E. The Australasian Society of Clinical Immunology and Allergy Infant Feeding for Allergy Prevention Guidelines. Med. J. Aust. 2019, 210, 89–93. [Google Scholar] [CrossRef]
- Greer, F.R.; Sicherer, S.H.; Burks, A.W. The Effects of Early Nutritional Interventions on the Development of Atopic Disease in Infants and Children: The Role of Maternal Dietary Restriction, Breastfeeding, Hydrolyzed Formulas, and Timing of Introduction of Allergenic Complementary Foods. Pediatrics 2019, 143, e20190281. [Google Scholar] [CrossRef]
- Castenmiller, J.; Hirsch-Ernst, K.-I.; Kearney, J.; Knutsen, H.K.; Maciuk, A.; Mangelsdorf, I.; McArdle, H.J.; Naska, A.; Pelaez, C.; Pentieva, K.; et al. Efficacy of an Infant Formula Manufactured from a Specific Protein Hydrolysate Derived from Whey Protein Isolate and Concentrate Produced by Société Des Produits Nestlé S.A. in Reducing the Risk of Developing Atopic Dermatitis. EFSA J. 2021, 19, e06603. [Google Scholar] [CrossRef]
- Cuello-Garcia, C.A.; Fiocchi, A.; Pawankar, R.; Yepes-Nuñez, J.J.; Morgano, G.P.; Zhang, Y.; Ahn, K.; Al-Hammadi, S.; Agarwal, A.; Gandhi, S.; et al. World Allergy Organization-McMaster University Guidelines for Allergic Disease Prevention (GLAD-P): Prebiotics. World Allergy Organ. J. 2016, 9, 10. [Google Scholar] [CrossRef] [PubMed]
- Fiocchi, A.; Pawankar, R.; Cuello-Garcia, C.; Ahn, K.; Al-Hammadi, S.; Agarwal, A.; Beyer, K.; Burks, W.; Canonica, G.W.; Ebisawa, M.; et al. World Allergy Organization-McMaster University Guidelines for Allergic Disease Prevention (GLAD-P): Probiotics. World Allergy Organ. J. 2015, 8, 4. [Google Scholar] [CrossRef] [PubMed]
- Vale, S.L.; Lobb, M.; Netting, M.J.; Murray, K.; Clifford, R.; Campbell, D.E.; Salter, S.M. A Systematic Review of Infant Feeding Food Allergy Prevention Guidelines-Can We AGREE? World Allergy Organ. J. 2021, 14, 100550. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| International Society/ Regulatory Entity | Recommendations Concerning *: | |
|---|---|---|
| Hydrolysed Formulas vs. Intact Protein Cow’s Milk Formulas | Addition of Prebiotics, Probiotics, and Synbiotics to Infant Formulas | |
| EAACI 2020 [51] |
|
|
| ASCIA 2019 [52] |
| - |
| AAP 2019 [53] |
| - |
| EFSA 2021 [54] |
| - |
| WAO 2015 [56] | - |
|
| WAO 2016 [55] | - |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dias, J.A.; Santos, E.; Asseiceira, I.; Jacob, S.; Koninckx, C.R. The Role of Infant Formulas in the Primary Prevention of Allergies in Non-Breastfed Infants at Risk of Developing Allergies—Recommendations from a Multidisciplinary Group of Experts. Nutrients 2022, 14, 4016. https://doi.org/10.3390/nu14194016
Dias JA, Santos E, Asseiceira I, Jacob S, Koninckx CR. The Role of Infant Formulas in the Primary Prevention of Allergies in Non-Breastfed Infants at Risk of Developing Allergies—Recommendations from a Multidisciplinary Group of Experts. Nutrients. 2022; 14(19):4016. https://doi.org/10.3390/nu14194016
Chicago/Turabian StyleDias, Jorge Amil, Edmundo Santos, Inês Asseiceira, Sylvia Jacob, and Carmen Ribes Koninckx. 2022. "The Role of Infant Formulas in the Primary Prevention of Allergies in Non-Breastfed Infants at Risk of Developing Allergies—Recommendations from a Multidisciplinary Group of Experts" Nutrients 14, no. 19: 4016. https://doi.org/10.3390/nu14194016
APA StyleDias, J. A., Santos, E., Asseiceira, I., Jacob, S., & Koninckx, C. R. (2022). The Role of Infant Formulas in the Primary Prevention of Allergies in Non-Breastfed Infants at Risk of Developing Allergies—Recommendations from a Multidisciplinary Group of Experts. Nutrients, 14(19), 4016. https://doi.org/10.3390/nu14194016