
Long-Term Adherence to a Mediterranean Diet 1-Year after Completion of the MedLey Study

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
2.1. Follow-Up Design
2.2. Outcomes
2.3. Dietary Adherence
2.4. Statistical Analysis
3. Results
3.1. Outcomes of the MedLey Study
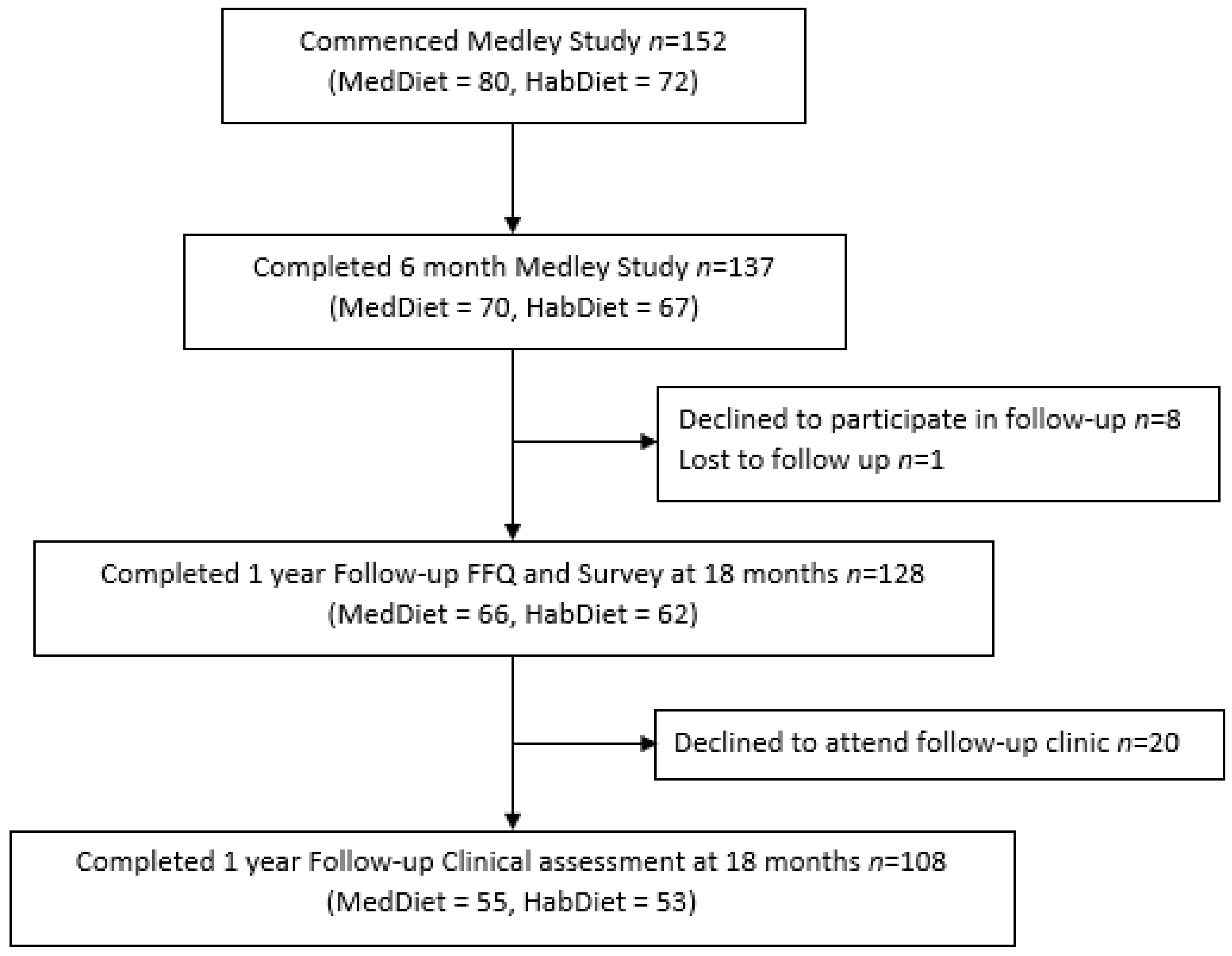
3.2. Follow-Up Population
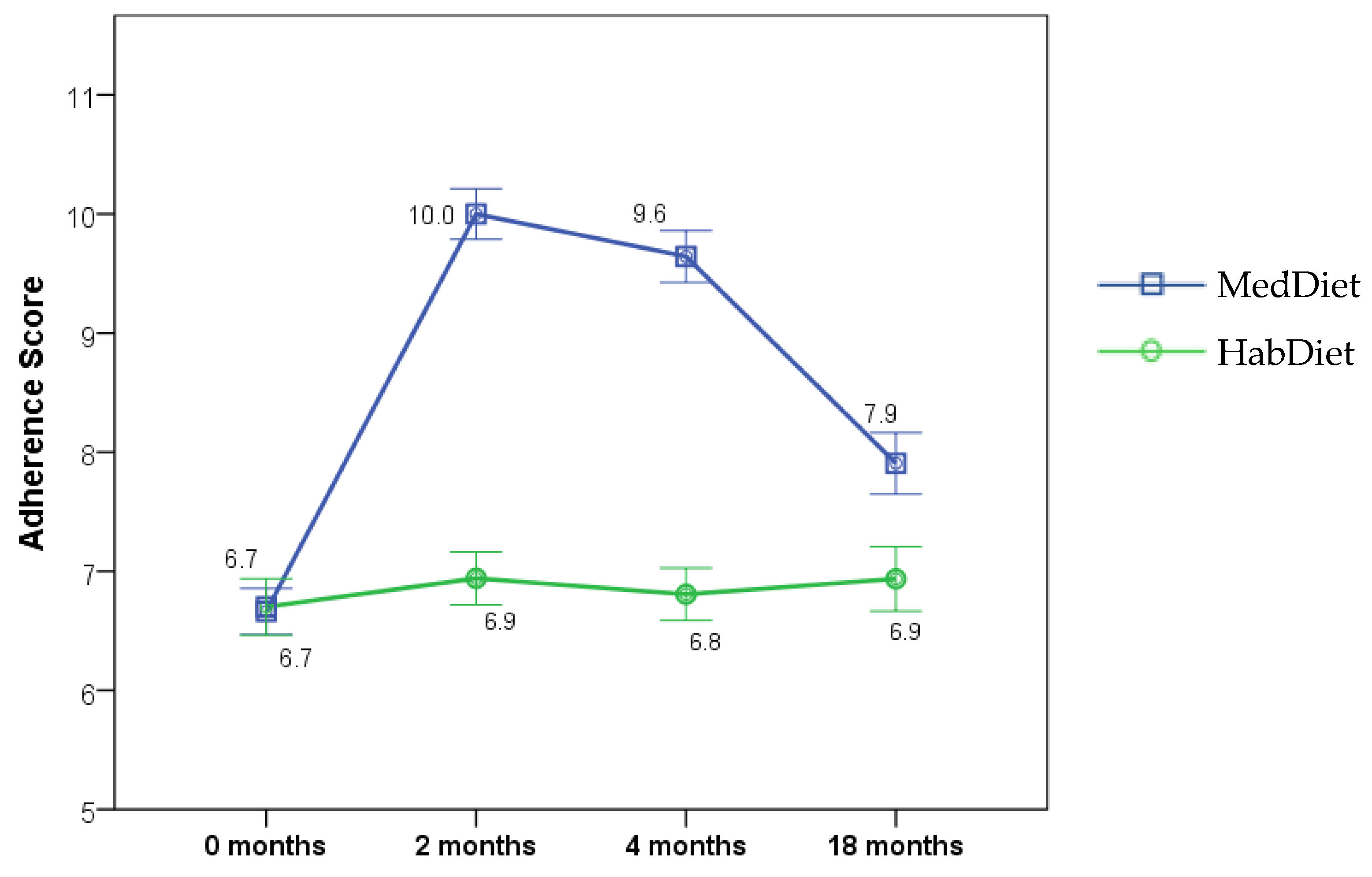
3.3. Mediterranean Diet Adherence
3.4. Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AUSMED | The AUStralian MEDiterranean Diet Heart Trial |
| BMI | body mass index |
| BP | blood pressure |
| FFQ | food frequency questionnaire |
| FMD | flow mediated dilatation |
| HabDiet | habitual diet |
| HELFIMED | Healthy Eating for LiFe with a MEDiterranean-style diet |
| hs-CRP | high-sensitivity C reactive protein |
| MedDairy | A Mediterranean diet supplemented with Dairy foods to improve cardiovascular and cognitive health |
| MedDiet | Mediterranean diet |
| MedLey | Mediterranean Diet for cognitive function and cardiovascular health in the elderly |
| MedPork | Including Pork in the MedDiet for an Australian population |
| TCD | trans cranial doppler |
| WFR | weighed food record |
References
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; a Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [PubMed]
- Radd-Vagenas, S.; Kouris-Blazos, A.; Singh, M.F.; Flood, V. Evolution of Mediterranean diets and cuisine: Concepts and definitions. Asia Pac. J. Clin. Nutr. 2017, 26, 749–763. [Google Scholar] [PubMed]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.; Battino, M.; Balahsen, R.; Miranda, G. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Bousiou, A.; Konstantopoulou, K.; Martimianaki, G.; Peppa, E.; Trichopoulou, A.; Polychronopoulou, A.; Halazonetis, D.J.; Schimmel, M.; Kossioni, A.E. Oral factors and adherence to Mediterranean diet in an older Greek population. Aging Clin. Exp. Res. 2021, 33, 3237–3244. [Google Scholar] [CrossRef]
- Cervo MM, C.; Scott, D.; Seibel, M.J.; Cumming, R.G.; Naganathan, V.; Blyth, F.M.; le Couteur, D.G.; Handelsman, D.J.; Ribeiro, R.V.; Waite, L.M.; et al. Adherence to Mediterranean diet and its associations with circulating cytokines, musculoskeletal health and incident falls in community-dwelling older men: The Concord Health and Ageing in Men Project. Clin. Nutr. 2021, 40, 5753–5763. [Google Scholar] [CrossRef] [PubMed]
- Antoniazzi, L.; Arroyo-Olivares, R.; Bittencourt, M.S.; Tada, M.T.; Lima, I.; Jannes, C.E.; Krieger, J.E.; Pereira, A.C.; Quintana-Navarro, G.; Muñiz-Grijalvo, O.; et al. Adherence to a Mediterranean diet, dyslipidemia and inflammation in familial hypercholesterolemia. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2014–2022. [Google Scholar] [CrossRef]
- Coelho-Junior, H.J.; Trichopoulou, A.; Panza, F. Cross-sectional and longitudinal associations between adherence to Mediterranean diet with physical performance and cognitive function in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2021, 70, 101395. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 4364.0.55.008—Australian Health Survey: Usual Nutrient Intakes; Australian Bureau of Statistics: Canberra, Australia, 2015.
- Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/health-pubhlth-strateg-phys-act-guidelines (accessed on 10 January 2022).
- Imamura, F.; Micha, R.; Khatibzadeh, S.; Fahimi, S.; Shi, P.; Powles, J.; Mozaffarian, D.; Global Burden of Disease, Nutrition Chronic Diseases Expert Group. Dietary quality among men and women in 187 countries in 1990 and 2010: A systematic assessment. Lancet Glob. Health 2015, 3, e132–e142. [Google Scholar] [CrossRef] [Green Version]
- Itsiopoulos, C.; Brazionis, L.; Kaimakamis, M.; Cameron, M.; Best, J.; O’Dea, K.; Rowley, K. Can the Mediterranean diet lower HbA1c in type 2 diabetes? Results from a randomized cross-over study. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Hodgson, J.; Bryan, J.; Garg, M.; Woodman, R.; Murphy, K. Older Australians Can Achieve High Adherence to the Mediterranean Diet during a 6 Month Randomised Intervention; Results from the Medley Study. Nutrients 2017, 9, 534. [Google Scholar] [CrossRef] [Green Version]
- Davis, C.R.; Bryan, J.; Hodgson, J.M.; Woodman, R.; Murphy, K. A Mediterranean Diet Reduces F2-Isoprostanes and Triglycerides among Older Australian Men and Women after 6 Months. J. Nutr. 2017, 147, 1348–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, C.R.; Hodgson, J.M.; Woodman, R.; Bryan, J.; Wilson, C.; Murphy, K.J. A Mediterranean diet lowers blood pressure and improves endothelial function: Results from the MedLey randomized intervention trial. Am. J. Clin. Nutr. 2017, 105, 1305–1313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.; Woodman, R.; Keage, H.; Murphy, K. A Mediterranean Diet with Fresh, Lean Pork Improves Processing Speed and Mood: Cognitive Findings from the MedPork Randomised Controlled Trial. Nutrients 2019, 11, 1521. [Google Scholar] [CrossRef] [Green Version]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.; Woodman, R.; Murphy, K. A Mediterranean diet supplemented with dairy foods improves markers of cardiovascular risk: Results from the MedDairy randomized controlled trial. Am. J. Clin. Nutr. 2018, 108, 1166–1182. [Google Scholar] [CrossRef] [Green Version]
- Opie, R.S.; O’Neil, A.; Jacka, F.N.; Pizzinga, J.; Itsiopoulos, C. A modified Mediterranean dietary intervention for adults with major depression: Dietary protocol and feasibility data from the SMILES trial. Nutr. Neurosci. 2018, 21, 487–501. [Google Scholar] [CrossRef] [Green Version]
- Parletta, N.; Zarnowiecki, D.; Cho, J.; Wilson, A.; Bogomolova, S.; Villani, A.; Itsiopoulos, C.; Niyonsenga, T.; Blunden, S.; Meyer, B.; et al. A Mediterranean-style dietary intervention supplemented with fish oil improves diet quality and mental health in people with depression: A randomized controlled trial (HELFIMED). Nutr. Neurosci. 2019, 22, 474–487. [Google Scholar] [CrossRef] [Green Version]
- Ryan, M.C.; Itsiopoulos, C.; Thodis, T.; Ward, G.; Trost, N.; Hofferberth, S.; O’Dea, K.; Desmond, P.; Johnson, N.; Wilson, A. The Mediterranean diet improves hepatic steatosis and insulin sensitivity in individuals with non-alcoholic fatty liver disease. J. Hepatol. 2013, 59, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Lopez, A.; Bullo, M.; Martinez-Gonzalez, M.A.; Guasch-Ferre, M.; Ros, E.; Basora, J.; Covas, M.; del Carmen Lopez-Sabater, M.; Salas-Salvado, J.; Predimed Reus Study Investigators. Effects of Mediterranean diets on kidney function: A report from the PREDIMED trial. Am. J. Kidney Dis. 2012, 60, 380–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papamichael, M.M.; Katsardis, C.; Lambert, K.; Tsoukalas, D.; Koutsilieris, M.; Erbas, B.; Itsiopoulos, C. Efficacy of a Mediterranean diet supplemented with fatty fish in ameliorating inflammation in paediatric asthma: A randomised controlled trial. J. Hum. Nutr. Diet. 2019, 32, 185–197. [Google Scholar] [CrossRef] [PubMed]
- Knight, A.; Bryan, J.; Wilson, C.; Hodgson, J.; Murphy, K. A randomised controlled intervention trial evaluating the efficacy of a Mediterranean dietary pattern on cognitive function and psychological wellbeing in healthy older adults: The MedLey study. BMC Geriatr. 2015, 15, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, C.R.; Bryan, J.; Hodgson, J.M.; Wilson, C.; Dhillon, V.; Murphy, K.J. A randomised controlled intervention trial evaluating the efficacy of an Australianised Mediterranean diet compared to the habitual Australian diet on cognitive function, psychological wellbeing and cardiovascular health in healthy older adults (MedLey study): Protocol paper. BMC Nutr. 2015, 1, 35. [Google Scholar]
- Knight, A.; Bryan, J.; Wilson, C.; Hodgson, J.; Davis, C.; Murphy, K. The Mediterranean Diet and Cognitive Function among Healthy Older Adults in a 6-Month Randomised Controlled Trial: The MedLey Study. Nutrients 2016, 8, 579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xinying, P.X.; Noakes, M.; Keogh, J. Can a food frequency questionnaire be used to capture dietary intake data in a 4 week clinical intervention trial? Asia Pac. J. Clin. Nutr. 2004, 13, 318–323. [Google Scholar]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichoopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.; Casini, A. Adherence to Mediterranean diet and health status: Meta-analysis. BMJ 2008, 337, a1344. [Google Scholar] [CrossRef] [Green Version]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef] [Green Version]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.J.; Keage, H.A.; Murphy, K.J. A Mediterranean Diet to Improve Cardiovascular and Cognitive Health: Protocol for a Randomised Controlled Intervention Study. Nutrients 2017, 9, 145. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, E.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Salas-Salvadó, J.; Estruch, R.; Corella, D.; Fito, M.; Ros, E.; Predimed Investigators. Benefits of the Mediterranean Diet: Insights from the PREDIMED Study. Prog. Cardiovasc. Dis. 2015, 58, 50–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Villegas, A.; Cabrera-Suárez, B.; Molero, P.; Gonzalez-Pinto, A.; Chiclana-Actis, C.; Cabrera, C.; Lahortiga-Ramos, F.; Florido-Rodriguez, M.; Vega-Perez, P.; Vega-Perez, R. Preventing the recurrence of depression with a Mediterranean diet supplemented with extra-virgin olive oil. The PREDI-DEP trial: Study protocol. BMC Psychiatry 2019, 19, 63. [Google Scholar] [CrossRef] [PubMed]
- Mayr, H.L.; Tierney, A.C.; Kucianski, T.; Thomas, C.; Itsiopoulos, C. Australian patients with coronary heart disease achieve high adherence to 6-month Mediterranean diet intervention: Preliminary results of the AUSMED Heart Trial. Nutrition 2019, 61, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Rees, C.; Mullumby, J. Trends in Australian meat consumption. Agric. Commod. 2017, 7, 82–85. [Google Scholar]
- Australian Bureau of Statistics. National Health Survey: First Results, 2014–2015 4364.0.55.001. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/health-pubhlth-strateg-phys-act-guidelines (accessed on 15 January 2022).
- Middleton, G.; Keegan, R.; Smith, M.F.; Alkhatib, A.; Klonizakis, M. Implementing a Mediterranean diet intervention into a RCT: Lessons learned from a non-Mediterranean based country. J. Nutr. Health Aging 2015, 19, 1019–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maher, C.A.; Davis, C.R.; Curtis, R.G.; Short, C.; Murphy, K. A Physical Activity and Diet Program Delivered by Artificially Intelligent Virtual Health Coach: Proof-of-Concept Study. JMIR Mhealth Uhealth 2020, 8, e17558. [Google Scholar] [CrossRef] [PubMed]
- Benajiba, N.; Dodge, E.; Khaled, M.B.; Chavarria, E.; Sammartino, C.; Aboul-Enein, B. Technology-based nutrition interventions using the Mediterranean diet: A systematic review. Nutr. Rev. 2021, 80, nuab076. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| MedDiet | Diet × Visit Interaction | Diet | Visit | ||||||||||
| 0-Month | 2-Month | 4-Month | 18-Month | Change 0–18 Month | Change 4–18 Month | ||||||||
| (n = 77) | (n = 70) | (n = 70) | (n = 64) | Mean Change | p-Value | 95% CI | Mean Change | p-Value | 95% CI | p-Value | p-Value | p-Value | |
| 15 pt MDAS | 6.7 ± 0.2 | 10.0 ± 0.2 | 9.6 ± 0.2 | 7.9 ± 0.3 | 1.3 ± 0.3 | <0.0001 | 0.6, 2.0 | −1.7 ± 0.3 | 0.000 | −2.4, −1.0 | <0.0001 | <0.0001 | <0.0001 |
| 9 pt MDAS | 7.8 ± 0.3 | 10.9 ± 0.2 | 10.3 ± 0.2 | 9.2 ± 0.3 | 1.3 ± 0.2 | <0.0001 | 0.7, 2.0 | −1.1 ± 0.3 | 0.000 | −1.8, −0.5 | <0.0001 | <0.0001 | <0.0001 |
| HabDiet | |||||||||||||
| 0-Month | 2-Month | 4-Month | 18-Month | Change 0–18 Month | Change 4–18 Month | ||||||||
| (n = 70) | (n = 67) | (n = 67) | (n = 62) | Mean Change | p-Value | 95% CI | Mean Change | p-Value | 95% CI | ||||
| 15 pt MDAS | 6.7 ± 0.2 | 6.9 ± 0.2 | 6.8 ± 0.2 | 6.9 ± 0.3 | 0.2 ± 0.3 | 1.000 | −0.5, 0.9 | 0.2 ± 0.3 | 1.000 | −0.5, 0.8 | |||
| 9 pt MDAS | 8.1 ± 0.3 | 7.9 ± 0.3 | 7.9 ± 0.3 | 8.0 ± 0.3 | −0.1 ± 0.2 | 1.000 | −0.8, 0.6 | 0.2 ± 0.3 | 1.000 | −0.5, 0.8 | |||
| MedDiet | Diet × Visit Interaction | Diet | Visit | ||||||||||
| 0-Month | 3-Month | 6-Month | 18-Month | Change 0–18 Month | Change 6–18 Month | ||||||||
| (n = 79) | (n = 73) | (n = 70) | (n = 55) | Mean Change | p-Value | 95% CI | Mean Change | p-Value | 95% CI | p-Value | p-Value | p-Value | |
| SBP (mm/Hg) ** | 123 ± 1 | 119 ± 1 | 117 ± 1 | 121 ± 2 | −2 ± 1 | 0.219 | −5.1, 0.6 | 4 ± 1 | 0.000 | 1.8, 6.4 | 0.040 | 0.324 | 0.000 |
| Morning SBP (mm/Hg) | 124 ± 2 | 120 ± 2 | 118 ± 2 | 123 ± 2 | −1 ± 1 | 1.000 | −3.9, 2.0 | 5 ± 1 | 0.000 | 2.4, 8.0 | 0.032 | 0.360 | 0.000 |
| Afternoon SBP (mm/Hg) | 122 ± 1 | 117 ± 1 | 116 ± 1 | 119 ± 2 | −3 ± 1 | 0.094 | −6.4, 0.3 | 3 ± 1 | 0.052 | −0.01, 5.6 | 0.093 | 0.165 | 0.000 |
| Evening SBP (mm/Hg) | 123 ± 2 | 119 ± 2 | 117 ± 2 | 120 ± 2 | −3 ± 1 | 0.136 | −6.4, 0.5 | 4 ± 1 | 0.003 | 1.0, 6.8 | 0.586 | 0.554 | 0.000 |
| DBP (mm/Hg) ** | 70 ± 1 | 68 ± 1 | 68 ± 1 | 68 ± 1 | −1 ± 1 | 0.326 | −2.5, 0.4 | 1 ± 0 | 0.391 | −0.4, 2.2 | 0.433 | 0.043 | 0.000 |
| Morning DBP (mm/Hg) | 71 ± 1 | 70 ± 1 | 70 ± 1 | 71 ± 1 | 0 ± 1 | 1.000 | −1.4, 1.7 | 2 ± 1 | 0.023 | 0.2, 3.2 | 0.376 | 0.134 | 0.000 |
| Afternoon DBP (mm/Hg) | 68 ± 1 | 67 ± 1 | 66 ± 1 | 67 ± 1 | −1 ± 1 | 0.542 | −3.1, 0.7 | 1 ± 1 | 1.000 | −1.0, 2.3 | 0.131 | 0.011 | 0.000 |
| Evening DBP (mm/Hg) | 69 ± 1 | 68 ± 1 | 66 ± 1 | 67 ± 1 | −2 ± 1 | 0.031 | −4.0, −0.1 | 1 ± 1 | 1.000 | −1.2, 2.4 | 0.989 | 0.075 | 0.000 |
| BMI (kg/m2) | 26.8 ± 0.4 | 26.2 ± 0.4 | 26.2 ± 0.4 | 26.1 ± 0.5 | −0.2 ± 0.1 | 1.000 | −0.5, 0.2 | 0.1 ± 0.1 | 1.000 | −0.2, 0.3 | 0.049 | 0.498 | 0.000 |
| Weight (kg) | 74.0 ± 1.5 | 72.8 ± 1.5 | 72.6 ± 1.6 | 72. 9 ± 1.8 | −0.4 ± 0.3 | 1.000 | −1.3, 0.5 | 0.2 ± 0.3 | 1.000 | −0.6, 0.9 | 0.019 | 0.387 | 0.002 |
| Total cholesterol (mmol/L) | 5.14 ± 0.10 | 4.92 ± 0.10 | 4.96 ± 0.11 | 4.84 ± 0.12 | −0.2 ± 0.1 | 0.194 | −0.4, 0.4 | −0.0 ± 0.1 | 1.000 | −0.3, 0.2 | 0.256 | 0.192 | 0.000 |
| LDL (mmol/L) | 2.92 ± 0.08 | 2.81 ± 0.08 | 2.83 ± 0.09 | 2.74 ± 0.10 | −0.1 ± 0.1 | 1.000 | −0.3, 0.1 | −0.1 ± 0.1 | 1.000 | −0.2, 0.1 | 0.942 | 0.105 | 0.126 |
| HDL cholesterol (mmol/L) | 1.63 ± 0.05 | 1.53 ± 0.05 | 1.58 ± 0.06 | 1.59 ± 0.06 | 1.0 ± 1.0 * | 0.767 | 0.9, 1.0 | 1.0 ± 1.0 * | 1.000 | 1.0, 1.1 | 0.046 | 0.741 | 0.000 |
| Triglycerides (mmol/L) | 1.19 ± 0.05 | 1.11 ± 0.06 | 1.04 ± 0.05 | 1.12 ± 0.07 | 1.0 ± 1.0 * | 1.000 | 0.9, 1.1 | 1.1 ± 1.0 * | 0.131 | 1.0, 1.2 | 0.020 | 0.508 | 0.001 |
| Total cholesterol:HDL ratio | 3.34 ± 0.10 | 3.42 ± 0.11 | 3.35 ± 0.12 | 3.20 ± 0.11 | 1.0 ± 1.0 * | 1.000 | 0.9, 1.0 | 1.0 ± 1.0 * | 0.619 | 0.9, 1.0 | 0.474 | 0.553 | 0.231 |
| CRP (mg/L) | 2.09 ± 0.29 | 1.43 ± 0.20 | 1.54 ± 0.25 | 1.44 ± 0.26 | 0.8 ± 1.1 * | 0.170 | 0.6, 1.1 | 0.9 ± 1.1 * | 1.000 | 0.7, 1.2 | 0.297 | 0.842 | 0.388 |
| HabDiet | |||||||||||||
| 0-Month | 3-Month | 6-Month | 18-Month | Change 0–18 Month | Change 6–18 Month | ||||||||
| (n = 70) | (n = 68) | (n = 67) | (n = 53) | Mean Change | p-Value | 95% CI | Mean Change | p-Value | 95% CI | ||||
| SBP (mm/Hg) ** | 125 ± 2 | 122 ± 2 | 120 ± 2 | 120 ± 2 | −4 ± 1 | 0.001 | −7.1, −1.3 | 1 ± 1 | 1.000 | −1.5, 3.2 | |||
| Morning SBP (mm/Hg) | 126 ± 2 | 123 ± 2 | 121 ± 2 | 122 ± 2 | −3 ± 1 | 0.040 | −6.2, −0.1 | 1 ± 1 | 1.000 | −2.0, 3.7 | |||
| Afternoon SBP (mm/Hg) | 124 ± 2 | 121 ± 1 | 119 ± 1 | 119 ± 2 | −5 ± 1 | 0.001 | −8.5, −1.6 | 0 ± 1 | 1.000 | −2.8, 2.9 | |||
| Evening SBP (mm/Hg) | 125 ± 2 | 121 ± 2 | 118 ± 2 | 120 ± 2 | −5 ± 1 | 0.004 | −8.2, −1.1 | 2 ± 1 | 0.591 | −1.1, 4.8 | |||
| DBP (mm/Hg) ** | 72 ± 1 | 71 ± 1 | 70 ± 1 | 70 ± 1 | −2 ± 1 | 0.008 | −3.3, 0.3 | 0 ± 0 | 1.000 | −1.2, 1.5 | |||
| Morning DBP (mm/Hg) | 74 ± 1 | 73 ± 1 | 72 ± 1 | 72 ± 1 | −1 ± 1 | 0.544 | −2.7, 0.6 | 1 ± 1 | 1.000 | 0.8, 2.3 | |||
| Afternoon DBP (mm/Hg) | 71 ± 1 | 71 ± 1 | 70 ± 1 | 68 ± 1 | −2 ± 1 | 0.007 | −4.4, −0.5 | 0 ± 1 | 1.000 | −2.1, 1.2 | |||
| Evening DBP (mm/Hg) | 71 ± 1 | 70 ± 1 | 69 ± 1 | 69 ± 1 | −2 ± 1 | 0.025 | −4.2, −0.2 | 0 ± 1 | 1.000 | −1.6, 2.2 | |||
| BMI (kg/m2) | 27.1 ± 0.5 | 26.9 ± 0.5 | 26.7 ± 0.5 | 26.9 ± 0.6 | −0.1 ± 0.1 | 1.000 | −0.5, 0.2 | 0.1 ± 0.1 | 1.000 | −0.2, 0.4 | |||
| Weight (kg) | 75.4 ± 1.6 | 75.2 ± 1.6 | 75.0 ± 1.6 | 75.7 ± 1.9 | −0.4 ± 0.3 | 1.000 | −1.3, 0.5 | 0.1 ± 0.3 | 1.000 | −0.6, 0.9 | |||
| Total cholesterol (mmol/L) | 5.29 ± 0.10 | 5.22 ± 0.09 | 5.14 ± 0.10 | 5.02 ± 0.11 | −0.2 ± 0.1 | 0.167 | −0.4, 0.4 | −0.0 ± 0.1 | 1.000 | −0.3, 0.2 | |||
| LDL (mmol/L) | 3.11 ± 0.09 | 3.06 ± 0.08 | 3.06 ± 0.09 | 2.92 ± 0.08 | −0.1 ± 0.1 | 0.428 | −0.3, 0.1 | −0.1 ± 0.1 | 0.684 | −0.3, 0.1 | |||
| HDL cholesterol (mmol/L) | 1.63 ± 0.05 | 1.60 ± 0.05 | 1.57 ± 0.04 | 1.53 ± 0.06 | 1.0 ± 1.0 * | 0.036 | 0.9, 1.0 | 1.0 ± 1.0 * | 1.000 | 1.0, 1.0 | |||
| Triglycerides (mmol/L) | 1.18 ± 0.07 | 1.21 ± 0.07 | 1.11 ± 0.06 | 1.24 ± 0.07 | 1.1 ± 1.0 * | 0.458 | 1.0, 1.2 | 1.1 ± 1.0 * | 0.032 | 1.0, 1.2 | |||
| Total cholesterol:HDL ratio | 3.41 ± 0.10 | 3.42 ± 0.10 | 3.40 ± 0.10 | 3.44 ± 0.11 | 1.0 ± 1.0 * | 1.000 | 1.0, 1.1 | 1.0 ± 1.0 * | 1.000 | 1.0, 1.1 | |||
| CRP (mg/L) | 1.90 ± 0.31 | 1.85 ± 0.26 | 1.92 ± 0.30 | 1.69 ± 0.30 | 1.0 ± 1.1 * | 1.000 | 0.7, 1.3 | 1.0 ± 1.1 * | 1.000 | 0.7, 1.4 | |||
| MedDiet | Diet × Visit Interaction | Diet | Visit | ||||||||||
| 0-Month | 2-Month | 4-Month | 18-Month | Change 0–18 Month | Change 4–18 Month | ||||||||
| (n = 77) | (n = 70) | (n = 70) | (n = 64) | Mean Change | p-Value | 95% CI | Mean Change | p-Value | 95% CI | p-Value | p-Value | p-Value | |
| Energy (kJ/day) | 8766 ± 264 | 8489 ± 267 | 8020 ± 248 | 8048 ± 287 | −645 ± 283 | 0.145 | −1403, 112 | 118 ± 247 | 1.000 | −543, 778 | 0.350 | 0.696 | 0.000 |
| Protein (en%) | 17.3 ± 0.3 | 17.1 ± 0.4 | 17.6 ± 0.4 | 17.5 ± 0.5 | |||||||||
| Fat (en%) | 40.0 ± 0.6 | 41.8 ± 0.9 | 41.9 ± 1.0 | 43.0 ± 1.0 | |||||||||
| SatFat (en%) | 13.3 ± 0.3 | 10.7 ± 0.2 | 10.8 ± 0.2 | 12.5 ± 0.3 | |||||||||
| PolyFat (en%) | 6.6 ± 0.2 | 6.8 ± 0.2 | 6.7 ± 0.2 | 6.4 ± 0.2 | |||||||||
| MonoFat (en%) | 17.0 ± 0.5 | 21.2 ± 0.7 | 21.3 ± 0.8 | 20.9 ± 0.8 | |||||||||
| CHO (en%) | 39.1 ± 0.7 | 36.8 ± 0.8 | 36.3 ± 0.8 | 35.5 ± 0.9 | |||||||||
| Alcohol (en%) | 4.3 ± 0.5 | 4.5 ± 0.5 | 4.6 ± 0.5 | 4.5 ± 0.7 | |||||||||
| Protein (g/MJ/day) | 10.2 ± 0.2 | 10.1 ± 0.2 | 10.3 ± 0.2 | 10.3 ± 0.3 | 0.2 ± 0.2 | 1.000 | −0.4, 0.8 | −0.1 ± 0.2 | 1.000 | −0.7, 0.5 | 0.545 | 0.745 | 0.743 |
| Fat (g/MJ/day) | 10.8 ± 0.2 | 11.3 ± 0.3 | 11.3 ± 0.3 | 11.6 ± 0.3 | 0.8 ± 0.2 | 0.008 | 0.1, 1.4 | 0.2 ± 0.2 | 1.000 | −0.3, 0.8 | 0.320 | 0.414 | 0.027 |
| SatFat (g/MJ/day) | 3.6 ± 0.1 | 2.9 ± 0.1 | 2.9 ± 0.1 | 3.4 ± 0.1 | −0.2 ± 0.1 | 0.025 | −0.5, −0.0 | 0.4 ± 0.1 | 0.000 | 0.3, 0.6 | 0.000 | 0.000 | 0.0000 |
| PolyFat (g/MJ/day) | 1.8 ± 0.1 | 1.8 ± 0.1 | 1.8 ± 0.1 | 1.7 ± 0.1 | −0.0 ± 0.1 | 1.000 | −0.2, 0.1 | −0.1 ± 0.1 | 0.554 | −0.2, 0.1 | 0.402 | 0.020 | 0.338 |
| MonoFat (g/MJ/day) | 4.6 ± 0.1 | 5.7 ± 0.2 | 5.8 ± 0.2 | 5.6 ± 0.2 | 1.0 ± 0.2 | 0.000 | 0.6, 1.5 | −0.1 ± 0.2 | 1.000 | −0.5, 0.3 | 0.000 | 0.005 | 0.000 |
| CHO (g/MJ/day) | 23.0 ± 0.4 | 21.7 ± 0.5 | 21.3 ± 0.5 | 20.9 ± 0.5 | −1.9 ± 0.4 | 0.000 | −3.0, −0.9 | −0.4 ± 0.4 | 1.000 | −1.3, 0.6 | 0.207 | 0.435 | 0.000 |
| Sugars (g/MJ/day) | 11.3 ± 0.3 | 10.6 ± 0.3 | 10.8 ± 0.3 | 10.9 ± 0.4 | −0.3 ± 0.3 | 1.000 | −1.0, 0.4 | 0.2 ± 0.3 | 1.000 | −0.5, 0.9 | 0.716 | 0.926 | 0.049 |
| Alcohol (g/MJ/day) | 1.5 ± 0.2 | 1.6 ± 0.2 | 1.6 ± 0.2 | 1.5 ± 0.2 | 0.1 ± 0.2 | 1.000 | −0.4, 0.5 | −0.0 ± 0.1 | 1.000 | −0.4, 0.3 | 0.504 | 0.716 | 0.259 |
| Fibre (g/MJ/day) | 2.8 ± 0.1 | 3.2 ± 0.1 | 3.0 ± 0.1 | 2.8 ± 0.1 | 0.0 ± 0.1 | 1.000 | −0.1, 0.2 | −0.2 ± 0.1 | 0.033 | −0.4, −0.0 | 0.004 | 0.053 | 0.001 |
| HabDiet | |||||||||||||
| 0-Month | 2-Month | 4-Month | 18-Month | Change 0–18 Month | Change 4–18 Month | ||||||||
| (n = 70) | (n = 67) | (n = 67) | (n = 62) | Mean Change | p-Value | 95% CI | Mean Change | p-Value | 95% CI | ||||
| Energy (kJ/day) | 9091 ± 327 | 8399 ± 301 | 8321 ± 296 | 7988 ± 340 | −1087 ± 289 | 0.002 | −1861, −313 | −311 ± 251 | 1.000 | −983, 362 | |||
| Protein (en%) | 17.2 ± 0.3 | 17.4 ± 0.3 | 17.3 ± 0.3 | 17.1 ± 0.3 | |||||||||
| Fat (en%) | 40.6 ± 0.7 | 41.1 ± 0.9 | 40.3 ± 0.9 | 41.2 ± 0.7 | |||||||||
| SatFat (en%) | 13.8 ± 0.3 | 13.7 ± 0.3 | 13.6 ± 0.3 | 13.8 ± 0.4 | |||||||||
| PolyFat (en%) | 6.2 ± 0.2 | 6.3 ± 0.3 | 6.0 ± 0.2 | 6.0 ± 0.2 | |||||||||
| MonoFat (en%) | 17.5 ± 0.5 | 17.9 ± 0.7 | 17.7 ± 0.7 | 18.2 ± 0.6 | |||||||||
| CHO (en%) | 38.6 ± 0.8 | 37.6 ± 0.8 | 38.0 ± 0.8 | 36.7 ± 0.8 | |||||||||
| Alcohol (en%) | 4.1 ± 0.5 | 4.4 ± 0.7 | 4.9 ± 0.8 | 5.5 ± 0.9 | |||||||||
| Protein (g/MJ/day) | 10.1 ± 0.2 | 10.3 ± 0.2 | 10.2 ± 0.2 | 10.1 ± 0.2 | −0.1 ± 0.2 | 1.000 | −0.7, 0.5 | −0.2 ± 0.2 | 1.000 | −0.8, 0.5 | |||
| Fat (g/MJ/day) | 11.0 ± 0.2 | 11.1 ± 0.2 | 10.9 ± 0.2 | 11.1 ± 0.2 | 0.2 ± 0.2 | 1.000 | −0.4, 0.9 | 0.3 ± 0.2 | 1.000 | −0.3, 0.8 | |||
| SatFat (g/MJ/day) | 3.7 ± 0.1 | 3.7 ± 0.1 | 3.7 ± 0.1 | 3.7 ± 0.1 | 0.0 ± 0.1 | 1.000 | −0.2, 0.3 | 0.1 ± 0.1 | 1.000 | −0.1, 0.3 | |||
| PolyFat (g/MJ/day) | 1.7 ± 0.1 | 1.7 ± 0.1 | 1.6 ± 0.1 | 1.6 ± 0.1 | −0.1 ± 0.1 | 1.000 | −0.2, 0.1 | 0.0 ± 0.1 | 1.000 | −0.1, 0.2 | |||
| MonoFat (g/MJ/day) | 4.7 ± 0.1 | 4.9 ± 0.2 | 4.8 ± 0.2 | 4.9 ± 0.2 | 0.2 ± 0.2 | 1.000 | −0.3, 0.7 | 0.2 ± 0.2 | 1.000 | −0.3, 0.6 | |||
| CHO (g/MJ/day) | 22.7 ± 0.4 | 22.1 ± 0.5 | 22.4 ± 0.5 | 21.6 ± 0.5 | −1.2 ± 0.4 | 0.023 | −2.3, −0.1 | −0.8 ± 0.4 | 0.169 | −1.8, 0.2 | |||
| Sugars (g/MJ/day) | 11.2 ± 0.4 | 10.7 ± 0.4 | 11.0 ± 0.4 | 10.7 ± 0.4 | −0.5 ± 0.3 | 0.685 | −1.2, 0.3 | −0.2 ± 0.3 | 1.000 | −0.9, 0.5 | |||
| Alcohol (g/MJ/day) | 1.4 ± 0.2 | 1.5 ± 0.2 | 1.7 ± 0.3 | 1.9 ± 0.3 | 0.4 ± 0.2 | 0.105 | −0.0, 0.8 | 0.2 ± 0.1 | 1.000 | −0.2, 0.5 | |||
| Fibre (g/MJ/day) | 2.8 ± 0.1 | 2.8 ± 0.1 | 2.8 ± 0.1 | 2.8 ± 0.1 | −0.0 ± 0.1 | 1.000 | −0.2, 0.2 | −0.0 ± 0.1 | 1.000 | −0.2, 0.2 | |||
| MedDiet | Diet × Visit Interaction | Diet | Visit | ||||||||||
| 0-Month | 2-Month | 4-Month | 18-Month | Change 0–18 Month | Change 4–18 Month | ||||||||
| (n = 77) | (n = 70) | (n = 70) | (n = 64) | Mean Change | p-Value | 95% CI | Mean Change | p-Value | 95% CI | p-Value | p-Value | p-Value | |
| Dietary Energy (MJ/day) | 8.8 ± 0.3 | 8.5 ± 0.3 | 8.0 ± 0.2 | 8.0 ± 0.3 | −0.6 ± 0.3 | 0.148 | −1.4, 0.1 | 0.1 ± 0.2 | 1.000 | −0.5, 0.8 | 0.350 | 0.696 | 0.000 |
| Olive Oil | 2.3 ± 0.2 | 4.5 ± 0.4 | 4.5 ± 0.4 | 4.1 ± 0.4 | 1.7 ± 0.3 | 0.000 | 1.0, 2.4 | −0.5 ± 0.3 | 0.438 | −1.2, 0.2 | 0.000 | 0.001 | 0.000 |
| Legumes | 1.6 ± 0.2 | 3.9 ± 0.3 | 3.5 ± 0.2 | 2.4 ± 0.3 | 0.8 ± 0.2 | 0.006 | 0.2, 1.4 | −1.1 ± 0.2 | 0.000 | −1.6, −0.5 | 0.000 | 0.000 | 0.000 |
| Fish | 5.6 ± 0.5 | 8.7 ± 0.5 | 9.4 ± 0.6 | 8.3 ± 0.9 | 2.7 ± 0.7 | 0.001 | 0.8, 4.6 | −1.1 ± 0.7 | 0.820 | −3.0, 0.8 | 0.000 | 0.000 | 0.000 |
| Meats | 8.8 ± 0.5 | 6.3 ± 0.3 | 6.4 ± 0.4 | 7.7 ± 0.5 | −1.0 ± 0.6 | 0.387 | −2.5, 0.5 | 1.3 ± 0.5 | 0.59 | −0.0, 2.5 | 0.005 | 0.035 | 0.000 |
| Fruits | 32.5 ± 1.9 | 39.2 ± 1.4 | 38.5 ± 1.5 | 37.3 ± 2.3 | 4.4 ± 1.8 | 0.104 | −0.5, 9.2 | −1.6 ± 1.8 | 1.000 | −6.2, 3.1 | 0.048 | 0.149 | 0.003 |
| Vegetables | 15.3 ± 0.8 | 20.0 ± 0.9 | 19.9 ± 0.8 | 18.0 ± 0.8 | 2.3 ± 0.7 | 0.009 | 0.4, 4.3 | −1.9 ± 0.7 | 0.032 | −3.7, −0.1 | 0.001 | 0.030 | 0.000 |
| Potatoes | 4.2 ± 0.4 | 2.4 ± 0.3 | 2.1 ± 0.3 | 3.1 ± 0.3 | −1.2 ± 0.4 | 0.059 | −2.3, 0.0 | 1.0 ± 0.4 | 0.074 | −0.1, 2.1 | 0.001 | 0.015 | 0.000 |
| Dairy | 45.9 ± 2.4 | 48.0 ± 2.2 | 50.7 ± 2.3 | 50.3 ± 3.0 | 4.6 ± 2.6 | 0.454 | −2.3, 11.5 | −0.2 ± 2.7 | 1.000 | −7.5, 7.0 | 0.672 | 0.220 | 0.219 |
| Breads | 8.1 ± 0.5 | 10.9 ± 0.6 | 10.5 ± 0.6 | 7.5 ± 0.6 | −0.4 ± 0.5 | 1.000 | −1.6, 0.8 | −3.0 ± 0.5 | 0.000 | −4.4, −1.6 | 0.000 | 0.050 | 0.000 |
| Cereals | 18.5 ± 1.2 | 18.3 ± 1.4 | 15.7 ± 1.4 | 16.6 ± 1.3 | −1.3 ± 1.1 | 1.000 | −4.3, 1.6 | 1.2 ± 1.1 | 1.000 | −1.7, 4.0 | 0.089 | 0.397 | 0.116 |
| Red Wine | 9.1 ± 1.5 | 14.4 ± 1.8 | 14.0 ± 1.6 | 10.5 ± 1.9 | 1.4 ± 1.4 | 1.000 | −2.4, 5.2 | −3.0 ± 1.2 | 0.063 | −6.2, 0.1 | 0.007 | 0.299 | 0.007 |
| Eggs | 2.8 ± 0.2 | 2.6 ± 0.2 | 2.8 ± 0.2 | 3.0 ± 0.2 | 0.2 ± 0.2 | 1.000 | −0.4, 0.8 | 0.2 ± 0.2 | 1.000 | −0.5, 0.8 | 0.259 | 0.680 | 0.117 |
| Sugars | 1.4 ± 0.1 | 1.1 ± 0.2 | 1.2 ± 0.2 | 1.1 ± 0.2 | −0.1 ± 0.1 | 0.898 | −0.4, 0.1 | −0.0 ± 0.1 | 1.000 | −0.3, 0.3 | 0.597 | 0.369 | 0.012 |
| Nuts | 1.5 ± 0.1 | 1.9 ± 0.1 | 1.8 ± 0.1 | 1.8 ± 0.1 | 0.3 ± 0.2 | 0.508 | −0.2, 0.8 | −0.0 ± 0.1 | 1.000 | −0.4, 0.3 | 0.029 | 0.087 | 0.718 |
| Other Alcohol | 7.4 ± 1.2 | 2.8 ± 0.7 | 3.6 ± 0.8 | 7.7 ± 1.7 | −0.2 ± 1.5 | 1.000 | −4.3, 3.9 | 3.8 ± 1.4 | 0.036 | 0.2, 7.5 | 0.004 | 0.014 | 0.008 |
| Discretionary Foods | 24.0 ± 1.4 | 10.4 ± 0.9 | 11.7 ± 1.1 | 18.9 ± 1.8 | −5.3 ± 1.8 | 0.021 | −10.0, −0.5 | 6.9 ± 1.6 | 0.000 | 2.7, 11.1 | 0.000 | 0.000 | 0.000 |
| HabDiet | |||||||||||||
| 0-Month | 2-Month | 4-Month | 18-Month | Change 0–18 Month | Change 4–18 Month | ||||||||
| (n = 70) | (n = 67) | (n = 67) | (n = 62) | Mean Change | p-Value | 95% CI | Mean Change | p-Value | 95% CI | ||||
| Dietary Energy (MJ/day) | 9.1 ± 0.3 | 8.4 ± 0.3 | 8.3 ± 0.3 | 8.0 ± 0.3 | −1.1 ± 0.3 | 0.002 | −1.9, −0.3 | −0.3 ± 0.3 | 1.000 | −1.0, 0.4 | |||
| Olive Oil | 2.3 ± 0.2 | 2.7 ± 0.3 | 2.5 ± 0.3 | 2.7 ± 0.2 | 0.4 ± 0.3 | 0.937 | −0.4, 1.2 | 0.3 ± 0.3 | 1.000 | −0.5, 1.0 | |||
| Legumes | 1.0 ± 0.1 | 1.2 ± 0.1 | 1.2 ± 0.1 | 1.2 ± 0.1 | 0.2 ± 0.2 | 1.000 | −0.5, 0.8 | −0.0 ± 0.2 | 1.000 | −0.6, 0.6 | |||
| Fish | 5.5 ± 0.4 | 6.2 ± 0.5 | 5.7 ± 0.4 | 6.1 ± 0.6 | 0.6 ± 0.7 | 1.000 | −1.3, 2.5 | 0.4 ± 0.7 | 1.000 | −1.5, 2.4 | |||
| Meats | 8.9 ± 0.6 | 8.5 ± 0.5 | 8.3 ± 0.5 | 8.4 ± 0.5 | −0.5 ± 0.6 | 1.000 | −2.0, 1.1 | −0.0 ± 0.5 | 1.000 | −1.3, 1.3 | |||
| Fruits | 32.1 ± 1.9 | 34.4 ± 2.0 | 32.4 ± 1.7 | 35.1 ± 2.1 | 3.3 ± 1.8 | 0.472 | −1.7, 8.2 | 3.2 ± 1.8 | 0.470 | −1.6, 8.0 | |||
| Vegetables | 15.3 ± 0.8 | 15.9 ± 0.8 | 16.1 ± 0.9 | 16.8 ± 1.0 | 1.2 ± 0.7 | 0.532 | −0.7, 3.2 | 0.6 ± 0.7 | 1.000 | −1.2, 2.5 | |||
| Potatoes | 3.8 ± 0.4 | 3.7 ± 0.4 | 3.7 ± 0.4 | 4.5 ± 0.5 | 0.7 ± 0.5 | 0.894 | −0.6, 1.9 | 0.7 ± 0.4 | 0.545 | −0.4, 1.8 | |||
| Dairy | 43.6 ± 2.8 | 45.3 ± 2.8 | 45.1 ± 2.9 | 43.9 ± 2.9 | 1.2 ± 2.6 | 1.000 | −5.8, 8.2 | −0.8 ± 2.7 | 1.000 | −8.2, 6.6 | |||
| Breads | 8.6 ± 0.5 | 8.3 ± 0.5 | 7.9 ± 0.5 | 7.6 ± 0.6 | −1.1 ± 0.5 | 0.110 | −2.3, 0.1 | −0.5 ± 0.5 | 1.000 | −1.9, 1.0 | |||
| Cereals | 19.0 ± 1.3 | 19.4 ± 1.4 | 19.5 ± 1.4 | 17.5 ± 1.5 | −1.8 ± 1.1 | 0.639 | −4.8, 1.2 | −2.4 ± 1.1 | 0.165 | −5.4, 0.5 | |||
| Red Wine | 8.1 ± 1.3 | 8.7 ± 1.6 | 9.9 ± 2.0 | 12.0 ± 2.5 | 3.2 ± 1.4 | 0.153 | −0.6, 7.1 | 1.7 ± 1.2 | 0.927 | −1.5, 4.9 | |||
| Eggs | 2.7 ± 0.2 | 2.9 ± 0.2 | 3.0 ± 0.2 | 3.2 ± 0.3 | 0.5 ± 0.2 | 0.111 | −0.1, 1.1 | 0.2 ± 0.3 | 1.000 | −0.5, 0.9 | |||
| Sugars | 1.2 ± 0.1 | 1.0 ± 0.1 | 1.2 ± 0.2 | 1.0 ± 0.1 | −0.2 ± 0.1 | 0.146 | −0.5, 0.0 | −0.2 ± 0.1 | 0.356 | −0.5, 0.1 | |||
| Nuts | 1.6 ± 0.2 | 1.4 ± 0.1 | 1.5 ± 0.1 | 1.6 ± 0.1 | −0.0 ± 0.2 | 1.000 | −0.5, 0.5 | 0.1 ± 0.1 | 1.000 | −0.3, 0.4 | |||
| Other Alcohol | 10.4 ± 2.3 | 11.6 ± 2.7 | 13.0 ± 3.1 | 14.1 ± 3.6 | 2.6 ± 1.6 | 0.570 | −1.6, 6.8 | 0.4 ± 1.4 | 1.000 | −3.3, 4.1 | |||
| Discretionary Foods | 27.7 ± 2.6 | 27.0 ± 3.0 | 28.7 ± 3.2 | 28.8 ± 3.8 | 0.8 ± 1.8 | 1.000 | −4.0, 5.6 | −0.3 ± 1.6 | 1.000 | −4.5, 4.0 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murphy, K.J.; Dyer, K.A.; Hyde, B.; Davis, C.R.; Bracci, E.L.; Woodman, R.J.; Hodgson, J.M. Long-Term Adherence to a Mediterranean Diet 1-Year after Completion of the MedLey Study. Nutrients 2022, 14, 3098. https://doi.org/10.3390/nu14153098
Murphy KJ, Dyer KA, Hyde B, Davis CR, Bracci EL, Woodman RJ, Hodgson JM. Long-Term Adherence to a Mediterranean Diet 1-Year after Completion of the MedLey Study. Nutrients. 2022; 14(15):3098. https://doi.org/10.3390/nu14153098
Chicago/Turabian StyleMurphy, Karen J., Kathryn A. Dyer, Belinda Hyde, Courtney R. Davis, Ella L. Bracci, Richard J. Woodman, and Jonathan M. Hodgson. 2022. "Long-Term Adherence to a Mediterranean Diet 1-Year after Completion of the MedLey Study" Nutrients 14, no. 15: 3098. https://doi.org/10.3390/nu14153098
APA StyleMurphy, K. J., Dyer, K. A., Hyde, B., Davis, C. R., Bracci, E. L., Woodman, R. J., & Hodgson, J. M. (2022). Long-Term Adherence to a Mediterranean Diet 1-Year after Completion of the MedLey Study. Nutrients, 14(15), 3098. https://doi.org/10.3390/nu14153098