
Nutritional Biomarkers and Factors Correlated with Poor Sleep Status among Young Females: A Case-Control Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
Sample Size
2.2. Data Collection
2.2.1. Anthropometric Measurements
2.2.2. Biochemical Blood Analysis
2.2.3. Sleep Index
2.2.4. Stress Scale
2.2.5. Physical Activity (PA)
2.2.6. Dietary Data
Polyphenol Intake
Estimation of Dietary Polyphenol Intake
2.3. Statistical Analysis
3. Results
3.1. The General, Anthropometric Measurements, and Biochemical Analysis
3.2. Dietary Intake and Lifestyle Characteristics
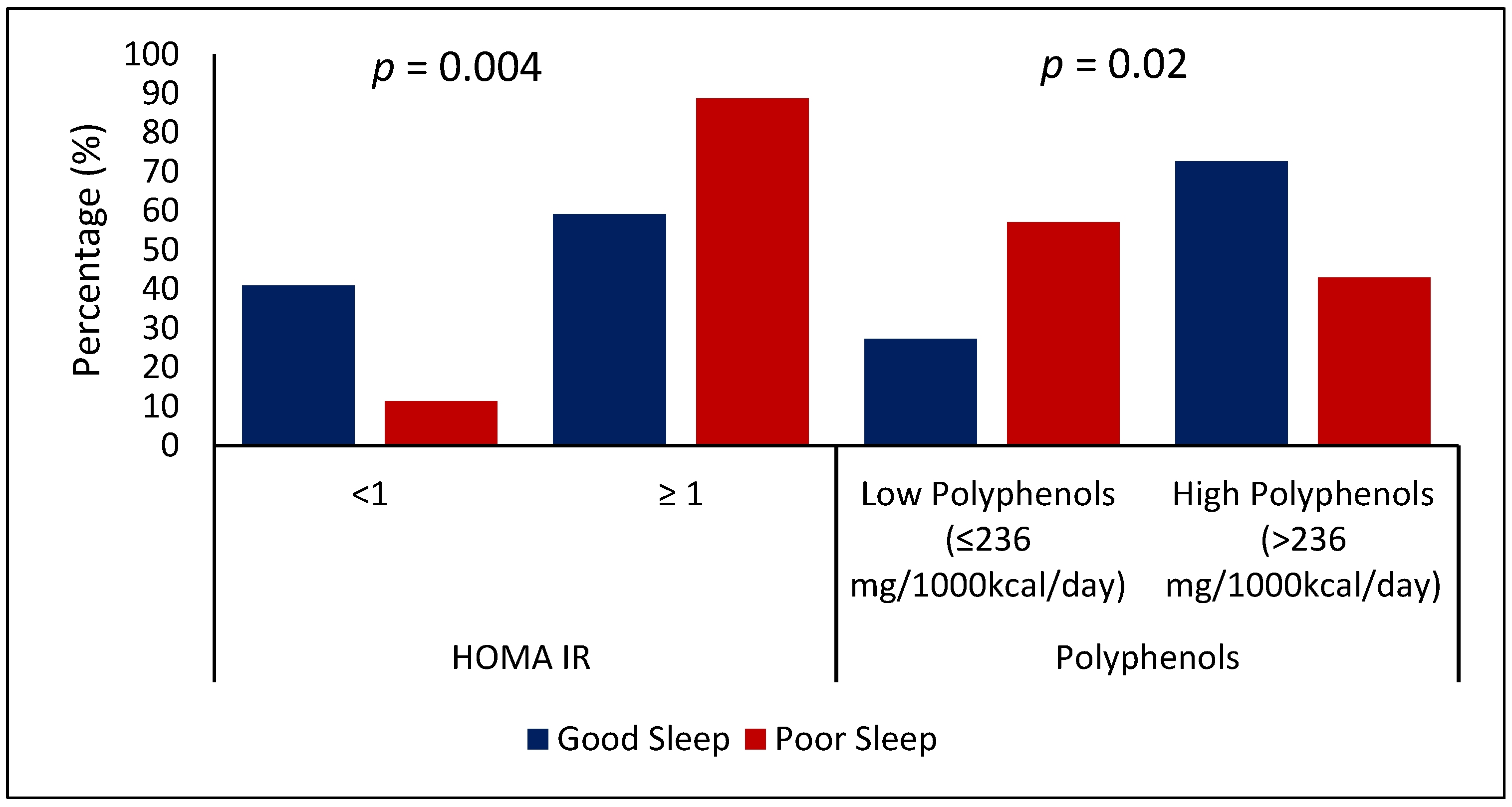
3.3. The Association between BMI, HDL, HOMA-IR, Dietary Intake, and Sleep Status
4. Discussion
4.1. Insulin Resistance and Sleep
4.2. Polyphenols and Sleep
4.3. Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kirov, R.; Brand, S. The Memory, Cognitive and Psychological Functions of Sleep: Update from Electroencephalographic and Neuroimaging Studies. Neuroimaging-Cogn. Clin. Neurosci. 2012, 8, 78–90. [Google Scholar] [CrossRef] [Green Version]
- Mehta, K.J. Effect of Sleep and Mood on Academic Performance—At Interface of Physiology, Psychology, and Education. Humanit. Soc. Sci. Commun. 2022, 9, 16. [Google Scholar] [CrossRef]
- Becker, S.P.; Jarrett, M.A.; Luebbe, A.M.; Garner, A.A.; Burns, G.L.; Kofler, M.J. Sleep in a Large, Multi-University Sample of College Students: Sleep Problem Prevalence, Sex Differences, and Mental Health Correlates. Sleep Health 2018, 4, 174–181. [Google Scholar] [CrossRef]
- Ibrahim, N.K.; Badawi, F.; Mansouri, Y.; Ainousa, A.; Jambi, S.; Fatani, A.N. Sleep Quality among Medical Students at King Abdulaziz University: A Cross-Sectional Study. J. Community Med. Health Educ. 2017, 7, 2161–2711. [Google Scholar] [CrossRef] [Green Version]
- Ogilvie, R.P.; Patel, S.R. The Epidemiology of Sleep and Obesity. Sleep Health 2017, 3, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Guo, J.; Gong, T.-T.; Lv, J.-L.; Li, X.-Y.; Liu, F.-H.; Zhang, M.; Shan, Y.-T.; Zhao, Y.-H.; Wu, Q.-J. Sleep Duration/Quality with Health Outcomes: An Umbrella Review of Meta-Analyses of Prospective Studies. Front. Med. 2022, 8, 813943. [Google Scholar] [CrossRef]
- Kothari, V.; Cardona, Z.; Chirakalwasan, N.; Anothaisintawee, T.; Reutrakul, S. Sleep Interventions and Glucose Metabolism: Systematic Review and Meta-Analysis. Sleep Med. 2021, 78, 24–35. [Google Scholar] [CrossRef]
- Mullington, J.M.; Simpson, N.S.; Meier-Ewert, H.K.; Haack, M. Sleep Loss and Inflammation. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 775–784. [Google Scholar] [CrossRef] [Green Version]
- Mallampalli, M.P.; Carter, C.L. Exploring Sex and Gender Differences in Sleep Health: A Society for Women’s Health Research Report. J. Women’s Health 2014, 23, 553–562. Available online: https://home.liebertpub.com/jwh (accessed on 1 March 2022). [CrossRef] [Green Version]
- Gardani, M.; Bradford, D.R.R.; Russell, K.; Allan, S.; Beattie, L.; Ellis, J.G.; Akram, U. A Systematic Review and Meta-Analysis of Poor Sleep, Insomnia Symptoms and Stress in Undergraduate Students. Sleep Med. Rev. 2022, 61, 101565. [Google Scholar] [CrossRef]
- Wang, L.; Jin, F. Association between Maternal Sleep Duration and Quality, and the Risk of Preterm Birth: A Systematic Review and Meta-Analysis of Observational Studies. BMC Pregnancy Childbirth 2020, 20, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.; Choh, A.C.; Demerath, E.W.; Knutson, K.L.; Duren, D.L.; Sherwood, R.J.; Sun, S.S.; Chumlea, W.M.C.; Towne, B.; Siervogel, R.M.; et al. Sleep Disturbance in Relation to Health-Related Quality of Life in Adults: The Fels Longitudinal Study. J. Nutr. Health Aging 2009, 13, 576–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kocevska, D.; Barclay, N.L.; Bramer, W.M.; Gehrman, P.R.; Van Someren, E.J.W. Heritability of Sleep Duration and Quality: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2021, 59, 101448. [Google Scholar] [CrossRef] [PubMed]
- Manzar, M.D.; Alghadir, A.H.; Khan, M.; Salahuddin, M.; Albougami, A.; Maniago, J.D.; Vasquez, B.A.; Pandi-Perumal, S.R.; Bahammam, A.S. Anxiety Symptoms Are Associated with Higher Psychological Stress, Poor Sleep, and Inadequate Sleep Hygiene in Collegiate Young Adults—A Cross-Sectional Study. Front. Psychiatry 2021, 12, 677136. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Tuo, H.; Wang, S.; Zhao, L. The Effects of Dietary Nutrition on Sleep and Sleep Disorders. Mediat. Inflamm. 2020, 2020, 3142874. [Google Scholar] [CrossRef]
- Gao, Q.; Kou, T.; Zhuang, B.; Ren, Y.; Dong, X.; Wang, Q. The Association between Vitamin D Deficiency and Sleep Disorders: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 1395. [Google Scholar] [CrossRef] [Green Version]
- Al-Musharaf, S.; Alabdulaaly, A.; Mujalli, H.B.; Alshehri, H.; Alajaji, H.; Bogis, R.; Alnafisah, R.; Alfehaid, S.; Alhodaib, H.; Murphy, A.; et al. Sleep Quality Is Associated with Vitamin B12 Status in Female Arab Students. Int. J. Environ. Res. Public Health 2021, 18, 4548. [Google Scholar] [CrossRef]
- Lian, Y.; Yuan, Q.; Wang, G.; Tang, F. Association between Sleep Quality and Metabolic Syndrome: A Systematic Review and Meta-Analysis. Psychiatry Res. 2019, 274, 66–74. [Google Scholar] [CrossRef]
- Godos, J.; Ferri, R.; Castellano, S.; Angelino, D.; Mena, P.; Del Rio, D.; Caraci, F.; Galvano, F.; Grosso, G. Specific Dietary (Poly)Phenols Are Associated with Sleep Quality in a Cohort of Italian Adults. Nutrients 2020, 12, 1226. [Google Scholar] [CrossRef]
- Fraga, C.G.; Croft, K.D.; Kennedy, D.O.; Tomás-Barberán, F.A. The Effects of Polyphenols and Other Bioactives on Human Health. Food Funct. 2019, 10, 514–528. [Google Scholar] [CrossRef] [Green Version]
- Noorwali, E.; Hardie, L.; Cade, J. Bridging the Reciprocal Gap between Sleep and Fruit and Vegetable Consumption: A Review of the Evidence, Potential Mechanisms, Implications, and Directions for Future Work. Nutrients 2019, 11, 1382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noorwali, E.; Hardie, L.; Cade, J. Fruit and Vegetable Consumption and Their Polyphenol Content Are Inversely Associated with Sleep Duration: Prospective Associations from the UK Women’s Cohort Study. Nutrients 2018, 10, 1803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tubbs, A.S.; Kennedy, K.E.R.; Alfonso-Miller, P.; Wills, C.C.A.; Grandner, M.A. A Randomized, Double-Blind, Placebo-Controlled Trial of a Polyphenol Botanical Blend on Sleep and Daytime Functioning. Int. J. Environ. Res. Public Health 2021, 18, 3044. [Google Scholar] [CrossRef]
- Hur, M.H.; Lee, M.K.; Seong, K.; Hong, J.H. Deterioration of Sleep Quality According to Glycemic Status. Diabetes Metab. J. 2020, 44, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhao, L.-H.; Li, D.-D.; Xu, F.; Wang, X.-H.; Lu, C.-F.; Wang, C.-H.; Yu, C.; Zhang, X.-L.; Ning, L.-Y.; et al. Association of Sleep Quality with Glycemic Variability Assessed by Flash Glucose Monitoring in Patients with Type 2 Diabetes. Diabetol. Metab. Syndr. 2021, 13, 102. [Google Scholar] [CrossRef] [PubMed]
- Barakat, S.; Abujbara, M.; Banimustafa, R.; Batieha, A.; Ajlouni, K. Sleep Quality in Patients with Type 2 Diabetes Mellitus. J. Clin. Med. Res. 2019, 11, 261–266. [Google Scholar] [CrossRef] [Green Version]
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; IDF: Brussels, Belgium, 2021. [Google Scholar]
- Hashemipour, S.; Ghorbani, A.; Khashayar, A.; Olfati, H. Association of Sleep Quality with Insulin Resistance in Obese or Overweight Subjects. Sleep Sci. (Sao Paulo Braz.) 2021, 14, 75–78. [Google Scholar] [CrossRef]
- Knutson, K.L.; Van Cauter, E.; Zee, P.; Liu, K.; Lauderdale, D.S. Cross-Sectional Associations Between Measures of Sleep and Markers of Glucose Metabolism Among Subjects with and without Diabetes: The Coronary Artery Risk Development in Young Adults (CARDIA) Sleep Study. Diabetes Care 2011, 34, 1171–1176. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation. Available online: https://apps.who.int/iris/handle/10665/42330 (accessed on 5 March 2022).
- World Health Organization. Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation. Available online: https://www.who.int/publications/i/item/9789241501491 (accessed on 20 May 2022).
- So, W.-Y.; Swearingin, B.; Crooms, B.; Lee, R.; Choi, Y.; Dail, T.K.; Melton, D.; Fuller, T.M.; Ha, C.-H. Body Composition Measurements Determined by Airdisplacement Plethysmography and Eight-Polar Bioelectrical Impedance Analysis Are Equivalent in African American College Students. Healthmed 2012, 6, 1896–1899. [Google Scholar]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Salgado, A.L.F.D.A.; De Carvalho, L.; Oliveira, A.C.; Dos Santos, V.N.; Vieira, J.G.; Parise, E.R. Insulin Resistance Index (HOMA-IR) in the Differentiation of Patients with Non-Alcoholic Fatty Liver Disease and Healthy Individuals. Arq. Gastroenterol. 2010, 47, 165–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Do, H.D.; Lohsoonthorn, V.; Jiamjarasrangsi, W.; Lertmaharit, S.; Williams, M.A. Prevalence of Insulin Resistance and Its Relationship with Cardiovascular Disease Risk Factors among Thai Adults over 35 Years Old. Diabetes Res. Clin. Pract. 2010, 89, 303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thacher, T.D.; Clarke, B.L. Vitamin D Insufficiency. Mayo Clin. Proc. 2011, 86, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suleiman, K.H.; Yates, B.C.; Berger, A.M.; Pozehl, B.; Meza, J. Translating the Pittsburgh Sleep Quality Index into Arabic. West. J. Nurs. Res. 2010, 32, 250–268. [Google Scholar] [CrossRef] [PubMed]
- Almadi, T.; Cathers, I.; Hamdan Mansour, A.M.; Chow, C.M. An Arabic Version of the Perceived Stress Scale: Translation and Validation Study. Int. J. Nurs. Stud. 2012, 49, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Alkahtani, S.A. Convergent Validity: Agreement between Accelerometry and the Global Physical Activity Questionnaire in College-Age Saudi Men. BMC Res. Notes 2016, 9, 436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D.; Alissa, E.M.; Bahjri, S.M. Validation of a Food Frequency Questionnaire Specific for Salt Intake in Saudi Arabian Adults Using Urinary Biomarker and Repeated Multiple Pass 24-Hour Dietary Recall. Proc. Nutr. Soc. 2015, 74, 337. [Google Scholar] [CrossRef] [Green Version]
- Bingham, S.A.; Gill, C.; Welch, A.; Cassidy, A.; Runswick, S.A.; Oakes, S.; Lubin, R.; Thurnham, D.I.; Key, T.J.A.; Roe, L.; et al. Validation of Dietary Assessment Methods in the UK Arm of EPIC Using Weighed Records, and 24-Hour Urinary Nitrogen and Potassium and Serum Vitamin C and Carotenoids as Biomarkers. Int. J. Epidemiol. 1997, 26 (Suppl. S1), S137–S151. [Google Scholar] [CrossRef]
- Rothwell, J.A.; Perez-Jimenez, J.; Neveu, V.; Medina-Remón, A.; M’Hiri, N.; García-Lobato, P.; Manach, C.; Knox, C.; Eisner, R.; Wishart, D.S.; et al. Phenol-Explorer 3.0: A Major Update of the Phenol-Explorer Database to Incorporate Data on the Effects of Food Processing on Polyphenol Content. Database J. Biol. Databases Curation 2013, 2013, bat070. [Google Scholar] [CrossRef]
- Neveu, V.; Perez-Jiménez, J.; Vos, F.; Crespy, V.; du Chaffaut, L.; Mennen, L.; Knox, C.; Eisner, R.; Cruz, J.; Wishart, D.; et al. Phenol-Explorer: An Online Comprehensive Database on Polyphenol Contents in Foods. Database J. Biol. Databases Curation 2010, 2010, bap024. [Google Scholar] [CrossRef]
- Pérez-Jiménez, J.; Neveu, V.; Vos, F.; Scalbert, A. Identification of the 100 Richest Dietary Sources of Polyphenols: An Application of the Phenol-Explorer Database. Eur. J. Clin. Nutr. 2010, 64, S112–S120. [Google Scholar] [CrossRef] [PubMed]
- Vitale, M.; Masulli, M.; Rivellese, A.A.; Bonora, E.; Cappellini, F.; Nicolucci, A.; Squatrito, S.; Antenucci, D.; Barrea, A.; Bianchi, C.; et al. Dietary Intake and Major Food Sources of Polyphenols in People with Type 2 Diabetes: The TOSCA.IT Study. Eur. J. Nutr. 2018, 57, 679–688. [Google Scholar] [CrossRef] [PubMed]
- Cedernaes, J.; Lampola, L.; Axelsson, E.K.; Liethof, L.; Hassanzadeh, S.; Yeganeh, A.; Broman, J.E.; Schiöth, H.B.; Benedict, C. A Single Night of Partial Sleep Loss Impairs Fasting Insulin Sensitivity but Does Not Affect Cephalic Phase Insulin Release in Young Men. J. Sleep Res. 2016, 25, 5–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joo, J.H.; Lee, J.G.; Kim, S.W.; Lee, J.H.; Lee, J.H.; Lee, K.J. Association between Sleep Duration and Impaired Fasting Glucose According to Work Type in Non-Regular Workers: Data from the First and Second Year (2016, 2017) of the 7th Korean National Health and Nutrition Examination (KNHANE) (a Cross-Sectional Study). Ann. Occup. Environ. Med. 2020, 32, e29. [Google Scholar] [CrossRef]
- Balkau, B.; Vol, S.; Loko, S.; Andriamboavonjy, T.; Lantieri, O.; Gusto, G.; Meslier, N.; Racineux, J.L.; Tichet, J.; Charles, M.A.; et al. High Baseline Insulin Levels Associated with 6-Year Incident Observed Sleep Apnea. Diabetes Care 2010, 33, 1044. [Google Scholar] [CrossRef] [Green Version]
- Pilcher, J.J.; Erikson, D.N.; Yochum, C.A. Fighting the Freshman Fifteen: Sleep, Exercise, and BMI in College Students. Am. J. Health Promot. 2021, 35, 580–583. [Google Scholar] [CrossRef]
- Rahe, C.; Czira, M.E.; Teismann, H.; Berger, K. Associations between Poor Sleep Quality and Different Measures of Obesity. Sleep Med. 2015, 16, 1225–1228. [Google Scholar] [CrossRef]
- Yiallourou, S.R.; Carrington, M.J. Improved Sleep Efficiency Is Associated with Reduced Cardio-Metabolic Risk: Findings from the MODERN Trial. J. Sleep Res. 2021, 30, e13389. [Google Scholar] [CrossRef]
- Romain, C.; Alcaraz, P.E.; Chung, L.H.; Cases, J. Regular Consumption of HolisFiit, a Polyphenol-Rich Extract-Based Food Supplement, Improves Mind and Body Well-Being of Overweight and Slightly Obese Volunteers: A Randomized, Double-Blind, Parallel Trial. Int. J. Food Sci. Nutr. 2017, 68, 840–848. [Google Scholar] [CrossRef]
- De Ligt, M.; Bergman, M.; Fuentes, R.M.; Essers, H.; Moonen-Kornips, E.; Havekes, B.; Schrauwen-Hinderling, V.B.; Schrauwen, P. No Effect of Resveratrol Supplementation after 6 Months on Insulin Sensitivity in Overweight Adults: A Randomized Trial. Am. J. Clin. Nutr. 2020, 112, 1029–1038. [Google Scholar] [CrossRef]
- Pourreza, S.; Khademi, Z.; Mirzababaei, A.; Yekaninejad, M.S.; Sadeghniiat-Haghighi, K.; Naghshi, S.; Mirzaei, K. Association of Plant-Based Diet Index with Inflammatory Markers and Sleep Quality in Overweight and Obese Female Adults: A Cross-Sectional Study. Int. J. Clin. Pract. 2021, 75, e14429. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.P.; Crawford, A.; Aggarwal, B. Plant-Based Diets: Reducing Cardiovascular Risk by Improving Sleep Quality? Curr. Sleep Med. Rep. 2018, 4, 74. [Google Scholar] [CrossRef]
- Manach, C.; Scalbert, A.; Morand, C.; Rémésy, C.; Jiménez, L. Polyphenols: Food Sources and Bioavailability. Am. J. Clin. Nutr. 2004, 79, 727–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campanini, M.Z.; Guallar-Castillón, P.; Rodríguez-Artalejo, F.; Lopez-Garcia, E. Mediterranean Diet and Changes in Sleep Duration and Indicators of Sleep Quality in Older Adults. Sleep 2017, 40, zsw083. [Google Scholar] [CrossRef]
- Haghighatdoost, F.; Bellissimo, N.; Totosy De Zepetnek, J.O.; Rouhani, M.H. Association of Vegetarian Diet with Inflammatory Biomarkers: A Systematic Review and Meta-Analysis of Observational Studies. Public Health Nutr. 2017, 20, 2713–2721. [Google Scholar] [CrossRef]
- Hu, Z.; Oh, S.; Ha, T.W.; Hong, J.T.; Oh, K.W. Sleep-Aids Derived from Natural Products. Biomol. Ther. 2018, 26, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.O.; Hong, J.T.; Oh, K.W. Rosmarinic Acid Potentiates Pentobarbital-Induced Sleep Behaviors and Non-Rapid Eye Movement (NREM) Sleep through the Activation of GABAa-Ergic Systems. Biomol. Ther. 2017, 25, 105–111. [Google Scholar] [CrossRef] [Green Version]
- Hepsomali, P.; Groeger, J.A.; Nishihira, J.; Scholey, A. Effects of Oral Gamma-Aminobutyric Acid (GABA) Administration on Stress and Sleep in Humans: A Systematic Review. Front. Neurosci. 2020, 14, 923. [Google Scholar] [CrossRef]
- Watson, C.J.; Baghdoyan, H.A.; Lydic, R. Neuropharmacology of Sleep and Wakefulness. Sleep Med. Clin. 2010, 5, 513–528. [Google Scholar] [CrossRef] [Green Version]
- Whitehouse, P.J. Acetylcholine. Encycl. Neurol. Sci. 2014, 7, 19–21. [Google Scholar] [CrossRef]
- Adachi, N.; Tomonaga, S.; Tachibana, T.; Denbow, D.M.; Furuse, M. (-)-Epigallocatechin Gallate Attenuates Acute Stress Responses through GABAergic System in the Brain. Eur. J. Pharmacol. 2006, 531, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Vignes, M.; Maurice, T.; Lanté, F.; Nedjar, M.; Thethi, K.; Guiramand, J.; Récasens, M. Anxiolytic Properties of Green Tea Polyphenol (-)-Epigallocatechin Gallate (EGCG). Brain Res. 2006, 1110, 102–115. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameters | PSQI Classification | p-Value | p-Value * | |
|---|---|---|---|---|
| Good Sleep 22 (23.9%) | Poor Sleep 70 (76.1%) | |||
| Anthropometric Measurements | ||||
| Age (years) | 20.6 ± 1.0 | 21.2 ± 1.6 | 0.07 | |
| BMI (kg/m2) | 24.8 ± 6.0 | 29.7 ± 8.2 | 0.004 | |
| WHR (ratio) | 0.7 ± 0.1 | 0.7 ± 0.1 | 0.11 | 0.27 |
| Fat (kg) | 39.3 ± 8.1 | 43.5 ± 9.6 | 0.07 | 0.39 |
| Protein (kg) | 7.2 ± 1.0 | 7.8 ± 1.2 | 0.04 | 0.94 |
| Fluid% | 44.7 ± 5.8 | 41.3 ± 6.9 | 0.05 | 0.46 |
| Clinical-Metabolic Blood Parameters | ||||
| Total cholesterol (mmol/L) | 4.2 ± 1.4 | 4.0 ± 1.5 | 0.67 | 0.23 |
| FBG (mmol/L) | 4.4 ± 0.7 | 4.7 ± 0.7 | 0.10 | 0.40 |
| HDL cholesterol (mmol/L) | 1.1 ± 0.4 | 1.0 ± 0.3 | 0.15 | 0.06 |
| LDL cholesterol (mmol/L) | 2.9 ± 1.2 | 2.9 ± 1.4 | 1.00 | 0.49 |
| Total cholesterol/HDL ratio | 4.0 ± 1.6 | 4.3 ± 1.7 | 0.43 | 0.73 |
| Triglyceride (mmol/L) # | 0.7 (0.5–0.9) | 0.8 (0.5–1.0) | 0.29 | 0.68 |
| Insulin (μIU/mL) # | 6.0 (4.3–12.4) | 11.3 (7.0–17.8) | <0.001 | 0.01 |
| HOMA-IR # | 1.2 (0.8–2.2) | 2.2 (1.2–3.9) | <0.001 | 0.03 |
| HOMA-β # | 98.8 (64.1–274.4) | 182.7 (131.3–306.1) | 0.06 | 0.29 |
| Vitamin D (nmol/L) | 33.0 (26.4–41.4) | 32.3 (22.8–46.8) | 0.75 | 0.73 |
| Severe vitamin D deficiency (<25 nmol/L) | 2 (10.0) | 23 (36.5) | 0.02 | 0.07 |
| Vitamin B12 (pg/mL) | 477.3 (322.2–683.3) | 389.6 (311.0–625.2) | 0.46 | 0.60 |
| Parameters | PSQI Classification | p-Value | p-Value * | |
|---|---|---|---|---|
| Good Sleep 22 (23.9%) | Poor Sleep 70 (76.1%) | |||
| Dietary Parameters | ||||
| Energy (kcal/day) | 3048.5 (2574.5–3539.7) | 3656.3 (2700.9–4649.3) | 0.08 | 0.07 |
| Fat (% of total kcal) | 37.1 (30.6–41.6) | 39.5 (33.6–46.5) | 0.11 | 0.20 |
| Protein (% of total kcal) | 14.1 (12.9–16.1) | 13.4 (11.6–15.1) | 0.15 | 0.16 |
| CHO (% of total kcal) | 48.6 (45.1–53.1) | 45.0 (39.6–52.8) | 0.18 | 0.33 |
| Fiber (g/1000 kcal) | 9.5 (8.0–12.6) | 9.8 (7.9–11.4) | 0.63 | 0.75 |
| Na (mg/1000 kcal) | 1459.9 (1278.0–1881.2) | 1323.7 (1110.7–1637.9) | 0.08 | 0.10 |
| Clinical-Metabolic Blood Parameters | ||||
| K (mg/1000 kcal) | 2070.0 (1418.2–2774.0) | 1761.9 (1449.3–2680.0) | 0.29 | 0.33 |
| Ca (mg/1000 kcal) | 39.2 (12.8–76.6) | 54.2 (19.3–108.8) | 0.33 | 0.86 |
| P (mg/1000 kcal) | 653.2 (527.0–1020.9) | 597.2 (520.2–749.9) | 0.25 | 0.27 |
| Fe (mg/1000 kcal) | 15.1 (9.9–20.8) | 11.6 (9.2–17.6) | 0.20 | 0.26 |
| Vitamin B12 intake (mcg/day) | 7.3 (5.8–12.3) | 7.8 (5.0–13.8) | 0.96 | 0.79 |
| Vitamin D intake (IU/day) | 3.3 (2.8–5.3) | 4.1 (2.2–6.2) | 0.71 | 0.82 |
| Polyphenols (mg/1000 kcal) | 348.6 (279.9–402.9) | 237.2 (180.7–311.2) | 0.004 | 0.03 |
| Low Polyphenols (≤236 mg/1000 kcal/day) | 194.8 (122.0–253.6) | 188.2 (148.6–217.8) | 0.69 | 0.75 |
| High Polyphenols (>236 mg/1000 kcal/day) | 392.2 (338.8–439.7) | 330.6 (284.4–480.2) | 0.13 | 0.88 |
| Food Groups | ||||
| Total dairy (g/1000 kcal) | 74.4 (43.5–96.9) | 99.1 (51.9–132.8) | 0.23 | 0.78 |
| Total fruit (g/1000 kcal) | 139.2 (78.1–316.9) | 94.1 (55.2–164.9) | 0.01 | 0.02 |
| Total vegetables (g/1000 kcal) | 201.4 (147.1–286.2) | 175.0 (116.4–247.6) | 0.18 | 0.30 |
| Total grains (g/1000 kcal) | 159.0 (128.0–194.6) | 134.2 (87.7–174.9) | 0.07 | 0.04 |
| Total red meat | 16.3 (14.6–19.4) | 13.5 (7.7–18.6) | 0.02 | 0.14 |
| Total white meat | 33.9 (29.0–39.8) | 30.3 (17.4–40.7) | 0.25 | 0.20 |
| Total dairy (g/1000 kcal) | 74.4 (43.5–96.9) | 99.1 (51.9–132.8) | 0.23 | 0.78 |
| Physical Activity Parameter | ||||
| GPAQ score | 8.1 ± 1.0 | 8.2 ± 1.1 | 0.86 | 0.79 |
| Stress Parameter | ||||
| PSS score | 16.9 ± 7.3 | 19.5 ± 6.0 | 0.09 | 0.11 |
| Crude | Multiple Regression | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| BMI | 1.10 (1.02–1.18) | 0.02 | 1.09 (0.99–1.20) | 0.08 |
| HDL | 0.32 (0.07–1.54) | 0.16 | 0.19 (0.03–1.10) | 0.06 |
| HOMA-IR (≥1) | 5.44 (1.71–17.32) | 0.004 | 4.97 (1.11–22.31) | 0.04 |
| Energy intake (>2200 kcal) | 0.95 (0.24–3.80) | 0.94 | 2.37 (0.35–16.01) | 0.38 |
| High polyphenol (>median) | 0.28 (0.10–0.80) | 0.02 | 0.24 (0.07–0.83) | 0.03 |
| Total grains (>Median g/1000 kcal) | 0.61 (0.23–1.63) | 0.33 | 0.72 (0.22–2.30) | 0.58 |
| Nagelkerke R Square (p-value) | -- | -- | 31.3% | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AL-Musharaf, S.; AlAjllan, L.; Aljuraiban, G.; AlSuhaibani, M.; Alafif, N.; Hussain, S.D. Nutritional Biomarkers and Factors Correlated with Poor Sleep Status among Young Females: A Case-Control Study. Nutrients 2022, 14, 2898. https://doi.org/10.3390/nu14142898
AL-Musharaf S, AlAjllan L, Aljuraiban G, AlSuhaibani M, Alafif N, Hussain SD. Nutritional Biomarkers and Factors Correlated with Poor Sleep Status among Young Females: A Case-Control Study. Nutrients. 2022; 14(14):2898. https://doi.org/10.3390/nu14142898
Chicago/Turabian StyleAL-Musharaf, Sara, Lama AlAjllan, Ghadeer Aljuraiban, Munirah AlSuhaibani, Noura Alafif, and Syed Danish Hussain. 2022. "Nutritional Biomarkers and Factors Correlated with Poor Sleep Status among Young Females: A Case-Control Study" Nutrients 14, no. 14: 2898. https://doi.org/10.3390/nu14142898