
Association between Habitual Tea Consumption and Metabolic Syndrome and Its Components among Chinese Adults Aged 18~59 Years: Based on China Nutrition and Health Surveillance 2015–2017


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Basic Information
2.3. Dietary Information
2.4. Medical Examination
2.5. Definition of Tea Consumption
2.6. Definition of MetS
2.7. Potential Confounders
2.8. Statistical Analyses
3. Results
3.1. Basic Characteristics
3.2. Energy Intake and Biomarkers of MetS
3.3. Association between Habitual Tea Consumption and MetS
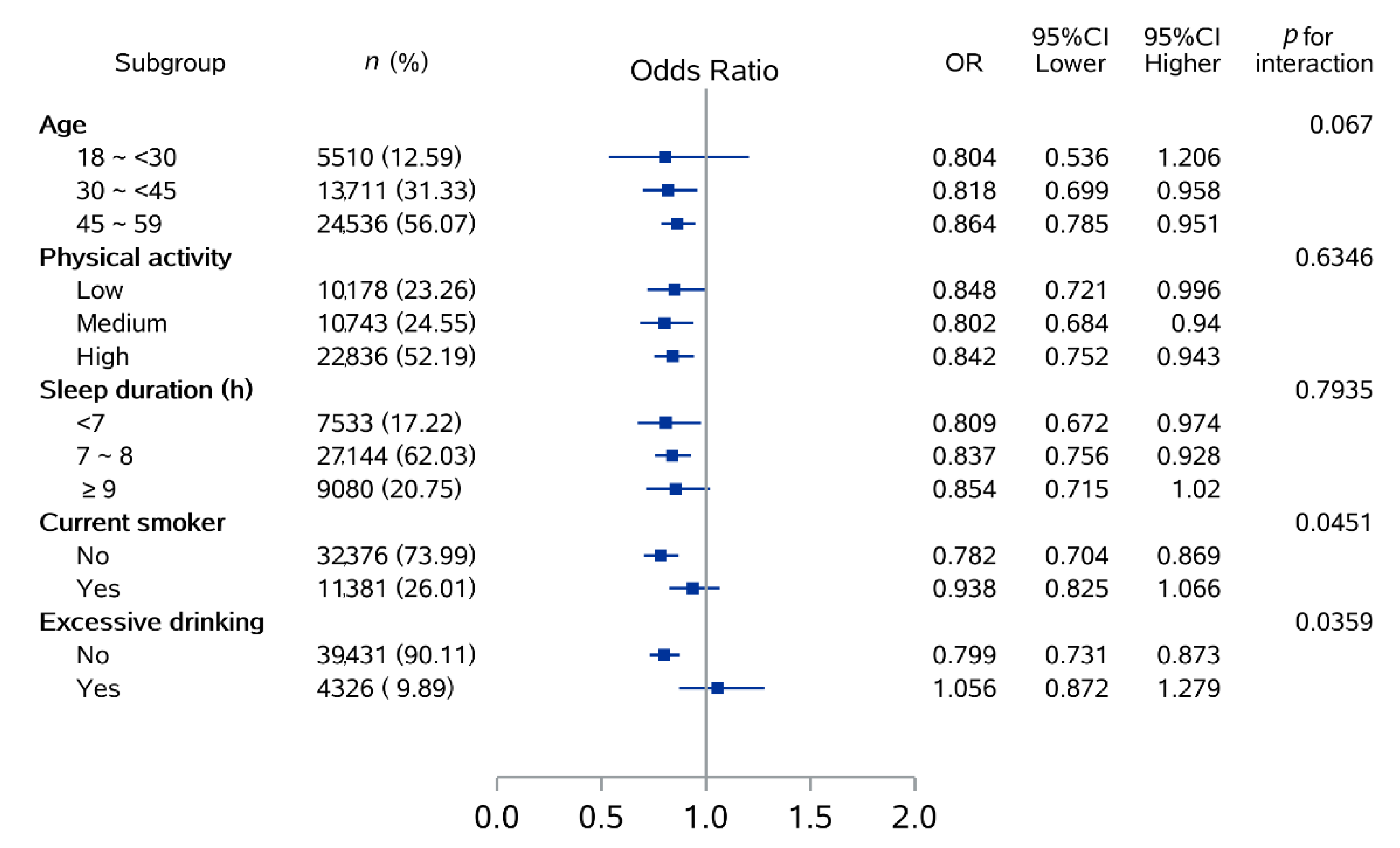
3.4. Subgroup Analysis
3.5. Association between Habitual Tea Consumption and Each Component of MetS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cicero, A.F.; Colletti, A. Role of phytochemicals in the management of metabolic syndrome. Phytomedicine 2016, 23, 1134–1144. [Google Scholar] [CrossRef]
- Dong, X.X.; Wang, R.R.; Liu, J.Y.; Ma, Q.H.; Pan, C.W. Habitual tea consumption and 5-year incident metabolic syndrome among older adults: A community-based cohort study. BMC Geriatr. 2021, 21, 728. [Google Scholar] [CrossRef]
- Ervin, R.B. Prevalence of metabolic syndrome among adults 20 years of age and over, by sex, age, race and ethnicity, and body mass index: United States, 2003-2006. Natl. Health Stat. Rep. 2009, 13, 1–7. [Google Scholar]
- Wu, S.H.; Liu, Z.; Ho, S.C. Metabolic syndrome and all-cause mortality: A meta-analysis of prospective cohort studies. Eur. J. Epidemiol. 2010, 25, 375–384. [Google Scholar] [CrossRef]
- Lu, J.; Wang, L.; Li, M.; Xu, Y.; Jiang, Y.; Wang, W.; Li, J.; Mi, S.; Zhang, M.; Li, Y.; et al. Metabolic Syndrome Among Adults in China: The 2010 China Noncommunicable Disease Surveillance. J. Clin. Endocrinol. Metab. 2017, 102, 507–515. [Google Scholar] [CrossRef]
- Buscemi, S.; Sprini, D.; Grosso, G.; Galvano, F.; Nicolucci, A.; Lucisano, G.; Massenti, F.M.; Amodio, E.; Rini, G.B. Impact of lifestyle on metabolic syndrome in apparently healthy people. Eat. Weight Disord 2014, 19, 225–232. [Google Scholar] [CrossRef]
- Yang, C.S.; Wang, H.; Sheridan, Z.P. Studies on prevention of obesity, metabolic syndrome, diabetes, cardiovascular diseases and cancer by tea. J. Food Drug Anal. 2018, 26, 1–13. [Google Scholar] [CrossRef]
- Cornelis, M.C.; van Dam, R.M. Habitual Coffee and Tea Consumption and Cardiometabolic Biomarkers in the UK Biobank: The Role of Beverage Types and Genetic Variation. J. Nutr. 2020, 150, 2772–2788. [Google Scholar] [CrossRef]
- Liu, W.; Wan, C.; Huang, Y.; Li, M. Effects of tea consumption on metabolic syndrome: A systematic review and meta-analysis of randomized clinical trials. Phytother. Res. 2020, 34, 2857–2866. [Google Scholar] [CrossRef]
- Psaltopoulou, T.; Ilias, I.; Alevizaki, M. The role of diet and lifestyle in primary, secondary, and tertiary diabetes prevention: A review of meta-analyses. Rev. Diabet. Stud. 2010, 7, 26–35. [Google Scholar] [CrossRef]
- Zheng, X.X.; Xu, Y.L.; Li, S.H.; Liu, X.X.; Hui, R.; Huang, X.H. Green tea intake lowers fasting serum total and LDL cholesterol in adults: A meta-analysis of 14 randomized controlled trials. Am. J. Clin. Nutr. 2011, 94, 601–610. [Google Scholar] [CrossRef] [Green Version]
- Marventano, S.; Salomone, F.; Godos, J.; Pluchinotta, F.; Del Rio, D.; Mistretta, A.; Grosso, G. Coffee and tea consumption in relation with non-alcoholic fatty liver and metabolic syndrome: A systematic review and meta-analysis of observational studies. Clin. Nutr. 2016, 35, 1269–1281. [Google Scholar] [CrossRef]
- Yu, D.; Zhao, L.; Zhang, J.; Yang, Z.; Yang, L.; Huang, J.; Fang, H.; Guo, Q.; Xu, X.; Ju, L.; et al. China Nutrition and Health Surveys (1982-2017). China CDC Wkly. 2021, 3, 193–195. [Google Scholar] [CrossRef]
- Liu, D.; He, L.; Zhang, X.; Zhai, Y.; Zhang, J.; Yang, X.; Chen, J.; Zhao, W. Establishment and application of food frequency questionnaire method among Chinese. Wei Sheng Yan Jiu 2018, 47, 744–755. [Google Scholar]
- Yang, Y.X.; Wang, G.Y.; He, M.; Pan, X.C.; Wang, Z. China Food Consumption Standard Edition; Peking University Medical Press: Beijing, China, 2018. [Google Scholar]
- Yang, Y.X.; Wang, G.Y.; Pan, X.C. China Food Composition, 2nd ed.; Peking University Medical Press: Beijing, China, 2009. [Google Scholar]
- Castro-Barquero, S.; Ruiz-Leon, A.M.; Sierra-Perez, M.; Estruch, R.; Casas, R. Dietary Strategies for Metabolic Syndrome: A Comprehensive Review. Nutrients 2020, 12, 2983. [Google Scholar] [CrossRef]
- Xiao, M.L.; Lin, J.S.; Li, Y.H.; Liu, M.; Deng, Y.Y.; Wang, C.Y.; Chen, Y.M. Adherence to the Dietary Approaches to Stop Hypertension (DASH) diet is associated with lower presence of non-alcoholic fatty liver disease in middle-aged and elderly adults. Public Health Nutr. 2020, 23, 674–682. [Google Scholar] [CrossRef]
- Miller, P.E.; Cross, A.J.; Subar, A.F.; Krebs-Smith, S.M.; Park, Y.; Powell-Wiley, T.; Hollenbeck, A.; Reedy, J. Comparison of 4 established DASH diet indexes: Examining associations of index scores and colorectal cancer. Am. J. Clin. Nutr. 2013, 98, 794–803. [Google Scholar] [CrossRef]
- Yang, Y.; Piao, W.; Huang, K.; Fang, H.; Ju, L.; Zhao, L.; Yu, D.; Ma, Y. Dietary Pattern Associated with the Risk of Hyperuricemia in Chinese Elderly: Result from China Nutrition and Health Surveillance 2015–2017. Nutrients 2022, 14, 844. [Google Scholar] [CrossRef]
- Yao, F.; Bo, Y.; Zhao, L.; Li, Y.; Ju, L.; Fang, H.; Piao, W.; Yu, D.; Lao, X. Prevalence and Influencing Factors of Metabolic Syndrome among Adults in China from 2015 to 2017. Nutrients 2021, 13, 4475. [Google Scholar] [CrossRef]
- Fan, M.; Lyu, J.; He, P. Chinese guidelines for data processing and analysis concerning the International Physical Activity Questionnaire. Zhonghua Liu Xing Bing Xue Za Zhi 2014, 35, 961–964. [Google Scholar]
- Grosso, G.; Stepaniak, U.; Micek, A.; Topor-Madry, R.; Pikhart, H.; Szafraniec, K.; Pajak, A. Association of daily coffee and tea consumption and metabolic syndrome: Results from the Polish arm of the HAPIEE study. Eur. J. Nutr. 2015, 54, 1129–1137. [Google Scholar] [CrossRef]
- Micek, A.; Grosso, G.; Polak, M.; Kozakiewicz, K.; Tykarski, A.; Puch Walczak, A.; Drygas, W.; Kwasniewska, M.; Pajak, A. Association between tea and coffee consumption and prevalence of metabolic syndrome in Poland—Results from the WOBASZ II study (2013–2014). Int. J. Food Sci. Nutr. 2018, 69, 358–368. [Google Scholar] [CrossRef]
- Vernarelli, J.A.; Lambert, J.D. Tea consumption is inversely associated with weight status and other markers for metabolic syndrome in US adults. Eur. J. Nutr. 2013, 52, 1039–1048. [Google Scholar] [CrossRef]
- Koziarska-Rosciszewska, M.; Gluba-Brzozka, A.; Franczyk, B.; Rysz, J. High-Sensitivity C-Reactive Protein Relationship with Metabolic Disorders and Cardiovascular Diseases Risk Factors. Life 2021, 11, 742. [Google Scholar] [CrossRef]
- Islam, M.A. Cardiovascular effects of green tea catechins: Progress and promise. Recent Pat. Cardiovasc. Drug Discov. 2012, 7, 88–99. [Google Scholar] [CrossRef]
- Meng, S.; Cao, J.; Feng, Q.; Peng, J.; Hu, Y. Roles of chlorogenic Acid on regulating glucose and lipids metabolism: A review. Evid. Based Complement. Altern. Med. 2013, 2013, 801457. [Google Scholar] [CrossRef]
- Sae-tan, S.; Grove, K.A.; Lambert, J.D. Weight control and prevention of metabolic syndrome by green tea. Pharmacol. Res. 2011, 64, 146–154. [Google Scholar] [CrossRef]
- Li, X.; Wang, W.; Hou, L.; Wu, H.; Wu, Y.; Xu, R.; Xiao, Y.; Wang, X. Does tea extract supplementation benefit metabolic syndrome and obesity? A systematic review and meta-analysis. Clin. Nutr. 2020, 39, 1049–1058. [Google Scholar] [CrossRef]
- Grosso, G.; Stepaniak, U.; Topor-Madry, R.; Szafraniec, K.; Pajak, A. Estimated dietary intake and major food sources of polyphenols in the Polish arm of the HAPIEE study. Nutrition 2014, 30, 1398–1403. [Google Scholar] [CrossRef]
- Wang, X.; Liu, F.; Li, J.; Yang, X.; Chen, J.; Cao, J.; Wu, X.; Lu, X.; Huang, J.; Li, Y.; et al. Tea consumption and the risk of atherosclerotic cardiovascular disease and all-cause mortality: The China-PAR project. Eur. J. Prev. Cardiol. 2020, 27, 1956–1963. [Google Scholar] [CrossRef]
- Hibi, M.; Takase, H.; Iwasaki, M.; Osaki, N.; Katsuragi, Y. Efficacy of tea catechin-rich beverages to reduce abdominal adiposity and metabolic syndrome risks in obese and overweight subjects: A pooled analysis of 6 human trials. Nutr. Res. 2018, 55, 1–10. [Google Scholar] [CrossRef]
- Voskoboinik, A.; Koh, Y.; Kistler, P.M. Cardiovascular effects of caffeinated beverages. Trends Cardiovasc. Med. 2019, 29, 345–350. [Google Scholar] [CrossRef]
- Godos, J.; Pluchinotta, F.R.; Marventano, S.; Buscemi, S.; Li Volti, G.; Galvano, F.; Grosso, G. Coffee components and cardiovascular risk: Beneficial and detrimental effects. Int. J. Food Sci. Nutr. 2014, 65, 925–936. [Google Scholar] [CrossRef]
- Jin, J.S.; Touyama, M.; Hisada, T.; Benno, Y. Effects of green tea consumption on human fecal microbiota with special reference to Bifidobacterium species. Microbiol. Immunol. 2012, 56, 729–739. [Google Scholar] [CrossRef]
- Yang, C.S.; Zhang, J.; Zhang, L.; Huang, J.; Wang, Y. Mechanisms of body weight reduction and metabolic syndrome alleviation by tea. Mol. Nutr. Food Res. 2016, 60, 160–174. [Google Scholar] [CrossRef]
- Munir, K.M.; Chandrasekaran, S.; Gao, F.; Quon, M.J. Mechanisms for food polyphenols to ameliorate insulin resistance and endothelial dysfunction: Therapeutic implications for diabetes and its cardiovascular complications. Am. J. Physiol. Endocrinol. Metab. 2013, 305, E679–E686. [Google Scholar] [CrossRef]
- Dinh, T.C.; Thi Phuong, T.N.; Minh, L.B.; Minh Thuc, V.T.; Bac, N.D.; Van Tien, N.; Pham, V.H.; Show, P.L.; Tao, Y.; Nhu Ngoc, V.T.; et al. The effects of green tea on lipid metabolism and its potential applications for obesity and related metabolic disorders—An existing update. Diabetes Metab. Syndr. 2019, 13, 1667–1673. [Google Scholar] [CrossRef]
- Sirotkin, A.V.; Kolesarova, A. The anti-obesity and health-promoting effects of tea and coffee. Physiol. Res. 2021, 70, 161–168. [Google Scholar] [CrossRef]
- van den Brandt, P.A. Coffee or Tea? A prospective cohort study on the associations of coffee and tea intake with overall and cause-specific mortality in men versus women. Eur. J. Epidemiol. 2018, 33, 183–200. [Google Scholar] [CrossRef]
- Yang, C.S.; Hong, J. Prevention of chronic diseases by tea: Possible mechanisms and human relevance. Annu. Rev. Nutr. 2013, 33, 161–181. [Google Scholar] [CrossRef]
- Schonthal, A.H. Adverse effects of concentrated green tea extracts. Mol. Nutr. Food Res. 2011, 55, 874–885. [Google Scholar] [CrossRef]
- Mineharu, Y.; Koizumi, A.; Wada, Y.; Iso, H.; Watanabe, Y.; Date, C.; Yamamoto, A.; Kikuchi, S.; Inaba, Y.; Toyoshima, H.; et al. Coffee, green tea, black tea and oolong tea consumption and risk of mortality from cardiovascular disease in Japanese men and women. J. Epidemiol. Community Health 2011, 65, 230–240. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Components of MetS | Gender | |
|---|---|---|
| Male | Female | |
| WC (cm) | WC ≥ 90 cm | WC ≥ 80 cm |
| BP (mmHg) | SBP ≥ 130 mmHg and (or) DBP ≥ 85 mmHg and (or) receiving anti-hypertension treatment | |
| TG (mmol/L) | TG ≥ 1.7 mmol/L and (or) receiving corresponding treatment | |
| HDL-C (mmol/L) | HDL-C < 1.03 mmol/L and (or) receiving corresponding treatment | HDL-C < 1.3 mmol/L and (or) receiving corresponding treatment |
| FPG (mmol/L) | FPG ≥ 5.6 mmol/L and (or) receiving anti-diabetes treatment and (or) had pre-diagnosed with diabetes | |
| Characteristics | Habitual Tea Consumption (n, %) | |||
|---|---|---|---|---|
| None | 1~2 Cups/Day | 3~4 Cups/Day | Over 5 Cups/Day | |
| Gender * | ||||
| Male | 11,366 (36.9%) | 2495 (53.89%) | 2142 (62.38%) | 3436 (70.25%) |
| Female | 19,436 (63.1%) | 2135 (46.11%) | 1292 (37.62%) | 1455 (29.75%) |
| Age (year) * | ||||
| 18~<30 | 4328 (14.05%) | 569 (12.29%) | 294 (8.56%) | 319 (6.52%) |
| 30~<45 | 9561 (31.04%) | 1608 (34.73%) | 1105 (32.18%) | 1437 (29.38%) |
| 45~59 | 16,913 (54.91%) | 2453 (52.98%) | 2035 (59.26%) | 3135 (64.1%) |
| BMI * | ||||
| Underweight | 1116 (3.62%) | 148 (3.2%) | 96 (2.8%) | 187 (3.82%) |
| Normal | 14,585 (47.35%) | 2130 (46%) | 1539 (44.82%) | 2207 (45.12%) |
| Overweight | 10,803 (35.07%) | 1610 (34.77%) | 1216 (35.41%) | 1722 (35.21%) |
| Obese | 4298 (13.95%) | 742 (16.03%) | 583 (16.98%) | 775 (15.85%) |
| Living area * | ||||
| Urban | 12,163 (39.49%) | 1968 (42.51%) | 1443 (42.02%) | 2016 (41.22%) |
| Rural | 18,639 (60.51%) | 2662 (57.49%) | 1991 (57.98%) | 2875 (58.78%) |
| Education level * | ||||
| Primary school or below | 12,063 (39.16%) | 1620 (34.99%) | 1240 (36.11%) | 1817 (37.15%) |
| Junior middle school | 11,219 (36.42%) | 1597 (34.49%) | 1246 (36.28%) | 1728 (35.33%) |
| High school or higher | 7520 (24.41%) | 1413 (30.52%) | 948 (27.61%) | 1346 (27.52%) |
| Income * | ||||
| Not given | 4660 (15.13%) | 664 (14.34%) | 423 (12.32%) | 578 (11.82%) |
| Low | 7420 (24.09%) | 1114 (24.06%) | 842 (24.52%) | 1181 (24.15%) |
| Medium | 11,740 (38.11%) | 1655 (35.75%) | 1317 (38.35%) | 1820 (37.21%) |
| High | 6982 (22.67%) | 1197 (25.85%) | 852 (24.81%) | 1312 (26.82%) |
| Marital status * | ||||
| Married | 28,487 (92.48%) | 4275 (92.33%) | 3227 (93.97%) | 4631 (94.68%) |
| Other status | 2315 (7.52%) | 355 (7.67%) | 207 (6.03%) | 260 (5.32%) |
| Current smoker * | ||||
| No | 24,503 (79.55%) | 3193 (68.96%) | 2081 (60.6%) | 2599 (53.14%) |
| Yes | 6299 (20.45%) | 1437 (31.04%) | 1353 (39.4%) | 2292 (46.86%) |
| Excessive drinking * | ||||
| No | 28,519 (92.59%) | 4102 (88.6%) | 2929 (85.29%) | 3881 (79.35%) |
| Yes | 2283 (7.41%) | 528 (11.4%) | 505 (14.71%) | 1010 (20.65%) |
| Physical activity | ||||
| Low | 7139 (23.18%) | 1080 (23.33%) | 802 (23.35%) | 1157 (23.66%) |
| Medium | 7601 (24.68%) | 1125 (24.3%) | 823 (23.97%) | 1194 (24.41%) |
| High | 16,062 (52.15%) | 2425 (52.38%) | 1809 (52.68%) | 2540 (51.93%) |
| Sedentary behavior (h) * | ||||
| <2 | 3952 (12.83%) | 503 (10.86%) | 388 (11.3%) | 514 (10.51%) |
| 2~3 | 11,717 (38.04%) | 1730 (37.37%) | 1301 (37.89%) | 1837 (37.56%) |
| ≥4 | 15,133 (49.13%) | 2397 (51.77%) | 1745 (50.82%) | 2540 (51.93%) |
| Sleep duration (h) * | ||||
| <7 | 5351 (17.37%) | 771 (16.65%) | 559 (16.28%) | 852 (17.42%) |
| 7~8 | 18,984 (61.63%) | 2958 (63.89%) | 2242 (65.29%) | 2960 (60.52%) |
| ≥9 | 6467 (21%) | 901 (19.46%) | 633 (18.43%) | 1079 (22.06%) |
| DASH-diet * | ||||
| Q1 | 8181 (26.56%) | 1203 (25.98%) | 974 (28.36%) | 1544 (31.57%) |
| Q2 | 8229 (26.72%) | 1172 (25.31%) | 910 (26.5%) | 1098 (22.45%) |
| Q3 | 7586 (24.63%) | 1151 (24.86%) | 770 (22.42%) | 1057 (21.61%) |
| Q4 | 6806 (22.1%) | 1104 (23.84%) | 780 (22.71%) | 1192 (24.37%) |
| Medical examination * | ||||
| No | 24,893 (80.82%) | 3638 (78.57%) | 2714 (79.03%) | 3693 (75.51%) |
| Yes | 5909 (19.18%) | 992 (21.43%) | 720 (20.97%) | 1198 (24.49%) |
| Family history of hypertension * | ||||
| No | 20,098 (65.25%) | 2895 (62.53%) | 2176 (63.37%) | 2980 (60.93%) |
| Yes | 10,704 (34.75%) | 1735 (37.47%) | 1258 (36.63%) | 1911 (39.07%) |
| Family history of diabetes * | ||||
| No | 27,321 (88.7%) | 4049 (87.45%) | 3011 (87.68%) | 4228 (86.44%) |
| Yes | 3481 (11.3%) | 581 (12.55%) | 423 (12.32%) | 663 (13.56%) |
| MetS | ||||
| No | 21,366 (69.37%) | 3207 (69.27%) | 2356 (68.61%) | 3434 (70.21%) |
| Yes | 9436 (30.63%) | 1423 (30.73%) | 1078 (31.39%) | 1457 (29.79%) |
| Habitual Tea Consumption | n of Cases (%) | OR (95% CI) * | ||
|---|---|---|---|---|
| Model I | Model II | Model III | ||
| Overall | ||||
| None | 9436 (30.63) | Ref. | Ref. | Ref. |
| 1~2 cups/day | 1423 (30.73) | 1.005 (0.94–1.074) | 0.993 (0.918–1.074) | 0.984 (0.909–1.065) |
| 3~4 cups/day | 1078 (31.39) | 1.036 (0.96–1.118) | 0.925 (0.846–1.012) | 0.91 (0.831–0.996) |
| Over 5 cups/day | 1457 (29.79) | 0.961 (0.9–1.026) | 0.869 (0.803–0.94) | 0.836 (0.771–0.905) |
| p for trend | - | 0.5415 | 0.0003 | <0.0001 |
| Male | ||||
| None | 3159 (27.79) | Ref. | Ref. | Ref. |
| 1~2 cups/day | 765 (30.66) | 1.149 (1.045–1.263) | 1.161 (1.04–1.297) | 1.137 (1.017–1.27) |
| 3~4 cups/day | 653 (30.49) | 1.139 (1.03–1.26) | 1.037 (0.921–1.168) | 0.999 (0.886–1.126) |
| Over 5 cups/day | 1053 (30.65) | 1.148 (1.056–1.248) | 1.046 (0.948–1.154) | 0.975 (0.882–1.078) |
| p for trend | - | 0.0002 | 0.2782 | 0.7261 |
| Female | ||||
| None | 6277 (32.3) | Ref. | Ref. | Ref. |
| 1~2 cups/day | 658 (30.82) | 0.934 (0.848–1.029) | 0.866 (0.773–0.97) | 0.874 (0.779–0.979) |
| 3~4 cups/day | 425 (32.89) | 1.028 (0.912–1.159) | 0.847 (0.736–0.975) | 0.848 (0.737–0.977) |
| Over 5 cups/day | 404 (27.77) | 0.806 (0.716–0.907) | 0.686 (0.596–0.79) | 0.679 (0.589–0.782) |
| p for trend | - | 0.0491 | <0.0001 | <0.0001 |
| Components of MetS | Habitual Tea Consumption | Overall | Male | Female | |||
|---|---|---|---|---|---|---|---|
| n of Cases (%) | OR (95% CI) * | n of Cases (%) | OR (95% CI) | n of Cases (%) | OR (95% CI) | ||
| Central obesity | None | 12,948 (42.04) | Ref. | 3333 (29.32) | Ref. | 9615 (49.47) | Ref. |
| 1~2 cups/day | 1883 (40.67) | 1.082 (0.988–1.184) | 798 (31.98) | 1.184 (1.039–1.35) | 1085 (50.82) | 0.999 (0.881–1.133) | |
| 3~4 cups/day | 1452 (42.28) | 1.2 (1.081–1.332) | 745 (34.78) | 1.317 (1.146–1.513) | 707 (54.72) | 1.076 (0.918–1.262) | |
| Over 5 cups/day | 1984 (40.56) | 1.354 (1.236–1.484) | 1201 (34.95) | 1.372 (1.221–1.541) | 783 (53.81) | 1.41 (1.209–1.644) | |
| p for trend | - | <0.0001 | – | <0.0001 | – | 0.0001 | |
| BP elevated | None | 14,604 (47.41) | Ref. | 6151 (54.12) | Ref. | 8453 (43.49) | Ref. |
| 1~2 cups/day | 2213 (47.8) | 0.929 (0.866–0.996) | 1332 (53.39) | 0.956 (0.869–1.051) | 881 (41.26) | 0.912 (0.821–1.012) | |
| 3~4 cups/day | 1734 (50.5) | 0.889 (0.821–0.963) | 1179 (55.04) | 0.933 (0.843–1.032) | 555 (42.96) | 0.854 (0.751–0.973) | |
| Over 5 cups/day | 2608 (53.32) | 0.906 (0.845–0.972) | 1980 (57.63) | 0.952 (0.874–1.036) | 628 (43.16) | 0.922 (0.815–1.043) | |
| p for trend | - | 0.0002 | – | 0.1389 | – | 0.0118 | |
| TG elevated | None | 8491 (27.58) | Ref. | 3845 (33.83) | Ref. | 4649 (23.92) | Ref. |
| 1~2 cups/day | 1405 (30.35) | 1.004 (0.934–1.078) | 956 (38.32) | 1.185 (1.077–1.303) | 449 (21.03) | 0.815 (0.727–0.914) | |
| 3~4 cups/day | 1055 (30.72) | 0.909 (0.837–0.987) | 728 (33.99) | 0.91 (0.82–1.01) | 327 (25.3) | 0.976 (0.852–1.118) | |
| Over 5 cups/day | 1440 (29.44) | 0.797 (0.741–0.857) | 1179 (34.31) | 0.913 (0.836–0.996) | 261 (17.94) | 0.625 (0.541–0.722) | |
| p for trend | - | <0.0001 | – | 0.0259 | – | <0.0001 | |
| HDL-C decreased | None | 13,093 (42.51) | Ref. | 3211 (28.25) | Ref. | 9882 (50.84) | Ref. |
| 1~2 cups/day | 1904 (41.12) | 1.073 (1.003–1.148) | 782 (31.34) | 1.133 (1.026–1.251) | 1122 (52.55) | 1.039 (0.947–1.14) | |
| 3~4 cups/day | 1293 (37.65) | 0.989 (0.915–1.07) | 628 (29.32) | 1.025 (0.921–1.142) | 665 (51.47) | 0.974 (0.867–1.095) | |
| Over 5 cups/day | 1680 (34.35) | 0.97 (0.905–1.04) | 1021 (29.71) | 1.1 (1.005–1.203) | 659 (45.29) | 0.799 (0.715–0.894) | |
| p for trend | - | 0.5893 | – | 0.0424 | – | 0.0018 | |
| FPG elevated | None | 7263 (23.58) | Ref. | 3100 (27.27) | Ref. | 4163 (21.42) | Ref. |
| 1~2 cups/day | 1076 (23.24) | 0.91 (0.843–0.982) | 636 (25.49) | 0.894 (0.807–0.99) | 440 (20.61) | 0.94 (0.838–1.055) | |
| 3~4 cups/day | 853 (24.84) | 0.89 (0.817–0.97) | 581 (27.12) | 0.897 (0.805–0.999) | 272 (21.05) | 0.893 (0.773–1.031) | |
| Over 5 cups/day | 1161 (23.74) | 0.772 (0.715–0.833) | 911 (26.51) | 0.808 (0.738–0.885) | 250 (17.18) | 0.704 (0.608–0.815) | |
| p for trend | - | <0.0001 | – | <0.0001 | – | <0.0001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.; Yu, D.; Piao, W.; Huang, K.; Zhao, L. Association between Habitual Tea Consumption and Metabolic Syndrome and Its Components among Chinese Adults Aged 18~59 Years: Based on China Nutrition and Health Surveillance 2015–2017. Nutrients 2022, 14, 3502. https://doi.org/10.3390/nu14173502
Yang Y, Yu D, Piao W, Huang K, Zhao L. Association between Habitual Tea Consumption and Metabolic Syndrome and Its Components among Chinese Adults Aged 18~59 Years: Based on China Nutrition and Health Surveillance 2015–2017. Nutrients. 2022; 14(17):3502. https://doi.org/10.3390/nu14173502
Chicago/Turabian StyleYang, Yuxiang, Dongmei Yu, Wei Piao, Kun Huang, and Liyun Zhao. 2022. "Association between Habitual Tea Consumption and Metabolic Syndrome and Its Components among Chinese Adults Aged 18~59 Years: Based on China Nutrition and Health Surveillance 2015–2017" Nutrients 14, no. 17: 3502. https://doi.org/10.3390/nu14173502
APA StyleYang, Y., Yu, D., Piao, W., Huang, K., & Zhao, L. (2022). Association between Habitual Tea Consumption and Metabolic Syndrome and Its Components among Chinese Adults Aged 18~59 Years: Based on China Nutrition and Health Surveillance 2015–2017. Nutrients, 14(17), 3502. https://doi.org/10.3390/nu14173502