
Relationship of Daily Coffee Intake with Vascular Function in Patients with Hypertension

 and
and
Abstract
:
1. Introduction
2. Materials and Methods
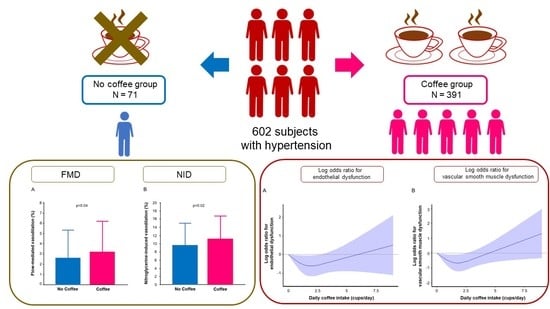
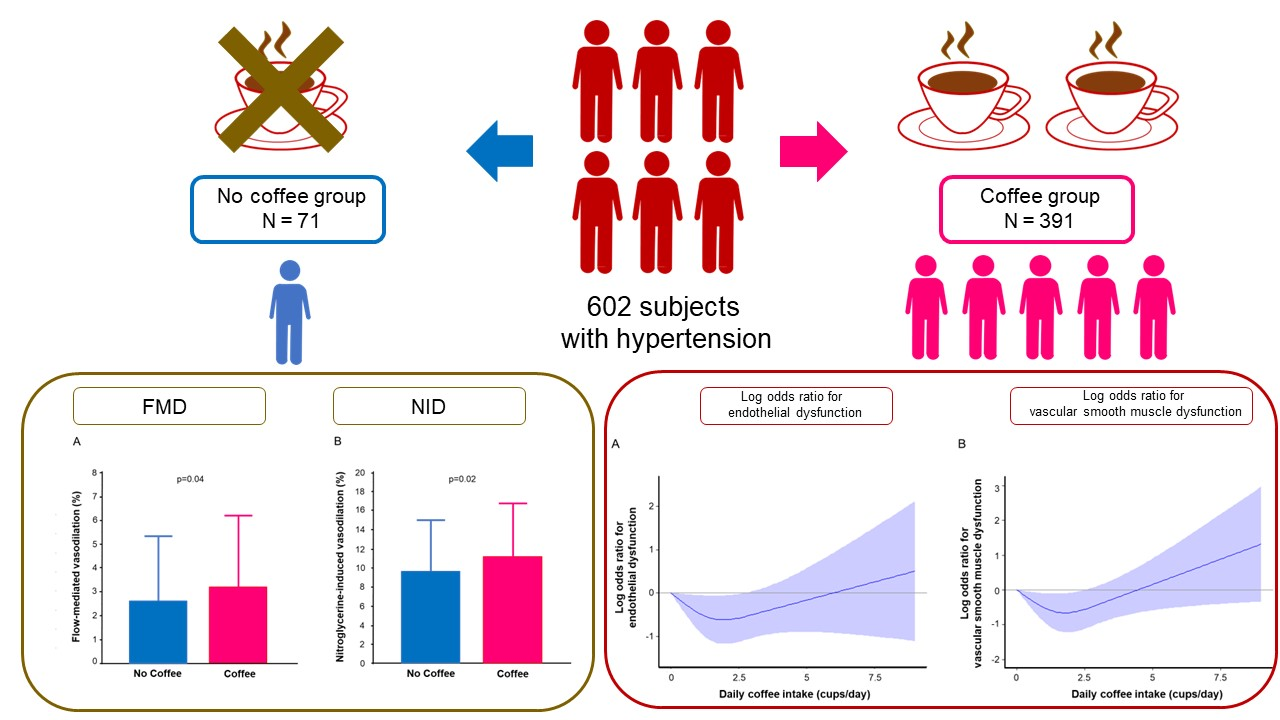
2.1. Study Subjects
2.2. Study Protocol
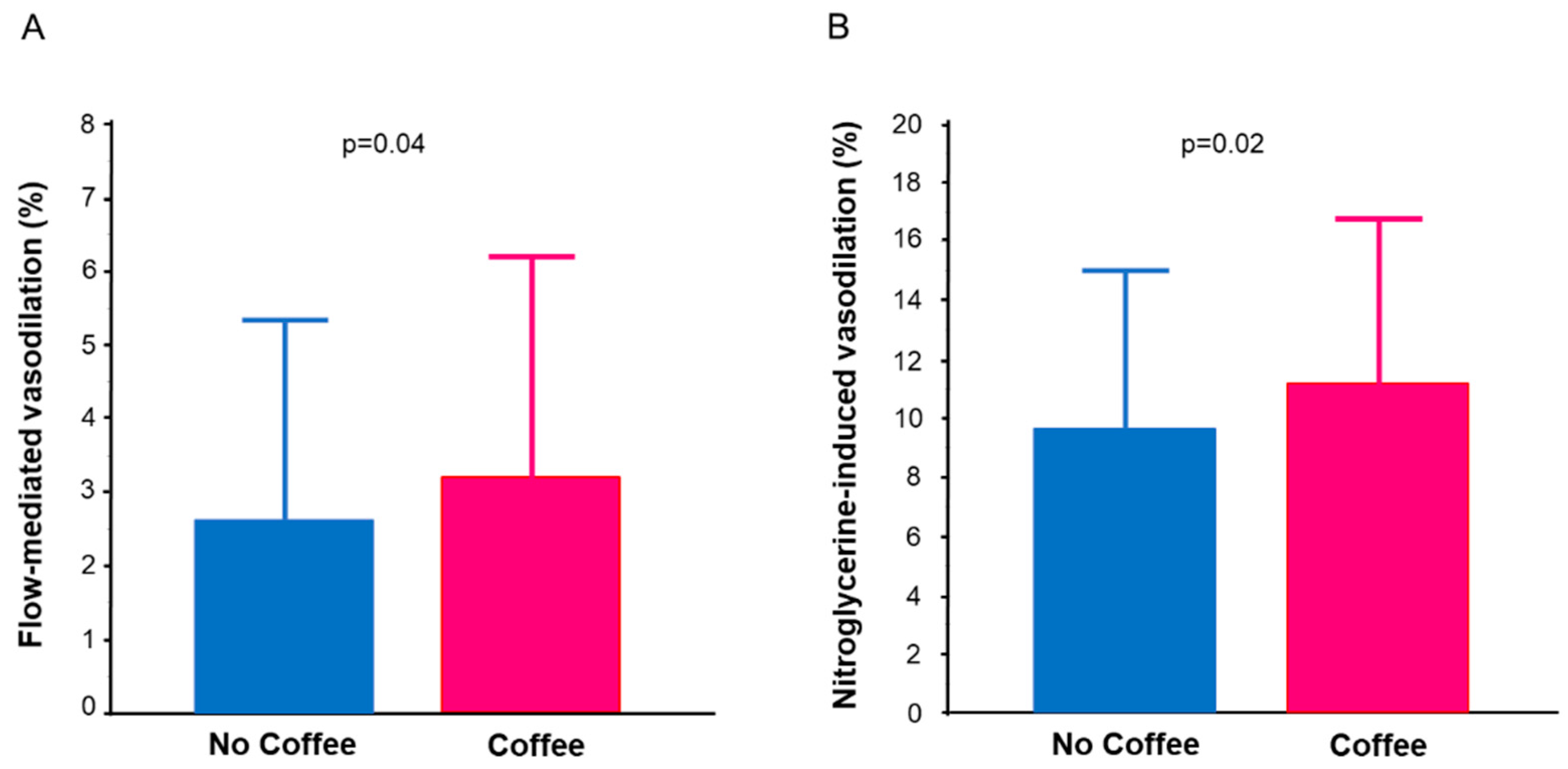
2.3. Measurements of FMD and NID
2.4. Evaluation of Daily Coffee Intake
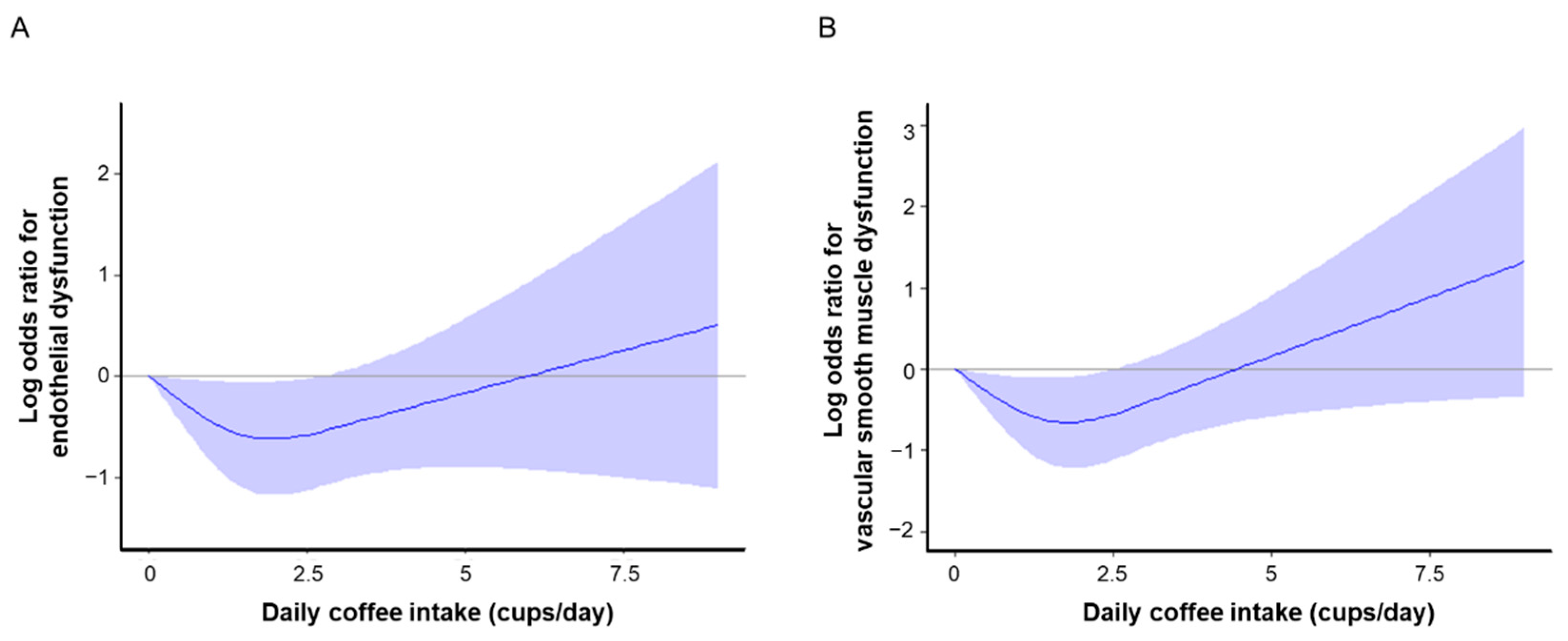
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Subjects
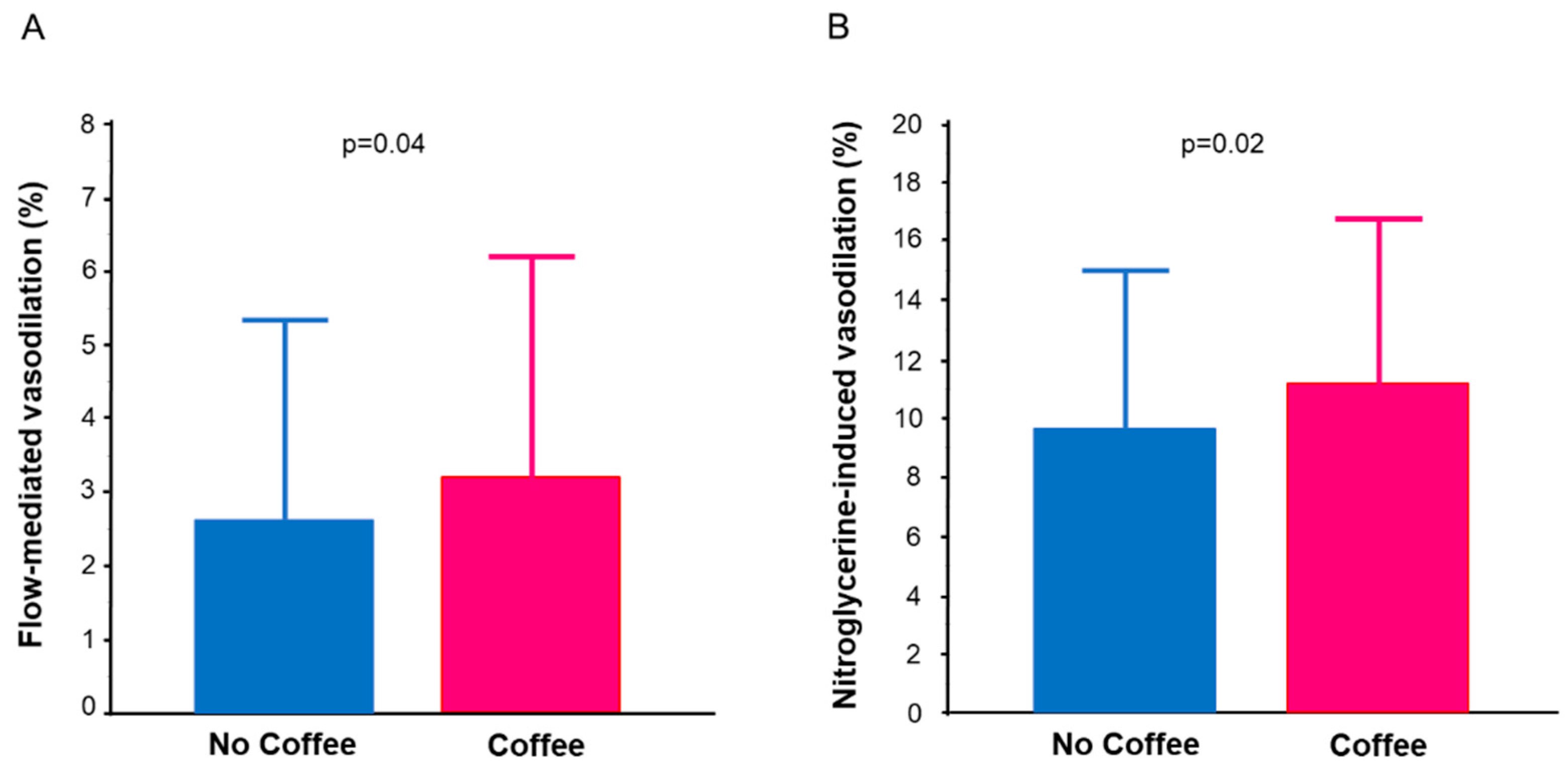
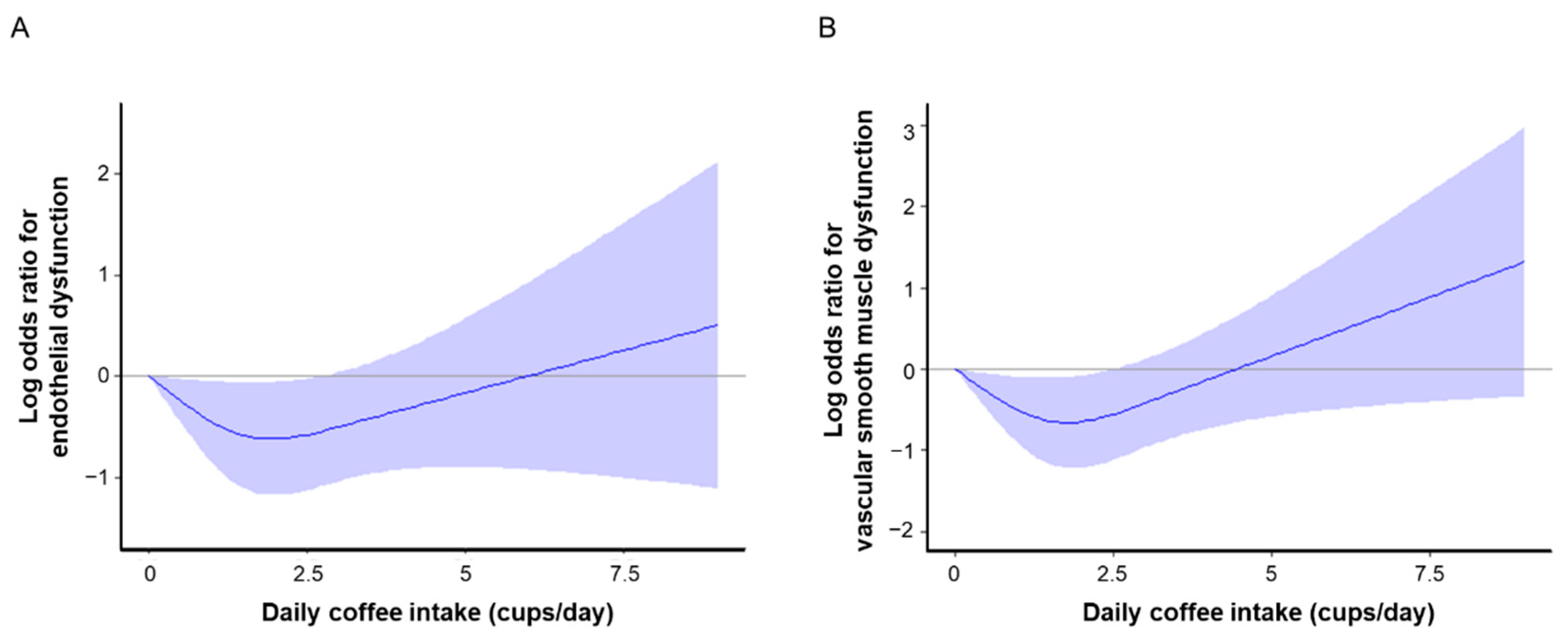
3.2. Vascular Function in the No Coffee Group and Coffee Group
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Minzer, S.; Losno, R.A.; Casas, R. The Effect of Alcohol on Cardiovascular Risk Factors: Is There New Information? Nutrients 2020, 12, 912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathers, C.D.; Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poole, R.; Kennedy, O.J.; Roderick, P.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Coffee consumption and health: Umbrella review of meta-analyses of multiple health outcomes. BMJ 2017, 359, j5024. [Google Scholar] [CrossRef] [Green Version]
- Fouad, H.; Commar, A.; Hamadeh, R.; El-Awa, F.; Shen, Z.; Fraser, C. Estimated and projected prevalence of tobacco smoking in males, Eastern Mediterranean Region, 2000–2025. East. Mediterr. Health J. 2021, 27, 76–82. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Alcohol. Available online: https://www.who.int/news-room/fact-sheets/detail/alcohol (accessed on 21 September 2018).
- Freedman, N.D.; Park, Y.; Abnet, C.C.; Hollenbeck, A.R.; Sinha, R. Association of coffee drinking with total and cause-specific mortality. N. Engl. J. Med. 2012, 366, 1891–1904. [Google Scholar] [CrossRef] [PubMed]
- Coffee, tea, mate, methylxanthines and methylglyoxal. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Lyon, 27 February to 6 March 1990. IARC Monogr. Eval. Carcinog. Risks Hum. 1991, 51, 1–513.
- Loomis, D.; Guyton, K.Z.; Grosse, Y.; Lauby-Secretan, B.; El Ghissassi, F.; Bouvard, V.; Benbrahim-Tallaa, L.; Guha, N.; Mattock, H.; Straif, K. Carcinogenicity of drinking coffee, mate, and very hot beverages. Lancet Oncol. 2016, 17, 877–878. [Google Scholar] [CrossRef]
- LaCroix, A.Z.; Mead, L.A.; Liang, K.Y.; Thomas, C.B.; Pearson, T.A. Coffee consumption and the incidence of coronary heart disease. N. Engl. J. Med. 1986, 315, 977–982. [Google Scholar] [CrossRef] [Green Version]
- Happonen, P.; Voutilainen, S.; Salonen, J.T. Coffee drinking is dose-dependently related to the risk of acute coronary events in middle-aged men. J. Nutr. 2004, 134, 2381–2386. [Google Scholar] [CrossRef]
- Wu, J.N.; Ho, S.C.; Zhou, C.; Ling, W.H.; Chen, W.Q.; Wang, C.L.; Chen, Y.M. Coffee consumption and risk of coronary heart diseases: A meta-analysis of 21 prospective cohort studies. Int. J. Cardiol. 2009, 137, 216–225. [Google Scholar] [CrossRef]
- Lopez-Garcia, E.; Rodriguez-Artalejo, F.; Rexrode, K.M.; Logroscino, G.; Hu, F.B.; van Dam, R.M. Coffee consumption and risk of stroke in women. Circulation 2009, 119, 1116–1123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Z.; Hu, G.; Caballero, B.; Appel, L.; Chen, L. Habitual coffee consumption and risk of hypertension: A systematic review and meta-analysis of prospective observational studies. Am. J. Clin. Nutr. 2011, 93, 1212–1219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Keefe, J.H.; Bhatti, S.K.; Patil, H.R.; DiNicolantonio, J.J.; Lucan, S.C.; Lavie, C.J. Effects of habitual coffee consumption on cardiometabolic disease, cardiovascular health, and all-cause mortality. J. Am. Coll. Cardiol. 2013, 62, 1043–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hakim, A.A.; Ross, G.W.; Curb, J.D.; Rodriguez, B.L.; Burchfiel, C.M.; Sharp, D.S.; Yano, K.; Abbott, R.D. Coffee consumption in hypertensive men in older middle-age and the risk of stroke: The Honolulu Heart Program. J. Clin. Epidemiol. 1998, 51, 487–494. [Google Scholar] [CrossRef]
- Larsson, S.C.; Virtamo, J.; Wolk, A. Coffee consumption and risk of stroke in women. Stroke 2011, 42, 908–912. [Google Scholar] [CrossRef] [Green Version]
- Vane, J.R.; Anggård, E.E.; Botting, R.M. Regulatory functions of the vascular endothelium. N. Engl. J. Med. 1990, 323, 27–36. [Google Scholar] [CrossRef]
- Higashi, Y.; Noma, K.; Yoshizumi, M.; Kihara, Y. Endothelial function and oxidative stress in cardiovascular diseases. Circ. J. Off. J. Jpn. Circ. Soc. 2009, 73, 411–418. [Google Scholar] [CrossRef] [Green Version]
- Matsui, S.; Kajikawa, M.; Hida, E.; Maruhashi, T.; Iwamoto, Y.; Iwamoto, A.; Oda, N.; Kishimoto, S.; Hidaka, T.; Kihara, Y.; et al. Optimal Target Level of Low-density Lipoprotein Cholesterol for Vascular Function in Statin Naïve Individuals. Sci. Rep. 2017, 7, 8422. [Google Scholar] [CrossRef] [Green Version]
- Yamaji, T.; Harada, T.; Hashimoto, Y.; Takaeko, Y.; Kajikawa, M.; Kihara, Y.; Hida, E.; Chayama, K.; Goto, C.; Han, Y.; et al. Pre-impaired fasting glucose state is a risk factor for endothelial dysfunction: Flow-mediated Dilation Japan (FMD-J) study. BMJ Open Diabetes Res. Care 2020, 8, e001610. [Google Scholar] [CrossRef]
- Maruhashi, T.; Soga, J.; Fujimura, N.; Idei, N.; Mikami, S.; Iwamoto, Y.; Kajikawa, M.; Matsumoto, T.; Hidaka, T.; Kihara, Y.; et al. Relationship between flow-mediated vasodilation and cardiovascular risk factors in a large community-based study. Heart 2013, 99, 1837–1842. [Google Scholar] [CrossRef]
- Hashimoto, H.; Maruhashi, T.; Yamaji, T.; Harada, T.; Han, Y.; Takaeko, Y.; Kihara, Y.; Chayama, K.; Goto, C.; Aibara, Y.; et al. Smoking status and endothelial function in Japanese men. Sci. Rep. 2021, 11, 95. [Google Scholar] [CrossRef] [PubMed]
- Maruhashi, T.; Soga, J.; Fujimura, N.; Idei, N.; Mikami, S.; Iwamoto, Y.; Kajikawa, M.; Matsumoto, T.; Hidaka, T.; Kihara, Y.; et al. Nitroglycerine-induced vasodilation for assessment of vascular function: A comparison with flow-mediated vasodilation. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1401–1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsui, S.; Kajikawa, M.; Maruhashi, T.; Iwamoto, Y.; Iwamoto, A.; Oda, N.; Kishimoto, S.; Hidaka, T.; Kihara, Y.; Chayama, K.; et al. Decreased frequency and duration of tooth brushing is a risk factor for endothelial dysfunction. Int. J. Cardiol. 2017, 241, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Yamaji, T.; Harada, T.; Hashimoto, Y.; Nakano, Y.; Kajikawa, M.; Yoshimura, K.; Chayama, K.; Goto, C.; Han, Y.; Mizobuchi, A.; et al. Stair climbing activity and vascular function in patients with hypertension. Hypertens. Res. 2021, 44, 1274–1282. [Google Scholar] [CrossRef]
- Lopez-Garcia, E.; Rodriguez-Artalejo, F.; Li, T.Y.; Mukamal, K.J.; Hu, F.B.; van Dam, R.M. Coffee consumption and mortality in women with cardiovascular disease. Am. J. Clin. Nutr. 2011, 94, 218–224. [Google Scholar] [CrossRef]
- Kajikawa, M.; Maruhashi, T.; Hidaka, T.; Nakano, Y.; Kurisu, S.; Matsumoto, T.; Iwamoto, Y.; Kishimoto, S.; Matsui, S.; Aibara, Y.; et al. Coffee with a high content of chlorogenic acids and low content of hydroxyhydroquinone improves postprandial endothelial dysfunction in patients with borderline and stage 1 hypertension. Eur. J. Nutr. 2019, 58, 989–996. [Google Scholar] [CrossRef] [Green Version]
- Molnar, J.; Somberg, J.C. Evaluation of the Effects of Different Energy Drinks and Coffee on Endothelial Function. Am. J. Cardiol. 2015, 116, 1457–1460. [Google Scholar] [CrossRef]
- Agudelo-Ochoa, G.M.; Pulgarín-Zapata, I.C.; Velásquez-Rodriguez, C.M.; Duque-Ramírez, M.; Naranjo-Cano, M.; Quintero-Ortiz, M.M.; Lara-Guzmán, O.J.; Muñoz-Durango, K. Coffee Consumption Increases the Antioxidant Capacity of Plasma and Has No Effect on the Lipid Profile or Vascular Function in Healthy Adults in a Randomized Controlled Trial. J. Nutr. 2016, 146, 524–531. [Google Scholar] [CrossRef] [Green Version]
- Buscemi, S.; Verga, S.; Batsis, J.A.; Donatelli, M.; Tranchina, M.R.; Belmonte, S.; Mattina, A.; Re, A.; Cerasola, G. Acute effects of coffee on endothelial function in healthy subjects. Eur. J. Clin. Nutr. 2010, 64, 483–489. [Google Scholar] [CrossRef] [Green Version]
- Papamichael, C.M.; Aznaouridis, K.A.; Karatzis, E.N.; Karatzi, K.N.; Stamatelopoulos, K.S.; Vamvakou, G.; Lekakis, J.P.; Mavrikakis, M.E. Effect of coffee on endothelial function in healthy subjects: The role of caffeine. Clin. Sci. 2005, 109, 55–60. [Google Scholar] [CrossRef] [Green Version]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robertson, D.; Frölich, J.C.; Carr, R.K.; Watson, J.T.; Hollifield, J.W.; Shand, D.G.; Oates, J.A. Effects of caffeine on plasma renin activity, catecholamines and blood pressure. N. Engl. J. Med. 1978, 298, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Dobmeyer, D.J.; Stine, R.A.; Leier, C.V.; Greenberg, R.; Schaal, S.F. The arrhythmogenic effects of caffeine in human beings. N. Engl. J. Med. 1983, 308, 814–816. [Google Scholar] [CrossRef]
- Nawrot, P.; Jordan, S.; Eastwood, J.; Rotstein, J.; Hugenholtz, A.; Feeley, M. Effects of caffeine on human health. Food Addit. Contam. 2003, 20, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, S.; Majhi, S.; Saha, B.P.; Mukherjee, P.K. Chlorogenic acid-phospholipid complex improve protection against UVA induced oxidative stress. J. Photochem. Photobiol. B 2014, 130, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.C.; Liou, S.S.; Tzeng, T.F.; Lee, S.L.; Liu, I.M. Effect of topical application of chlorogenic acid on excision wound healing in rats. Planta Med. 2013, 79, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Higashi, Y. Coffee and Endothelial Function: A Coffee Paradox? Nutrients 2019, 11, 2104. [Google Scholar] [CrossRef] [Green Version]
- Saito, E.; Inoue, M.; Sawada, N.; Shimazu, T.; Yamaji, T.; Iwasaki, M.; Sasazuki, S.; Noda, M.; Iso, H.; Tsugane, S. Association of coffee intake with total and cause-specific mortality in a Japanese population: The Japan Public Health Center-based Prospective Study. Am. J. Clin. Nutr. 2015, 101, 1029–1037. [Google Scholar] [CrossRef] [Green Version]
- Zhou, A.; Hyppönen, E. Long-term coffee consumption, caffeine metabolism genetics, and risk of cardiovascular disease: A prospective analysis of up to 347,077 individuals and 8368 cases. Am. J. Clin. Nutr. 2019, 109, 509–516. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 462) | No Coffee (n = 71) | Coffee (n = 391) | p Value |
|---|---|---|---|---|
| Age, year | 65 ± 13 | 67 ± 13 | 64 ± 13 | 0.08 |
| Men, n (%) | 274 (59.7) | 51 (71.8) | 223 (57.5) | 0.02 |
| Body mass index, kg/m2 | 24.4 ± 3.8 | 24.5 ± 3.8 | 24.4 ± 3.7 | 0.84 |
| Heart rate, bpm | 69 ± 11 | 70 ± 14 | 69 ± 11 | 0.49 |
| Systolic blood pressure, mmHg | 130 ± 17 | 133 ± 20 | 129 ± 16 | 0.10 |
| Diastolic blood pressure, mmHg | 79 ± 12 | 81 ± 12 | 78 ± 12 | 0.10 |
| Total cholesterol, mmol/L | 4.91 ± 0.93 | 4.73 ± 0.88 | 4.94 ± 0.93 | 0.12 |
| Triglycerides, mmol/L | 1.28 (0.93, 1.81) | 1.31 (0.86, 1.87) | 1.26 (0.94, 1.80) | 0.63 |
| High-density lipoprotein cholesterol, mmol/L | 1.55 ± 0.41 | 1.55 ± 0.39 | 1.55 ± 0.44 | 0.97 |
| Low-density lipoprotein cholesterol, mmol/L | 2.79 ± 0.78 | 2.61 ± 0.75 | 2.84 ± 0.78 | 0.04 |
| Creatinine, mmol/L | 71.6 (61.0, 85.8) | 84.9 (64.5, 97.2) | 70.7 (60.1, 84.6) | <0.01 |
| Glucose, mmol/L | 5.94 ± 1.28 | 5.88 ± 1.33 | 5.94 ± 1.28 | 0.73 |
| Hemoglobin A1c, % | 5.9 ± 0.9 | 5.8 ± 1.3 | 5.9 ± 0.8 | 0.59 |
| Medical history, n (%) | ||||
| Dyslipidemia | 301 (65.2) | 48 (67.6) | 253 (64.7) | 0.64 |
| Diabetes mellitus | 135 (29.2) | 14 (19.7) | 121 (31.0) | 0.048 |
| Cardiovascular disease, n (%) | 94 (20.6) | 23 (32.4) | 71 (18.4) | <0.01 |
| Smoker, n (%) | 252 (54.7) | 39 (54.9) | 213 (54.6) | 0.96 |
| Medication, n (%) | ||||
| Antihypertensive drugs | 421 (91.9) | 65 (92.9) | 356 (91.8) | 0.75 |
| Lipid-lowering drugs | 190 (62.5) | 30 (62.5) | 160 (62.5) | 1.00 |
| Anti-diabetic drugs | 130 (28.1) | 14 (19.7) | 116 (29.7) | 0.09 |
| Odds Ratio (95% Confidence Interval); p Value | |||||
|---|---|---|---|---|---|
| Coffee | Unadjusted | Model 1 | Model 2 | Model 3 | Model 4 |
| No coffee | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| Coffee | 0.57 (0.34–0.95); 0.03 | 0.58 (0.34–0.99); 0.04 | 0.56 (0.33–0.96); 0.04 | 0.55 (0.32–0.95); 0.03 | 0.55 (0.32–0.95); 0.03 |
| Odds ratio (95% Confidence Interval); p Value | |||||
|---|---|---|---|---|---|
| Coffee | Unadjusted | Model 1 | Model 2 | Model 3 | Model 4 |
| No coffee | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| Coffee | 0.51 (0.30–0.86); 0.01 | 0.49 (0.28–0.84); 0.01 | 0.45 (0.25–0.78); <0.01 | 0.49 (0.27–0.87); 0.02 | 0.50 (0.28–0.89); 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamaji, T.; Harada, T.; Hashimoto, Y.; Nakano, Y.; Kajikawa, M.; Yoshimura, K.; Goto, C.; Mizobuchi, A.; Tanigawa, S.; Yusoff, F.M.; et al. Relationship of Daily Coffee Intake with Vascular Function in Patients with Hypertension. Nutrients 2022, 14, 2719. https://doi.org/10.3390/nu14132719
Yamaji T, Harada T, Hashimoto Y, Nakano Y, Kajikawa M, Yoshimura K, Goto C, Mizobuchi A, Tanigawa S, Yusoff FM, et al. Relationship of Daily Coffee Intake with Vascular Function in Patients with Hypertension. Nutrients. 2022; 14(13):2719. https://doi.org/10.3390/nu14132719
Chicago/Turabian StyleYamaji, Takayuki, Takahiro Harada, Yu Hashimoto, Yukiko Nakano, Masato Kajikawa, Kenichi Yoshimura, Chikara Goto, Aya Mizobuchi, Shunsuke Tanigawa, Farina Mohamad Yusoff, and et al. 2022. "Relationship of Daily Coffee Intake with Vascular Function in Patients with Hypertension" Nutrients 14, no. 13: 2719. https://doi.org/10.3390/nu14132719
APA StyleYamaji, T., Harada, T., Hashimoto, Y., Nakano, Y., Kajikawa, M., Yoshimura, K., Goto, C., Mizobuchi, A., Tanigawa, S., Yusoff, F. M., Kishimoto, S., Maruhashi, T., Nakashima, A., & Higashi, Y. (2022). Relationship of Daily Coffee Intake with Vascular Function in Patients with Hypertension. Nutrients, 14(13), 2719. https://doi.org/10.3390/nu14132719