
Measured Energy Expenditure Using Indirect Calorimetry in Post-Intensive Care Unit Hospitalized Survivors: A Comparison with Predictive Equations

Abstract
1. Introduction
2. Materials and Methods
2.1. Population
2.2. Indirect Calorimetry
2.3. Estimated Energy Expenditure
2.4. Other Clinical Data
2.5. Statistical Analysis
3. Results
3.1. Patients
3.2. Indirect Calorimetry
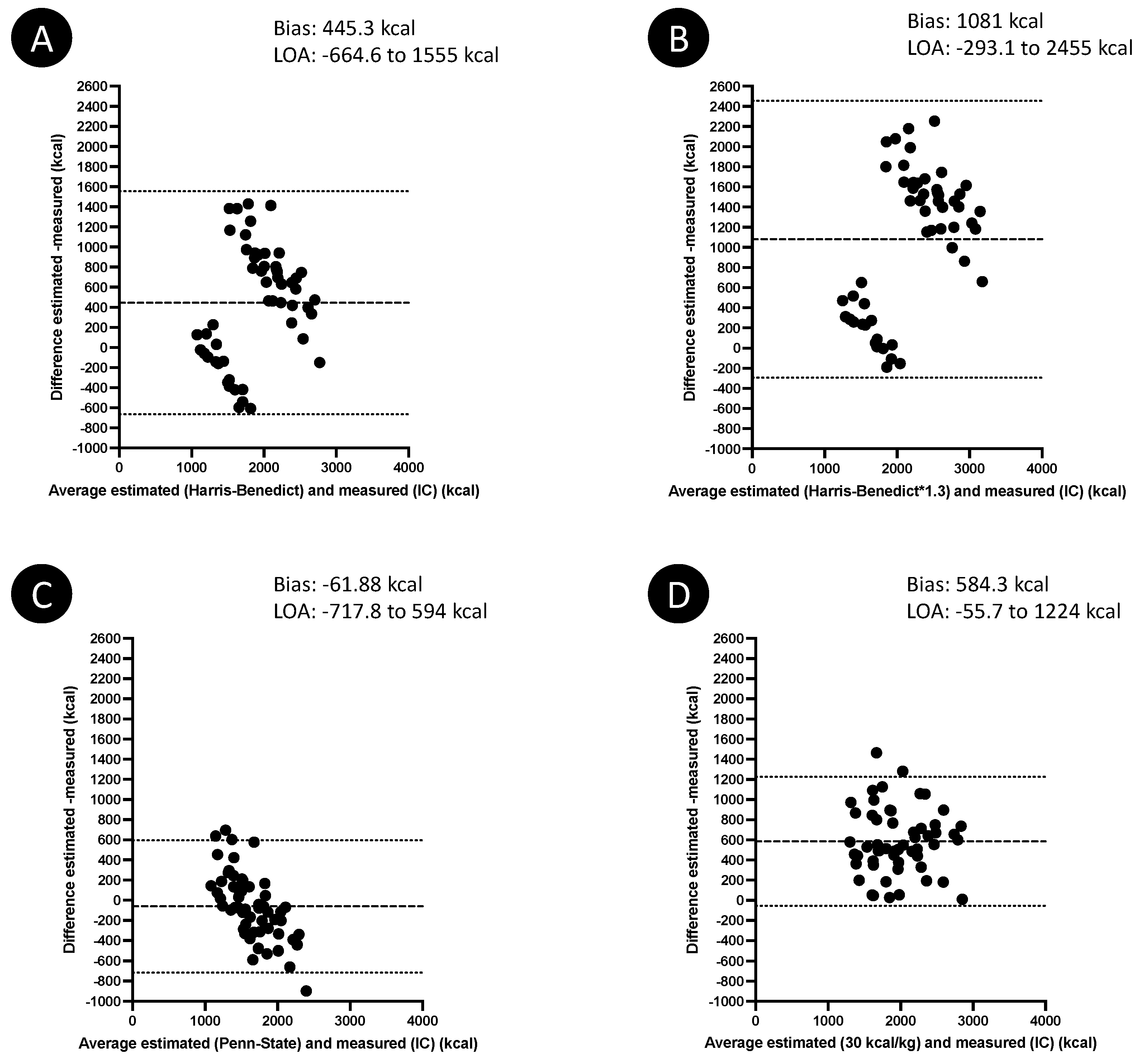
3.3. Estimated Energy Expenditure
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Preiser, J.C.; van Zanten, A.R.; Berger, M.M.; Biolo, G.; Casaer, M.P.; Doig, G.S.; Griffiths, R.D.; Heyland, D.K.; Hiesmayr, M.; Iapichino, G.; et al. Metabolic and nutritional support of critically ill patients: Consensus and controversies. Crit. Care 2015, 19, 35. [Google Scholar] [CrossRef] [PubMed]
- Rougier, L.; Preiser, J.C.; Fadeur, M.; Verbrugge, A.M.; Paquot, N.; Ledoux, D.; Misset, B.; Rousseau, A.F. Nutrition During Critical Care: An Audit on Actual Energy and Protein Intakes. J. Parenter. Enter. Nutr. 2020, 45, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Ridley, E.J.; Chapple, L.S.; Chapman, M.J. Nutrition intake in the post-ICU hospitalization period. Curr. Opin. Clin. Nutr. Metab. Care 2020, 23, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Moisey, L.L.; Pikul, J.; Keller, H.; Yeung, C.Y.E.; Rahman, A.; Heyland, D.K.; Mourtzakis, M. Adequacy of Protein and Energy Intake in Critically Ill Adults Following Liberation From Mechanical Ventilation Is Dependent on Route of Nutrition Delivery. Nutr. Clin. Pract. 2021, 36, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Peterson, S.J.; Tsai, A.A.; Scala, C.M.; Sowa, D.C.; Sheean, P.M.; Braunschweig, C.L. Adequacy of oral intake in critically ill patients 1 week after extubation. J. Am. Diet. Assoc. 2010, 110, 427–433. [Google Scholar] [CrossRef]
- Merriweather, J.; Smith, P.; Walsh, T. Nutritional rehabilitation after ICU—Does it happen: A qualitative interview and observational study. J. Clin. Nurs. 2014, 23, 654–662. [Google Scholar] [CrossRef]
- Prado, C.M.; Landi, F.; Chew, S.T.; Atherton, P.J.; Molinger, J.; Ruck, T.; Gonzalez, M.C. Advances in muscle health and nutrition: A toolkit for healthcare professionals. Clin. Nutr. 2022; in press. [Google Scholar] [CrossRef]
- Rousseau, A.F.; Prescott, H.C.; Brett, S.J.; Weiss, B.; Azoulay, E.; Creteur, J.; Latronico, N.; Hough, C.L.; Weber-Carstens, S.; Vincent, J.L.; et al. Long-term outcomes after critical illness: Recent insights. Crit Care 2021, 25, 108. [Google Scholar] [CrossRef]
- Van Zanten, A.R.H.; De Waele, E.; Wischmeyer, P.E. Nutrition therapy and critical illness: Practical guidance for the ICU, post-ICU, and long-term convalescence phases. Crit. Care 2019, 23, 368. [Google Scholar] [CrossRef]
- Ridley, E.J.; Parke, R.L.; Davies, A.R.; Bailey, M.; Hodgson, C.; Deane, A.M.; McGuinness, S.; Cooper, D.J. What Happens to Nutrition Intake in the Post-Intensive Care Unit Hospitalization Period? An Observational Cohort Study in Critically Ill Adults. J. Parenter. Enter. Nutr. 2019, 43, 88–95. [Google Scholar] [CrossRef]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef] [PubMed]
- Wischmeyer, P.E.; Molinger, J.; Haines, K. Point-Counterpoint: Indirect Calorimetry Is Essential for Optimal Nutrition Therapy in the Intensive Care Unit. Nutr. Clin. Pract. 2021, 36, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Oshima, T.; Delsoglio, M.; Dupertuis, Y.M.; Singer, P.; De Waele, E.; Veraar, C.; Heidegger, C.P.; Wernermann, J.; Wischmeyer, P.E.; Berger, M.M.; et al. The clinical evaluation of the new indirect calorimeter developed by the ICALIC project. Clin. Nutr. 2020, 39, 3105–3111. [Google Scholar] [CrossRef] [PubMed]
- Oshima, T.; Berger, M.M.; De Waele, E.; Guttormsen, A.B.; Heidegger, C.P.; Hiesmayr, M.; Singer, P.; Wernerman, J.; Pichard, C. Indirect calorimetry in nutritional therapy. A position paper by the ICALIC study group. Clin. Nutr. 2017, 36, 651–662. [Google Scholar] [CrossRef]
- Delsoglio, M.; Dupertuis, Y.M.; Oshima, T.; van der Plas, M.; Pichard, C. Evaluation of the accuracy and precision of a new generation indirect calorimeter in canopy dilution mode. Clin. Nutr. 2020, 39, 1927–1934. [Google Scholar] [CrossRef]
- Gandotra, S.; Files, D.C.; Shields, K.L.; Berry, M.; Bakhru, R.N. Activity Levels in Survivors of the Intensive Care Unit. Phys. Ther. 2021, 101, pzab135. [Google Scholar] [CrossRef]
- Fraipont, V.; Preiser, J.C. Energy estimation and measurement in critically ill patients. J. Parenter. Enter. Nutr. 2013, 37, 705–713. [Google Scholar] [CrossRef]
- Frankenfield, D.C.; Ashcraft, C.M. Toward the Development of Predictive Equations for Resting Metabolic Rate in Acutely Ill Spontaneously Breathing Patients. J. Parenter. Enter. Nutr. 2017, 41, 1155–1161. [Google Scholar] [CrossRef]
- Uehara, M.; Plank, L.D.; Hill, G.L. Components of energy expenditure in patients with severe sepsis and major trauma: A basis for clinical care. Crit. Care Med. 1999, 27, 1295–1302. [Google Scholar] [CrossRef]
- Whittle, J.; Molinger, J.; MacLeod, D.; Haines, K.; Wischmeyer, P.E.; Group, L.-C.S. Persistent hypermetabolism and longitudinal energy expenditure in critically ill patients with COVID-19. Crit. Care 2020, 24, 581. [Google Scholar] [CrossRef]
- Zusman, O.; Kagan, I.; Bendavid, I.; Theilla, M.; Cohen, J.; Singer, P. Predictive equations versus measured energy expenditure by indirect calorimetry: A retrospective validation. Clin. Nutr. 2019, 38, 1206–1210. [Google Scholar] [CrossRef] [PubMed]
- Vasileiou, G.; Qian, S.; Iyengar, R.; Mulder, M.B.; Gass, L.M.; Parks, J.; Pust, G.D.; Rattan, R.; Lineen, E.; Byers, P.; et al. Use of Predictive Equations for Energy Prescription Results in Inaccurate Estimation in Trauma Patients. Nutr. Clin. Pract. 2020, 35, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Smetana, K.S.; Hannawi, Y.; May, C.C. Indirect Calorimetry Measurements Compared With Guideline Weight-Based Energy Calculations in Critically Ill Stroke Patients. J. Parenter. Enter. Nutr. 2021, 45, 1484–1490. [Google Scholar] [CrossRef] [PubMed]
- Israfilov, E.; Kir, S. Comparison of Energy Expenditure in Mechanically Ventilated Septic Shock Patients in Acute and Recovery Periods via Indirect Calorimetry. J. Parenter. Enter. Nutr. 2021, 45, 1523–1531. [Google Scholar] [CrossRef]
- De Waele, E.; Honore, P.M.; Spapen, H.D. New generation indirect calorimeters for measuring energy expenditure in the critically ill: A rampant or reticent revolution? Crit. Care 2016, 20, 138. [Google Scholar] [CrossRef] [PubMed][Green Version]
- De Waele, E.; Jonckheer, J.; Wischmeyer, P.E. Indirect calorimetry in critical illness: A new standard of care? Curr. Opin. Crit. Care 2021, 27, 334–343. [Google Scholar] [CrossRef]
- Gonzalez-Granda, A.; Seethaler, B.; Haap, M.; Riessen, R.; Bischoff, S.C. Effect of an intensified individual nutrition therapy on serum metabolites in critically ill patients—A targeted metabolomics analysis of the ONCA study. Clin. Nutr. ESPEN 2021, 43, 267–275. [Google Scholar] [CrossRef]
- Fetterplace, K.; Beach, L.J.; MacIsaac, C.; Presneill, J.; Edbrooke, L.; Parry, S.M.; Rechnitzer, T.; Curtis, R.; Berney, S.; Deane, A.M.; et al. Associations between nutritional energy delivery, bioimpedance spectroscopy and functional outcomes in survivors of critical illness. J. Hum. Nutr. Diet. 2019, 32, 702–712. [Google Scholar] [CrossRef]
- Duan, J.Y.; Zheng, W.H.; Zhou, H.; Xu, Y.; Huang, H.B. Energy delivery guided by indirect calorimetry in critically ill patients: A systematic review and meta-analysis. Crit. Care 2021, 25, 88. [Google Scholar] [CrossRef]
- Davies, T.W.; van Gassel, R.J.J.; van de Poll, M.; Gunst, J.; Casaer, M.P.; Christopher, K.B.; Preiser, J.C.; Hill, A.; Gundogan, K.; Reintam-Blaser, A.; et al. Core outcome measures for clinical effectiveness trials of nutritional and metabolic interventions in critical illness: An international modified Delphi consensus study evaluation (CONCISE). Crit. Care 2022, 26, 240. [Google Scholar] [CrossRef]
- Achamrah, N.; Delsoglio, M.; De Waele, E.; Berger, M.M.; Pichard, C. Indirect calorimetry: The 6 main issues. Clin. Nutr. 2021, 40, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Frankenfield, D.C.; Ashcraft, C.M. Estimating energy needs in nutrition support patients. J. Parenter. Enter. Nutr. 2011, 35, 563–570. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Equations | Estimated Resting Energy Expenditure |
|---|---|
| Harris–Benedict (HB), kcal/day | Men: (13.75 × W) + (5 × H) − (6.8 × age) + 66 Women: (9.6 × W) + (1.8 × H) − (4.7 × age) + 655 |
| Penn–State (PS), kcal/day | Mifflin: Men: (10 × W) + (6.25 × H) − (5 × age) + 5 Women: (10 × W) + (6.25 × H) − (5 × age) − 161 Penn-State: PS = (Mifflin × 0.94) + (36.6 × 186) − 6597 |
| Post-ICU, kcal/kg/day | 30 |
| Data | Cohort n = 55 | Men n = 37 (67.3%) | Women n = 18 (32.7%) | |
|---|---|---|---|---|
| Age, y | 60 (52–67) | 58 (52–67.5) | 64 (50.5–67.8) | |
| Comorbidities, n (%) | Cardiovascular a | 38 (69.1) | 26 (70.3) | 12 (66.7) |
| Respiratory b | 15 (27.3) | 12 (32.4) | 3 (16.7) | |
| Digestive c | 26 (47.3) | 19 (51.4) | 7 (22.2) | |
| Metabolic and endocrine d | 20 (36.4) | 13 (35.1) | 7 (22.2) | |
| Chronic kidney disease | 28 (50.9) | 22 (59.5) | 6 (33.3) | |
| Oncologic | 6 (11) | 3 ((8.1) | 3 (16.7) | |
| Chronic alcoholism | 17 (30.9) | 15 (40.5) | 2 (11.1) | |
| SAPS II | 40 (25.7–54.5) | 46 (24.7–64.3) | 34 (24.5–45) | |
| Admission reason, n (%) | Medical | 30 (54.5) | 17 (45.9) | 13 (72.2) |
| Surgical | 25 (45.5) | 20 (54.1) | 5 (27.8) | |
| Admission failure, n (%) | Cardiovascular | 21 (38.2) | 16 (43.2) | 5 (27.8) |
| Pulmonary | 10 (18.2) | 8 (21.6) | 2 (11) | |
| Neurologic | 12 (21.8) | 3 (8.2) | 9 (50) | |
| Digestive | 5 (9) | 4 (10.8) | 1 (5.6) | |
| Trauma | 3 (5.5) | 2 (5.4) | 1 (5.6) | |
| Other | 4 (7.3) | 4 (10.8) | 0 | |
| Mechanical ventilation, n (%) | 39 (70.9) | 28 (75.7) | 11 (61.1) | |
| Duration of mechanical ventilation, days | 6 (2–10) | 5 (2–9) | 7 (2–15) | |
| Renal replacement therapy (RRT), n (%) | 2 (3.6) | 1 (2.7) | 1 (5.6) | |
| RRT duration, days | 6 and 9 | 9 | 6 | |
| Insulin, n (%) | 35 (63.6) | 25 (67.6) | 10 (55.6) | |
| Insulin duration, days | 6 (2–11) | 6 (1.5–11.5) | 6 (3.2–8.5) | |
| Nutrition route, n (%) | PO | 17 (30.9) | 13 (35.2) | 4 (22.2) |
| PO + EN | 6 (11) | 4 (10.8) | 2 (11) | |
| EN | 24 (43.6) | 14 (37.8) | 10 (55.6) | |
| EN + PN | 5 (9) | 4 (10.8) | 1 (5.6) | |
| PN | 3 (5.5) | 2 (5.4) | 1 (5.6) | |
| ICU LOS, days | 12 (7–16) | 12 (7–16) | 11.5 (7–17) | |
| Hospital LOS, days | 25 (17–41) | 22 (17–32.2) | 34 (20–58) | |
| Data | Cohort n = 55 | Men n = 37 (67.3%) | Women n = 18 (32.7%) | p Value | |
|---|---|---|---|---|---|
| Actual weight, kg | 77 (63–94) | 83.7 (64–96.8) | 71 (58.2–81.7) | 0.048 | |
| Actual weight considered for nutritional calculation, kg | 74 (63–88) | 80 (64–92.3) | 70.8 (58.2–76.1) | 0.011 | |
| BMI, kg/m2 | 26.1 (22.2–29.7) | 26 (21.7–29.6) | 26.6 (22.8–29.9) | 0.528 | |
| Nutrition route, n (%) | PO | 31 (56.4) | 22 (59.4) | 9 (50) | |
| PO + EN | 7 (12.7) | 3 (8.2) | 4 (22.2) | ||
| EN | 15 (27.3) | 10 (27) | 5 (27.8) | ||
| PN | 1 (1.8) | 1 (2.7) | 0 | ||
| PO + PN | 1 (1.8) | 1 (2.7) | 0 | ||
| VO2, mL/min | 243.5 (188.5–281) | 257 (202–302.5) | 217 (170.5–257) | 0.091 | |
| VCO2, mL/min | 189.5 (155.3–238) | 196.5 (157.8–245.8) | 180 (135.8–202.3) | 0.158 | |
| RQ | 0.83 (0.76–0.88) | 0.83 (0.77–0.89) | 0.80 (0.72–0.88) | 0.374 | |
| Measured EE, kcal/day | 1682 (1328–1975) | 1762 (1415–2123) | 1478 (1199–1836) | 0.093 | |
| Measured EE, kcal.kg/day | 22.9 (19.1–24.2) | 22.6 918.6–24.4) | 23.1 (20.9–24.4) | 0.756 | |
| Predicted EE, kcal/day | Harris–Benedict | 2344 (1389–2563) | 2500 (2335–2690) | 1344 (1242–1394) | <0.001 |
| Harris–Benedict corrected with a stress factor of 1.3 | 3048 (1805–3332) | 3250 (3036–3496) | 1747 (1614–1813) | <0.001 | |
| Penn–State | 1589 (1443–1809) | 1704 (1529–1888) | 1385 (1285–1457) | <0.001 | |
| 30 kcal/kg | 2220 (1890–2640) | 2400 (1920–2769) | 2124 (1748–2283) | 0.011 | |
| Blood Analysis | Reference Ranges | n = 55 |
|---|---|---|
| C-reactive protein (CRP), mg/L | 0–5 | 29.1 (11.4–60.8) |
| Total protein, g/L | 58–83 | 60 (55–69.5) |
| Albumin, g/L | ≤60 years: 35–52 >60 years: 32–46 | 32 (29.7–36) |
| Prealbumin, g/L | 0.2–0.4 | 0.21 (0.18–0.27) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rousseau, A.-F.; Fadeur, M.; Colson, C.; Misset, B. Measured Energy Expenditure Using Indirect Calorimetry in Post-Intensive Care Unit Hospitalized Survivors: A Comparison with Predictive Equations. Nutrients 2022, 14, 3981. https://doi.org/10.3390/nu14193981
Rousseau A-F, Fadeur M, Colson C, Misset B. Measured Energy Expenditure Using Indirect Calorimetry in Post-Intensive Care Unit Hospitalized Survivors: A Comparison with Predictive Equations. Nutrients. 2022; 14(19):3981. https://doi.org/10.3390/nu14193981
Chicago/Turabian StyleRousseau, Anne-Françoise, Marjorie Fadeur, Camille Colson, and Benoit Misset. 2022. "Measured Energy Expenditure Using Indirect Calorimetry in Post-Intensive Care Unit Hospitalized Survivors: A Comparison with Predictive Equations" Nutrients 14, no. 19: 3981. https://doi.org/10.3390/nu14193981
APA StyleRousseau, A.-F., Fadeur, M., Colson, C., & Misset, B. (2022). Measured Energy Expenditure Using Indirect Calorimetry in Post-Intensive Care Unit Hospitalized Survivors: A Comparison with Predictive Equations. Nutrients, 14(19), 3981. https://doi.org/10.3390/nu14193981