
Dietary Diversity and its Association with Nutritional Status, Cardiometabolic Risk Factors and Food Choices of Adults at Risk for Type 2 Diabetes Mellitus in Cape Town, South Africa

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Ethics
2.3. Diabetes Risk Screening
2.4. Socio-Demographic and Behavioural Risk Factors
2.5. Anthropometric Measurements
2.6. Biomedical Indicators
2.7. Food Groups Consumed and Dietary Diversity
2.8. Food Choices and Practices
2.9. Statistical Analysis
3. Results
3.1. Socio-Demography and Behavioural Risk Factors
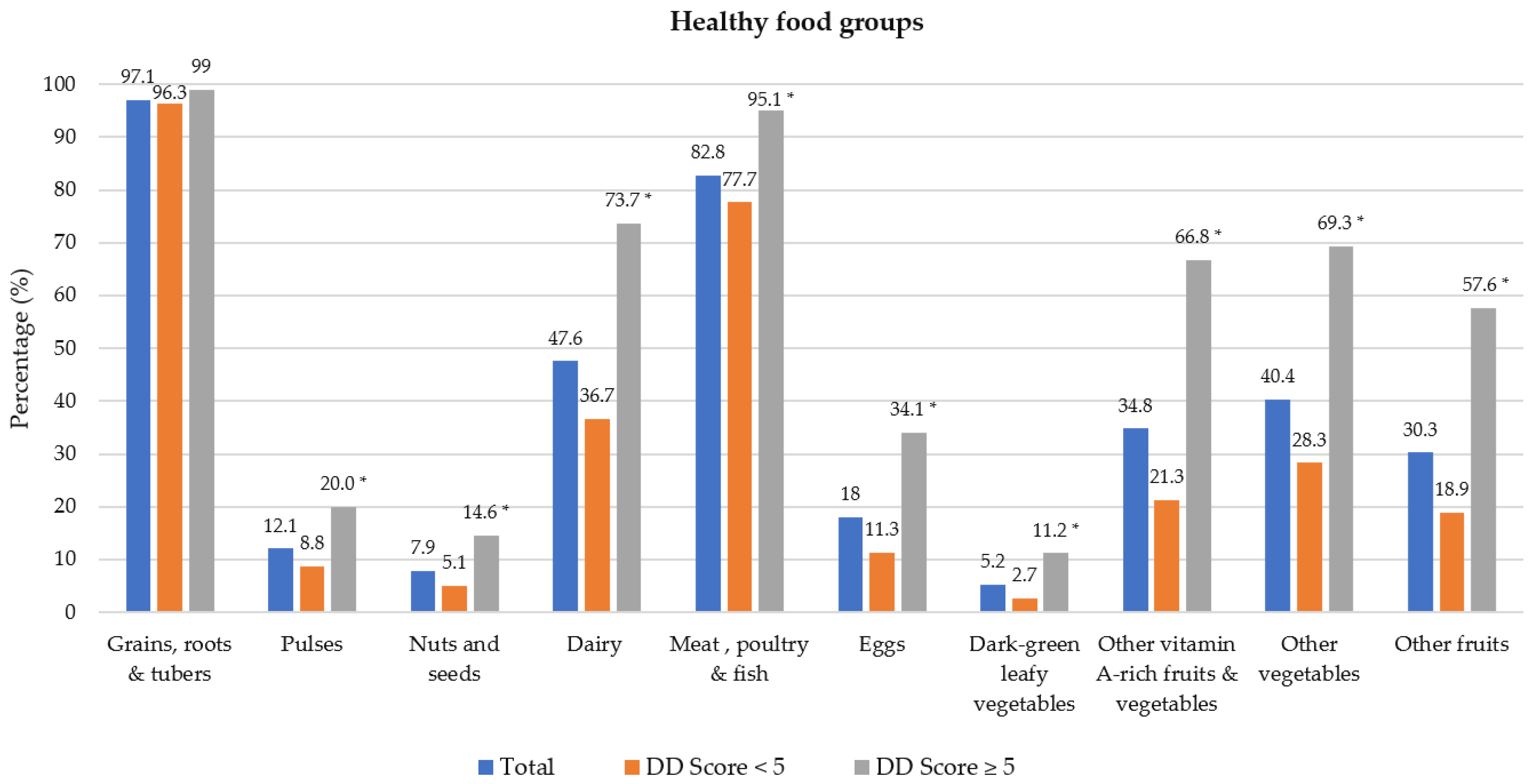
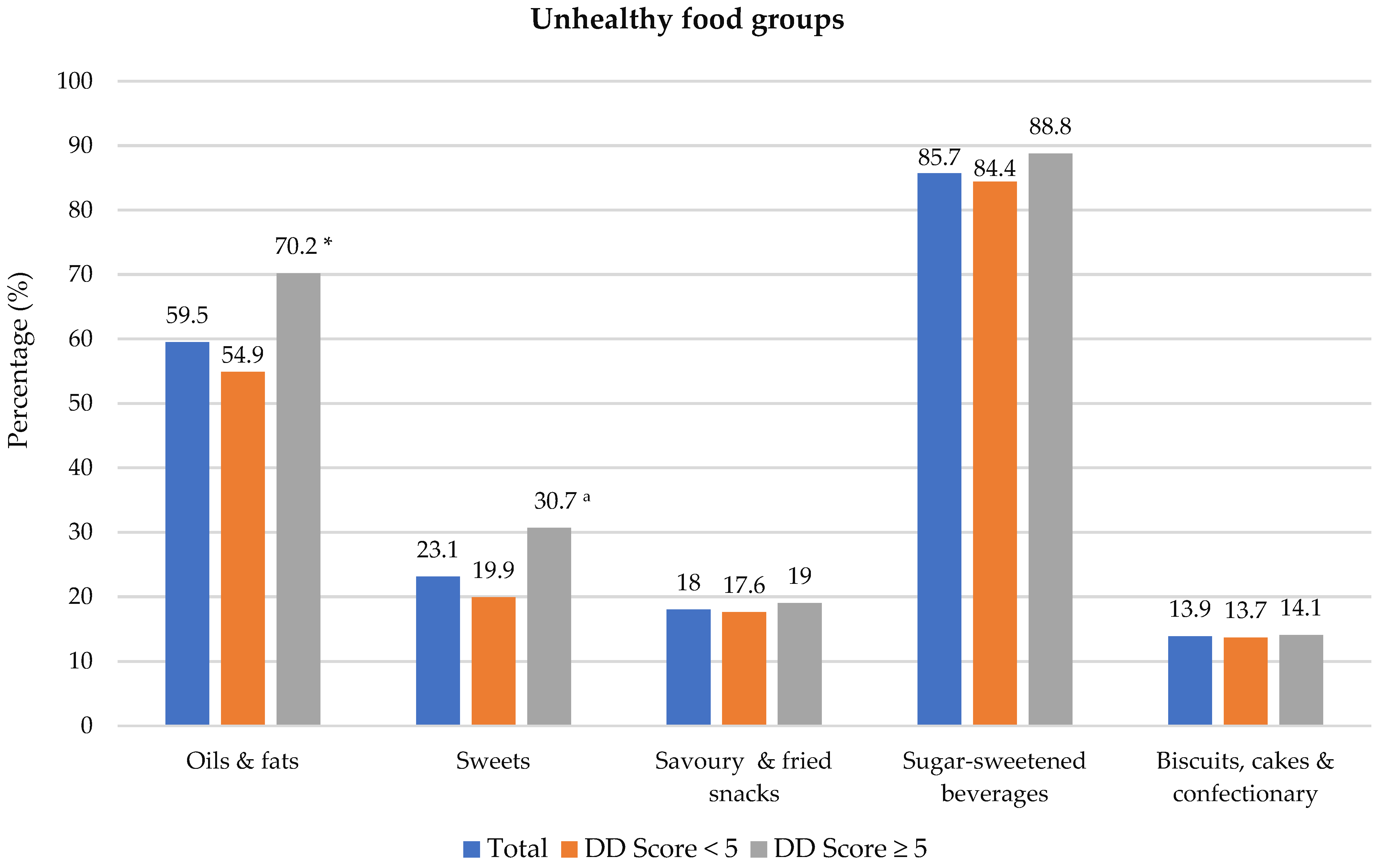
3.2. Dietary Diversity Food Groups
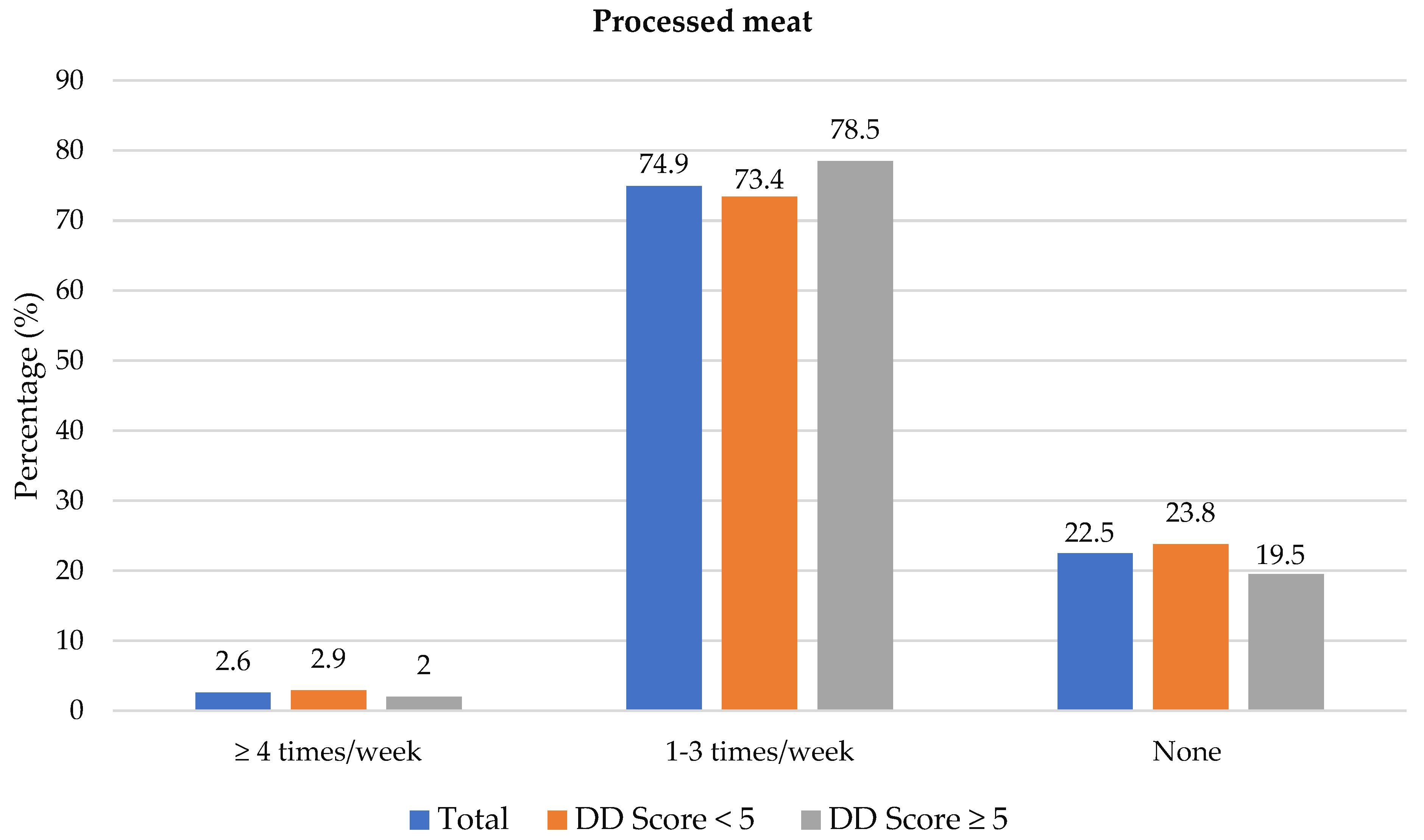
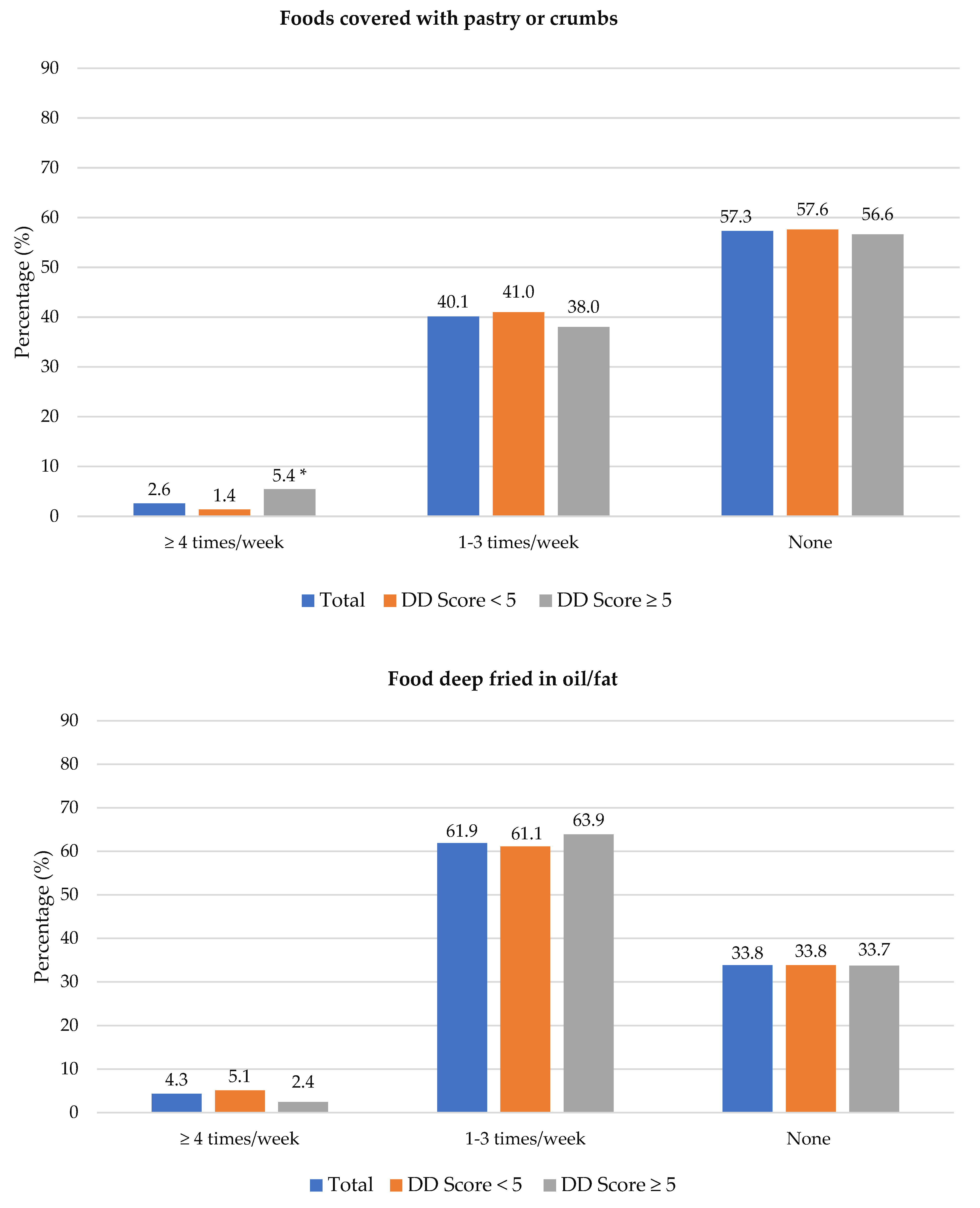
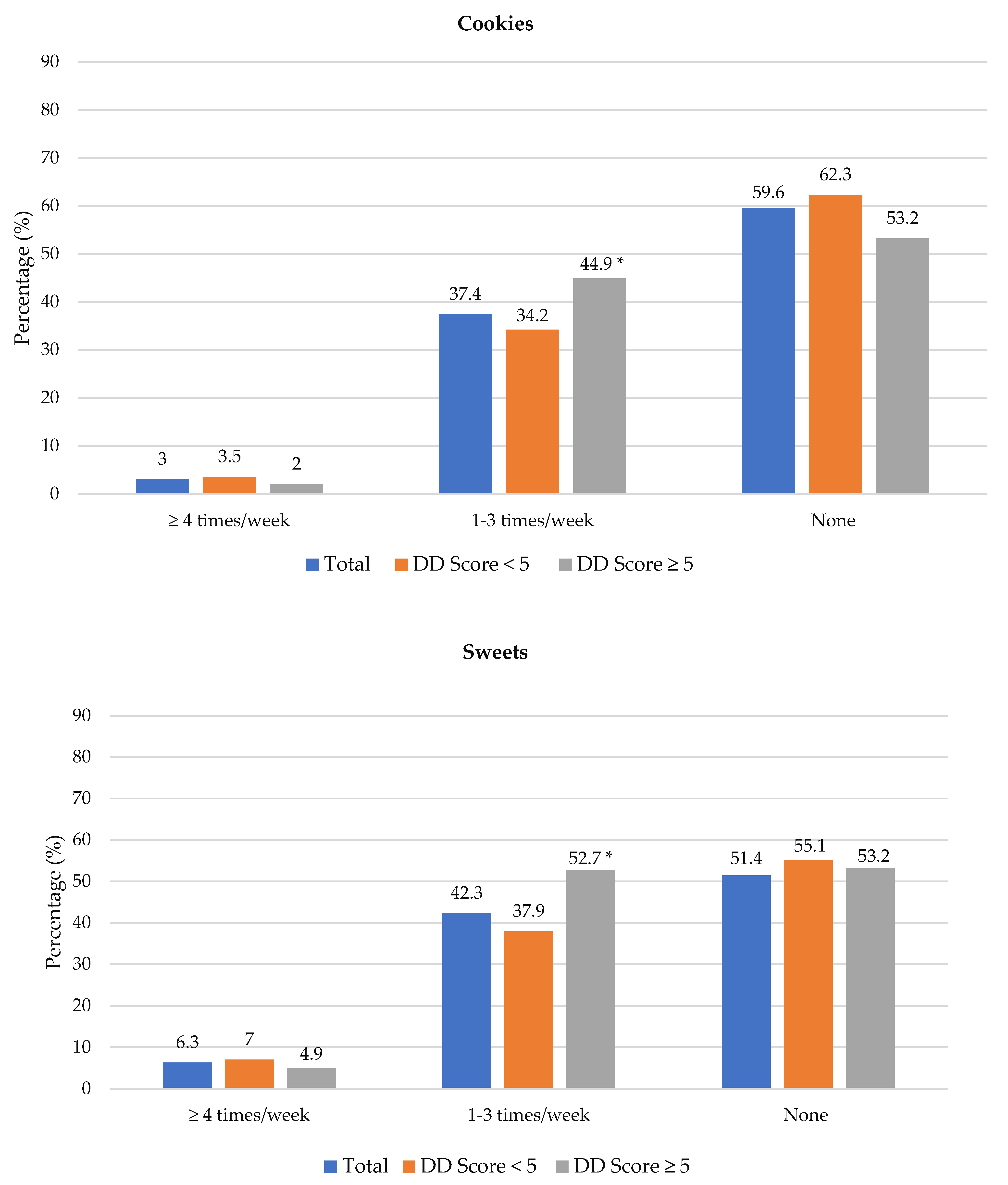
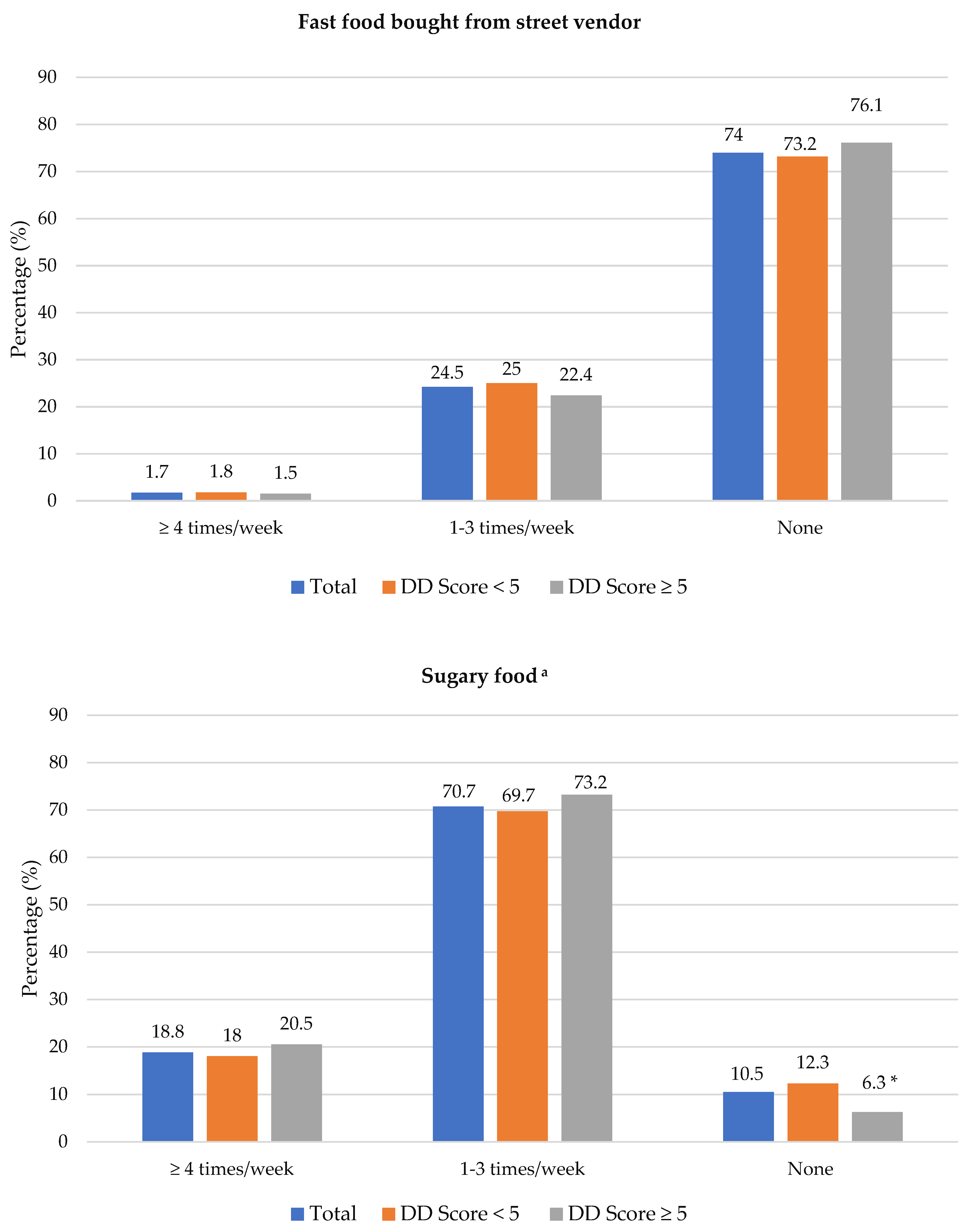
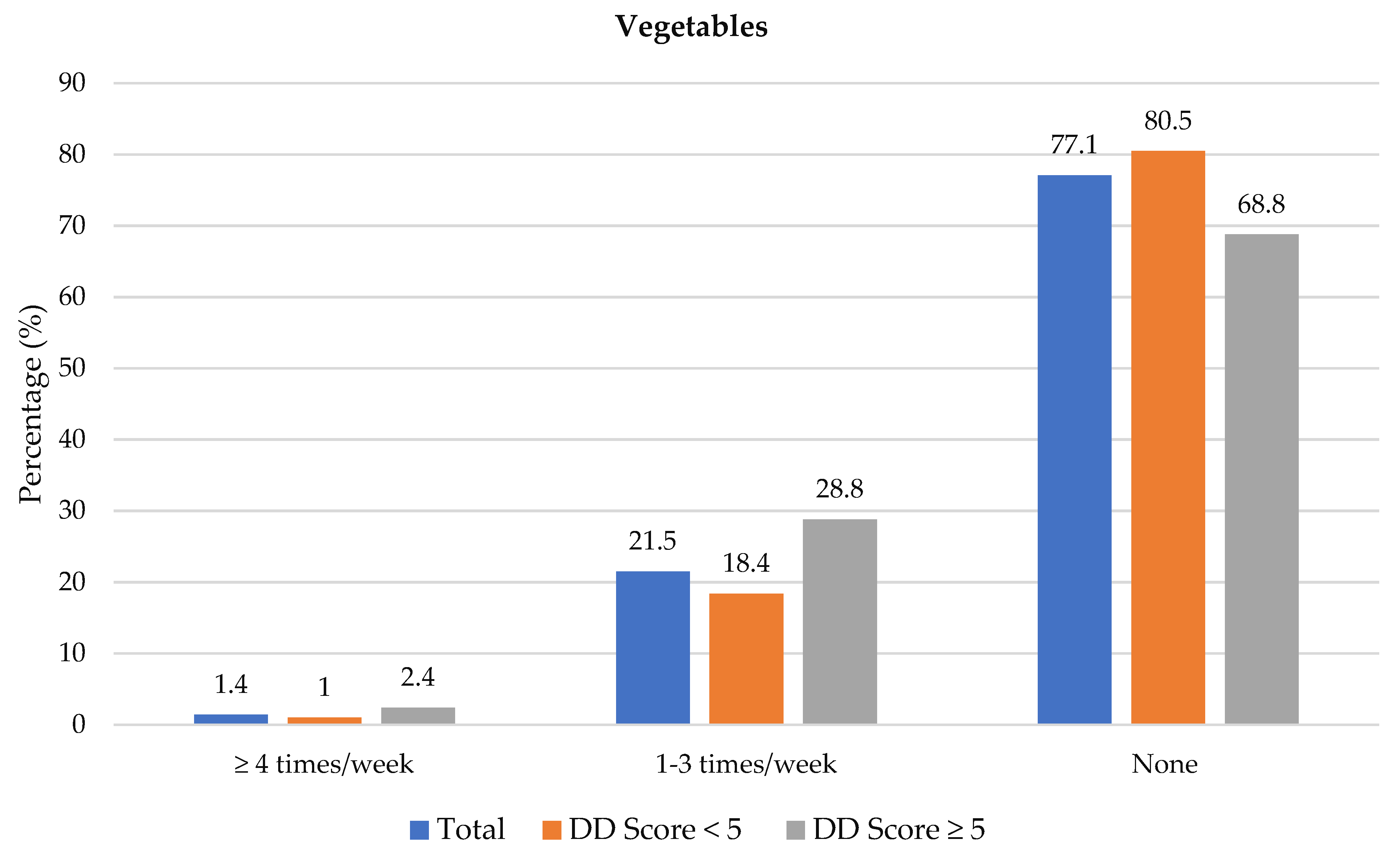
3.3. Food Choices
3.4. Nutritional Status and Cardiometabolic Risk Factors
3.4.1. Nutritional Status
3.4.2. Cardiometabolic Risk Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 14 January 2021).
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; IDF: Brussels, Belgium, 2021; Available online: https://diabetesatlas.org/atlas/tenth-edition/ (accessed on 22 February 2022).
- Pillay-van Wyk, V.; Msemburi, W.; Laubscher, R.; Dorrington, R.E.; Groenewald, P.; Glass, T.; Nojilana, B.; Joubert, J.D.; Matzopoulos, R.; Prinsloo, M.; et al. Mortality trends and differentials in South Africa from 1997 to 2012: Second National Burden of Disease Study. Lancet Glob. Health 2016, 4, e642–e665. [Google Scholar] [CrossRef] [Green Version]
- Non-Communicable Diseases (NCD) Country Profiles. Available online: https://www.who.int/nmh/publications/ncd-profiles-2018/en/ (accessed on 28 September 2020).
- Leon, B.M.; Maddox, T.M. Diabetes and cardiovascular disease: Epidemiology, biological mechanisms, treatment recommendations and future research. World J. Diabetes 2015, 6, 1246–1258. [Google Scholar] [CrossRef] [PubMed]
- Pheiffer, C.; Pillay-van Wyk, V.; Joubert, J.D.; Levitt, N.; Nglazi, M.D.; Bradshaw, D. The prevalence of type 2 diabetes in South Africa: A systematic review protocol. BMJ Open. 2018, 8, e021029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkerwi, A. Diet quality concept. Nutrition 2014, 30, 613–618. [Google Scholar] [CrossRef]
- Herforth, A.; Arimond, M.; Álvarez-Sánchez, C.; Coates, J.; Christianson, K.; Muehlhoff, E. A global review of food-based dietary guidelines. Adv. Nutr. 2019, 10, 590–605. [Google Scholar] [CrossRef] [Green Version]
- FAO and FHI 360. Minimum Dietary Diversity for Women: A Guide for Measurement; FAO: Rome, Italy, 2016; Available online: http://www.fao.org/3/a-i5486e.pdf (accessed on 23 March 2020).
- McCullough, M.L.; Feskanich, D.; Stampfer, M.J.; Giovannucci, E.L.; Rimm, E.B.; Hum, F.B.; Spiegelman, D.; Hunter, D.J.; Colditz, G.A.; Willett, W.C. Diet quality and major chronic disease risk in men and women: Moving toward improved dietary guidance. Am. J. Clin. Nutr. 2002, 76, 1261–1271. [Google Scholar] [CrossRef] [Green Version]
- Fanelli Kuczmarski, M.; Brewer, B.C.; Rawal, R.; Pohlig, R.T.; Zonderman, A.B.; Evans, M.K. Aspects of dietary diversity differ in their association with atherosclerotic cardiovascular risk in a racially diverse US adult population. Nutrients 2019, 11, 1034. [Google Scholar] [CrossRef] [Green Version]
- Farhangi, M.A.; Jahangiry, L. Dietary diversity score is associated with cardiovascular risk factors and serum adiponectin concentrations in patients with metabolic syndrome. BMC Cardiovasc. Disord. 2018, 18, 68. [Google Scholar] [CrossRef] [Green Version]
- Kapoor, D.; Iqbal, R.; Singh, K.; Jaacks, L.M.; Shivashankar, R.; Sudha, V.; Anjana, R.M.; Kadir, M.; Mohan, V.; Ali, M.K.; et al. Association of dietary patterns and dietary diversity with cardiometabolic disease risk factors among adults in South Asia: The CARRS study. Asia Pac. J. Clin. Nutr. 2018, 27, 1332–1343. [Google Scholar]
- Zhang, Q.; Chen, X.; Liu, Z.; Varma, D.S.; Wan, R.; Zhao, S. Diet diversity and nutritional status among adults in southwest China. PLoS ONE 2017, 12, e0172406. [Google Scholar] [CrossRef]
- Vadiveloo, M.; Dixon, L.B.; Parekh, N. Associations between dietary variety and measures of body adiposity: A systematic review of epidemiological studies. Br. J. Nutr. 2013, 109, 1557–1572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Oliveira Otto, M.C.; Anderson, C.A.M.; Dearborn, J.L.; Ferranti, E.P.; Mozaffarian, D.; Rao, G.; Wylie-Rosett, J.; Lichtenstein, A.H. Dietary diversity: Implications for obesity prevention in adult populations: A science advisory from the American Heart Association. Circulation 2018, 138, e160–e168. [Google Scholar] [CrossRef] [PubMed]
- Azadbakht, L.; Esmaillzadeh, A. Dietary diversity score is related to obesity and abdominal adiposity among Iranian female youth. Public Health Nutr. 2011, 14, 62–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verger, E.; Le Port, A.; Borderon, A.; Bourbon, G.; Moursi, M.; Savy, M.; Mariotti, F.; Martin-Prevel, Y. Dietary diversity indicators and their associations with dietary adequacy and health outcomes: A systematic scoping review. Adv. Nutr. 2021, 12, 1659–1672. [Google Scholar] [CrossRef]
- Claasen, N.; van der Hoeven, M.; Covic, N. Food Environments, Health and Nutrition in South Africa; Working Paper 34; PLAAS, UWC and Centre of Excellence on Food Security: Cape Town, South Africa, 2016. [Google Scholar]
- Shisana, O.; Labadarios, D.; Rehle, T.; Simbayi, L.; Zuma, K.; Dhansay, A.; Reddy, P.; Parker, W.; Hoosain, E.; Naidoo, P.; et al. South African National Health and Nutrition Examination Survey (SANHANES-1); HSRC Press: Cape Town, South Africa, 2013; Available online: http://www.hsrc.ac.za/uploads/pageNews/72/SANHANES-launch%20edition%20(online%20version).pdf (accessed on 19 January 2020).
- Labadarios, D.; Steyn, N.P.; Nel, J. How diverse is the diet of adult South Africans? Nutr. J. 2011, 10, 33. [Google Scholar] [CrossRef]
- Statistic South Africa. Mortality and Causes of Death in South Africa: Findings from Death Notification, Statistical Release P0309.3; Stats SA: Pretoria, South Africa, 2018. Available online: https://www.statssa.gov.za/publications/P03093/P030932018.pdf (accessed on 15 November 2021).
- Hill, J.; Peer, N.; Jonathan, D.; Mayige, M.; Sobngwi, E.; Kengne, A.P. Findings from community-based screenings for type 2 diabetes mellitus in at risk communities in Cape Town, South Africa: A pilot study. Int. J. Environ. Res. Public Health. 2020, 17, 2876. [Google Scholar] [CrossRef]
- Erasmus, R.T.; Soita, D.J.; Hassan, M.S.; Blanco-Blanco, E.; Vergotine, Z.; Kengne, A.P.; Matsha, T.E. High prevalence of diabetes mellitus and metabolic syndrome in a South African coloured population: Baseline data of a study in Bellville, Cape Town. S. Afr. Med. J. 2012, 102, 841–844. [Google Scholar] [CrossRef] [Green Version]
- Peer, N.; Steyn, K.; Lombard, C.; Lambert, E.V.; Vythilingum, B.; Levitt, N.S. Rising diabetes prevalence among urban-dwelling black South Africans. PLoS ONE 2012, 7, e43336. [Google Scholar] [CrossRef] [Green Version]
- Statistics South Africa. Quarterly Labour Force Survey (QLFS): Quarter 3: 2019. Statistical Release P0211; Stats SA: Pretoria, South Africa, 2019. Available online: https://www.statssa.gov.za/publications/P0211/P02113rdQuarter2019.pdf (accessed on 17 May 2020).
- Statistics South Africa. Quarterly Labour Force Survey, Quarter 4: 2020, Statistical Release P0211; Stats SA: Pretoria, South Africa, 2021. Available online: http://www.statssa.gov.za/publications/P0211/P02114thQuarter2020.pdf (accessed on 1 July 2021).
- Battersby, J. The Food desert as a concept and policy tool in African Cities: An opportunity and a risk. Sustainability 2019, 11, 458. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO STEPS Surveillance Manual; WHO: Geneva, Switzerland, 2020; Available online: https://cdn.who.int/media/docs/default-source/ncds/ncd-surveillance/steps/steps-manual_f0075411-1e6d-46ef-85be-fe826d2b9c47.pdf?sfvrsn=c281673d_5 (accessed on 8 April 2021).
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey: Anthropometry Procedures Manual. 2011. Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes_11_12/Anthropometry_Procedures_Manual.pdf (accessed on 9 June 2020).
- NHLBI Obesity Education Initiative Expert Panel on the Identification, Evaluation, and Treatment of Obesity in Adults (US). Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: The Evidence Report; National Heart, Lung, and Blood Institute: Bethesda, ML, USA, 1998. Available online: https://www.ncbi.nlm.nih.gov/books/NBK2003/ (accessed on 8 April 2020).
- World Health Organisation. Waist Circumference and Waist–Hip Ratio: Report of a WHO Expert Consultation; WHO: Geneva, Switzerland, 2008; Available online: https://apps.who.int/iris/bitstream/handle/10665/44583/9789241501491_eng.pdf;jsessionid=4BC2C8AC2200A99B4ED62DD43B5A0EAC?sequence=1 (accessed on 3 August 2020).
- World Health Organization. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications; WHO: Geneva, Switzerland, 1999. [Google Scholar]
- Klug, E.; Raal, F.J.; Marais, A.D.; Smuts, C.M.; Schamroth, C.; Jankelow, D.; Blom, D.J.; Webb, D.A. South African dyslipidaemia guideline consensus statement: 2018 update A joint statement from the South African Heart Association (SA Heart) and the Lipid and Atherosclerosis Society of Southern Africa (LASSA). S. Afr. Med. J. 2018, 108, 973–1000. [Google Scholar] [CrossRef]
- Zhang, J.; Liang, D.; Zhao, A. Dietary diversity and the risk of fracture in adults: A prospective study. Nutrients 2020, 12, 3655. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Isanaka, S.; Hu, F.B.; Willett, W.C. International food group–based diet quality and risk of coronary heart disease in men and women. Am. J. Clin. Nutr. 2018, 107, 120–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morseth, M.S.; Grewal, N.K.; Kaasa, I.S.; Hatloy, A.; Barikmo, I.; Henjum, S. Dietary diversity is related to socioeconomic status among adult Saharawi refugees living in Algeria. BMC Public Health 2017, 17, 621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Temple, N.; Steyn, N. Food prices and energy density as barriers to healthy food patterns in Cape Town, South Africa. J. Hunger. Environ. Nutr. 2009, 4, 203–213. [Google Scholar] [CrossRef]
- Statistics South Africa. Quarterly Labour Force Survey (QLFS), 4th Quarter 2021; Stats SA: Pretoria, South Africa, 2022. Available online: http://www.statssa.gov.za/publications/P0211/P02114thQuarter2021.pdf (accessed on 12 April 2022).
- South African Social Security Agency. Annual Report. Department of Social Development; SASSA: Pretoria, South Africa, 2021. Available online: https://www.sassa.gov.za/statistical-reports/Documents/Annual%20Report%20-%202021.pdf (accessed on 12 April 2022).
- Mbunyuza, L. Zero Rated and Exempt Supplies. National Department of Treasury. 2008. Available online: https://static.pmg.org.za/docs/Zero-rated%20and%20exempt%20supplies.pdf (accessed on 14 March 2022).
- Miller, V.; Yusuf, S.; Chow, C.K.; Dehghan, M.; Corsi, D.J.; Lock, K.; Popkin, B.; Rangarajan, S.; Khatib, R.; Lear, S.A.; et al. Availability, affordability, and consumption of fruits and vegetables in 18 countries across income levels: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet Glob. Health. 2016, 4, e695–e703. [Google Scholar] [CrossRef] [Green Version]
- Drimie, S.; Faber, M.; Vearey, J.; Nunez, L. Dietary diversity of formal and informal residents in Johannesburg, South Africa. BMC Public Health 2013, 13, 911. [Google Scholar] [CrossRef]
- Mekonnen, D.A.; Trijsburg, L.; Achterbosch, T.; Brouwer, I.D.; Kennedy, G.; Linderhof, V.; Ruben, R.; Talsma, E.F. Food consumption patterns, nutrient adequacy, and the food systems in Nigeria. Agric. Food Econ. 2021, 9, 16. [Google Scholar] [CrossRef]
- Ochieng, J.; Afari-Sefa, V.; Lukumay, P.J.; Dubois, T. Determinants of dietary diversity and the potential role of men in improving household nutrition in Tanzania. PLoS ONE 2017, 12, e0189022. [Google Scholar] [CrossRef] [Green Version]
- Nnyepi, M.S.; Gwisai, N.; Lekgoa, M.; Seru, T. Evidence of nutrition transition in Southern Africa. Proc. Nutr. Soc. 2015, 74, 478–486. [Google Scholar] [CrossRef] [Green Version]
- Ronquest-Ross, L.C.; Vink, N.; Sigge, G. Food consumption changes in South Africa since 1994. S. Afr. J. Sci. 2015, 111, 1–12. [Google Scholar] [CrossRef]
- Mchiza, Z.J.; Steyn, N.P.; Hill, J.; Kruger, A.; Schönfeldt, H.; Nel, J.; Wentzel-Viljoen, E. A Review of dietary surveys in the adult South African population from 2000 to 2015. Nutrients 2015, 7, 8227–8250. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Fact Sheet: Healthy Diet; WHO: Geneva, Switzerland, 2018; Available online: www.who.int/news-room/fact-sheets/detail/healthy-diet (accessed on 20 May 2019).
- Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [CrossRef] [Green Version]
- Faber, M.; Wenhold, F.A.; Laurie, S.M. Dietary diversity and vegetable and fruit consumption of households in a resource-poor peri-urban South Africa community differ by food security status. Ecol. Food Nutr. 2017, 56, 62–80. [Google Scholar] [CrossRef] [PubMed]
- Okop, K.J.; Ndayi, K.; Tsolekile, L.; Sanders, D.; Puoane, T. Low intake of commonly available fruits and vegetables in socio-economically disadvantaged communities of South Africa: Influence of affordability and sugary drinks intake. BMC Public Health 2019, 19, 940. [Google Scholar] [CrossRef] [Green Version]
- de Oliveira Otto, M.C.; Padhye, N.S.; Bertoni, A.G.; Jacobs, D.R., Jr.; Mozaffarian, D. Everything in moderation—Dietary diversity and quality, central obesity and risk of diabetes. PLoS ONE 2015, 10, e0141341. [Google Scholar] [CrossRef] [Green Version]
- National Department of Health (NDoH) SSASS; South African Medical Research Council (SAMRC); ICF. South Africa Demographic and Health Survey 2016; NDoH, Stats SA; SAMRC: Pretoria, South Africa; ICF: Rockville, ML, USA, 2019. Available online: https://dhsprogram.com/pubs/pdf/FR337/FR337.pdf (accessed on 29 March 2022).
- Igumbor, E.U.; Sanders, D.; Puoane, T.R.; Tsolekile, L.; Schwarz, C.; Purdy, C.; Swart, R.; Durão, S.; Hawkes, C. “Big Food,” the Consumer Food Environment, Health, and the Policy Response in South Africa. PLoS Med. 2012, 9, e1001253. [Google Scholar] [CrossRef] [Green Version]
- National Department of Health. National Strategic Plan for the Prevention and Control of Non-Communicable Diseases 2020–2025. Available online: https://www.sancda.org.za/wp-content/uploads/2020/05/17-May-2020-South-Africa-NCD-STRATEGIC-PLAN_For-Circulation.pdf (accessed on 8 March 2022).
- Qorbani, M.; Mahdavi-Gorabi, A.; Khatibi, N.; Ejtahed, H.-S.; Khazdouz, M.; Djalalinia, S.; Sahebkar, A.; Esmaeili-Abdar, M.; Hasani, M. Dietary diversity score and cardio-metabolic risk factors: An updated systematic review and meta-analysis. Eat. Weight. Disord. 2022, 27, 85–100. [Google Scholar] [CrossRef]
- Salehi-Abargouei, A.; Akbari, F.; Bellissimo, N.; Azadbakht, L. Dietary diversity score and obesity: A systematic review and meta-analysis of observational studies. Eur. J. Clin. Nutr. 2016, 70, 1–9. [Google Scholar] [CrossRef]
- Rico-Campà, A.; Martínez-González, M.A.; Alvarez-Alvarez, I.; Mendonça, R.d.D.; de la Fuente-Arrillaga, C.; Gómez-Donoso, C.; Bes-Rastrollo, M. Association between consumption of ultra-processed foods and all cause mortality: SUN prospective cohort study. BMJ 2019, 365, l1949. [Google Scholar] [CrossRef] [Green Version]
- Zhang, A.; Yao, Y.; Xue, Z.; Guo, X.; Dou, J.; Lv, Y.; Shen, L.; Yu, Y.; Jin, L. A Study on the Factors Influencing Triglyceride Levels among Adults in Northeast China. Sci. Rep. 2018, 8, 6388. [Google Scholar] [CrossRef] [Green Version]
- Bromage, S.; Batis, C.; Bhupathiraju, S.N.; Fawzi, W.W.; Fung, T.T.; Li, Y.; Deitchler, M.; Angulo, E.; Birk, N.; Castellanos-Gutiérrez, A.; et al. Development and Validation of a Novel Food-Based Global Diet Quality Score (GDQS). J. Nutr. 2021, 151, 75S–92S. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 693) | DD Score < 5 (n = 488) | DD Score ≥ 5 (n = 205) | p Value a |
|---|---|---|---|---|
| Number of participants | 693 (100) | 488 (70.4) | 205 (29.6) | |
| Age, years, n (%) | 0.117 | |||
| 25–44 years | 155 (22.4) | 119 (24.4) | 36 (17.6) | |
| 45–54 years | 256 (36.9) | 179 (36.7) | 77 (37.6) | |
| 55–65 years | 282 (40.7) | 190 (38.9) | 92 (44.9) | |
| Gender, n (%) | 0.151 | |||
| Male | 131 (18.9) | 99 (20.3) | 32 (15.6) | |
| Female | 562 (81.1) | 389 (79.7) | 173 (84.4) | |
| Ethnicity b, n (%) | 0.392 | |||
| Mixed-Ancestry | 281 (40.7) | 193 (39.6) | 88 (43.1) | |
| Black | 410 (59.3) | 294 (60. 4) | 116 (56.9) | |
| Marital status b, n (%) | 0.495 | |||
| Single | 217 (31.5) | 161 (33.2) | 56 (27.5) | |
| Married | 296 (43.0) | 202 (41.6) | 94 (46.1) | |
| Divorced | 72 (10.4) | 53 (10.9) | 19 (9.3) | |
| Widowed | 64 (9.3) | 43 (8.9) | 21 (10.3) | |
| Other c | 40 (5.8) | 26 (5.4) | 14 (6.9) | |
| Education level b, n (%) | 0.038 | |||
| <Grade 12 | 580 (84.2) | 419 (86.0) | 161 (79.7) | |
| ≥Grade 12 | 109 (15.8) | 68 (14.0) | 41 (20.3) | |
| Occupation, n (%) | 0.445 | |||
| Employed | 237 (35.0) | 161 (33.6) | 76 (38.2) | |
| Unemployed d | 296 (43.7) | 216 (45.1) | 80 (40.2) | |
| Pensioner/Disability grant | 145 (21.4) | 102 (21.3) | 43 (21.6) | |
| Type of housing, n (%) | 0.024 | |||
| Built formal unit/privately owned | 244 (35.4) | 157 (32.2) | 87 (42.9) * | |
| Council/core house | 273 (39.6) | 199 (40.9) | 74 (36.5) | |
| Informal shack/shelter/hostel/other | 173 (25.1) | 131 (26.9) | 42 (20.7) | |
| Monthly household income, n (%) | <0.001 | |||
| R0–R3200 | 494 (71.6) | 367 (75.4) | 127 (62.6) * | |
| R3201–R6400 | 117 (17.0) | 77 (15.8) | 40 (19.7) | |
| R6401–R51200 | 79 (11.4) | 43 (8.8) | 36 (17.7) * | |
| Alcohol consumption during last 12 months, n (%) | 0.165 | |||
| ≥5 days per week | 4 (0.6) | 3 (0.6) | 1 (0.5) | |
| 1–4 days per week | 59 (8.5) | 49 (10.0) | 10 (4.9) | |
| Seldom (≤3 days per month) | 187 (27.0) | 131 (26.8) | 56 (27.3) | |
| None | 443 (63.9) | 305 (62.5) | 138 (67.3) | |
| Smoking status, n (%) | 0.391 | |||
| Non-smoker | 519 (74.9) | 361 (74.0) | 158 (77.1) | |
| Smoker | 174 (25.1) | 127 (26.0) | 47 (22.9) |
| Quintile 1 (1–2 Groups) (n = 128) | Quintile 2 (3 Food Groups) (n = 175) | Quintile 3 (4 Food Groups) (n = 185) | Quintile 4 (5 Food Groups) (n = 139) | Quintile 5 (≥ 6 Food Groups) (n = 66) |
|---|---|---|---|---|
| Grains/roots/tubers | Grains/roots/tubers | Grains/roots/tubers | Grains/roots/tubers | Grains/roots/tubers |
| Meat/poultry/fish | Meat/poultry/fish | Meat/poultry/fish | Meat/poultry/fish | Meat/poultry/fish |
| Dairy | Dairy | Dairy | ||
| Other vitamin A-rich fruits and vegetables * | Other vitamin A-rich fruits and vegetables | |||
| Other vegetables | Other vegetables | |||
| Other fruits | ||||
| Eggs |
| Variable | Total (n = 693) | DD Score < 5 (n = 488) | DD Score ≥ 5 (n = 205) | p Value a |
|---|---|---|---|---|
| Gender | ||||
| Male | 131 (18.9) | 99 (20.3) | 32 (15.6) | 0.151 |
| Female | 562 (81.1) | 389 (79.7) | 173 (84.4) | |
| Ethnicity | ||||
| Mixed ancestry | 281 (40.7) | 193 (39.6) | 88 (43.1) | 0.392 |
| Black | 410 (59.3) | 294 (60.4) | 116 (56.9) | |
| BMI | 35.6 (30.5–40.5) | 35.6 (30.6–40.9) | 35.4 (30.4–39.5) | 0.579 |
| Normal weight (18.5–24.9 kg/m2) | 29 (4.2) | 19 (3.9) | 10 (4.9) | 0.827 |
| Overweight (25.0–29.9 kg/m2) | 128 (18.6) | 91 (18.7)) | 37(18.2) | |
| Obese (≥30 kg/m2) | 533 (77.2) | 377 (77.4) | 156 (76.8) | |
| Total | 690 (100) | 487 (100) | 203 (100) | |
| WHR | 0.91 (0.86–0.97) | 0.93 (0.87–0.97) | 0.91 (0.85–0.97) | 0.192 |
| Normal b | 156 (24.7) | 100 (22.5) | 56 (29.8) | 0.053 |
| High c | 476 (75.3) | 344 (77.5) | 132 (70.2) | |
| Total | 681 (100) | 444 (100) | 188 (100) | |
| Glycaemic status | 6.0 (5.0–7.4) | 5.9 (4.9–7.3) | 6.1 (5.1–7.8) | 0.643 |
| Normoglycemia (FPG ≤ 6 and 2-h glucose < 7.8 mmol/L) | 496 (72.9) | 358 (74.7) | 138 (68.7) | 0.211 |
| Prediabetes (FPG 6.1– 7 mmol/L and 2-h glucose ≥ 7.8–11.1 mmol/L) | 114 (16.8) | 77 (16.1) | 37 (18.4) | |
| Diabetes (FPG > 7 mmol/L and 2-h glucose > 11.1 mmol/L) | 70 (10.3) | 44 (9.2) | 26 (12.9) | |
| Total | 680 (100) | 479 (100) | 201 (100) | |
| TC | 4.9 (4.3–5.7) | 4.9 (4.2–5.8) | 5.0 (4.3–5.6) | 0.783 |
| Normal (<5 mmol/L) | 451 (66.2) | 255 (53.1) | 99 (49.3) | 0.356 |
| Elevated (≥5 mmol/L) | 230 (38.0) | 225 (46.9) | 102 (50.7) | |
| Total | 681 (100) | 480 (100) | 201 (100) | |
| HDL-C | 1.2 (1.1–1.4) | 1.2 (1.1–1.4) | 1.2 (1.1–1.4) | 0.645 |
| Normal (≥1.2 mmol/L) | 272 (40.1) | 192 (40.2) | 80 (39.8) | 0.929 |
| Low (<1.2 mmol/L) | 407 (59.9) | 286 (59.8) | 121 (60.2) | |
| Total | 679 (100) | 478 (100) | 201 (100) | |
| LDL-C | 3.1 (2.5–3.8) | 3.1 (2.5–3.8) | 3.1 (2.5–3.7) | 0.856 |
| Normal (<3 mmol/L) | 81 (29.1) | 215 (45.0) | 88 (43.8) | 0.774 |
| Elevated (≥3 mmol/L) | 197 (70.1) | 263 (55.0) | 113 (56.2) | |
| Total | 679 (100) | 478 (100) | 201 (100) | |
| TG | 1.3 (0.9–1.7) | 1.3 (0.9–1.7) | 1.2 (0.9–1.5) | 0.402 |
| Normal (≤1.5 mmol/L) | 451 (66.2) | 307 (64.0) | 144 (71.6) | 0.053 |
| Elevated (>1.5 mmol/L) | 230 (33.8) | 173 (36.0) | 57 (28.4) | |
| Total | 681 (100) | 480 (100) | 201 (100) |
| Variable | Crude Model OR (95% CI) | p Value | Model 1 AOR (95% CI) | p Value | Model 2 AOR (95% CI) | p Value |
|---|---|---|---|---|---|---|
| BMI | ||||||
| Normal weight (18.5–24.9 kg/m2) | 1 | 1 | 1 | |||
| Overweight and obese (≥25.0 kg/m2) | 1.27 (0.58, 2.78) | 0.550 | 1.58 (0.69, 3.62) | 0.280 | 1.24 (0.53, 2.94) | 0.619 |
| WHR | ||||||
| Normal a | 1 | 1 | 1 | |||
| High b | 1.46 (0.99, 2.14) | 0.054 | 1.49 (0.99, 2.21) | 0.052 | 1.45 (0.97, 2.16) | 0.071 |
| Glycaemic status | ||||||
| Normoglycemia (FPG ≤ 6 and 2-h glucose < 7.8 mmol/L) | 1 | 1 | 1 | |||
| Prediabetes (FPG 6.1–7 and2-h glucose ≥ 7.8–11.1 mmol/L) | 0.80 (0.52, 1.24) | 0.325 | 0.80 (0.52, 1.23) | 0.337 | 0.82 (0.52, 1.31) | 0.416 |
| Diabetes (FPG > 7 and 2-h glucose > 11.1 mmol/L) | 0.65 (0.39, 1.10) | 0.109 | 0.63 (0.37, 1.07) | 0.088 | 0.59 (0.34, 1.03) | 0.062 |
| TC | ||||||
| Normal (<5 mmol/L) | 1 | 1 | 1 | |||
| Elevated (≥5 mmol/L) | 0.86 (0.62, 1.19) | 0.357 | 0.87 (0.62, 1.22) | 0.425 | 0.94 (0.66, 1.33) | 0.715 |
| HDL-C | ||||||
| Normal (≥1.2 mmol/L) | 1 | 1 | 1 | |||
| Low (<1.2 mmol/L) | 0.99 (0.70, 1.38) | 0.929 | 1.03 (0.73, 1.44) | 0.882 | 1.09 (0.78, 1.55) | 0.601 |
| LDL-C | ||||||
| Normal (<3 mmol/L) | 1 | 1 | 1 | |||
| Elevated (≥3 mmol/L) | 0.95 (0.68, 1.33) | 0.774 | 0.99 (0.69, 1.39) | 0.937 | 1.06 (0.74, 1.50) | 0.760 |
| TG | ||||||
| Normal (≤1.5 mmol/L) | 1 | 1 | 1 | |||
| Elevated (>1.5 mmol/L) | 1.42 (0.99, 2.04) | 0.054 | 1.45 (1.00, 2.09) | 0.048 | 1.49 (1.03, 2.15) | 0.036 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Madlala, S.S.; Hill, J.; Kunneke, E.; Kengne, A.P.; Peer, N.; Faber, M. Dietary Diversity and its Association with Nutritional Status, Cardiometabolic Risk Factors and Food Choices of Adults at Risk for Type 2 Diabetes Mellitus in Cape Town, South Africa. Nutrients 2022, 14, 3191. https://doi.org/10.3390/nu14153191
Madlala SS, Hill J, Kunneke E, Kengne AP, Peer N, Faber M. Dietary Diversity and its Association with Nutritional Status, Cardiometabolic Risk Factors and Food Choices of Adults at Risk for Type 2 Diabetes Mellitus in Cape Town, South Africa. Nutrients. 2022; 14(15):3191. https://doi.org/10.3390/nu14153191
Chicago/Turabian StyleMadlala, Samukelisiwe S., Jillian Hill, Ernesta Kunneke, Andre P. Kengne, Nasheeta Peer, and Mieke Faber. 2022. "Dietary Diversity and its Association with Nutritional Status, Cardiometabolic Risk Factors and Food Choices of Adults at Risk for Type 2 Diabetes Mellitus in Cape Town, South Africa" Nutrients 14, no. 15: 3191. https://doi.org/10.3390/nu14153191
APA StyleMadlala, S. S., Hill, J., Kunneke, E., Kengne, A. P., Peer, N., & Faber, M. (2022). Dietary Diversity and its Association with Nutritional Status, Cardiometabolic Risk Factors and Food Choices of Adults at Risk for Type 2 Diabetes Mellitus in Cape Town, South Africa. Nutrients, 14(15), 3191. https://doi.org/10.3390/nu14153191