Abstract
As non-high-density lipoprotein cholesterol (non-HDL-C) levels account for all atherogenic lipoproteins, serum non-HDL-C level has been suggested to be a marker for cardiovascular (CV) risk stratification. Therefore, to unveil the association of serum non-HDL-C levels with CV outcomes in patients with non-dialysis chronic kidney disease (ND-CKD), the patients at stages 1 to 5 (n = 2152) from the Korean Cohort Study for Outcomes in Patients with Chronic Kidney Disease (KNOW-CKD) were prospectively analyzed. The subjects were divided into quintiles by serum non-HDL-C level. The primary outcome was a composite of all-cause death or non-fatal CV events. The median duration of follow-up was 6.940 years. The analysis using the Cox proportional hazard model unveiled that the composite CV event was significantly increased in the 5th quintile (adjusted hazard ratio 2.162, 95% confidence interval 1.174 to 3.981), compared to that of the 3rd quintile. A fully adjusted cubic spline model depicted a non-linear, J-shaped association between non-HDL-C and the risk of a composite CV event. The association remained robust in a series of sensitivity analyses, including the analysis of a cause-specific hazard model. Subgroup analyses reveled that the association is not significantly altered by clinical conditions, including age, gender, body mass index, estimated glomerular filtration rate, and albuminuria. In conclusion, high serum non-HDL-C level increased the risk of adverse CV outcomes among the patients with ND-CKD. Further studies are warranted to define the optimal target range of non-HDL-C levels in this population.
1. Introduction
Deaths in chronic kidney disease (CKD) most frequently results from cardiovascular (CV) disease [1,2], while the CV risk factors, including diabetes mellitus (DM), hypertension (HTN), and dyslipidemia, are prevalent in patients with CKD [3]. As even mild impairment in the kidney function increases the risk of an adverse CV event [4], CKD is also one of the nontraditional risk factors for CV disease [5,6]. Hence, the management of CV risk factors is an issue of clinical importance for better outcomes in patients with CKD.
A decrease in high-density lipoprotein cholesterol (HDL-C) levels, along with the elevation of serum triglycerides (TG) levels, is a characteristic feature of dyslipidemia in CKD [7,8,9]. HDL-C is known to provide cardioprotection, as it is involved in reverse cholesterol transport, where excess cholesterol in peripheral tissues is cleared [10,11]. Accordingly, an inverse association between HDL-C levels and the risk of adverse CV events has been proposed [12,13,14], although a large population-based study reported a non-linear, U-shaped association between HDL-C levels and all-cause mortality [15], suggesting that the role of HDL-C as a predictor of CV outcomes may depend on various clinical circumstances [16]. In this regard, mounting evidence indicates that the antioxidant and anti-inflammatory activity of HDL-C is impaired in patients with CKD [17,18]. Another study reported that, among patients with CKD, inflammation status modifies the association of HDL-C level and the risk of adverse CV events [19]. These collectively suggest that the prediction of CV outcomes by the measurement of a single lipid parameter has only a limited value, especially in patients with CKD.
Serum non-HDL-C levels are calculated as a subtraction of HDL-C from total cholesterol [20]. As non-HDL-C accounts for all atherogenic lipoproteins, such as intermediate-density lipoprotein, lipoprotein(a), low-density lipoprotein cholesterol (LDL-C), and very LDL remnants [21], serum non-HDL-C level has been suggested to be a marker for CV risk stratification. Indeed, it has been reported that high serum non-HDL-C level is associated with an increased risk of incident CV disease in the general population and that non-HDL-C may better predict CV outcomes than conventional lipid parameters do [22,23,24,25]. However, the association between non-HDL-C and adverse CV events in patients with CKD has not yet been fully evaluated.
Therefore, we hypothesized that high serum non-HDL-C levels may predict the risk of adverse CV outcomes in patient with CKD. In the present study, we aimed to investigate the association of serum non-HDL-C levels and CV outcomes among patients with non-dialysis CKD (ND-CKD).
2. Materials and Methods
2.1. Study Design
The study design of the Korean Cohort Study for Outcomes in Patients With Chronic Kidney Disease (KNOW-CKD) has been previously described (NCT01630486 at http://www.clinicaltrials.gov, accessed on 5 June 2019) [26]. Briefly, the patients with CKD at stages 1 to 5 (non-dialysis) were enrolled between 2011 and 2016. All the participants were closely monitored until 31 March 2021. Each participating center reported the study outcome events, which were cross-checked by the participating investigators. The median duration of follow-up was 6.940 years. Among those who were longitudinally followed up (n = 2238), after excluding those lacking the baseline measurement of total cholesterol or HDL-C in serum or those lacking the data on follow-up duration, only 2152 participants were ultimately analyzed (Figure 1). The current study followed the principles of the Declaration of Helsinki and was approved the institutional review board at each participating center (Seoul National University Hospital (1104–089-359), Seoul National University Bundang Hospital (B-1106/129–008), Yonsei University Severance Hospital (4–2011-0163), Kangbuk Samsung Medical Center (2011–01-076), Seoul St. Mary’s Hospital (KC11OIMI0441), Gil Hospital (GIRBA2553), Eulji General Hospital (201105–01), Chonnam National University Hospital (CNUH-2011-092), and Busan Paik Hospital (11–091)).
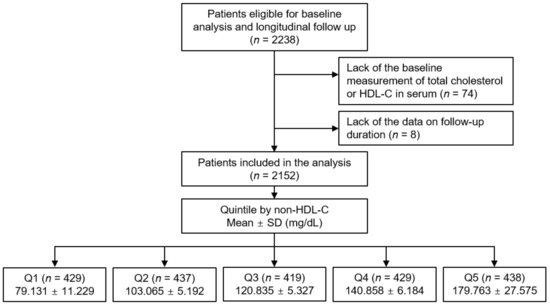
Figure 1.
Schematic diagram of study design. Abbreviations: Non-HDL-C, non-high-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; SD, standard deviation; Q1, 1st quintile; Q2, 2nd quintile, Q3, 3rd quintile; Q4, 4th quintile; Q5, 5th quintile.
2.2. Data Collection from Participants
All eligible participants presented demographic information, which included age, sex, medications (statins, angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers (angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin receptor blockers (ARBs)), diuretic use and the number of anti-HTN drugs), Charlson comorbid index, smoking history, and primary renal disease [27]. Anthropometric measures, such as height, weight, body mass index (BMI), and systolic and diastolic blood pressures (SBP and DBP), were obtained as previously described [28]. Following overnight fasting, hemoglobin, fasting glucose, albumin, HDL-C, LDL-C, TG, total cholesterol, creatinine (Cr), 25-hydroxyvitamin D (25(OH) vitamin D), and high-sensitivity C-reactive protein (hs-CRP) levels at the baseline were determined from venous samples. Serum non-HDL-C level was defined as the subtraction of HDL-C from total cholesterol. Chronic Kidney Disease Epidemiology Collaboration equation was used to calculate the estimated glomerular filtration rate (eGFR) [29]. The classification of CKD stages followed the Kidney Disease Improving Global Outcomes guidelines [30]. Spot urine albumin-to-Cr ratio (ACR) was measured at random, preferably from second-voided urine samples. Echocardiographic data were collected from complete two-dimensional M-mode and Doppler studies following standard approaches at the participating hospitals, where the cardiologists were blinded to the clinical data. M-mode examination followed a previous guideline [31]. The echocardiographic data, such as left atrial diameter, left ventricular (LV) end diastolic diameter, the ratio of the early transmitral blood flow velocity to early diastolic velocity of the mitral annulus, valve calcification, inter-ventricular septum thickness, left ventricular (LV) ejection fraction (LVEF), regional wall motion abnormality, LV posterior wall thickness, and LV end systolic diameter were recorded [32]. The Devereux formula was used to determine LV mass [31]. LV mass index (LVMI) was determined by normalizing LV mass to height2 (g/m2).
2.3. Exposure and Study Outcome
The exposure of primary interest was categorized serum non-HDL-C level, where the subjects were divided into the quintile (Q1, Q2, Q3, Q4, and Q5) by serum non-HDL-C level (Figure 1). The primary outcome was composite CV event, defined as a composite of all-cause death or non-fatal CV events. Secondary outcomes included the individual outcomes of all CV events (both fatal and non-fatal), 6-point MACE, and all-cause death. The CV events included any non-fatal coronary artery events (unstable angina, myocardial infarction, or coronary revascularization or surgery), hospitalization for heart failure, cerebrovascular events (ischemic or hemorrhagic stroke, or carotid intervention), or symptomatic arrhythmia [33]. The 6-point MACE was the composite of nonfatal myocardial infarction, unstable angina, revascularization, nonfatal stroke, heart failure, symptomatic arrhythmia, or cardiac death [34]. Survival time was defined as the period between study enrollment and outcome event.
2.4. Statistics
The Kolmogorov–Smirnov test was used to test the normality of distribution. The baseline characteristics by serum non-HDL-C level were compared by one-way analysis of variance and χ2 test for continuous and categorical variates, respectively. The cumulative incidences of study outcomes were estimated by Kaplan–Meier curve analyses with log-rank test. The participants with any missing data were excluded for further analyses. Cox proportional hazard regression models were utilized to evaluate the association between serum non-HDL-C level and study outcomes, where the participants lost to follow-up were censored at the date of the last visit. Models were constructed after adjusting for the following variables. Model 1 represents crude hazard ratios (HRs). Model 2 was adjusted for age and gender. Model 3 was further adjusted for medication (statins, ACEIs/ARBs, number of anti-HTN drugs and diuretics), current smoking status, Charlson comorbidity index, primary renal disease, BMI, and SBP and DBP. Model 4 was additionally adjusted for hemoglobin, fasting glucose, albumin, hs-CRP, LDL-C, triglycerides (TG), 25(OH) vitamin D, eGFR, spot urine ACR, LVMI, and LVEF. The analysis results of Cox proportional hazard models were presented as HRs and 95% confidence intervals (CIs). The association between serum non-HDL-C levels (as a continuous variable) and HRs for study outcomes was visualized by restricted cubic splines. Our findings were validated by a series of sensitivity analyses conducted as follows. First, the subjects with CKD stage 1 were excluded, because the subjects with CKD stage 1 have nearly normal kidney function and may not be clearly affected by the burden of disease. Second, the subjects with CKD stage 5 were excluded, because the subjects with CKD stage 5 are relatively small in number, and, at the same time, the association between serum TG level and study outcomes may be exaggerated due the advanced CKD. Third, we assessed cause-specific HRs for the primary study outcome through the serum non-HDL-C level, where non-cardiac death or kidney failure with replacement therapy before the occurrence of the primary outcome were censored at the time of death and the initiation of renal replacement therapy, respectively [34]. We also conducted subgroup analyses to test whether the association of serum non-HDL-C level with study outcomes was significantly altered by clinical conditions. Subgroups were pre-specified by gender (male versus (vs.) female), age (<60 vs. ≥60 years), BMI (<23 vs. ≥23 kg/m2), eGFR (<45 vs. ≥45 mL/min/1.73 m2), and spot urine ACR (<300 vs. ≥300 mg/g) [33]. The cut-off for statistical significance was a two-sided p value < 0.05. Statistical analysis was performed using SPSS for Windows version 22.0 (IBM Corp., Armonk, NY, USA) and R (version 4.1.1; R project for Statistical Computing, Vienna, Austria).
3. Results
3.1. Baseline Characteristics
To describe the baseline characteristics (Table 1), the study participants were di-vided into the quintile by serum non-HDL-C level (Table 1). The mean age of the participants was higher in the subjects in Q1 than those in the Q2, Q3, Q4, and Q5. The proportion of male participants was highest in Q1. The proportion of the participants with Charlson comorbidity index 0–3 was lowest in Q1, whereas those with Charlson comorbidity index 6–7 were also most frequently observed in Q1. The history of DM was most frequent in Q1, whereas the prevalence of glomerulonephritis and PKD was highest in Q3 and Q4, respectively. The use of diuretics was most prevalent in Q5. Hemoglobin and albumin levels were lowest in Q1 and Q5, respectively. Total cholesterol, LDL-C, and TG levels were lowest in Q1, while HDL-C levels were lowest in Q5. Fasting glucose levels were highest in Q5. 25(OH) vitamin D level was significantly lower in Q5. Spot urine ACR and serum creatinine levels were significantly higher in Q5 and Q1, respectively. Accordingly, eGFR was significantly lower in Q1, while the frequency of advanced CKD was relatively higher in Q1. The echocardiographic findings of study participants by serum non-HDL-C levels did not show significant difference across the groups, except in terms of valve calcification, interventricular wall thickness, and left ventricular end-diastolic diameter (Supplementary Materials Table S1). To summarize, unfavorable clinical features were predominantly observed in Q1 and Q5.

Table 1.
Baseline characteristics of study participants by non-HDL-C level.
3.2. Association of Serum Non-HDL-C Level with Adverse CV Events
To determine the cumulative incidences of the primary and secondary outcomes, Kaplan–Meier curves were analyzed. The risk of a composite CV event (p < 0.001, by Log-rank test) was significantly differed by serum non-HDL-C level, with the lowest risk of the events in Q3 (Figure 2). The risks of all CV events (p = 0.003, by Log-rank test, Supplementary Materials Figure S1), 6-point MACE (p < 0.001, by Log-rank test, Supplementary Materials Figure S2), all-cause death (p = 0.015, by Log-rank test, Supplementary Materials Figure S3) were also significantly differed by serum non-HDL-C level, with the lowest risk of the events in Q3. To unveil the independent association of serum non-HDL-C level with study outcomes, Cox proportional hazard models were used. The composite CV event significantly increased in Q5 (adjusted HR 2.162, 95% CI 1.174 to 3.981), compared to that of Q3 (Table 2), suggesting that high serum non-HDL-C level increases the risk of adverse CV outcomes in patients with ND-CKD. The risks of all CV events (adjusted HR 3.350, 95% CI 1.533 to 7.321) and 6-point MACE (adjusted HR 4.298, 95% CI 1.597 to 11.569) were significantly higher in Q5, compared to that of Q3, although the risk of all-cause death was not significantly different across the groups (Table 3). Restricted cubic spline curves depicted a non-linear, J-shaped association between non-HDL-C and the risk of composite CV event (Figure 3). Similarly, restricted cubic spline curve analysis visualized the non-linear, U-shaped associations of serum non-HDL-C levels with the risk of fatal and non-fatal CV events (Supplementary Materials Figure S4), 6-point MACE (Supplementary Materials Figure S5), and all-cause death (Supplementary Materials Figure S6).
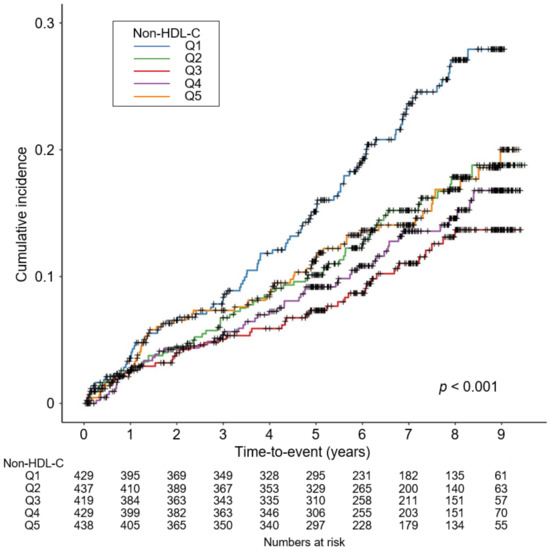
Figure 2.
Kaplan–Meier survival curve for cumulative incidence of composite CV event by non-HDL-C. p value by Log-rank test. Abbreviations: CV, cardiovascular; HDL-C, high density lipoprotein cholesterol; Q1, 1st quartile; Q2, 2nd quartile; Q3, 3rd quartile; Q4, 4th quartile; Q5, 5th quintile.
Table 2.
HRs for the primary outcome by non-HDL-C level.
Table 3.
HRs for the secondary outcomes by non-HDL-C level.
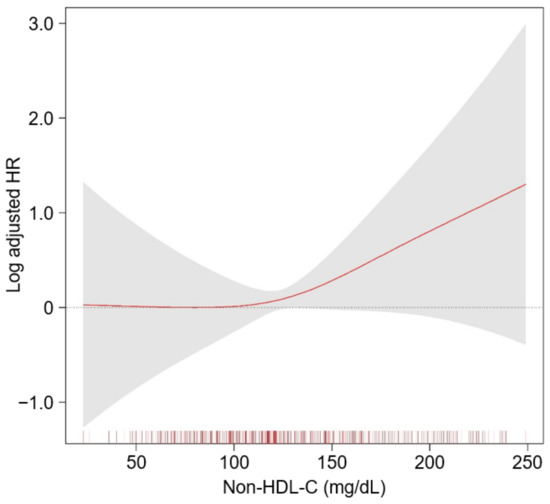
Figure 3.
Restricted cubic spline of non-HDL-C on a composite CV event. The adjusted HR of non-HDL-C as a continuous variable for composite CV event is depicted. The model was adjusted for age and sex, Charlson comorbidity index, primary renal disease, current smoking status, medication (ACEIs/ARBs, diuretics, number of anti-HTN drugs, statins), BMI, SBP, DBP, hemoglobin, albumin, LDL-C, TG, fasting glucose, 25(OH) vitamin D, hs-CRP, eGFR, spot urine ACR, LVMI, and LVEF. Abbreviations: CI, confidence interval; HDL-C, high-density lipoprotein cholesterol; HR, hazard ratio; ACEIs, angiotensin converting enzyme inhibitors; ARBs, angiotensin receptor blocker; HTN, hypertension; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; LDL-C, low density lipoprotein cholesterol; TG, triglyceride; hs-CRP, high-sensitivity C-reactive protein; eGFR, estimated glomerular filtration rate; ACR, albumin-to-creatinine ratio; LVMI, left ventricular mass index; LVEF, left ventricular ejection fraction.
3.3. Sensitivity Analyses
To examine the robustness of the findings, a series of sensitivity analyses were performed. After excluding the subjects with CKD stage 1, the risk of composite CV event was significantly higher in Q4 (adjusted HR 1.737, 95% CI 1.037 to 2.910) and Q5 (adjusted HR 2.355, 95% CI 1.244 to 4.458), compared to that of Q3 (Supplementary Materials Table S2). Next, after excluding the subjects with CKD stage 5, the risk of composite CV event was still significantly higher in Q4 (adjusted HR 1.708, 95% CI 1.020 to 2.860) and Q5 (adjusted HR 2.274, 95% CI 1.202 to 4.300), compared to that of Q3 (Supplementary Materials Table S3). Finally, we analyzed cause-specific hazard model for the primary study outcome by serum non-HDL-C level, where the risk of a composite CV event remained robustly higher in Q5 (adjusted HR 2.250, 95% CI 1.178 to 4.297), compared to that of Q3 (Table 4).
Table 4.
Cause-specific HRs for the primary outcome by non-HDL-C level.
3.4. Subgroup Analyses
To test whether the association between serum non-HDL-C level and the risk of a composite CV event is altered by certain clinical conditions, pre-specified subgroup analyses were conducted (Table 5), where the interactions between subgroups according to age, gender, BMI, eGFR, and albuminuria were tested. We could not find any significant interactions (all p values for interaction > 0.05), suggesting significant associations between serum non-HDL-C level with adverse CV outcomes across the aforementioned subgroups.
Table 5.
HRs for the primary outcome by non-HDL-C level in various subgroups.
4. Discussion
In the present study, we demonstrated that high serum non-HDL-C level is associated with adverse CV outcomes in patients with ND-CKD. A fully adjusted cubic spline model depicted a non-linear, J-shaped association between non-HDL-C and the risk of CV events. The association remained robust in a series of sensitivity analyses, including the analysis of a cause-specific hazard model. Subgroup analyses reveled that the association is not significantly altered by clinical conditions, including age, gender, BMI, eGFR, and albuminuria.
Recent studies have raised a question in the traditional concept of HDL-C as a “good cholesterol”. A cohort study of the patients with CKD stage 3 to 5 (non-dialysis) reported a U-shaped association of non-HDL-C both with all-cause and CV mortality [35]. Moreover, a more dramatic paradoxical association has been reported among the patients undergoing incident hemodialysis, where all-cause and CV mortality was inversely correlated with serum HDL-C level [36]. In this context, a cohort study analyzing 1864 Korean patients with ND-CKD reported meaningful data, where inflammation status modified the association trend between serum HDL-C level and the risk of adverse CV events: Serum HDL-C level was inversely associated with the risk of CV events in the absence of inflammation, whereas the risk of CV event positively correlated with serum HDL-C level in the presence of inflammation [19]. These collectively complicate the role of HDL-C in the CV risk stratification among the patients with CKD. In the current study, we found that among the patients with CKD high serum non-HDL-C level is associated with an increased risk of adverse CV events, although the association is non-linear, suggesting that non-HDL-C may be a marker for CV risk stratification in relation to dyslipidemia.
A major finding of the current study—the association between high serum non-HDL-C level and adverse CV outcomes—is readily expectable, based on the following rationale [35]: First, the non-HDL-C level accounts for all atherogenic lipoproteins, such as intermediate-density lipoprotein, lipoprotein(a), low-density lipoprotein cholesterol (LDL-C), and LDL remnants [21]. Second, the serum non-HDL-C level is positively correlated with apolipoprotein B level, a major protein on pro-atherogenic lipoproteins [37]. Third, as LDL-C particle size inversely correlates with the serum non-HDL-C level [38], a high serum level of non-HDL-C may indicate the relative abundance of small dense LDL-C particles, which is more atherogenic.
On the other hand, it is also of note that the risk of an adverse CV event increased, but not significantly, in the subjects with very low serum non-HDL-C levels (1st and 2nd quintiles). This could be attributed to either low total cholesterol or high HDL-C levels, because non-HDL-C level is calculated by subtracting HDL-C level from total cholesterol level. The studies reporting the association of low serum total cholesterol level with an increased risk of mortality indicating a higher prevalence of malnutrition and inflammation among the subjects with low serum total cholesterol level [39,40]. It is well-known that malnutrition leads to a worsening of inflammation, accelerating the progression of atherosclerosis [41,42,43]. In addition, a high serum HDL-C level with altered anti-inflammatory property may also explain the increased risk of CV events in the subjects with very low serum non-HDL-C levels. On top of the reports indicating a decrease in the anti-inflammatory activity of HDL-C in patients with CKD [18,44,45], some reported that HDL-C could be even pro-inflammatory under uremic conditions [46,47]. Collectively, these all indicate that very low serum non-HDL-C levels may not result in favorable CV outcomes in patients with CKD.
Although LDL-C is the primary target for the management of dyslipidemia in patients with CKD, the optimal therapeutic goal in regard to serum LDL-C levels has not been specified yet [48], as statin therapy targeting serum LDL-C level in patients with CKD failed to demonstrate benefits on CV or overall survival [49]. The current Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guidelines recommend a complete evaluation of the lipid profile, including total cholesterol and HDL-C, whereas the role of serum non-HDL-C level is not determined [48]. Provided that no specific goal of dyslipidemia management in patients with CKD is established, further studies are warranted in order to define the role of serum non-HDL-C as a marker for CV risk stratification and the optimal target range of non-HDL-C level in this population.
Usui et al. [50] previously reported that high serum non-HDL-C levels are associated with an increased risk of incident coronary heart disease, where only a small portion of the subjects with CKD (357 out of 2630 subjects in total) were included. Chiu et al. [35] also reported a U-shaped association between non-HDL-C level with the risk of all-cause death and CV mortality, which also enrolled a small number of the patients with CKD (n = 429) and did not analyze the incidence of non-fatal CV events. In the current study, we included a total of 2521 patients with CKD at the stages 1 to 5 (non-dialysis), to present definitive evidence for the association between serum non-HDL-C level and adverse CV outcomes. A relatively long follow-up duration of up to 10 years and rigorous adjustment of potential confounders, including echocardiographic parameters (i.e., LVMI and LVEF), are additional strengths of our study.
There are a number of limitations in the present study. First, due to the observational nature of the present study, we cannot confirm the casual relation between serum non-HDL-C level and the risk of adverse CV event in patients with CKD. However, it is not difficult to provide the rationale to support the major finding of the current study [21,35,37,38]. Second, all the variables were measured once at the baseline. However, the same limitation is shared with the previous observational study, which reports similar results that are largely concordant with ours. Therefore, we assume that the limitation does not significantly interfere with the overall impact of the current study. Third, as this cohort study enrolled only ethnic Koreans, a precaution is required to extrapolate the data to other populations. It should be also noted that, however, a similar result was reported by the studies conducted in Japan and Taiwan [35,50].
In conclusion, we report that high serum non-HDL-C level is associated with adverse CV outcomes in patients with ND-CKD, suggesting that non-HDL-C may be a useful marker for CV risk stratification. Further studies are warranted to define the optimal target range of non-HDL-C levels in this population.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/nu14183792/s1, Figure S1: Kaplan-Meier survival curve for cumulative incidence of fatal and non-fatal CV event by non-HDL-C; Figure S2: Kaplan–Meier survival curve for cumulative incidence of 6-point MACE by non-HDL-C; Figure S3: Kaplan–Meier survival curve for cumulative incidence of all-cause death by non-HDL-C; Figure S4: Restricted cubic spline of non-HDL-C on fatal and non-fatal CV event; Figure S5: Restricted cubic spline of non-HDL-C on 6-point MACE; Figure S6: Restricted cubic spline of non-HDL-C on all-cause death; Table S1. Summary of echocardiographic findings of study participants by non-HDL-C; Table S2: HRs for the primary outcome by non-HDL-C level after excluding the subjects at CKD stage 1; Table S3: HRs for the primary outcome by non-HDL-C level after excluding the subjects at CKD stage 5.
Author Contributions
Conceptualization, S.H.S.; methodology, S.H.S., T.R.O., H.S.C. and C.S.K.; formal analysis, S.H.S.; resources, E.H.B., K.-H.O. and S.H.H.; data curation, S.H.S.; writing—original draft preparation, S.H.S.; writing—review and editing, S.H.S., S.K.M. and S.W.K.; supervision, S.K.M. and S.W.K.; funding acquisition, S.H.S., K.-H.O. and S.W.K. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Research Program funded by the Korea Disease Control and Prevention Agency (2011E3300300, 2012E3301100, 2013E3301600, 2013E3301601, 2013E3301602, 2016E3300200, 2016E3300201, 2016E3300202, 2019E320100, 2019E320101, 2019E320102, and 2022-11-007), by the National Research Foundation of Korea (NRF) funded by the Korea government (MSIT) (NRF-2020R1F1A1074001 and NRF-2019R1A2C2086276), and by a grant (BCRI22042 and BCRI22079) from the Chonnam National University Hospital Biomedical Research Institute.
Institutional Review Board Statement
The study protocol was approved by the Institutional Review Board at each participating clinical center (Seoul National University Hospital (1104–089-359, 25 May 2011), Seoul Navtional University Bundang Hospital (B-1106/129–008, 24 August 2011), Yonsei University Severance Hospital (4–2011-0163, 2 June 2011), Kangbuk Samsung Medical Center (2011–01-076, 16 June 2012), Seoul St. Mary’s Hospital (KC11OIMI0441, 30 June 2011), Gil Hospital (GIRBA2553, 8 August 2011), Eulji General Hospital (201105–01, 10 June 2011), Chonnam National University Hospital (CNUH-2011-092, 5 July 2011), and Busan Paik Hospital (11–091, 26 July 2011)).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
KNOW-CKD: Study Group Clinical Centers. Seoul National University, Curie Ahn, Kook-Hwan Oh, Dong Wan Chae, Ho Jun Chin, Hayne Cho Park, Seungmi Lee, Hyun Hwa Jang, and Hyun Jin Cho. Yonsei University, Severance Hospital, Kyu Hun Choi, Seung Hyeok Han, Tae Hyun Yoo, and Mi Hyun Yu. Kangbuk Samsung Medical Center, Kyubeck Lee, and Sooyeon Jin. The Catholic University of Korea, Seoul St. Mary’s Hospital, Yong-Soo Kim, and Sol Ji Kim. Gachon University, Gil Hospital, Wookyung Chung, Youkyoung Jang and Ji Hye Park. Eulji University, Eulji General Hospital. Young-Hwan Hwang, Su-Ah Sung and Jeong Ok So. Chonnam University, Soo Wan Kim, MD and Ji Seon Lee. Inje University, Pusan Paik Hospital, Yeong Hoon Kim, Sun Woo Kang and Yun Jin Kim. Epidemiology and Biostatistics. Department of Preventive Medicine, Seoul National University College of Medicine, Byung-Joo Park, Sue Kyung Park and Juyeon Lee. Coordinating Center. Medical Research Collaborating Center, Seoul National University Hospital and Seoul National University College of Medicine, Joongyub Lee, Dayeon Nam, Soohee Kang and Heejung Ahn. Central Laboratory, Donghee Seo, Lab Genomics, Korea and Dae Yeon Cho, Lab Genomics, Korea. Biobank. Korea Biobank, Korea Centers for Disease Control and Prevention, Osong, Korea. Korea Center for Disease Control and Prevention, Dukhyoung Lee, Hyekyung Park (Project Officer), Eunkyeong Jung (Project Officer), Suyeon Jeong, Eunmi Ahn and Sil-Hea Sung.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jankowski, J.; Floege, J.; Fliser, D.; Böhm, M.; Marx, N. Cardiovascular Disease in Chronic Kidney Disease. Circulation 2021, 143, 1157–1172. [Google Scholar] [CrossRef] [PubMed]
- Vallianou, N.G.; Mitesh, S.; Gkogkou, A.; Geladari, E. Chronic Kidney Disease and Cardiovascular Disease: Is there Any Relationship? Curr. Cardiol. Rev. 2019, 15, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Gregg, L.P.; Hedayati, S.S. Management of Traditional Cardiovascular Risk Factors in CKD: What Are the Data? Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2018, 72, 728–744. [Google Scholar] [CrossRef] [PubMed]
- Thompson, S.; James, M.; Wiebe, N.; Hemmelgarn, B.; Manns, B.; Klarenbach, S.; Tonelli, M. Cause of Death in Patients with Reduced Kidney Function. J. Am. Soc. Nephrol. JASN 2015, 26, 2504–2511. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Briasoulis, A.; Bakris, G.L. Chronic kidney disease as a coronary artery disease risk equivalent. Curr. Cardiol. Rep. 2013, 15, 340. [Google Scholar] [CrossRef] [PubMed]
- Kwan, B.C.; Kronenberg, F.; Beddhu, S.; Cheung, A.K. Lipoprotein metabolism and lipid management in chronic kidney disease. J. Am. Soc. Nephrol. JASN 2007, 18, 1246–1261. [Google Scholar] [CrossRef]
- Ritz, E.; Wanner, C. Lipid abnormalities and cardiovascular risk in renal disease. J. Am. Soc. Nephrol. JASN 2008, 19, 1065–1070. [Google Scholar] [CrossRef]
- Kaysen, G.A. Lipid and lipoprotein metabolism in chronic kidney disease. J. Renal Nutr. Off. J. Council Renal Nutr. Natl. Kidney Found. 2009, 19, 73–77. [Google Scholar] [CrossRef]
- Nagao, M.; Nakajima, H.; Toh, R.; Hirata, K.I.; Ishida, T. Cardioprotective Effects of High-Density Lipoprotein Beyond its Anti-Atherogenic Action. J. Atheroscler. Thromb. 2018, 25, 985–993. [Google Scholar] [CrossRef] [Green Version]
- Ouimet, M.; Barrett, T.J.; Fisher, E.A. HDL and Reverse Cholesterol Transport. Circ. Res. 2019, 124, 1505–1518. [Google Scholar] [CrossRef]
- Lewington, S.; Whitlock, G.; Clarke, R.; Sherliker, P.; Emberson, J.; Halsey, J.; Qizilbash, N.; Peto, R.; Collins, R. Blood cholesterol and vascular mortality by age, sex, and blood pressure: A meta-analysis of individual data from 61 prospective studies with 55,000 vascular deaths. Lancet 2007, 370, 1829–1839. [Google Scholar] [CrossRef]
- Sun, L.; Clarke, R.; Bennett, D.; Guo, Y.; Walters, R.G.; Hill, M.; Parish, S.; Millwood, I.Y.; Bian, Z.; Chen, Y.; et al. Causal associations of blood lipids with risk of ischemic stroke and intracerebral hemorrhage in Chinese adults. Nat. Med. 2019, 25, 569–574. [Google Scholar] [CrossRef]
- Zhang, Y.; Tuomilehto, J.; Jousilahti, P.; Wang, Y.; Antikainen, R.; Hu, G. Total and high-density lipoprotein cholesterol and stroke risk. Stroke 2012, 43, 1768–1774. [Google Scholar] [CrossRef]
- Bowe, B.; Xie, Y.; Xian, H.; Balasubramanian, S.; Zayed, M.A.; Al-Aly, Z. High Density Lipoprotein Cholesterol and the Risk of All-Cause Mortality among U.S. Veterans. Clin. J. Am. Soc. Nephrol. CJASN 2016, 11, 1784–1793. [Google Scholar] [CrossRef]
- Wu, Z.; Huang, Z.; Lichtenstein, A.H.; Jin, C.; Chen, S.; Wu, S.; Gao, X. Different associations between HDL cholesterol and cardiovascular diseases in people with diabetes mellitus and people without diabetes mellitus: A prospective community-based study. Am. J. Clin. Nutr. 2021, 114, 907–913. [Google Scholar] [CrossRef]
- Vaziri, N.D. HDL abnormalities in nephrotic syndrome and chronic kidney disease. Nat. Rev. Nephrol. 2016, 12, 37–47. [Google Scholar] [CrossRef]
- Moradi, H.; Pahl, M.V.; Elahimehr, R.; Vaziri, N.D. Impaired antioxidant activity of high-density lipoprotein in chronic kidney disease. Transl. Res. J. Lab. Clin. Med. 2009, 153, 77–85. [Google Scholar] [CrossRef]
- Kim, J.Y.; Park, J.T.; Kim, H.W.; Chang, T.I.; Kang, E.W.; Ahn, C.; Oh, K.H.; Lee, J.; Chung, W.; Kim, Y.S.; et al. Inflammation Alters Relationship Between High-Density Lipoprotein Cholesterol and Cardiovascular Risk in Patients With Chronic Kidney Disease: Results From KNOW-CKD. J. Am. Heart Assoc. 2021, 10, e021731. [Google Scholar] [CrossRef]
- Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [CrossRef]
- Su, X.; Kong, Y.; Peng, D. Evidence for changing lipid management strategy to focus on non-high density lipoprotein cholesterol. Lipids Health Dis. 2019, 18, 134. [Google Scholar] [CrossRef] [PubMed]
- Wongcharoen, W.; Sutthiwutthichai, S.; Gunaparn, S.; Phrommintikul, A. Is non-HDL-cholesterol a better predictor of long-term outcome in patients after acute myocardial infarction compared to LDL-cholesterol?: A retrospective study. BMC Cardiovasc. Disord. 2017, 17, 10. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Sempos, C.; Donahue, R.P.; Dorn, J.; Trevisan, M.; Grundy, S.M. Joint distribution of non-HDL and LDL cholesterol and coronary heart disease risk prediction among individuals with and without diabetes. Diabetes Care 2005, 28, 1916–1921. [Google Scholar] [CrossRef] [PubMed]
- Di Angelantonio, E.; Gao, P.; Pennells, L.; Kaptoge, S.; Caslake, M.; Thompson, A.; Butterworth, A.S.; Sarwar, N.; Wormser, D.; Saleheen, D.; et al. Lipid-related markers and cardiovascular disease prediction. JAMA 2012, 307, 2499–2506. [Google Scholar] [CrossRef]
- Levinson, S.S. High density- and beta-lipoprotein screening for risk of coronary artery disease in the context of new findings on reverse cholesterol transport. Ann. Clin. Lab. Sci. 2002, 32, 123–136. [Google Scholar]
- Oh, K.H.; Park, S.K.; Park, H.C.; Chin, H.J.; Chae, D.W.; Choi, K.H.; Han, S.H.; Yoo, T.H.; Lee, K.; Kim, Y.S.; et al. KNOW-CKD (KoreaN cohort study for Outcome in patients With Chronic Kidney Disease): Design and methods. BMC Nephrol. 2014, 15, 80. [Google Scholar] [CrossRef]
- Suh, S.H.; Oh, T.R.; Choi, H.S.; Kim, C.S.; Bae, E.H.; Oh, K.H.; Lee, J.; Oh, Y.K.; Jung, J.Y.; Ma, S.K.; et al. Abdominal Aortic Calcification and Cardiovascular Outcomes in Chronic Kidney Disease: Findings from KNOW-CKD Study. J. Clin. Med. 2022, 11, 1157. [Google Scholar] [CrossRef]
- Suh, S.H.; Oh, T.R.; Choi, H.S.; Kim, C.S.; Bae, E.H.; Oh, K.H.; Lee, K.B.; Han, S.H.; Sung, S.; Ma, S.K.; et al. Association of Body Weight Variability With Progression of Coronary Artery Calcification in Patients With Predialysis Chronic Kidney Disease. Front. Cardiovasc. Med. 2021, 8, 794957. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Levey, A.S.; Eckardt, K.U.; Tsukamoto, Y.; Levin, A.; Coresh, J.; Rossert, J.; De Zeeuw, D.; Hostetter, T.H.; Lameire, N.; Eknoyan, G. Definition and classification of chronic kidney disease: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2005, 67, 2089–2100. [Google Scholar] [CrossRef]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for chamber quantification: A report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef]
- Suh, S.H.; Oh, T.R.; Choi, H.S.; Kim, C.S.; Bae, E.H.; Oh, K.H.; Lee, J.; Jung, J.Y.; Lee, K.B.; Ma, S.K.; et al. Association Between Left Ventricular Geometry and Renal Outcomes in Patients With Chronic Kidney Disease: Findings From Korean Cohort Study for Outcomes in Patients With Chronic Kidney Disease Study. Front. Cardiovasc. Med. 2022, 9, 848692. [Google Scholar] [CrossRef]
- Suh, S.H.; Oh, T.R.; Choi, H.S.; Kim, C.S.; Bae, E.H.; Oh, K.H.; Choi, K.H.; Oh, Y.K.; Ma, S.K.; Kim, S.W. Association of Left Ventricular Diastolic Dysfunction With Cardiovascular Outcomes in Patients With Pre-dialysis Chronic Kidney Disease: Findings From KNOW-CKD Study. Front. Cardiovasc. Med. 2022, 9, 844312. [Google Scholar] [CrossRef]
- Park, C.H.; Kim, H.W.; Joo, Y.S.; Park, J.T.; Chang, T.I.; Yoo, T.H.; Park, S.K.; Chae, D.W.; Chung, W.; Kim, Y.S.; et al. Association Between Systolic Blood Pressure Variability and Major Adverse Cardiovascular Events in Korean Patients With Chronic Kidney Disease: Findings From KNOW-CKD. J. Am. Heart Assoc. 2022, 11, e025513. [Google Scholar] [CrossRef]
- Chiu, H.; Wu, P.Y.; Huang, J.C.; Tu, H.P.; Lin, M.Y.; Chen, S.C.; Chang, J.M. There is a U shaped association between non high density lipoprotein cholesterol with overall and cardiovascular mortality in chronic kidney disease stage 3-5. Sci. Rep. 2020, 10, 12749. [Google Scholar] [CrossRef]
- Chang, T.I.; Streja, E.; Ko, G.J.; Naderi, N.; Rhee, C.M.; Kovesdy, C.P.; Kashyap, M.L.; Vaziri, N.D.; Kalantar-Zadeh, K.; Moradi, H. Inverse Association Between Serum Non-High-Density Lipoprotein Cholesterol Levels and Mortality in Patients Undergoing Incident Hemodialysis. J. Am. Heart Assoc. 2018, 7, 1–13. [Google Scholar] [CrossRef]
- Leroux, G.; Lemieux, I.; Lamarche, B.; Cantin, B.; Dagenais, G.R.; Lupien, P.J.; Després, J.P. Influence of triglyceride concentration on the relationship between lipoprotein cholesterol and apolipoprotein B and A-I levels. Metab. Clin. Exp. 2000, 49, 53–61. [Google Scholar] [CrossRef]
- El Harchaoui, K.; van der Steeg, W.A.; Stroes, E.S.; Kuivenhoven, J.A.; Otvos, J.D.; Wareham, N.J.; Hutten, B.A.; Kastelein, J.J.; Khaw, K.T.; Boekholdt, S.M. Value of low-density lipoprotein particle number and size as predictors of coronary artery disease in apparently healthy men and women: The EPIC-Norfolk Prospective Population Study. J. Am. Coll. Cardiol. 2007, 49, 547–553. [Google Scholar] [CrossRef]
- Liu, Y.; Coresh, J.; Eustace, J.A.; Longenecker, J.C.; Jaar, B.; Fink, N.E.; Tracy, R.P.; Powe, N.R.; Klag, M.J. Association between cholesterol level and mortality in dialysis patients: Role of inflammation and malnutrition. JAMA 2004, 291, 451–459. [Google Scholar] [CrossRef]
- Contreras, G.; Hu, B.; Astor, B.C.; Greene, T.; Erlinger, T.; Kusek, J.W.; Lipkowitz, M.; Lewis, J.A.; Randall, O.S.; Hebert, L.; et al. Malnutrition-inflammation modifies the relationship of cholesterol with cardiovascular disease. J. Am. Soc. Nephrol. JASN 2010, 21, 2131–2142. [Google Scholar] [CrossRef]
- Levin, N.W.; Handelman, G.J.; Coresh, J.; Port, F.K.; Kaysen, G.A. Reverse epidemiology: A confusing, confounding, and inaccurate term. Semin. Dial. 2007, 20, 586–592. [Google Scholar] [CrossRef]
- Chen, S.C.; Lin, T.H.; Hsu, P.C.; Chang, J.M.; Lee, C.S.; Tsai, W.C.; Su, H.M.; Voon, W.C.; Chen, H.C. Impaired left ventricular systolic function and increased brachial-ankle pulse-wave velocity are independently associated with rapid renal function progression. Hypertens. Res. Off. J. Jpn. Soc. Hypertens. 2011, 34, 1052–1058. [Google Scholar] [CrossRef]
- Chen, S.C.; Su, H.M.; Hung, C.C.; Chang, J.M.; Liu, W.C.; Tsai, J.C.; Lin, M.Y.; Hwang, S.J.; Chen, H.C. Echocardiographic parameters are independently associated with rate of renal function decline and progression to dialysis in patients with chronic kidney disease. Clin. J. Am. Soc. Nephrol. CJASN 2011, 6, 2750–2758. [Google Scholar] [CrossRef]
- Gluba-Brzozka, A.; Franczyk, B.; Rysz, J. Cholesterol Disturbances and the Role of Proper Nutrition in CKD Patients. Nutrients 2019, 11, 2820. [Google Scholar] [CrossRef]
- Vaziri, N.D.; Navab, M.; Fogelman, A.M. HDL metabolism and activity in chronic kidney disease. Nat. Rev. Nephrol. 2010, 6, 287–296. [Google Scholar] [CrossRef]
- Yamamoto, S.; Yancey, P.G.; Ikizler, T.A.; Jerome, W.G.; Kaseda, R.; Cox, B.; Bian, A.; Shintani, A.; Fogo, A.B.; Linton, M.F.; et al. Dysfunctional high-density lipoprotein in patients on chronic hemodialysis. J. Am. Coll. Cardiol. 2012, 60, 2372–2379. [Google Scholar] [CrossRef]
- Moradi, H.; Vaziri, N.D.; Kashyap, M.L.; Said, H.M.; Kalantar-Zadeh, K. Role of HDL dysfunction in end-stage renal disease: A double-edged sword. J. Renal Nutr. Off. J. Counc. Renal Nutr. Natl. Kidney Found. 2013, 23, 203–206. [Google Scholar] [CrossRef]
- Wanner, C.; Tonelli, M. KDIGO Clinical Practice Guideline for Lipid Management in CKD: Summary of recommendation statements and clinical approach to the patient. Kidney Int. 2014, 85, 1303–1309. [Google Scholar] [CrossRef]
- Baigent, C.; Landray, M.J.; Reith, C.; Emberson, J.; Wheeler, D.C.; Tomson, C.; Wanner, C.; Krane, V.; Cass, A.; Craig, J.; et al. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): A randomised placebo-controlled trial. Lancet 2011, 377, 2181–2192. [Google Scholar] [CrossRef]
- Usui, T.; Nagata, M.; Hata, J.; Mukai, N.; Hirakawa, Y.; Yoshida, D.; Kishimoto, H.; Kitazono, T.; Kiyohara, Y.; Ninomiya, T. Serum Non-High-Density Lipoprotein Cholesterol and Risk of Cardiovascular Disease in Community Dwellers with Chronic Kidney Disease: The Hisayama Study. J. Atheroscler. Thromb. 2017, 24, 706–715. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).