

Associations of Dietary Fats with All-Cause Mortality and Cardiovascular Disease Mortality among Patients with Cardiometabolic Disease


Abstract
:1. Introduction
2. Materials and Methods
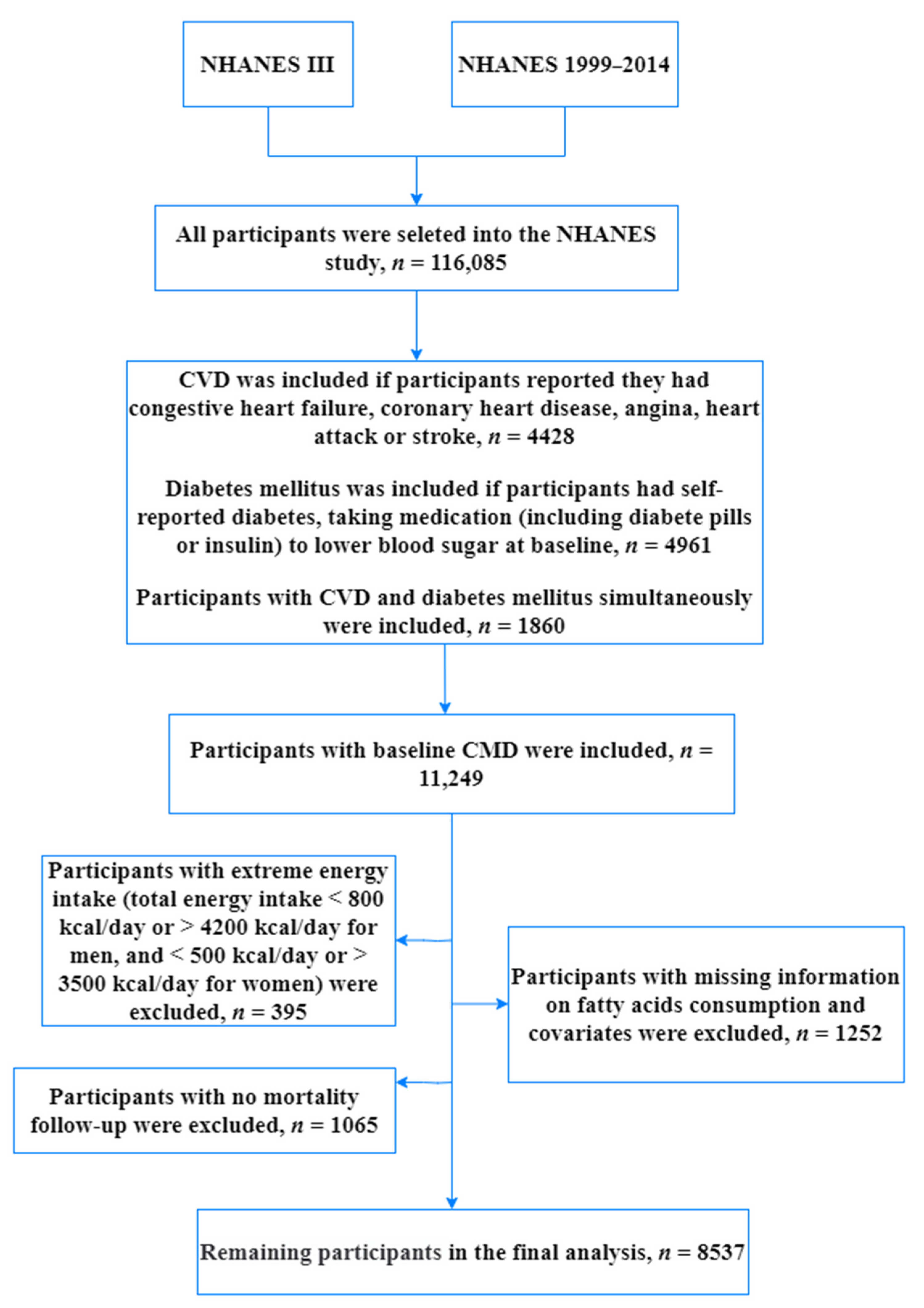
2.1. Study Population
2.2. Dietary Assessment and Other Covariates
2.3. Ascertainment of Death
2.4. Statistical Analyses
3. Results
3.1. Population Characteristics
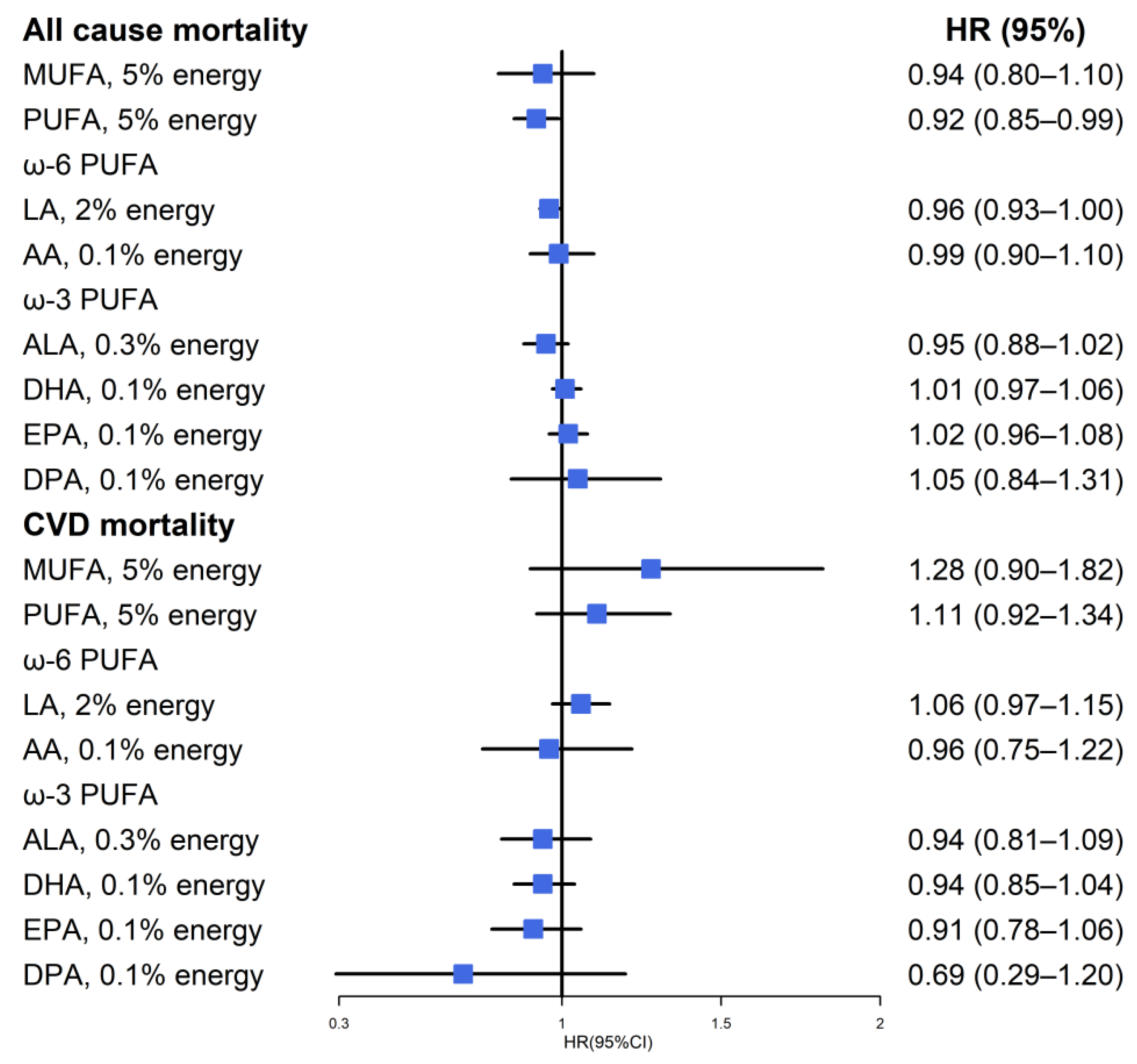
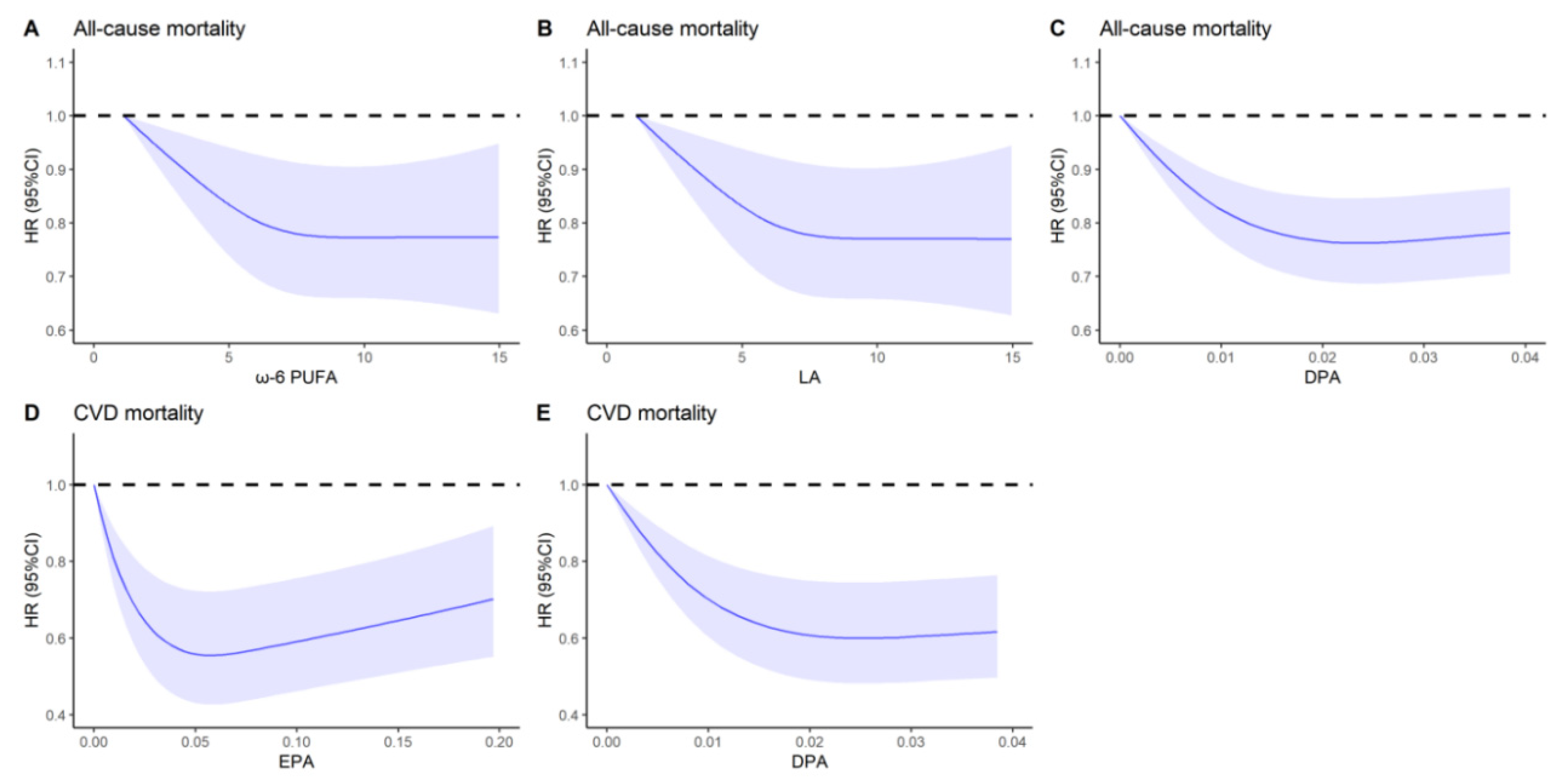
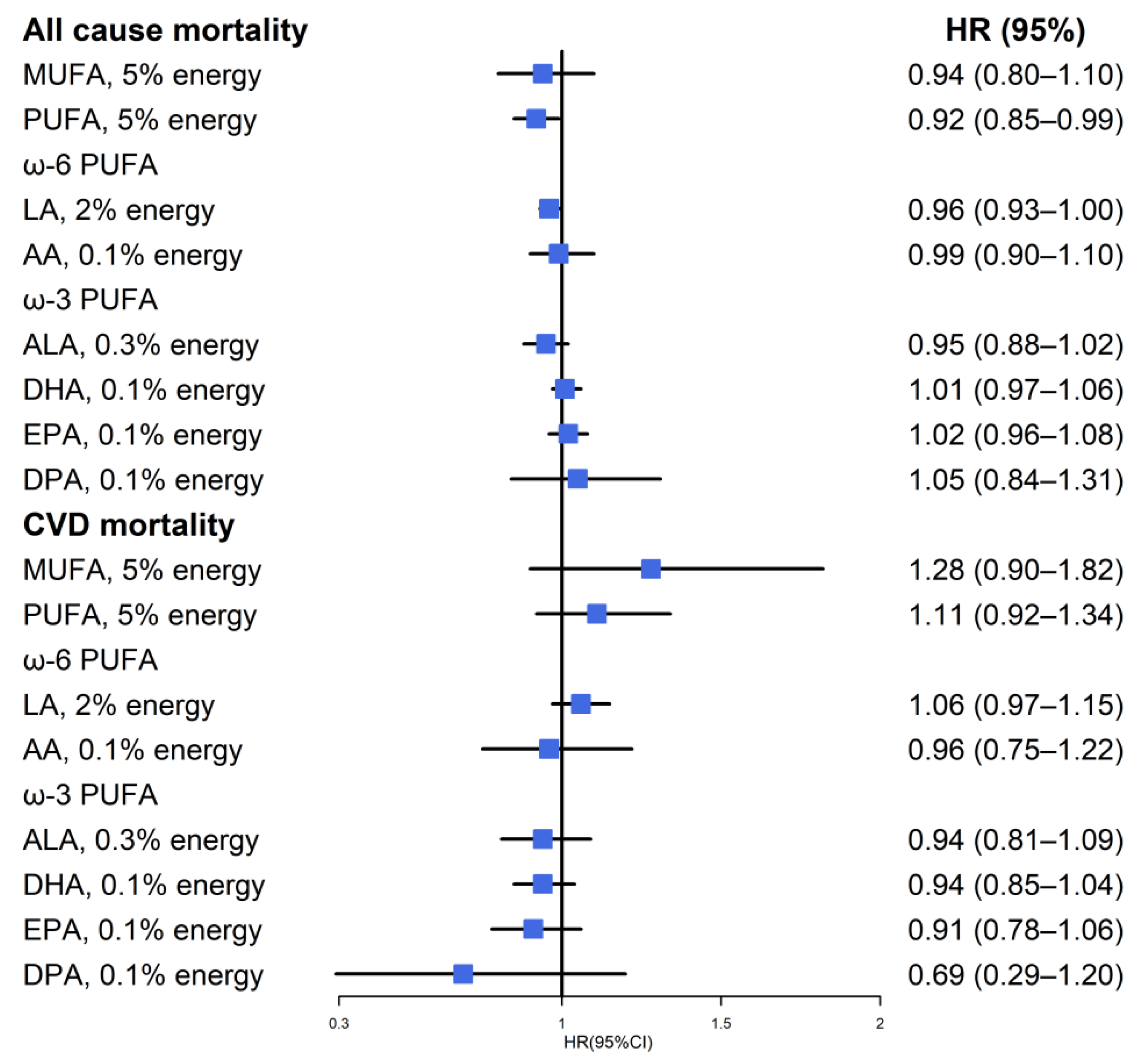
3.2. All-Cause Mortality
3.3. CVD Mortality
3.4. Sensitivity Analyses
4. Discussion
5. Conclusion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Third Report of the National Cholesterol Education Program (NCEP). Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Liberopoulos, E.N.; Mikhailidis, D.P.; Elisaf, M.S. Diagnosis and management of the metabolic syndrome in obesity. Obes. Rev. 2005, 6, 283–296. [Google Scholar] [CrossRef]
- Vasudevan, A.R.; Ballantyne, C.M. Cardiometabolic risk assessment: An approach to the prevention of cardiovascular disease and diabetes mellitus. Clin. Cornerstone 2005, 7, 7–16. [Google Scholar] [CrossRef]
- Guan, B.; Tong, J.; Hao, H.; Yang, Z.; Chen, K.; Xu, H.; Wang, A. Bile acid coordinates microbiota homeostasis and systemic immunometabolism in cardiometabolic diseases. Acta Pharm. Sin. B 2022, 12, 2129–2149. [Google Scholar] [CrossRef]
- Dove, A.; Marseglia, A.; Shang, Y.; Grande, G.; Vetrano, D.L.; Laukka, E.J.; Fratiglioni, L.; Xu, W. Cardiometabolic multimorbidity accelerates cognitive decline and dementia progression. Alzheimers Dement. 2022. [Google Scholar] [CrossRef]
- Jiang, Z.; Zhuo, L.B.; He, Y.; Fu, Y.; Shen, L.; Xu, F.; Gou, W.; Miao, Z.; Shuai, M.; Liang, Y.; et al. The gut microbiota-bile acid axis links the positive association between chronic insomnia and cardiometabolic diseases. Nat. Commun. 2022, 13, 3002. [Google Scholar] [CrossRef]
- Xu, C.; Zhang, P.; Cao, Z. Cardiovascular health and healthy longevity in people with and without cardiometabolic disease: A prospective cohort study. EClinicalMedicine 2022, 45, 101329. [Google Scholar] [CrossRef]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Noël, C.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- World Health Organization. Noncommunicable Diseases Country Profiles 2018; World Health Organization: Geneva, Switzerland, 2018; p. 10. [Google Scholar]
- Vinke, P.C.; Navis, G.; Kromhout, D.; Corpeleijn, E. Associations of Diet Quality and All-Cause Mortality Across Levels of Cardiometabolic Health and Disease: A 7.6-Year Prospective Analysis from the Dutch Lifelines Cohort. Diabetes Care 2021, 44, 1228–1235. [Google Scholar] [CrossRef]
- Wang, D.D.; Li, Y.; Chiuve, S.E.; Stampfer, M.J.; Manson, J.E.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Association of Specific Dietary Fats With Total and Cause-Specific Mortality. JAMA Intern. Med. 2016, 176, 1134–1145. [Google Scholar] [CrossRef]
- Beckman, J.A.; Paneni, F.; Cosentino, F.; Creager, M.A. Diabetes and vascular disease: Pathophysiology, clinical consequences, and medical therapy: Part II. Eur. Heart J. 2013, 34, 2444–2452. [Google Scholar] [CrossRef]
- Kim, Y.; Je, Y.; Giovannucci, E.L. Association between dietary fat intake and mortality from all-causes, cardiovascular disease, and cancer: A systematic review and meta-analysis of prospective cohort studies. Clin. Nutr. 2021, 40, 1060–1070. [Google Scholar] [CrossRef]
- Zhuang, P.; Zhang, Y.; He, W.; Chen, X.; Chen, J.; He, L.; Mao, L.; Wu, F.; Jiao, J. Dietary Fats in Relation to Total and Cause-Specific Mortality in a Prospective Cohort of 521 120 Individuals With 16 Years of Follow-Up. Circ. Res. 2019, 124, 757–768. [Google Scholar] [CrossRef]
- Mente, A.; Dehghan, M.; Rangarajan, S.; McQueen, M. Prospective Urban Rural Epidemiology (PURE) study investigators. Association of dietary nutrients with blood lipids and blood pressure in 18 countries: A cross-sectional analysis from the PURE study. Lancet Diabetes Endocrinol. 2017, 5, 774–787. [Google Scholar] [CrossRef]
- Jiao, J.; Liu, G.; Shin, H.J.; Hu, F.B.; Rimm, E.B.; Rexrode, K.M.; Manson, J.E.; Zong, G.; Sun, Q. Dietary fats and mortality among patients with type 2 diabetes: Analysis in two population based cohort studies. BMJ 2019, 366, l4009. [Google Scholar] [CrossRef]
- Colin-Ramirez, E.; Castillo-Martinez, L.; Orea-Tejeda, A.; Zheng, Y.; Westerhout, C.M.; Ezekowitz, J.A. Dietary fatty acids intake and mortality in patients with heart failure. Nutrition 2014, 30, 1366–1371. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC); National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention: Hyattsville, MD, USA, 2022.
- National Center for Health Statistics (NCHS). About the National Health and Nutrition Examination Survey; NCHS: Hyattsville, MD, USA, 2017.
- Matsushita, Y.; Takahashi, T.; Asahi, K.; Harashima, E.; Takahashi, H.; Tanaka, H.; Tsumuraya, Y.; Sarukura, N.; Furuta, M.; Tanaka, H.; et al. Validation of improved 24-h dietary recall using a portable camera among the Japanese population. Nutr. J. 2021, 20, 68. [Google Scholar] [CrossRef]
- Basiotis, P.P.; Welsh, S.O.; Cronin, F.J.; Kelsay, J.L.; Mertz, W. Number of days of food intake records required to estimate individual and group nutrient intakes with defined confidence. J. Nutr. 1987, 117, 1638–1641. [Google Scholar] [CrossRef]
- Ahluwalia, N.; Dwyer, J.; Terry, A.; Moshfegh, A.; Johnson, C. Update on NHANES Dietary Data: Focus on Collection, Release, Analytical Considerations, and Uses to Inform Public Policy. Adv. Nutr. 2016, 7, 121–134. [Google Scholar] [CrossRef] [Green Version]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef]
- National Center for Health Statistics (NCHS). 2015 Public-Use Linked Mortality Files; NCHS: Hyattsville, MD, USA, 2019.
- Menke, A.; Muntner, P.; Batuman, V.; Silbergeld, E.K.; Guallar, E. Blood lead below 0.48 micromol/L (10 microg/dL) and mortality among US adults. Circulation 2006, 114, 1388–1394. [Google Scholar] [CrossRef]
- Willett, W.C. Chapter 5: Food Frequency Methods; Chapter 6: Reproducibility and Validity of Food-Frequency Questionnaires; Chapter 11: Implications of Total Energy Intake for Epidemiologic Analyses. In Nutritional Epidemiology, 3rd ed.; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Maki, K.C.; Eren, F.; Cassens, M.E.; Dicklin, M.R.; Davidson, M.H. ω-6 Polyunsaturated Fatty Acids and Cardiometabolic Health: Current Evidence, Controversies, and Research Gaps. Adv. Nutr. 2018, 9, 688–700. [Google Scholar] [CrossRef]
- Nagai, T.; Honda, Y.; Sugano, Y.; Nishimura, K.; Nakai, M.; Honda, S.; Iwakami, N.; Okada, A.; Asaumi, Y.; Aiba, T.; et al. Circulating Omega-6, But Not Omega-3 Polyunsaturated Fatty Acids, are Associated with Clinical Outcomes in Patients with Acute Decompensated Heart Failure. PLoS ONE 2016, 11, e0165841. [Google Scholar] [CrossRef]
- Wu, J.H.Y.; Marklund, M.; Imamura, F.; Tintle, N.; Ardisson Korat, A.V.; de Goede, J.; Zhou, X.; Yang, W.S.; de Oliveira Otto, M.C.; Kröger, J.; et al. Cohorts for Heart and Aging Research in Genomic Epidemiology (CHARGE) Fatty Acids and Outcomes Research Consortium (FORCE). Omega-6 fatty acid biomarkers and incident type 2 diabetes: Pooled analysis of individual-level data for 39 740 adults from 20 prospective cohort studies. Lancet Diabetes Endocrinol. 2017, 5, 965–974. [Google Scholar] [CrossRef]
- Ramsden, C.E.; Zamora, D.; Leelarthaepin, B.; Majchrzak-Hong, S.F.; Faurot, K.R.; Suchindran, C.M.; Ringel, A.; Davis, J.M.; Hibbeln, J.R. Use of dietary linoleic acid for secondary prevention of coronary heart disease and death: Evaluation of recovered data from the Sydney Diet Heart Study and updated meta-analysis. BMJ 2013, 346, e8707. [Google Scholar] [CrossRef]
- Chowdhury, R.; Warnakula, S.; Kunutsor, S.; Crowe, F.; Ward, H.A.; Johnson, L.; Franco, O.H.; Butterworth, A.S.; Forouhi, N.G.; Thompson, S.G.; et al. Association of dietary, circulating, and supplement fatty acids with coronary risk: A systematic review and meta-analysis. Ann. Intern. Med. 2014, 160, 398–406. [Google Scholar] [CrossRef]
- Rimm, E.B.; Appel, L.J.; Chiuve, S.E.; Djoussé, L.; Engler, M.B.; Kris-Etherton, P.M.; Mozaffarian, D.; Siscovick, D.S.; Lichtenstein, A.H.; American Heart Association Nutrition Committee of the Council on Lifestyle and Cardiometabolic Health; et al. Seafood Long-Chain n-3 Polyunsaturated Fatty Acids and Cardiovascular Disease: A Science Advisory From the American Heart Association. Circulation 2018, 138, e35–e47. [Google Scholar] [CrossRef]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Albert, C.M.; Gordon, D.; Copeland, T.; et al. Marine n-3 Fatty Acids and Prevention of Cardiovascular Disease and Cancer. N. Engl. J. Med. 2019, 380, 23–32. [Google Scholar] [CrossRef]
- Hu, Y.; Hu, F.B.; Manson, J.E. Marine Omega-3 Supplementation and Cardiovascular Disease: An Updated Meta-Analysis of 13 Randomized Controlled Trials Involving 127 477 Participants. J. Am. Heart Assoc. 2019, 8, e013543. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Lemaitre, R.N.; King, I.B.; Song, X.; Huang, H.; Sacks, F.M.; Rimm, E.B.; Wang, M.; Siscovick, D.S. Plasma phospholipid long-chain ω-3 fatty acids and total and cause-specific mortality in older adults: A cohort study. Ann. Intern. Med. 2013, 158, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, M.; Origasa, H.; Matsuzaki, M.; Matsuzawa, Y.; Saito, Y.; Ishikawa, Y.; Oikawa, S.; Sasaki, J.; Hishida, H.; Itakura, H.; et al. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): A randomised open-label, blinded endpoint analysis. Lancet 2007, 369, 1090–1098. [Google Scholar] [CrossRef]
- Jiang, H.; Wang, L.; Wang, D.; Yan, N.; Li, C.; Wu, M.; Wang, F.; Mi, B.; Chen, F.; Jia, W.; et al. Omega-3 polyunsaturated fatty acid biomarkers and risk of type 2 diabetes, cardiovascular disease, cancer, and mortality. Clin. Nutr. 2022, 41, 1798–1807. [Google Scholar] [CrossRef] [PubMed]
- Innes, J.K.; Calder, P.C. The Differential Effects of Eicosapentaenoic Acid and Docosahexaenoic Acid on Cardiometabolic Risk Factors: A Systematic Review. Int. J. Mol. Sci. 2018, 19, 532. [Google Scholar] [CrossRef]
- Sherratt, S.C.R.; Mason, R.P. Eicosapentaenoic acid and docosahexaenoic acid have distinct membrane locations and lipid interactions as determined by X-ray diffraction. Chem. Phys. Lipids 2018, 212, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Mason, R.P.; Jacob, R.F.; Shrivastava, S.; Sherratt, S.C.R.; Chattopadhyay, A. Eicosapentaenoic acid reduces membrane fluidity, inhibits cholesterol domain formation, and normalizes bilayer width in atherosclerotic-like model membranes. Biochim. Biophys. Acta 2016, 1858, 3131–3140. [Google Scholar] [CrossRef]
- Nelson, J.R.; Wani, O.; May, H.T.; Budoff, M. Potential benefits of eicosapentaenoic acid on atherosclerotic plaques. Vasc. Pharmacol. 2017, 91, 1–9. [Google Scholar] [CrossRef]
- Watanabe, T.; Ando, K.; Daidoji, H.; Otaki, Y.; Sugawara, S.; Matsui, M.; Ikeno, E.; Hirono, O.; Miyawaki, H.; Yashiro, Y.; et al. A randomized controlled trial of eicosapentaenoic acid in patients with coronary heart disease on statins. J. Cardiol. 2017, 70, 537–544. [Google Scholar] [CrossRef]
- Del Gobbo, L.C.; Imamura, F.; Aslibekyan, S.; Marklund, M.; Virtanen, J.K.; Wennberg, M.; Yakoob, M.Y.; Chiuve, S.E.; dela Cruz, L.; Frazier-Wood, A.C.; et al. ω-3 Polyunsaturated Fatty Acid Biomarkers and Coronary Heart Disease: Pooling Project of 19 Cohort Studies. JAMA Intern. Med. 2016, 176, 1155–1166. [Google Scholar] [CrossRef]
- Drouin, G.; Rioux, V.; Legrand, P. The n-3 docosapentaenoic acid (DPA): A new player in the n-3 long chain polyunsaturated fatty acid family. Biochimie 2019, 159, 36–48. [Google Scholar] [CrossRef]
- Li, K.; Sinclair, A.J.; Zhao, F.; Li, D. Uncommon Fatty Acids and Cardiometabolic Health. Nutrients 2018, 10, 1559. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Katsuki, A.; Romanazzi, D.; Miller, M.R.; Adams, S.L.; Miyashita, K.; Hosokawa, M. Docosapentaenoic Acid (22:5n-3) Downregulates mRNA Expression of Pro-inflammatory Factors in LPS-activated Murine Macrophage Like RAW264.7 Cells. J. Oleo Sci. 2017, 66, 1149–1156. [Google Scholar] [CrossRef]
- Chen, J.; Jiang, Y.; Liang, Y.; Tian, X.; Peng, C.; Ma, K.Y.; Liu, J.; Huang, Y.; Chen, Z.Y. DPA n-3, DPA n-6 and DHA improve lipoprotein profiles and aortic function in hamsters fed a high cholesterol diet. Atherosclerosis 2012, 221, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, I.A.; Katan, M.B.; Zock, P.L. Dietary alpha-linolenic acid is associated with reduced risk of fatal coronary heart disease, but increased prostate cancer risk: A meta-analysis. J. Nutr. 2004, 134, 919–922. [Google Scholar] [CrossRef]
- Mozaffarian, D. Does alpha-linolenic acid intake reduce the risk of coronary heart disease? A review of the evidence. Altern. Ther. Health Med. 2005, 11, 24–30. [Google Scholar]
- Wang, C.; Harris, W.S.; Chung, M.; Lichtenstein, A.H.; Balk, E.M.; Kupelnick, B.; Jordan, H.S.; Lau, J. n-3 Fatty acids from fish or fish-oil supplements, but not alpha-linolenic acid, benefit cardiovascular disease outcomes in primary- and secondary-prevention studies: A systematic review. Am. J. Clin. Nutr. 2006, 84, 5–17. [Google Scholar] [CrossRef]
- Shen, T.; Xing, G.; Zhu, J.; Zhang, S.; Cai, Y.; Li, D.; Xu, G.; Xing, E.; Rao, J.; Shi, R. Effects of 12-week supplementation of marine Omega-3 PUFA-based formulation Omega3Q10 in older adults with prehypertension and/or elevated blood cholesterol. Lipids Health Dis. 2017, 16, 253. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.; Briskey, D.; Nalley, J.O.; Ganuza, E. Omega-3 Eicosapentaenoic Acid (EPA) Rich Extract from the Microalga Nannochloropsis Decreases Cholesterol in Healthy Individuals: A Double-Blind, Randomized, Placebo-Controlled, Three-Month Supplementation Study. Nutrients 2020, 12, 1869. [Google Scholar] [CrossRef]
- Xyda, S.E.; Vuckovic, I.; Petterson, X.M.; Dasari, S.; Lalia, A.Z.; Parvizi, M.; Macura, S.I.; Lanza, I.R. Distinct Influence of Omega-3 Fatty Acids on the Plasma Metabolome of Healthy Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 875–884. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Tertile of SFA Intake | Tertile of MUFA Intake | Tertile of PUFA Intake | ||||||
|---|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | T1 | T2 | T3 | T1 | T2 | T3 | |
| Participants (n) | 2840 | 2851 | 2846 | 2845 | 2846 | 2846 | 2845 | 2849 | 2843 |
| Fatty acid intake (% of energy) | 7.19 | 10.77 | 14.92 | 8.58 | 12.29 | 16.65 | 4.47 | 7.03 | 10.67 |
| Male (%) | 45.05 | 49.17 | 50.90 | 42.57 | 47.53 | 54.40 | 46.97 | 48.68 | 49.92 |
| Age (years) | 62.38 | 61.76 | 59.98 | 62.37 | 62.32 | 59.57 | 61.33 | 61.92 | 60.74 |
| Race (%) | |||||||||
| Non-Hispanic White | 63.76 | 72.69 | 76.75 | 67.45 | 69.70 | 76.18 | 70.40 | 70.79 | 72.96 |
| Non-Hispanic Black | 15.10 | 13.57 | 12.17 | 12.94 | 14.07 | 13.59 | 12.50 | 14.53 | 13.64 |
| Mexican American | 7.47 | 6.07 | 5.07 | 7.03 | 6.80 | 4.83 | 6.25 | 6.63 | 5.57 |
| Others | 13.68 | 7.67 | 6.014 | 12.58 | 9.43 | 5.40 | 10.85 | 8.05 | 7.83 |
| Education level (%) | |||||||||
| Less than high school | 35.41 | 31.66 | 31.63 | 35.73 | 31.32 | 31.57 | 37.07 | 33.97 | 27.53 |
| High school or equivalent | 26.76 | 28.87 | 27.64 | 25.74 | 28.36 | 29.00 | 26.07 | 29.30 | 28.05 |
| College or above | 37.83 | 39.47 | 40.73 | 38.53 | 40.32 | 39.43 | 36.87 | 36.73 | 44.42 |
| Family income-poverty ratio level (%) | |||||||||
| <1.3 | 30.39 | 22.58 | 23.58 | 31.00 | 25.81 | 20.16 | 29.05 | 25.13 | 21.87 |
| 1.3–2.4 | 30.44 | 33.37 | 30.89 | 31.03 | 32.11 | 31.59 | 31.36 | 33.72 | 29.82 |
| ≥2.4 | 39.17 | 44.05 | 45.53 | 37.96 | 42.08 | 48.25 | 39.59 | 41.15 | 48.31 |
| BMI group (%) | |||||||||
| <18.5 | 1.66 | 1.12 | 0.67 | 1.456 | 1.46 | 1.05 | 0.86 | 1.934 | 0.64 |
| 18.5–25 | 23.27 | 18.90 | 17.97 | 22.73 | 22.73 | 17.43 | 21.89 | 20.30 | 17.59 |
| 25–30 | 31.73 | 31.50 | 30.95 | 31.66 | 31.66 | 30.43 | 33.06 | 29.64 | 31.31 |
| ≥30 | 43.34 | 48.48 | 50.41 | 44.15 | 44.15 | 51.10 | 44.19 | 48.13 | 50.46 |
| Smoking status (%) | |||||||||
| Never smoker | 45.50 | 42.48 | 39.61 | 46.10 | 43.91 | 37.93 | 42.11 | 42.54 | 42.50 |
| Former smoker | 38.10 | 37.84 | 37.75 | 36.53 | 36.61 | 40.10 | 37.20 | 37.06 | 39.31 |
| Current smoker | 16.40 | 19.68 | 22.64 | 17.37 | 19.48 | 21.97 | 20.69 | 20.40 | 18.19 |
| Alcohol drinking (%) | |||||||||
| Non-drinker | 80.17 | 79.48 | 82.00 | 78.58 | 80.74 | 82.18 | 79.78 | 78.94 | 82.93 |
| Low to moderate drinker | 10.95 | 12.69 | 12.86 | 11.59 | 12.45 | 12.55 | 11.18 | 14.58 | 11.06 |
| Heavy drinker | 8.88 | 7.83 | 5.14 | 9.83 | 6.81 | 5.27 | 9.04 | 6.48 | 6.01 |
| Physical activity (%) | |||||||||
| Inactive | 39.78 | 39.41 | 42.20 | 40.12 | 40.95 | 40.51 | 38.11 | 39.92 | 43.47 |
| Insufficiently active | 33.05 | 33.41 | 34.27 | 33.02 | 32.32 | 35.19 | 34.98 | 34.19 | 31.72 |
| Active | 27.18 | 27.19 | 23.53 | 26.86 | 26.73 | 24.30 | 26.91 | 25.89 | 24.81 |
| Self-reported health status (%) | |||||||||
| Poor to fair | 44.29 | 43.29 | 42.37 | 45.99 | 43.08 | 41.12 | 46.88 | 41.22 | 41.58 |
| Good | 35.79 | 33.62 | 38.49 | 31.30 | 37.21 | 39.06 | 32.23 | 37.91 | 38.08 |
| Very good/excellent | 19.91 | 23.09 | 19.14 | 22.71 | 19.71 | 19.82 | 20.89 | 20.87 | 20.34 |
| Self-reported chronic diseases (%) | |||||||||
| Hypertension | 61.53 | 66.05 | 39.03 | 61.18 | 64.13 | 63.13 | 59.66 | 64.65 | 64.29 |
| Hyperlipemia | 69.14 | 70.11 | 67.37 | 68.70 | 71.07 | 67.04 | 64.75 | 69.98 | 71.80 |
| Cancer | 17.70 | 19.02 | 17.34 | 17.41 | 19.49 | 17.27 | 16.26 | 19.98 | 17.92 |
| Total energy intake (kcal/day) | 1624.05 | 1840.65 | 1938.68 | 1601.17 | 1820.33 | 1975.98 | 1694.55 | 1798.49 | 1932.44 |
| Protein intake (% of energy) | 16.79 | 16.42 | 16.75 | 16.90 | 16.51 | 16.56 | 17.20 | 16.81 | 15.97 |
| Carbohydrate intake (% of energy) | 56.61 | 49.02 | 42.50 | 57.53 | 49.50 | 41.40 | 53.43 | 49.03 | 44.64 |
| Tertiles of Percentage Energy from Specific Fatty Acids | ||||
|---|---|---|---|---|
| Tertile 1 | Tertile 2 | Tertile 3 | p Trend b | |
| SFA | ||||
| Mean, % of energy | 7.19 ± 0.05 | 10.77 ± 0.03 | 14.92 ± 0.08 | |
| No. of deaths/person years | 1180/287,779 | 1147/269,766 | 1179/287,119 | |
| Model 1 c | 1 (ref.) | 0.92 (0.81–1.06) | 0.99 (0.90–1.09) | 0.83 |
| Model 2 d | 1 (ref.) | 0.94 (0.81–1.09) | 0.99 (0.84–1.15) | 0.94 |
| MUFA | ||||
| Mean, % of energy | 8.58 ± 0.05 | 12.29 ± 0.02 | 16.65 ± 0.11 | |
| No. of deaths/person years | 1208/279,237 | 1099/260,626 | 1199/304,801 | |
| Model 1 c | 1 (ref.) | 0.99 (0.88–1.13) | 0.99 (0.88–1.12) | 0.93 |
| Model 2 d | 1 (ref.) | 1.09 (0.93–1.26) | 1.08 (0.86–1.35) | 0.56 |
| PUFA | ||||
| Mean, % of energy | 4.49 ± 0.03 | 7.03 ± 0.02 | 10.67 ± 0.07 | |
| No. of deaths/person years | 1406/306,092 | 1106/269,233 | 984/269,339 | |
| Model 1 c | 1 (ref.) | 0.96 (0.84–1.08) | 0.90 (0.80–1.03) | 0.07 |
| Model 2 d | 1 (ref.) | 0.94 (0.82–1.06) | 0.88 (0.76–1.02) | 0.06 |
| ω-6 PUFA | ||||
| Mean, % of energy | 3.92 ± 0.03 | 6.26 ± 0.02 | 9.58 ± 0.07 | |
| No. of deaths/person years | 1413/302,958 | 1091/270,768 | 1002/270,938 | |
| Model 1 c | 1 (ref.) | 0.90 (0.79–1.03) | 0.86 (0.74–0.99) | 0.07 |
| Model 2 d | 1 (ref.) | 0.86 (0.74–1.01) | 0.85 (0.73–0.99) | 0.03 |
| LA | ||||
| Mean, % of energy | 3.86 ± 0.03 | 6.17 ± 0.02 | 9.49 ± 0.07 | |
| No. of deaths/person years | 1409/303,023 | 1101/270,272 | 996/271,369 | |
| Model 1 c | 1 (ref.) | 0.92 (0.80–1.05) | 0.89 (0.78–1.01) | 0.06 |
| Model 2 d | 1 (ref.) | 0.92 (0.80–1.05) | 0.86 (0.75–1.00) | 0.05 |
| AA | ||||
| Mean, % of energy | 0.02 ± 0.0004 | 0.06 ± 0.0003 | 0.13 ± 0.0001 | |
| No. of deaths/person years | 1250/287,909 | 1078/274,846 | 1178/281,909 | |
| Model 1 c | 1 (ref.) | 0.94 (0.83–1.06) | 0.98 (0.86–1.12) | 0.80 |
| Model 2 d | 1 (ref.) | 0.96 (0.85–1.09) | 1.05 (0.89–1.23) | 0.51 |
| ω-3 PUFA | ||||
| Mean, % of energy | 0.41 ± 0.003 | 0.65 ± 0.001 | 1.12 ± 0.012 | |
| No. of deaths/person years | 1430/321,955 | 1145/271,423 | 931/251,286 | |
| Model 1 c | 1(ref.) | 1.04(0.93–1.15) | 0.91(0.79–1.03) | 0.12 |
| Model 2 d | 1(ref.) | 1.04(0.93–1.17) | 0.90(0.89–1.04) | 0.15 |
| ALA | ||||
| Mean, % of energy | 0.37 ± 0.003 | 0.59 ± 0.001 | 1.00 ± 0.010 | |
| No. of deaths/person years | 1422/320,237 | 1143/276,767 | 941/247,660 | |
| Model 1 c | 1 (ref.) | 1.04 (0.92–1.18) | 0.94 (0.81–1.09) | 0.36 |
| Model 2 d | 1 (ref.) | 1.02 (0.89–1.17) | 0.93 (0.80–1.09) | 0.36 |
| Marine ω-3 PUFA | ||||
| Mean, % of energy | 0.002 ± 0.0001 | 0.022 ± 0.0003 | 0.19 ± 0.008 | |
| No. of deaths/person years | 1638/342,543 | 829/227,727 | 1039/274,394 | |
| Model 1 c | 1 (ref.) | 0.92 (0.80–1.06) | 0.92 (0.80–1.06) | 0.29 |
| Model 2 d | 1 (ref.) | 0.91 (0.78–1.07) | 0.97 (0.84–1.12) | 0.83 |
| DHA | ||||
| Mean, % of energy | 0.0005 ± 0.00003 | 0.01 ± 0.0001 | 0.11 ± 0.004 | |
| No. of deaths/person years | 1549/326,118 | 872/233,996 | 1053/284,550 | |
| Model 1 c | 1 (ref.) | 0.92 (0.80–1.05) | 0.93 (0.81–1.07) | 0.34 |
| Model 2 d | 1 (ref.) | 0.92 (0.79–1.06) | 0.99 (0.86–1.14) | 0.98 |
| EPA | ||||
| Mean, % of energy | 0.00003 ± 0.000003 | 0.003 ± 0.00005 | 0.06 ± 0.003 | |
| No. of deaths/person years | 1848/385,458 | 771/208,040 | 887/251,166 | |
| Model 1 c | 1 (ref.) | 0.99 (0.84–1.16) | 0.92 (0.80–1.06) | 0.19 |
| Model 2 d | 1 (ref.) | 0.95 (0.79–1.13) | 0.93 (0.80–1.07) | 0.36 |
| DPA | ||||
| Mean, % of energy | 0 ± 0 | 0.004 ± 0.00007 | 0.03 ± 0.0010 | |
| No. of deaths/person years | 2024/418,989 | 714/195,684 | 768/229,991 | |
| Model 1 c | 1 (ref.) | 0.84 (0.72–0.96) | 0.85 (0.74–0.98) | 0.02 |
| Model 2 d | 1 (ref.) | 0.80 (0.69–0.93) | 0.86 (0.75–0.98) | 0.03 |
| Tertiles of Percentage Energy from Specific Fatty Acids | ||||
|---|---|---|---|---|
| Tertile 1 | Tertile 2 | Tertile 3 | p-Trend b | |
| SFA | ||||
| Mean, % of energy | 7.19 ± 0.05 | 10.77 ± 0.03 | 14.92 ± 0.08 | |
| No. of deaths/person years | 292/287,779 | 290/269,766 | 300/287,119 | |
| Model 1 c | 1 (ref.) | 0.76 (0.55–1.05) | 0.85 (0.64–1.11) | 0.25 |
| Model 2 d | 1 (ref.) | 0.84 (0.60–1.19) | 0.93 (0.65–1.34) | 0.65 |
| MUFA | ||||
| Mean, % of energy | 8.58 ± 0.05 | 12.29 ± 0.02 | 16.6 5 ± 0.11 | |
| No. of deaths/person years | 316/279,237 | 260/260,626 | 306/304,801 | |
| Model 1 c | 1 (ref.) | 0.86 (0.69–1.09) | 0.94 (0.75–1.18) | 0.50 |
| Model 2 d | 1 (ref.) | 0.99 (0.78–1.27) | 1.18 (0.85–1.65) | 0.27 |
| PUFA | ||||
| Mean, % of energy | 4.49 ± 0.03 | 7.03 ± 0.02 | 10.67 ± 0.07 | |
| No. of deaths/person years | 363/306,092 | 287/269,233 | 232/269,339 | |
| Model 1 c | 1 (ref.) | 1.20 (0.94–1.54) | 0.91 (0.70–1.19) | 0.32 |
| Model 2 d | 1 (ref.) | 1.20 (0.95–1.52) | 0.92 (0.67–1.25) | 0.51 |
| ω-6 PUFA | ||||
| Mean, % of energy | 3.92 ± 0.03 | 6.26 ± 0.02 | 9.58 ± 0.07 | |
| No. of deaths/person years | 361/302,958 | 286/270,768 | 235/270,938 | |
| Model 1 c | 1 (ref.) | 1.12 (0.86–1.46) | 0.91 (0.69–1.21) | 0.23 |
| Model 2 d | 1 (ref.) | 1.13 (0.87–1.47) | 0.91 (0.65–1.26) | 0.48 |
| LA | ||||
| Mean, % of energy | 3.86 ± 0.03 | 6.17 ± 0.02 | 9.49 ± 0.07 | |
| No. of deaths/person years | 363/303,023 | 286/270,272 | 233/271,369 | |
| Model 1 c | 1 (ref.) | 1.07 (0.83–1.37) | 0.92 (0.69–1.24) | 0.58 |
| Model 2 d | 1 (ref.) | 1.09 (0.85–1.39) | 0.93 (0.67–1.30) | 0.66 |
| AA | ||||
| Mean, % of energy | 0.02 ± 0.0003 | 0.06 ± 0.0002 | 0.13 ± 0.001 | |
| No. of deaths/person years | 337/250,636 | 262/237,907 | 283/244,070 | |
| Model 1 c | 1 (ref.) | 0.78 (0.60–1.02) | 0.82 (0.67–1.01) | 0.07 |
| Model 2 d | 1 (ref.) | 0.86 (0.64–1.14) | 1.02 (0.75–1.37) | 0.90 |
| ω-3 PUFA | ||||
| Mean, % of energy | 0.41 ± 0.003 | 0.65 ± 0.001 | 1.12 ± 0.012 | |
| No. of deaths/person years | 387/321,955 | 279/271,423 | 216/251,286 | |
| Model 1 c | 1 (ref.) | 1.04 (0.93–1.15) | 0.91 (0.79–1.03) | 0.12 |
| Model 2 d | 1 (ref.) | 0.93 (0.74–1.17) | 0.78 (0.58–1.03) | 0.09 |
| ALA | ||||
| Mean, % of energy | 0.37 ± 0.003 | 0.59 ± 0.001 | 1.00 ± 0.010 | |
| No. of deaths/person years | 380/320,237 | 280/276,767 | 222/247,660 | |
| Model 1 c | 1 (ref.) | 0.99 (0.81–1.21) | 0.89 (0.68–1.15) | 0.36 |
| Model 2 d | 1 (ref.) | 0.99 (0.80–1.22) | 0.90 (0.67–1.22) | 0.49 |
| Marine ω-3 PUFA | ||||
| Mean, % of energy | 0.002 ± 0.0001 | 0.022 ± 0.0003 | 0.19 ± 0.008 | |
| No. of deaths/person years | 453/342,543 | 183/227,727 | 246/274,394 | |
| Model 1 | 1 (ref.) | 0.72 (0.53–0.98) | 0.73(0.60–0.90) | 0.01 |
| Model 2 | 1 (ref.) | 0.73 (0.53–1.00) | 0.80(0.62–1.02) | 0.13 |
| DHA | ||||
| Mean, % of energy | 0.0005 ± 0.00003 | 0.01 ± 0.0001 | 0.11 ± 0.004 | |
| No. of deaths/person years | 432/326,118 | 193/233,996 | 257/284,550 | |
| Model 1 c | 1 (ref.) | 0.64 (0.49–0.85) | 0.75 (0.60–0.94) | 0.04 |
| Model 2 d | 1 (ref.) | 0.65 (0.48–0.88) | 0.83 (0.64–1.08) | 0.36 |
| EPA | ||||
| Mean, % of energy | 0.00003 ± 0.000003 | 0.003 ± 0.00005 | 0.06 ± 0.003 | |
| No. of deaths/person years | 531/385,458 | 167/208,040 | 184/251,166 | |
| Model 1 c | 1 (ref.) | 0.61 (0.48–0.79) | 0.60 (0.49–0.74) | <0.0001 |
| Model 2 d | 1 (ref.) | 0.56 (0.45–0.75) | 0.60 (0.48–0.75) | 0.002 |
| DPA | ||||
| Mean, % of energy | 0 ± 0 | 0.004 ± 0.00007 | 0.03 ± 0.0010 | |
| No. of deaths/person years | 550/418,989 | 156/195,684 | 176/229,991 | |
| Model 1 c | 1(ref.) | 0.66 (0.50–0.86) | 0.64 (0.50–0.82) | 0.001 |
| Model 2 d | 1(ref.) | 0.61 (0.46–0.82) | 0.64 (0.48–0.85) | 0.002 |
| Biomarkers | Total Effect | Direct Effect | Indirect Effect | MediatingProportion (%) | |
|---|---|---|---|---|---|
| EPA | TC | 0.62 (0.54–0.73) | 0.64 (0.55–0.75) | 0.97 (0.94–1.00) | 5.33% |
| TG | 0.62 (0.51–0.76) | 0.65 (0.53–0.79) | 0.96 (0.93–1.00) | 6.18% | |
| HDL | 0.63 (0.54–0.73) | 0.63 (0.54–0.74) | 0.99 (0.98–1.00) | 1.84% | |
| LDL | 0.64 (0.50–0.82) | 0.65 (0.51–0.84)) | 0.98 (0.93–1.03) | 3.94% | |
| DPA | TC | 0.69 (0.59–0.81) | 0.72 (0.61–0.85) | 0.96 (0.93–0.99) | 9.55% |
| TG | 0.63 (0.51–0.78) | 0.66 (0.53–0.81) | 0.96 (0.93–1.00) | 6.53% | |
| HDL | 0.70 (0.59–0.82) | 0.71 (0.60–0.83) | 0.99 (0.97–1.00) | 2.74% | |
| LDL | 0.71 (0.54–0.91) | 0.74 (0.57–0.96) | 0.96 (0.91–1.01) | 11.12% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, T.; Yi, J.; He, Y.; Zhang, J.; Li, X.; Ke, S.; Xia, L.; Liu, L. Associations of Dietary Fats with All-Cause Mortality and Cardiovascular Disease Mortality among Patients with Cardiometabolic Disease. Nutrients 2022, 14, 3608. https://doi.org/10.3390/nu14173608
Yang T, Yi J, He Y, Zhang J, Li X, Ke S, Xia L, Liu L. Associations of Dietary Fats with All-Cause Mortality and Cardiovascular Disease Mortality among Patients with Cardiometabolic Disease. Nutrients. 2022; 14(17):3608. https://doi.org/10.3390/nu14173608
Chicago/Turabian StyleYang, Tingting, Jing Yi, Yangting He, Jia Zhang, Xinying Li, Songqing Ke, Lu Xia, and Li Liu. 2022. "Associations of Dietary Fats with All-Cause Mortality and Cardiovascular Disease Mortality among Patients with Cardiometabolic Disease" Nutrients 14, no. 17: 3608. https://doi.org/10.3390/nu14173608
APA StyleYang, T., Yi, J., He, Y., Zhang, J., Li, X., Ke, S., Xia, L., & Liu, L. (2022). Associations of Dietary Fats with All-Cause Mortality and Cardiovascular Disease Mortality among Patients with Cardiometabolic Disease. Nutrients, 14(17), 3608. https://doi.org/10.3390/nu14173608