
Lower All-Cause Mortality for Coronary Heart or Stroke Patients Who Adhere Better to Mediterranean Diet-An NHANES Analysis


Abstract
1. Introduction
2. Materials and Methods
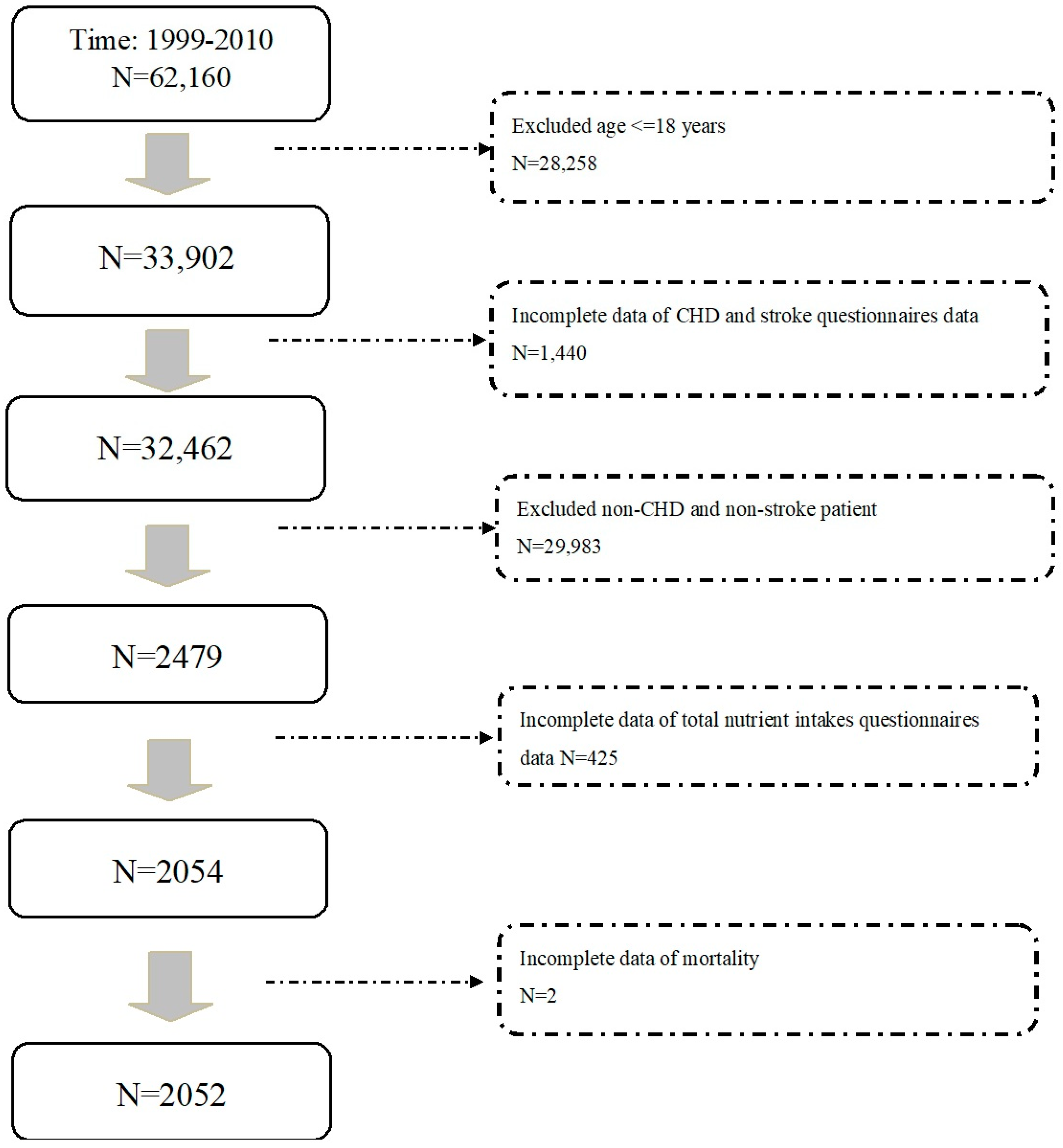
2.1. Study Participants
2.2. Definition and Scoring for MED Diet
2.3. Mortality Assessment
2.4. Statistics
3. Results
3.1. Baseline Demographic Data from NHANES Study Participants with CHD or Stroke Related to MED Diet Score
3.2. Cox Regression Analysis of Subjects with a History of CHD or Stroke for All-Cause Mortality
3.3. Cox Regression Analysis of Subjects with a History of CHD or Stroke for Cardiovascular Mortality
3.4. Cox Regression Analysis of Subjects with a History of CHD or Stroke for Cancer Mortality
3.5. Cox Regression Analysis of Subjects with a History of CHD or Stroke for Respiratory Disease, Diabetes Mellitus Related Death
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvado, J.; Covas, M.I.; Corella, D.; Aros, F.; Gomez-Gracia, E.; Ruiz-Gutierrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- de Lorgeril, M.; Salen, P.; Martin, J.L.; Monjaud, I.; Delaye, J.; Mamelle, N. Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: Final report of the Lyon Diet Heart Study. Circulation 1999, 99, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Garcia, E.; Rodriguez-Artalejo, F.; Li, T.Y.; Fung, T.T.; Li, S.; Willett, W.C.; Rimm, E.B.; Hu, F.B. The Mediterranean-style dietary pattern and mortality among men and women with cardiovascular disease. Am. J. Clin. Nutr. 2014, 99, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Shikany, J.M.; Safford, M.M.; Bryan, J.; Newby, P.K.; Richman, J.S.; Durant, R.W.; Brown, T.M.; Judd, S.E. Dietary Patterns and Mediterranean Diet Score and Hazard of Recurrent Coronary Heart Disease Events and All-Cause Mortality in the REGARDS Study. J. Am. Heart Assoc. 2018, 7, e008078. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.L.; Liu, W.J.; Wang, J.S. Association of diurnal calorie trajectory with all-cause mortality: Findings from the National Health and Nutrition Examination Survey. Clin. Nutr. 2021, 40, 1920–1925. [Google Scholar] [CrossRef] [PubMed]
- Jayanama, K.; Theou, O.; Godin, J.; Cahill, L.; Shivappa, N.; Hebert, J.R.; Wirth, M.D.; Park, Y.M.; Fung, T.T.; Rockwood, K. Relationship between diet quality scores and the risk of frailty and mortality in adults across a wide age spectrum. BMC Med. 2021, 19, 64. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; McCullough, M.L.; Newby, P.K.; Manson, J.E.; Meigs, J.B.; Rifai, N.; Willett, W.C.; Hu, F.B. Diet-quality scores and plasma concentrations of markers of inflammation and endothelial dysfunction. Am. J. Clin. Nutr. 2005, 82, 163–173. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lee, C.L.; Liu, W.J.; Wang, J.S. Associations of low-carbohydrate and low-fat intakes with all-cause mortality in subjects with prediabetes with and without insulin resistance. Clin. Nutr. 2021, 40, 3601–3607. [Google Scholar] [CrossRef] [PubMed]
- Carter, S.J.; Roberts, M.B.; Salter, J.; Eaton, C.B. Relationship between Mediterranean Diet Score and atherothrombotic risk: Findings from the Third National Health and Nutrition Examination Survey (NHANES III), 1988–1994. Atherosclerosis 2010, 210, 630–636. [Google Scholar] [CrossRef] [PubMed]
- Ha, K.; Kim, K.; Sakaki, J.R.; Chun, O.K. Relative Validity of Dietary Total Antioxidant Capacity for Predicting All-Cause Mortality in Comparison to Diet Quality Indexes in US Adults. Nutrients 2020, 12, 1210. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.Y.; Lee, C.L.; Liu, W.J.; Wang, J.S. Association of Adherence to the Mediterranean Diet with All-Cause Mortality in Subjects with Heart Failure. Nutrients 2022, 14, 842. [Google Scholar] [CrossRef] [PubMed]
- Guenther, P.M.; Casavale, K.O.; Reedy, J.; Kirkpatrick, S.I.; Hiza, H.A.; Kuczynski, K.J.; Kahle, L.L.; Krebs-Smith, S.M. Update of the Healthy Eating Index: HEI-2010. J. Acad. Nutr. Diet. 2013, 113, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Whole grain consumption and risk of cardiovascular disease, cancer, and all cause and cause specific mortality: Systematic review and dose-response meta-analysis of prospective studies. BMJ 2016, 353, i2716. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Nut consumption and risk of cardiovascular disease, total cancer, all-cause and cause-specific mortality: A systematic review and dose-response meta-analysis of prospective studies. BMC Med. 2016, 14, 207. [Google Scholar] [CrossRef] [PubMed]
- Iso, H.; Kobayashi, M.; Ishihara, J.; Sasaki, S.; Okada, K.; Kita, Y.; Kokubo, Y.; Tsugane, S. Intake of fish and n3 fatty acids and risk of coronary heart disease among Japanese: The Japan Public Health Center-Based (JPHC) Study Cohort I. Circulation 2006, 113, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef] [PubMed]
- Morze, J.; Danielewicz, A.; Przybylowicz, K.; Zeng, H.; Hoffmann, G.; Schwingshackl, L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur. J. Nutr. 2021, 60, 1561–1586. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total | aMED | aMED | aMED | p # Value | p * Value | |
|---|---|---|---|---|---|---|
| (Below Median) | (Median) | (Above Median) | ||||
| (Score 0–2) | (Score 3) | (Score 4–9) | ||||
| Number of subjects | 2052 | 630 | 511 | 911 | ||
| Age (year) | 65.1 (64.2–65.9) | 61.2 (59.9–62.4) | 64.9 (63.5–66.4) | 67.9 (66.7–69.1) | <0.0001 | <0.0001 |
| Male, n (%) | 1227 (55.2) | 361 (50.4) | 304 (55.3) | 562 (58.5) | 0.029 | 0.0073 |
| BMI (kg/m2) | 29.5 (29.2–29.8) | 30.2 (29.5–30.8) | 29.9 (29.3–30.6) | 28.8 (28.4–29.3) | <0.0001 | <0.0001 |
| SBP (mmHg) | 133.8 (132.3–135.3) | 133.1 (130.4–135.8) | 132.0 (128.7–135.2) | 135.4 (133.5–137.3) | <0.0001 | <0.0001 |
| DBP (mmHg) | 68.4 (67.4–69.4) | 70.4 (68.8–72.1) | 68.6 (66.9–70.2) | 67.0 (65.5–68.4) | <0.0001 | <0.0001 |
| Smoking, n (%) | 369 (31.7) | 181 (46.4) | 104 (36.3) | 84 (16.8) | <0.0001 | <0.0001 |
| HT, n (%) | 1469 (69.3) | 446 (67.4) | 367 (68.2) | 656 (71.2) | 0.399 | 0.1614 |
| Cholesterol (mg/dL) | 191.5 (188.2–194.9) | 194.8 (189.5–200.1) | 192.7 (187.6–197.9) | 188.6 (184.1–193.1) | <0.0001 | <0.0001 |
| HDL-C (mg/dL) | 49.1 (48.2–50.0) | 48.0 (46.5–49.4) | 48.0 (46.5–49.5) | 50.4 (49.2–51.7) | <0.0001 | <0.0001 |
| TG (mg/dL) | 174.4 (166.1–182.8) | 178.6 (165.4–191.8) | 185.8 (170.6–200.9) | 165.1 (154.2–176.0) | <0.0001 | <0.0001 |
| FPG (mg/dL) | 110.6 (108.0–113.2) | 109.0 (104.6–113.4) | 114.3 (109.0–119.6) | 109.7 (106.2–113.1) | <0.0001 | <0.0001 |
| HbA1c, % | 6.0 (5.9–6.1) | 6.0 (5.8–6.1) | 6.1 (6.0–6.3) | 6.0 (5.9–6.0) | <0.0001 | <0.0001 |
| HOMA-IR | 5.2 (4.5–6.0) | 5.7 (4.9–6.4) | 4.8 (3.9–5.6) | 5.2 (3.8–6.6) | <0.0001 | <0.0001 |
| eGFR, mL/min/1.73 m2 | 74.3 (72.9–75.7) | 78.0 (75.7–80.3) | 73.6 (70.8–76.5) | 72.1 (70.4–73.8) | <0.0001 | <0.0001 |
| Diet components | ||||||
| Calorie intake, kcal/day | 1808.9 (1753.4–1864.4) | 1700.0 (1596.9–1803.2) | 1834.7 (1706.2–1963.2) | 1871.2 (1806.4–1935.9) | <0.0001 | <0.0001 |
| % from carbohydrate | 50.7 (50.1–51.3) | 49.0 (47.8–50.2) | 50.8 (49.7–51.9) | 51.8 (51.2–52.6) | <0.0001 | <0.0001 |
| % from fat | 33.4 (32.9–34.0) | 35.1 (34.1–36.2) | 33.2 (32.2–34.1) | 32.4 (31.8–33.02) | <0.0001 | <0.0001 |
| % from protein | 15.9 (15.6–16.1) | 15.9 (15.4–16.3) | 16.1 (15.6–16.6) | 15.8 (15.3–16.2) | <0.0001 | <0.0001 |
| HEI 2010 score | 50.0 (49.1–50.9) | 40.0 (38.9–41.1) | 48.3 (47.0–49.5) | 58.9 (57.5–60.3) | <0.0001 | <0.0001 |
| Fiber (gm) | 14.9 (14.3–15.5) | 10.1 (9.2–10.9) | 14.2 (13.2–15.2) | 18.8 (18.0–19.6) | <0.0001 | <0.0001 |
| Cholesterol (mg) | 258.2 (247.8–268.7) | 260.3 (240.9–279.7) | 282.2 (251.9–312.5) | 243.4 (229.5–257.3) | <0.0001 | <0.0001 |
| Calcium (mg) | 776.9 (747.7–806.0) | 740.6 (679.5–801.7) | 749.0 (703.8–794.2) | 818.0 (780.9–855.1) | <0.0001 | <0.0001 |
| Magnesium (mg) | 257.6 (250.1–265.1) | 208.2 (195.3–221.1) | 249.4 (234.1–264.7) | 297.0 (287.6–306.5) | <0.0001 | <0.0001 |
| Sodium (mg) | 3010.8 (2904.2–3117.4) | 2813.2 (2624.4–3002.0) | 3149.6 (2918.6–3380.6) | 3072.4 (2925.4–3219.4) | <0.0001 | <0.0001 |
| Potassium (mg) | 2549.0 (2475.6–2622.5) | 2196.3 (2054.6–2338.1) | 2524.9 (2379.0–2670.9) | 2810.9 (2718.0–2903.8) | <0.0001 | <0.0001 |
| Saturated fat acids (%) | 10.9 (10.7–11.1) | 12.8 (12.3–13.3) | 10.9 (10.6–11.3) | 9.6 (9.3–9.9) | <0.0001 | <0.0001 |
| Vegetables (cup) | 0.7 (0.6–0.7) | 0.4 (0.3–0.4) | 0.7 (0.6–0.8) | 0.9 (0.8–1.0) | <0.0001 | <0.0001 |
| Fruits (cup) | 0.9 (0.9–1) | 0.4 (0.4–0.5) | 0.9 (0.7–1.0) | 1.3 (1.2–1.4) | <0.0001 | <0.0001 |
| Whole grains (gm) | 21.6 (19.6–23.6) | 8.8 (7.1–10.5) | 19.3 (15.5–23.1) | 31.9 (28.6–35.1) | <0.0001 | <0.0001 |
| Meat (gm) | 70.5 (65.6–75.4) | 98.5 (88.0–109.0) | 79.3 (68.9–89.7) | 46.1 (40.8–51.4) | <0.0001 | <0.0001 |
| Legumes (gm) | 11.8 (10.0–13.7) | 4.2 (2.7–5.7) | 9.0 (5.6–12.3) | 18.8 (15.4–22.1) | <0.0001 | <0.0001 |
| Seafood (gm) | 18.5 (14.9–22.1) | 5.4 (2.3–8.6) | 15.2 (6.8–23.7) | 29.4 (23.7–35.0) | <0.0001 | <0.0001 |
| Nuts (gm) | 13.1 (11.3–14.9) | 2.3 (1.3–3.2) | 10.6 (7.1–14.1) | 22.0 (18.7–25.3) | <0.0001 | <0.0001 |
| MUFA/SFA | 1.29 (1.17–1.21) | 1.01 (0.98–1.04) | 1.18 (1.14–1.22) | 1.32 (1.29–1.36) | <0.0001 | <0.0001 |
| Alcohol (gm) | 5.9 (4.8–7.1) | 6.3 (4.4–8.2) | 4.7 (3.0–6.5) | 6.3 (4.3–8.3) | <0.0001 | <0.0001 |
| Factors | HR | 95% CI of HR | p Value | ||
|---|---|---|---|---|---|
| Death Per 1000 Person-Years | Lower Limit | Upper Limit | |||
| All-Cause Mortality | |||||
| aMED score (below median, score 0–2) | 50.8 | 1 (reference) | |||
| aMED score (median, score 3) | 44.7 | 0.703 | 0.527 | 0.939 | 0.0175 |
| aMED score (above median, score 4–9) | 46.29 | 0.646 | 0.498 | 0.84 | 0.0013 |
| Cardiovascular Mortality | |||||
| aMED score (below median, score 0–2) | 15.41 | 1 (reference) | |||
| aMED score (median, score 3) | 16.42 | 0.861 | 0.480 | 1.545 | 0.6121 |
| aMED score (above median, score 4–9) | 14.34 | 0.699 | 0.429 | 1.137 | 0.1470 |
| Cancer Mortality | |||||
| aMED score (below median, score 0–2) | 8.94 | 1 (reference) | |||
| aMED score (median, score 3) | 8.84 | 0.838 | 0.394 | 1.783 | 0.6432 |
| aMED score (above median, score 4–9) | 6.25 | 0.543 | 0.290 | 1.016 | 0.0561 |
| Respiratory Diseases Related Mortality | |||||
| aMED score (below median, score 0–2) | 3.52 | 1 (reference) | |||
| aMED score (median, score 3) | 1.79 | 0.385 | 0.076 | 1.945 | 0.2449 |
| aMED score (above median, score 4–9) | 2.2 | 0.519 | 0.166 | 1.619 | 0.2550 |
| Diabetes Mellitus Related Mortality | |||||
| aMED score (below median, score 0–2) | 3.11 | 1 (reference) | |||
| aMED score (median, score 3) | 1.34 | 0.389 | 0.079 | 1.924 | 0.2439 |
| aMED score (above median, score 4–9) | 3.6 | 0.785 | 0.236 | 2.612 | 0.6900 |
| All Other Miscellaneous Causes Related Mortality (Residual) | |||||
| aMED score (below median, score 0–2) | 13.66 | 1 (reference) | |||
| aMED score (median, score 3) | 12.72 | 0.806 | 0.459 | 1.414 | 0.4475 |
| aMED score (above median, score 4–9) | 15.05 | 0.785 | 0.473 | 1.303 | 0.3452 |
| All-cause Mortality | CV Mortality | Cancer Mortality | ||||
|---|---|---|---|---|---|---|
| Adjusted HR (95% CI) a | p | Adjusted HR (95% CI) a | p | Adjusted HR (95% CI) a | p | |
| Components of aMED | ||||||
| Alcohol | 0.767 (0.516–1.138) | 0.1846 | 0.639 (0.269–1.517) | 0.3061 | 1.239 (0.529–2.901) | 0.6178 |
| Red/processed meat | 0.995 (0.783–1.264) | 0.968 | 0.969 (0.619–1.517) | 0.8887 | 0.817 (0.455–1.468) | 0.4953 |
| Sea food | 0.807 (0.597–1.091) | 0.1618 | 0.396 (0.163–0.964) | 0.0414 | 0.892 (0.434–1.832) | 0.7532 |
| Whole grains | 0.781 (0.615–0.992) | 0.0432 | 0.809 (0.511–1.279) | 0.3595 | 0.619 (0.334–1.144) | 0.1241 |
| Legumes | 0.979 (0.797–1.202) | 0.8386 | 1.07 (0.684–1.674) | 0.7634 | 0.62 (0.318–1.209) | 0.1587 |
| Nuts | 0.769 (0.6–0.986) | 0.0382 | 0.756 (0.49–1.166) | 0.203 | 0.948 (0.562–1.599) | 0.8393 |
| Fruits | 0.916 (0.721–1.164) | 0.4701 | 0.951 (0.609–1.484) | 0.8224 | 0.986 (0.561–1.734) | 0.9616 |
| Vegetables | 0.793 (0.613–1.027) | 0.0777 | 0.803 (0.54–1.193) | 0.2734 | 0.916 (0.575–1.458) | 0.7077 |
| MUFA/SFA | 0.923 (0.733–1.163) | 0.4923 | 0.868 (0.576–1.31) | 0.4974 | 0.808 (0.487–1.341) | 0.4054 |
| Factors | Deaths Per 1000 | HR | 95% CI of HR | p Value | |
|---|---|---|---|---|---|
| Person-Years | Lower Limit | Upper Limit | |||
| All-Cause Mortality | |||||
| aMED score (below median, score 0–2) | 40.42 | 1 (reference) | |||
| aMED score (median, score 3) | 29.53 | 0.571 | 0.393 | 0.829 | 0.0037 |
| aMED score (above median, score 4–9) | 36.09 | 0.588 | 0.431 | 0.801 | 0.0010 |
| Cardiovascular Mortality | |||||
| aMED score (below median, score 0–2) | 11.76 | 1 (reference) | |||
| aMED score (median, score 3) | 8.47 | 0.586 | 0.277 | 1.239 | 0.1596 |
| aMED score (above median, score 4–9) | 10.28 | 0.514 | 0.280 | 0.944 | 0.0323 |
| Cancer Mortality | |||||
| aMED score (below median, score 0–2) | 6.13 | 1 (reference) | |||
| aMED score (median, score 3) | 7.63 | 0.986 | 0.407 | 2.393 | 0.9754 |
| aMED score (above median, score 4–9) | 5.52 | 0.690 | 0.347 | 1.368 | 0.2837 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, K.-W.; Lee, C.-L.; Liu, W.-J. Lower All-Cause Mortality for Coronary Heart or Stroke Patients Who Adhere Better to Mediterranean Diet-An NHANES Analysis. Nutrients 2022, 14, 3203. https://doi.org/10.3390/nu14153203
Liang K-W, Lee C-L, Liu W-J. Lower All-Cause Mortality for Coronary Heart or Stroke Patients Who Adhere Better to Mediterranean Diet-An NHANES Analysis. Nutrients. 2022; 14(15):3203. https://doi.org/10.3390/nu14153203
Chicago/Turabian StyleLiang, Kae-Woei, Chia-Lin Lee, and Wei-Ju Liu. 2022. "Lower All-Cause Mortality for Coronary Heart or Stroke Patients Who Adhere Better to Mediterranean Diet-An NHANES Analysis" Nutrients 14, no. 15: 3203. https://doi.org/10.3390/nu14153203
APA StyleLiang, K.-W., Lee, C.-L., & Liu, W.-J. (2022). Lower All-Cause Mortality for Coronary Heart or Stroke Patients Who Adhere Better to Mediterranean Diet-An NHANES Analysis. Nutrients, 14(15), 3203. https://doi.org/10.3390/nu14153203