Optimization of Omega-3 Index Levels in Athletes at the US Naval Academy: Personalized Omega-3 Fatty Acid Dosage and Molecular Genetic Approaches



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Details
2.2.1. Study Design
2.2.2. Data Collection
2.2.3. Biomarkers
2.2.4. Intervention
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Primary Analysis Results
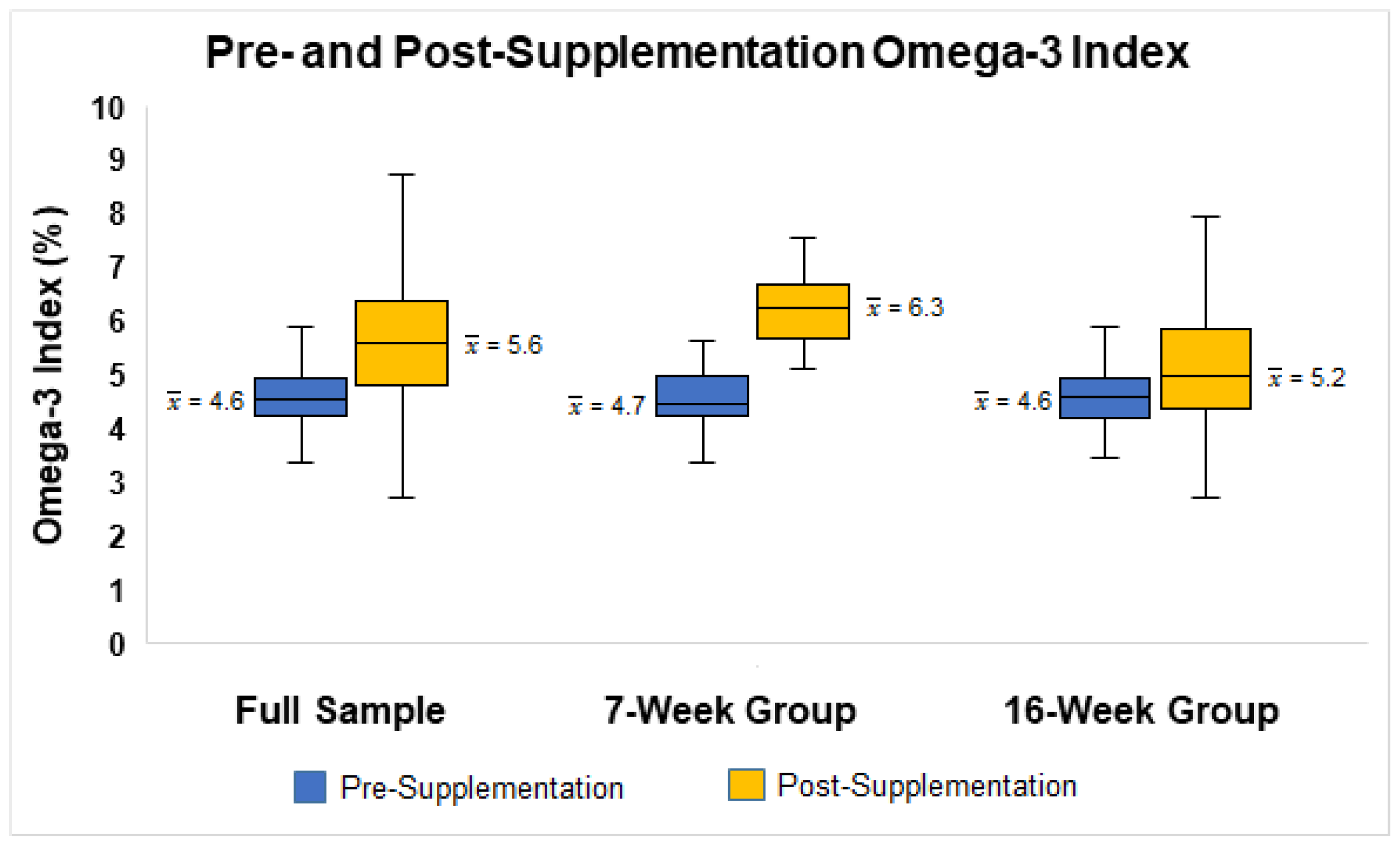
3.2.1. Omega-3 Index
3.2.2. Predictors of Omega-3 Index
3.2.3. Genetics and Omega-3 Index
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Elagizi, A.; Lavie, C.J.; Marshall, K.; DiNicolantonio, J.J.; O’Keefe, J.H.; Milani, R.V. Omega-3 Polyunsaturated Fatty Acids and Cardiovascular Health: A Comprehensive Review. Prog. Cardiovasc. Dis. 2018, 61, 76–85. [Google Scholar] [CrossRef] [Green Version]
- Harris, W.S.; Del Gobbo, L.; Tintle, N.L. The Omega-3 Index and relative risk for coronary heart disease mortality: Estimation from 10 cohort studies. Atherosclerosis 2017, 262, 51–54. [Google Scholar] [CrossRef]
- Xin, G.; Eshaghi, H. Effect of omega-3 fatty acids supplementation on indirect blood markers of exercise-induced muscle damage: Systematic review and meta-analysis of randomized controlled trials. Food Sci. Nutr. 2021, 9, 6429–6442. [Google Scholar] [CrossRef]
- Papadopoulou, S.K. Rehabilitation Nutrition for Injury Recovery of Athletes: The Role of Macronutrient Intake. Nutrients 2020, 12, 2449. [Google Scholar] [CrossRef]
- Calder, P.C. Omega-3 fatty acids and inflammatory processes. Nutrients 2010, 2, 355–374. [Google Scholar] [CrossRef] [Green Version]
- Djuricic, I.; Calder, P.C. Beneficial Outcomes of Omega-6 and Omega-3 Polyunsaturated Fatty Acids on Human Health: An Update for 2021. Nutrients 2021, 13, 2421. [Google Scholar] [CrossRef]
- United States Department of Agriculture; United States Department of Health and Human Services. Dietary Guidelines for Americans 2020–2025. Available online: DietaryGuidelines.gov (accessed on 1 July 2022).
- Rittenhouse, M.; Scott, J.; Deuster, P. Healthy Eating Index and Nutrition Biomarkers among Army Soldiers and Civilian Control Group Indicate an Intervention Is Necessary to Raise Omega-3 Index and Vitamin D and Improve Diet Quality. Nutrients 2020, 13, 122. [Google Scholar] [CrossRef]
- Walker, R.E.; Jackson, K.H.; Tintle, N.L.; Shearer, G.C.; Bernasconi, A.; Masson, S.; Latini, R.; Heydari, B.; Kwong, R.Y.; Flock, M.; et al. Predicting the effects of supplemental EPA and DHA on the omega-3 index. Am. J. Clin. Nutr. 2019, 110, 1034–1040. [Google Scholar] [CrossRef]
- Kris-Etherton, P.M.; Richter, C.K.; Bowen, K.J.; Skulas-Ray, A.C.; Jackson, K.H.; Petersen, K.S.; Harris, W.S. Recent Clinical Trials Shed New Light on the Cardiovascular Benefits of Omega-3 Fatty Acids. Methodist Debakey Cardiovasc. J. 2019, 15, 171–178. [Google Scholar] [CrossRef]
- Rimm, E.B.; Appel, L.J.; Chiuve, S.E.; Djoussé, L.; Engler, M.B.; Kris-Etherton, P.M.; Mozaffarian, D.; Siscovick, D.S.; Lichtenstein, A.H. Seafood Long-Chain n-3 Polyunsaturated Fatty Acids and Cardiovascular Disease: A Science Advisory From the American Heart Association. Circulation 2018, 138, e35–e47. [Google Scholar] [CrossRef]
- Flock, M.R.; Skulas-Ray, A.C.; Harris, W.S.; Etherton, T.D.; Fleming, J.A.; Kris-Etherton, P.M. Determinants of erythrocyte omega-3 fatty acid content in response to fish oil supplementation: A dose-response randomized controlled trial. J. Am. Hear. Assoc. 2013, 2, e000513. [Google Scholar] [CrossRef] [Green Version]
- Laidlaw, M.; Cockerline, C.A.; Rowe, W.J. A randomized clinical trial to determine the efficacy of manufacturers’ recommended doses of omega-3 fatty acids from different sources in facilitating cardiovascular disease risk reduction. Lipids Health Dis. 2014, 13, 99. [Google Scholar] [CrossRef] [Green Version]
- Harris, W.S.; Von Schacky, C. The Omega-3 Index: A new risk factor for death from coronary heart disease? Prev. Med. 2004, 39, 212–220. [Google Scholar] [CrossRef]
- Dretsch, M.N.; Johnston, D.; Bradley, R.S.; MacRae, H.; Deuster, P.A.; Harris, W.S. Effects of omega-3 fatty acid supplementation on neurocognitive functioning and mood in deployed U.S. soldiers: A pilot study. Mil. Med. 2014, 179, 396–403. [Google Scholar] [CrossRef] [Green Version]
- Johnston, D.T.; Deuster, P.A.; Harris, W.S.; Macrae, H.; Dretsch, M.N. Red blood cell omega-3 fatty acid levels and neurocognitive performance in deployed U.S. Servicemembers. Nutr. Neurosci. 2013, 16, 30–38. [Google Scholar] [CrossRef]
- Anzalone, A.; Carbuhn, A.; Jones, L.; Gallop, A.; Smith, A.; Johnson, P.; Swearingen, L.; Moore, C.; Rimer, E.; McBeth, J.; et al. The Omega-3 Index in National Collegiate Athletic Association Division I Collegiate Football Athletes. J. Athl. Train. 2019, 54, 7–11. [Google Scholar] [CrossRef] [Green Version]
- Da Boit, M.; Hunter, A.M.; Gray, S.R. Fit with good fat? The role of n-3 polyunsaturated fatty acids on exercise performance. Metabolism 2017, 66, 45–54. [Google Scholar] [CrossRef] [Green Version]
- Drobnic, F.; Rueda, F.; Pons, V.; Banquells, M.; Cordobilla, B.; Domingo, J.C. Erythrocyte Omega-3 Fatty Acid Content in Elite Athletes in Response to Omega-3 Supplementation: A Dose-Response Pilot Study. J. Lipids 2017, 2017, 1–7. [Google Scholar] [CrossRef]
- Jakeman, J.R.; Lambrick, D.M.; Wooley, B.; Babraj, J.A.; Faulkner, J.A. Effect of an acute dose of omega-3 fish oil following exercise-induced muscle damage. Eur. J. Appl. Physiol. 2017, 117, 575–582. [Google Scholar] [CrossRef] [Green Version]
- Lewis, M.D.; Hibbeln, J.R.; Johnson, J.E.; Lin, Y.H.; Hyun, D.Y.; Loewke, J.D. Suicide deaths of active-duty US military and omega-3 fatty-acid status: A case-control comparison. J. Clin. Psychiatry 2011, 72, 1585–1590. [Google Scholar] [CrossRef] [Green Version]
- Marriott, B.P.; Turner, T.H.; Hibbeln, J.R.; Pregulman, M.; Newman, J.; Johnson, K.B.; Malek, A.M.; Malcolm, R.J.; Burbelo, G.A.; Wissman, J.W.; et al. Design and methods for the Ranger Resilience and Improved Performance on Phospholipid bound Omega-3′s (RRIPP-3 study). Contemp. Clin. Trials Commun. 2019, 15, 100359. [Google Scholar] [CrossRef] [PubMed]
- Mickleborough, T.D. Omega-3 Polyunsaturated Fatty Acids in Physical Performance Optimization. Int. J. Sport Nutr. Exerc. Metab. 2013, 23, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Oliver, J.M. Omega-3 Fatty Acids and Student-Athletes: Is It Time for Better Education and a Policy Change? J. Athl. Train. 2019, 54, 5–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Philpott, J.D.; Witard, O.C.; Galloway, S.D.R. Applications of omega-3 polyunsaturated fatty acid supplementation for sport performance. Res. Sports Med. 2019, 27, 219–237. [Google Scholar] [CrossRef] [PubMed]
- Teo, L.; Crawford, C.; Yehuda, R.; Jaghab, D.; Bingham, J.J.; Chittum, H.K.; Gallon, M.D.; O’Connell, M.L.; Arzola, S.M.; Berry, K. Omega-3 polyunsaturated fatty acids to optimize cognitive function for military mission-readiness: A systematic review and recommendations for the field. Nutr. Rev. 2017, 75, 36–48. [Google Scholar] [CrossRef] [Green Version]
- Wilson, P.B.; Madrigal, L.A. Associations among Omega-3 Fatty Acid Status, Anxiety, and Mental Toughness in Female Collegiate Athletes. J. Am. Coll. Nutr. 2017, 36, 602–607. [Google Scholar] [CrossRef]
- Lembke, P.; Capodice, J.; Hebert, K.; Swenson, T. Influence of omega-3 (n3) index on performance and wellbeing in young adults after heavy eccentric exercise. J. Sports Sci. Med. 2014, 13, 151–156. [Google Scholar]
- Lattka, E.; Illig, T.; Heinrich, J.; Koletzko, B. Do FADS genotypes enhance our knowledge about fatty acid related phenotypes? Clin. Nutr. 2010, 29, 277–287. [Google Scholar] [CrossRef]
- Merino, D.M.; Ma, D.W.; Mutch, D.M. Genetic variation in lipid desaturases and its impact on the development of human disease. Lipids Health Dis. 2010, 9, 63. [Google Scholar] [CrossRef] [Green Version]
- Roke, K.; Mutch, D.M. The role of FADS1/2 polymorphisms on cardiometabolic markers and fatty acid profiles in young adults consuming fish oil supplements. Nutrients 2014, 6, 2290–2304. [Google Scholar] [CrossRef]
- Hedges, L.V. Distribution Theory for Glass’s Estimator of Effect size and Related Estimators. J. Educ. Stat. 1981, 6, 107–128. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Marriott, B.P.; Turner, T.H.; Hibbeln, J.R.; Newman, J.C.; Pregulman, M.; Malek, A.M.; Malcolm, R.J.; Burbelo, G.A.; Wismann, J.W. Impact of Fatty Acid Supplementation on Cognitive Performance among United States (US) Military Officers: The Ranger Resilience and Improved Performance on Phospholipid-Bound Omega-3′s (RRIPP-3) Study. Nutrients 2021, 13, 1854. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, A.S.; Lutz, L.J.; Smith, T.J.; Hatch-McChesney, A.; O’Connor, K.L.; Carrigan, C.T.; Hawes, M.R.; McGraw, S.M.; Taylor, K.M.; Champagne, C.M.; et al. A Food-Based Intervention in a Military Dining Facility Improves Blood Fatty Acid Profile. Nutrients 2022, 14, 743. [Google Scholar] [CrossRef] [PubMed]
- Young, A.J.; Marriott, B.P.; Champagne, C.M.; Hawes, M.R.; Montain, S.J.; Johannsen, N.M.; Berry, K.; Hibbeln, J.R. Blood fatty acid changes in healthy young Americans in response to a 10-week diet that increased n-3 and reduced n-6 fatty acid consumption: A randomised controlled trial. Br. J. Nutr. 2017, 117, 1257–1269. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Outcomes | Frequency/Mean (SD) | ||
|---|---|---|---|
| Full Sample (n = 90) | 7-Week Group (n = 35) | 16-Week Group (n = 55) | |
| Sex | |||
| Male | 76% | 37% | 100% |
| Female | 24% | 63% | |
| Race | |||
| White | 63% | 83% | 51% |
| Black | 22% | 3% | 34% |
| Other | 14% | 14% | 15% |
| Age | 19.9 (1.3) | 19.7 (1.4) | 20 (1.2) |
| Height (in) | 70.8 (3.1) | 68.54 (3.1) | 72.3 (2.1) |
| Weight (lb) | 203.3 (50.1) | 161.4 (22.3) | 229.9 (44.2) |
| Waist circumference (in) | 34.1 (5.2) | 30.3 (2.3) | 36.6 (5.1) |
| Body Mass Index (BMI) | 28.2 (5.4) | 24.1 (2.4) | 30.8 (5.2) |
| Total Fat (%) | 20 (5.1) | 21.3 (5.4) | 19.2 (4.8) |
| FADS1 | |||
| GG | 50% | 31% | 62% |
| GT/TT | 50% | 69% | 38% |
| FADS2 | |||
| CC | 43% | 30% | 51% |
| CA/AA | 57% | 70% | 49% |
| Fish intake (pre-supplementation) | |||
| None | 27% | 29% | 26% |
| Every other week | 36% | 37% | 35% |
| Every week | 21% | 11% | 26% |
| 2+ times per week | 16% | 20% | 13% |
| Fish intake (post-supplementation) | |||
| None | 26% | 26% | 20% |
| Every other week | 34% | 17% | 36% |
| Every week | 26% | 26% | 20% |
| 2+ times per week | 14% | 14% | 11% |
| Omega-3 Index (pre-supplementation) | 4.6 (0.8) | 4.7 (1) | 4.6 (0.6) |
| Omega-3 Index (post-supplementation) | 5.6 (1.2) | 6.3 (0.9) | 5.2 (1.1) |
| ∆ Omega-3 Index | 1 (1.2) | 1.6 (1.1) | 0.7 (1.13) |
| Target Omega-3 Index met (≥8%) | |||
| Yes | 3% | 3% | 2% |
| No | 97% | 97% | 98% |
| Target ∆ Omega-3 Index met (≥2%) | |||
| Yes | 18% | 34% | 8% |
| No | 82% | 66% | 92% |
| O3I Risk Categories (n = 78) | Pre-Supplementation (n = 78) | Post-Supplementation (n = 78) |
|---|---|---|
| 4% or less | 17.9% | 6.4% |
| 4.01–7.99% | 80.8% | 91% |
| 8% or more | 1.3% | 2.6% |
| Predictors | Unadjusted Models | Adjusted Model 1a 1 | Adjusted Model 1b 2 | ||||
|---|---|---|---|---|---|---|---|
| B (SE) | β | Radj2 | B (SE) | β | B (SE) | β | |
| Pre-Supplementation O3I | 0.49 (0.77) † | 0.32 † | 0.09 * | 0.4 (0.16) † | 0.28 † | 0.39 (0.16) † | 0.27 † |
| Supplementation Duration | 0.21 * | ||||||
| 16 weeks (reference) | |||||||
| 7 weeks | 1.14 (0.25) † | 0.47 † | 0.92 (0.43) † | 0.38 † | 0.91 (0.42) † | 0.39 † | |
| Fish Intake | 0.01 | ||||||
| None (reference) | |||||||
| Every other week | −0.11 (0.36) | −0.05 | −0.08 (0.31) | −0.03 | −0.18 (0.3) | −0.08 | |
| Every week | −0.12 (0.4) | −0.04 | −0.11 (0.36) | −0.04 | −0.22 (0.36) | −0.08 | |
| 2+ times per week | 0.19 (0.44) | 0.06 | −0.34 (0.39) | −0.11 | −0.41 (0.39) | −0.13 | |
| BMI | −0.07 (0.03) † | −0.28 † | 0.07 * | 0.03 (0.05) | 0.12 | 0.03 (0.05) | 0.12 |
| Total Fat (%) | 0.02 (0.03) | 0.08 | −0.01 | −0.04 (0.05) | −0.2 | −0.04 (0.05) | −0.17 |
| Sex | 0.12 * | ||||||
| Male (reference) | |||||||
| Female | 0.99 (0.29) † | −0.36 † | 0.27 (0.59) | 0.1 | 0.17 (0.59) | 0.06 | |
| Race | 0.23 * | ||||||
| White (reference) | |||||||
| Black | −1.03 (0.28) † | −0.37 † | −0.75 (0.32) † | −0.27 † | −0.76 (0.32) † | −0.28 † | |
| Other | −1.45 (0.35) † | −0.43 † | −1.22 (0.37) † | −0.36 † | −1.2 (0.37) † | −0.36 † | |
| FADS1 | −0.01 | ||||||
| GG (reference) | |||||||
| GT/TT | 0.2 (0.27) | 0.09 | −0.11 (0.27) | −0.05 | |||
| FADS2 | −0.01 | ||||||
| CC (reference) | |||||||
| CA/AA | 0.02 (0.27) | 0.01 | −0.05 (0.25) | −0.02 | |||
| Radj2 | 0.32 * | 0.32 * | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rittenhouse, M.; Sambuughin, N.; Deuster, P. Optimization of Omega-3 Index Levels in Athletes at the US Naval Academy: Personalized Omega-3 Fatty Acid Dosage and Molecular Genetic Approaches. Nutrients 2022, 14, 2966. https://doi.org/10.3390/nu14142966
Rittenhouse M, Sambuughin N, Deuster P. Optimization of Omega-3 Index Levels in Athletes at the US Naval Academy: Personalized Omega-3 Fatty Acid Dosage and Molecular Genetic Approaches. Nutrients. 2022; 14(14):2966. https://doi.org/10.3390/nu14142966
Chicago/Turabian StyleRittenhouse, Melissa, Nyamkhishig Sambuughin, and Patricia Deuster. 2022. "Optimization of Omega-3 Index Levels in Athletes at the US Naval Academy: Personalized Omega-3 Fatty Acid Dosage and Molecular Genetic Approaches" Nutrients 14, no. 14: 2966. https://doi.org/10.3390/nu14142966
APA StyleRittenhouse, M., Sambuughin, N., & Deuster, P. (2022). Optimization of Omega-3 Index Levels in Athletes at the US Naval Academy: Personalized Omega-3 Fatty Acid Dosage and Molecular Genetic Approaches. Nutrients, 14(14), 2966. https://doi.org/10.3390/nu14142966