
Chokeberry (A. melanocarpa (Michx.) Elliott)—A Natural Product for Metabolic Disorders?




Abstract
:1. Introduction
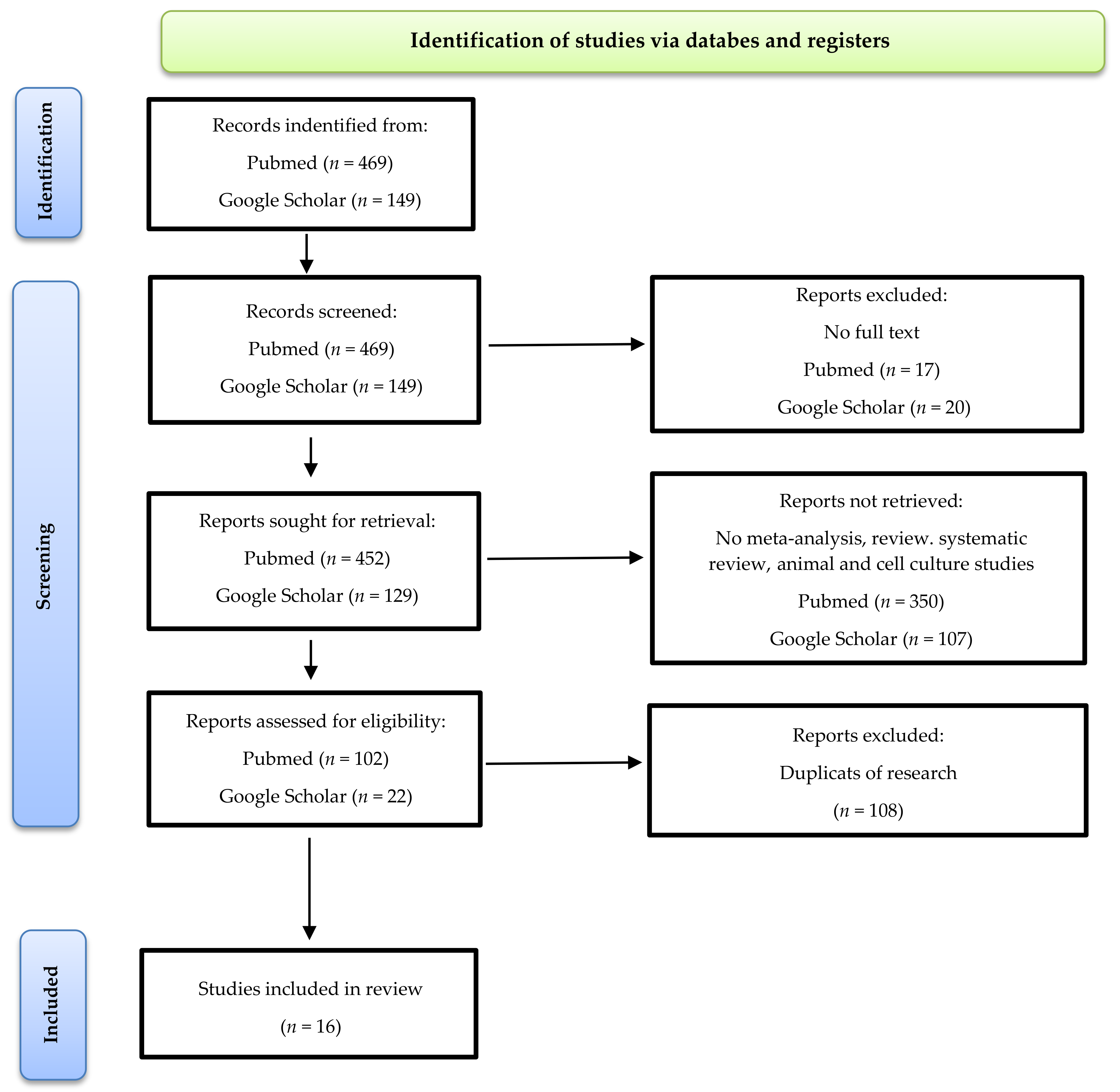
2. Materials and Methods
3. Results and Discussion
3.1. Impact of Chokeberry on Anthropometric Measurements

{kind=link}
{kind=link}
| Number of Participants (n) (Women/Men) | Characteristics of the Group | Type of Chokeberry Product | Dose of Chokeberry Product per Day | Time of Intervention (Weeks) | Changes in Diet | Results | References |
|---|---|---|---|---|---|---|---|
| n = 44 (11/33) | Myocardial infarctionand statin therapy for at least 6 months (mean age 66, BMI 26.5 kg/m2) | Chokeberry flavonoid extract (Aronox, Agropharm, Pieńków, Poland) | 3 × 85 mg | 6 | No changes | BMI↔ | [78] |
| n = 47 (32/15) | MetS (n = 25, age 42–65, BMI 31.05 kg/m2) Healthy (n = 22, BMI 24.15 kg/m2) | Chokeberry extract (Aronox, Agropharm, Pieńków, Poland) | 3 × 100 mg | 8 | No changes | BMI↔, WC↔ | [77] |
| n = 52 (31/21) | MetS (n = 38, age 42–65, BMI 31.1 kg/m2), healthy (n = 14, age 42–65, BMI 24.4 kg/m2) | Chokeberry extract (Agropharm, Pieńków, Poland) | 3 × 100 mg | 8 | Low-fat diet | BMI↔, WC↔ | [74] |
| n = 70 (42/28) | Group I: patients with MetS who received chokeberry extract supplements (n = 25, age 50–69, BMI 30.9 kg/m2) Group II: healthy—control group (n = 45, age 55–71, BMI 23 kg/m2) Group III: patients with MetS treated with ACE inhibitors—control group (n = 25, age 50–69, BMI 29.2 kg/m2) | Chokeberry extract (Aronox, Agropharm, Pieńków, Poland) | 3 × 100 mg | 8 | No changes (inhibition product containing chokeberry) | BMI↔, WC↔ | [75] |
| n = 20 (20/0) | Postmenopausal women with abdominal obesity (WC > 88 cm, age 45–65, BMI 36.1 kg/m2) | Chokeberry supplement (Nutrika d.o.o., Belgrade, Serbia), prepared from pure chokeberry juice enriched with 2 g of stable glucomannan fibers (Luralean, Shimizu, Japan) | 100 mL | 4 | No changes | BMI↓, WC↓ BW↔ | [72] |
| n = 38 (24/14) | Mildly elevated BP, SBP 130–159 mmHg, DBP 85–99 mmHg (mean age 55.8, BMI < 35 kg/m2) | Cold-pressed 100% chokeberry juice (Kiantama Ltd., Suomussalmi, Finland) or convection oven-dried chokeberry powder (Finnish Berry Powders Ltd., Ähtäri, Finland) | 300 mL chokeberry juice or 3 g dried chokeberry powder | 8 | No changes | BMI↔, BW↔ | [76] |
| n = 84 (52/32) | Subjects with cardiovascular risks (mean age 40.6, BMI 27.29 kg/m2) | Chokeberry juice with a high-dose of polyphenols and chokeberry juice with a low-dose of polyphenols (Nutrika Ltd., Belgrade, Serbia) | 100 mL | 4 | Avoiding excessive quantities of other foods rich in polyphenols | Low-dose of polyphenols group: BMI↔ High-dose of polyphenols group: BMI↔ | [73] |
| n = 144 (74/70) | MetS according to the AHA guidelines (age 50–60, BMI 30.1–34.4 kg/m2) I. n = 42, fMetS II. n = 42, mMetS III. n = 32, fMetS-DM IV. n = 28, mMetS-DM | Standarized chokeberry extract (Alixir 400 PROTECT, Pharmanova, Belgrade, Serbia) | 30 mL of extract (prior or during dinner) | 4 | No changes | fMetS: BW↓, WC↓, BMI↔ mMetS: BW↓, WC↓, BMI↔ fMetS-DM: BW↓, WC↓, BMI↔ mMetS-DM: BW↓, WC↓, BMI↓ | [71] |
3.2. Impact of Chokeberry on Carbohydrate Metabolism
| Number of Participants (n) (Women/Men) | Characteristics of the Group | Type of Chokeberry Product | Dose of Chokeberry Product per Day | Time of Intervention (Weeks) | Changes in Diet | Results | References |
|---|---|---|---|---|---|---|---|
| n = 44 (11/33) | Myocardial infarction and statin therapy for at least 6 months (mean age 66, BMI 26.5 kg/m2) | Chokeberry flavonoid extract (Aronox, Agropharm, Pieńków, Poland) | 3 × 85 mg | 6 | No changes | glucose ↔ adiponectin↑ | [78] |
| n = 58 (0/58) | Mild hypocholesterolemia (TC > 200 mg/dL) without pharmacological treatment (mean age 54.1, BMI 27.7 kg/m2) without DM2 | Organic chokebery juice (A. M. Lech, Dzieciolowo, Poland) | 250 mL | 18 (12 weeks with drinking chokeberry juice) | No changes | glucose↓ | [103] |
| n = 47 (32/15) | MetS (n = 25, age 42–65, BMI 31.05 kg/m2) without DM2, healthy (n = 22, BMI 24.15 kg/m2) | Chokeberry extract (Aronox, Agropharm, Pieńków, Poland) | 3 × 100 mg | 8 | No changes | glucose↔ | [77] |
| n = 1 | Hypercholesterolemia, arterial hypertension, and deregulated protein metabolism (67 years old) without DM2 | Alcoholic extract of crude chokeberry fruits (10%) | 30 mL | 10 | nd | glucose level↔ | [102] |
| n = 20 (20/0) | Postmenopausal women with abdominal obesity (WC > 88 cm, age 45–65, BMI 36.1 kg/m2) | Chokeberry supplement (Nutrika d.o.o., Belgrade, Serbia), prepared from pure chokeberry juice enriched with 2 g of stable glucomannan fibers (Luralean, Shimizu, Japan) | 100 mL | 4 | No changes | glucose↔ | [72] |
| n =23 (11/12) | High normal BP or grade I hypertension: SBP = 130–159 mmHg, DBP = 85–99 mmHg, no regular use of antihypertensive drugs was declared by 23 patients (mean age 47.5, BMI nd) | Organic chokeberry juice (Conimex Trade d.o.o., Belgrade, Serbia) | 200 mL | 4 | No changes | glucose↔ | [79] |
| n = 38 (24/14) | Mildly elevated BP: SBP 130–159 mmHg, DBP 85–99 mmHg (mean age 55.8, BMI < 35 kg/m2) without DM2 | Cold-pressed 100% chokeberry juice (Kiantama Ltd., Finland) or convection oven-dried chokeberry powder (Finnish Berry Powders Ltd., Finland) | 300 mL chokeberry juice or 3 g dried chokeberry powder | 8 | No changes | glucose↔ | [76] |
| n = 35 (23/12) | DM2 and oral antidiabetic drugs therapy for at least 6 months (mean age 56.3, BMI 28.8 kg/m2) | Chokeberry juice (Nutrica d.o.o., Belgrade, Serbia) | 150 mL (three times daily for 50 mL) | 12 | No changes | glucose↓, HbA1c↓ | [100] |
| n = 144 (74/70) | MetS according to the AHA guidelines (age 50–60, BMI 30.1–34.4 kg/m2) I. n = 42, fMetS II. n = 42, mMetS III. n = 32, fMetS-DM IV. n = 28, mMetS-DM | Standarized chokeberry extract (Alixir 400 PROTECT, Pharmanova, Belgrade, Serbia) | 30 mL (prior or during dinner) | 4 | No changes | fMetS: glucose↔ mMetS: glucose↑ fMetS-DM: glucose↓ mMetS-DM: glucose↓ | [71] |
| n = 22 (13/9) | Overweight (n = 11, mean age 51.9, BMI 25–30 kg/m2), healthy (n = 11, mean age 41.4, BMI 18–25 kg/m2) | Chokeberry juice (Aronia Alive Agriculture Ltd., Sofia, Bulgaria) | 150 mL (50 mL, three times daily before meals) | 12 | nd | FPG↓, HbA1c↓ | [104] |
3.3. Impact of Chokeberry on Blood Pressure
| Number of Participants (n) (Women/Men) | Characteristics of the Group | Type of Chokeberry Product | Dose of Chokeberry Product per Day | Time of Intervention (Weeks) | Changes in Diet | Results | References |
|---|---|---|---|---|---|---|---|
| n = 44 (11/33) | Myocardialinfarction and statin therapy for at least 6 months (mean age 66, BMI 26.5 kg/m2) | Chokeberry flavonoid extract (Aronox, Agropharm, Pieńków, Poland) | 3 × 85 mg | 6 | No changes | SBP↓, DBP↓ | [78] |
| n = 58 (0/58) | Mild hypocholesterolemia (TC > 200 mg/dL) without pharmacological treatment (mean age 54.1, BMI 27.7 kg/m2) | Organic chokebery juice (A. M. Lech, Dzieciolowo, Poland) | 250 mL | 18 (12 weeks with drinking chokeberry juice) | No changes | SBP↓, DBP↓ | [103] |
| n = 47 (32/15) | MetS (n = 25, age 42–65, BMI 31.05 kg/m2), healthy (n = 22, BMI 24.15 kg/m2) | Chokeberry extract (Aronox, Agropharm, Pieńków, Poland) | 3 × 100 mg | 8 | No changes | SBP↓, DBP↓ endthoteline-1↓ | [77] |
| n = 70 (42/28) | Group I: patients with MetS who received chokeberry extract supplements (n = 25, age 50–69, BMI 30.9 kg/m2) Group II: healthy—control group (n = 45, age 55–71, BMI 23 kg/m2) Group III: patients with MetS treated with ACE inhibitors—control group (n = 25, age 50–69, BMI 29.2 kg/m2) | Chokeberry extract (Aronox, Agropharm, Pieńków, Poland) | 3 × 100 mg | 8 | No changes (inhibition product containing chokeberry) | SBP↓, DBP↓, ACE↓ | [75] |
| n = 20 (20/0) | Postmenopausal women withabdominal obesity (WC > 88 cm, age 45–65, BMI 36.1 kg/m2) | Chokeberry supplement (Nutrika d.o.o., Belgrade, Serbia), prepared from pure chokeberry juice enriched with 2 g of stable glucomannan fibers (Luralean, Shimizu, Japan) | 100 mL | 4 | No changes | SBP↓, DBP↔ | [72] |
| n = 23 (11/12) | High normal BP or grade I hypertension: SBP = 130–159 mmHg, DBP = 85–99 mmHg, no regular use of antihypertensive drugs (mean age 47.5, BMI nd) | Organic chokeberry juice (Conimex Trade d.o.o., Belgrade, Serbia) | 200 mL | 4 | No changes | 24 h SBP↓, 24 h DBP↔, awake SBP↓, awake DBP↓, sleep SBP↔, sleep DBP↔ 24 h pulse blood pressure↔, sleep pulse blood pressure↔, awake pulse blood pressure↓ | [79] |
| n = 38 (24/14) | Mildly elevated BP: SBP 130–159 mmHg, DBP 85–99 mmHg (mean age 55.8, BMI < 35 kg/m2) without DM2 | Cold-pressed 100% chokeberry juice (Kiantama Ltd., Finland) or convection oven-dried chokeberry powder (Finnish Berry Powders Ltd., Finland) | 300 mL chokeberry juice or 3 g dried chokeberry powder | 8 | No changes | daytime ambulatory DBP↓ 24 h SBP/DBP↔, daytime ambulatory SBP↔, night SBP/DBP↔, awake SBP/DBP↔, sleep SBP/DBP↔ | [76] |
| n = 35 (23/12) | DM2 and oral antidiabetic drugs therapy for at least 6 months (mean age 56.3, BMI 28.8 kg/m2) | Chokeberry juice (Nutrica d.o.o., Belgrade, Serbia) | 150 mL (three times daily for 50 mL) | 12 | No changes | SBP↔, DBP↔ | [100] |
| n = 84 (52/32) | Subjects with cardiovascular risks (mean age 40.6, BMI 27.29 kg/m2) | Chokeberry juice with a high dose of polyphenols and chokeberry juice with a low dose of polyphenols (Nutrika LTD, Belgrade, Serbia) | 100 mL | 4 | Avoiding excessive quantities of other foods rich in polyphenols | low-dose of polyphenols group: SBP↔, DBP↔ high-dose of polyphenols group: SBP↓, DBP↓ | [73] |
| n = 144 (74/70) | MetS according to the AHA guidelines (age 50–60, BMI 30.1–34.4 kg/m2) I. n = 42, fMetS II. n = 42, mMetS III. n = 32, fMetS-DM IV. n = 28, mMetS-DM | Standarized chokeberry extract (Alixir 400 PROTECT, Pharmanova, Belgrade, Serbia) | 30 mL of extract (prior or during dinner) | 4 | No changes | fMetS: SBP↓, DBP↓, HR↔ mMetS: SBP↓, DBP↓, HR↔ fMetS-DM: SBP↓, DBP↓, HR↔ mMetS-DM: SBP↓, DBP↓, HR↔ | [71] |
3.4. Impact of Chokeberry on Lipid Profile
| Number of Participants (n) (Women/Men) | Characteristics of the Group | Type of Chokeberry Product | Dose of Chokeberry Product per Day | Time of Intervention (Weeks) | Changes in Diet | Results | References |
|---|---|---|---|---|---|---|---|
| n = 44 (11/33) | Myocardial infarction and statin therapy for at least 6 months in 44 patients (mean age 66, BMI 26.5 kg/m2) | Chokeberry flavonoid extract (Aronox, Agropharm, Pieńków, Poland) | 3 × 85 mg | 6 | No changes | TC↔, LDL-C↔, HDL-C↔, TG↔, homocysteine↔ | [78] |
| n = 58 (0/58) | Mild hypocholesterolemia (TC > 200 mg/dL) without pharmacological treatment (mean age 54.1, BMI 27.7 kg/m2) | Organic chokebery juice (A. M. Lech, Dzieciolowo, Poland) | 250 mL | 18 (12 weeks with drinking chokeberry juice) | No changes | TC↓ LDL-C↓ TG↓ homocysteine↓ | [103] |
| n = 47 (32/15) | MetS (n = 25, age 42–65, BMI 31.05 kg/m2), healthy (n = 22, BMI 24.15 kg/m2) | Chokeberry extract (Agropharm, Pieńków, Poland) | 3 × 100 mg | 8 | No changes | TC↓ LDL-C↓ TG↓ | [77] |
| n = 45 (31/14) | Hypercholesterolemia without pharmacological treatment (n = 25, mean age 55.9,BMI nd), healthy (n = 20, mean age 50.3, BMI nd) | Chokeberry extract (Aronox, Agropharm, Pieńków, Poland) | 3 × 100 mg | 8 | No changes | erythrocytes: TC↓ lipid peroxidation↓ TBARS↓ | [148] |
| n = 1 | Hypercholesterolemia, arterial hypertension, and deregulated protein metabolism (67 years old) without DM2 | Alcoholic extract of crude chokeberry fruits (10%) | 30 mL | 10 | nd | TC↓ LDL-C↓ HDL-C↔, TG↓ | [102] |
| n = 52 (31/21) | MetS (n = 38, age 42–65, BMI 31.1 kg/m2), healthy (n = 14, age 42–65, BMI 24.4 kg/m2) | Chokeberry extract (Agropharm, Pieńków, Poland) | 3 × 100 mg | 8 | Low-fat diet | TC↓, LDL-C↓, HDL-C↔, TG↓ | [74] |
| n = 20 (2/0) | Postmenopausal women with abdominal obesity (WC > 88 cm, age 45–65, BMI 36.1 kg/m2) | Chokeberry supplement (Nutrika d.o.o., Belgrade, Serbia), prepared from pure chokeberry juice enriched with 2 g of stable glucomannan fibers (Luralean, Shimizu, Japan) | 100 mL | 4 | No changes | TC↔, LDL-C↔, HDL-C↓, TG↔ membrane fatty acid profile in erythrocytes: SFA↔, MUFA, n-6 PUFA ↔, n-3 PUFA↑, total PUFA ↔, n-6/n-3↓ unsaturation index↑ | [72] |
| n = 70 (42/28) | Group I: patients with MetS who received chokeberry extract supplements (n = 25, age 50–69, BMI 30.9 kg/m2) Group II: healthy—control group (n = 45, age 55–71, BMI 23 kg/m2) Group III: patients with MetS treated with ACE inhibitors—control group (n = 25, age 50–69, BMI 29.2 kg/m2) | Chokeberry extract (Aronox, Agropharm, Pieńków, Poland) | 3 × 100 mg | 8 | No changes (inhibition product containing chokeberry) | TC↓, LDL-C↓, HDL-C↓ | [75] |
| n = 23 (11/12) | High normal BP or grade I hypertension: SBP = 130–159 mmHg, DBP = 85–99 mmHg, no regular useof antihypertensive drugs (mean age 47.5 ± 10.4, BMI nd) | Organic chokeberry juice (Conimex Trade d.o.o., Belgrade, Serbia) | 200 mL | 4 | No changes | TC↔ LDL-C↔ HDL-C↔ TG↓ | [79] |
| n = 38 (24/14) | Mildly elevated BP: SBP 130–159 mmHg, DBP 85–99 mmHg (mean age 55.8, BMI <35 kg/m2) without DM2 | Cold-pressed 100% chokeberry juice (KiantamaLtd, Finland) or convection oven-dried chokeberry powder (Finnish Berry Powders Ltd., Finland) | 300 mL chokeberry juice or 3 g dried chokeberry powder | 8 | No changes | TC↔ HDL-C↔ TG↔ Apo-A1↔ Apo-B↔ | [76] |
| n = 77 (40/37) | Children and adolescents (age 13–19) with MetS (modified criteria of the IDF) | Chokeberry extract (Aronox, Agropharm, Pieńków, Poland) | 3 × 100 mg | 8 | No changes | TC↓ LDL-C↓ HDL-C↑ TG↓ | [137] |
| n = 35 (23/12) | DM2 and oral antidiabetic drugs therapy for at least 6 months (mean age 56.3, BMI 28.8 kg/m2) | Chokeberry juice (Nutrica d.o.o., Belgrade, Serbia) | 150 mL (three times daily for 50 mL) | 12 | No changes | TC↓ LDL-C↓ HDL-C↓ | [100] |
| n = 84 (52/32) | Subjects with cardiovascular risks (mean age 40.6, BMI 27.29 kg/m2) | Chokeberry juice with a high dose of polyphenols and chokeberry juice with a low dose of polyphenols (Nutrika LTD, Belgrade, Serbia) | 100 mL | 4 | Avoiding excessive quantities of other foods rich in polyphenols | low-dose of polyphenols group: TC↔, LDL-C↔, HDL-C↓, TG↔ high-dose of polyphenols group: TC↔, LDL-C↔, HDL-C↔, TG↔ oxLDL↓, oxLDL/TC ratio↓, oxLDL/LDL-C↓ changes in fatty acids in both groups: - PUFA n-6↑ - n6/n3 ratio (low-dose of polyphenols group)↑ - arachidonic/eicosapenteonic acid rate↑ - saturated fatty acids↑ | [73] |
| n = 22 (13/9) | Overweight (n = 11, mean age 51.9, BMI 25–30 kg/m2), healthy (n = 11, mea n age 41.4, BMI 18–25 kg/m2) | Chokeberry juice (Aronia Alive Agriculture Ltd., Sofia, Bulgaria) | 150 mL (50 mL—three times daily before meals) | 12 | nd | TC↔, LDL-C↔, HDLC↔, TG↔, TBARS↓ | [104] |
| n = 144 patients (74/70) | MetS according to the AHA guidelines (age 50–60, BMI 30.1–34.4 kg/m2) I. n = 42, fMetS II. n = 42, mMetS III. n = 32, fMetS-DM IV. n = 28, mMetS-DM | Standarized chokeberry extract (Alixir 400 PROTECT, Pharmanova, Belgrade, Serbia) | 30 mL (prior or during dinner) | 4 | No changes | fMetS: TC↓, LDL-C↓, HDL-C↑, TG↔ mMetS: TC↓, LDL-C↓, HDL-C↔, TG↔ fMetS-DM: TC↓, LDL-C↓, HDL-C↔,TG↓ mMetS-DM: TC↓, LDL-C↓, HDL-C↔, TG↓ | [71] |
3.5. Impact of Chokeberry on Inflammation and Antioxidant Status
| Number of Participants (n) (Women/Men) | Characteristics of the GROUP | Type of Chokeberry Product | Dose of Chokeberry Product per Day | Time of Intervention (Weeks) | Changes in Diet | Results | References |
|---|---|---|---|---|---|---|---|
| n = 44 (11/33) | Myocardial infarction and statin therapy for at least 6 months (mean age 66, BMI 26.5 kg/m2) | Chokeberry flavonoid extract (Aronox, Pieńków, Agropharm, Poland) | 3 × 85 mg | 6 | No changes | hsCRP↓, hsIL-6↓, ox-LDL↓, S-ICAM↓, S-CAM↓, MCP-1↓, F1-isoprostane↓ | [78] |
| n = 58 (0/58) | Mild hypocholesterolemia (TC > 200 mg/dL) without pharmacologicaltreatment (mean age 54.1, BMI 27.7 kg/m2) | Organic chokebery juice (A. M. Lech, Dzieciolowo, Poland) | 250 mL | 18 (12 weeks with drinking chokeberry juice) | No changes | CRP↔ | [103] |
| n = 47 (32/15) | MetS (n = 25, age 42–65, BMI 31.05 kg/m2), healthy (n = 22, BMI 24.15 kg/m2) | Chokeberry extract (Aronox, Agropharm, Pieńków, Poland) | 3 × 100 mg | 8 | No changes | CRP↔ | [77] |
| n = 70 (42/28) | Group I: patients with MetS who received chokeberry extract supplements (n = 25, age 50–69, BMI 30.9 kg/m2) Group II: healthy—control group (n = 45, age 55–71, BMI 23 kg/m2) Group III: patients with MetS treated with ACE inhibitors—control group (n = 25, age 50–69, BMI 29.2 kg/m2) | Chokeberry extract (Aronox, Agropharm, Pieńków, Poland) | 3 × 100 mg | 8 | No changes (inhibition product containing chokeberry) | CRP↔ | [75] |
| n = 23 (11/12) | High normal BP or grade I hypertension: SBP = 130–159 mmHg, DBP = 85–99 mmHg, no regular use of antihypertensive drugs (mean age 47.5, BMI nd) | Organic chokeberry juice (Conimex Trade d.o.o., Belgrade, Serbia) | 200 mL | 4 | No changes | CRP↔ | [79] |
| n = 38 (24/14) | Mildly elevated BP: SBP 130–159 mmHg, DBP 85–99 mmHg (mean age 55.8, BMI < 35 kg/m2) without DM2 | Cold-pressed 100% chokeberry juice (Kiantama Ltd, Finland) or convection oven-dried chokeberry powder (Finnish Berry Powders Ltd., Finland) | 300 mL chokeberry juice or 3 g dried chokeberry powder | 8 | No changes | IL-10↓, TNFα↓, IL-4-↔, IL-5↔, IL-6↔, IL-7↔, IL-8↔, IL-13↔, GM-CSF↔ | [76] |
| n = 35 (23/1) | DM2 2 and oral antidiabetic drugs therapy for at least 6 months (mean age 56.3, BMI 28.8 kg/m2) | Chokeberry juice (Nutrica d.o.o., Belgrade, Serbia) | 150 mL (three times daily for 50 mL) | 12 | No changes | WBC↓, LYM↓, CRP↔ | [100] |
| n = 22 (13/9) | Overweight (n = 11, mean age 51.9, BMI 25–30 kg/m2), healthy (n = 11, mean age 41.4, BMI 18–25 kg/m2) | Chokeberry juice (Aronia Alive Agriculture Ltd., Sofia, Bulgaria) | 150 mL (50 mL, three times daily before meals) | 12 | nd | CRP↓ | [104] |
| n = 30 (11/19) | Anemia: Hb < 110 g/L, and hemodialysis >3 months, >3 times week (mean age 62.93, BMI 25.82 kg/m2) | Polyphenol-rich standardized chokeberry extract (EU-Chem Company, Belgrade, Serbia) | 30 mL | 4 | nd | CRP↔, leukocytes↔, TNFα↔ | [177] |
| n = 144 (74/70) | MetS according to the AHA guidelines (age 50–60, BMI 30.1–34.4 kg/m2) I. n = 42, fMetS II. n = 42, mMetS III. n = 32, fMetS-DM IV. n = 28, mMetS-DM | Standarized chokeberry extract(Alixir 400 PROTECT, Pharmanova, Belgrade, Serbia) | 30 mL (prior or during dinner) | 4 | No changes | fMetS: WBC↓, CRP↓, LYM↔ mMetS: WBC↓, CRP↔, LYM↔ fMetS-DM: WBC↔, CRP↔, LYM↔ mMetS-DM: WBC↔, CRP↔, LYM↔ | [71] |
| Number of Participants (n) (Women/Men) | Characteristics of the Group | Type of Chokeberry Product | Dose of Chokeberry Product per Day | Time of Intervention (Weeks) | Changes in Diet | Results | References |
|---|---|---|---|---|---|---|---|
| n = 20 (20/0) | Postmenopausal women withabdominal obesity (WC > 88 cm, age 45–65, BMI 36.1 kg/m2) | Chokeberry supplement (Nutrika d.o.o., Belgrade, Serbia), prepared from pure chokeberry juice enriched with 2 g of stable glucomannan fibers (Luralean, Shimizu, Japan) | 100 mL | 4 | No changes | GSH-Px↑, SOD↔, CAT↔ | [72] |
| n = 22 (13/9) | Overweight (n = 11, mean age 51.9, BMI 25–30 kg/m2), healthy (n = 11, mean age 41.4, BMI 18–25 kg/m2) | Chokeberry juice (Aronia Alive Agriculture Ltd., Sofia, Bulgaria) | 150 mL (50 mL—three times daily before meals) | 12 | nd | SOD↑ CAT↔ | [104] |
| n = 30 (11/19) | Anemia: Hb < 110 g/L and hemodialysis >3 months, >3 times week (mean age 62.93, BMI 25.82 kg/m2) | Polyphenol-rich standardized chokeberry extract (EU-Chem Company, Belgrade, Serbia) | 30 mL | 4 | nd | CAT↑, reduced glutathione↑superoxide anion↓, radical↓, nitrite↓ hydrogen peroxide↔, SOD↔ | [177] |
3.6. Impact of Chokeberry on Blood Clotting
| Number of Participants (n) (Women/Men) | Characteristics of the Group | Type of Chokeberry Product | Dose of Chokeberry Product per Day | Time of Intervention (Weeks) | Changes in Diet | Results | References |
|---|---|---|---|---|---|---|---|
| n = 58 (0/58) | Mild hypocholesterolemia (TC > 200 mg/dL) without pharmacological treatment (mean age 54.1, BMI 27.7 kg/m2) | Organic chokebery juice (A. M. Lech, Dzieciolowo, Poland) | 250 mL | 18 (12 weeks with drinking chokeberry juice) | No changes | fibrinogen↓ | [103] |
| n = 47 (32/15) | MetS (n = 25, age 42–65, BMI 31.05 kg/m2), healthy (n = 22, BMI 24.15 kg/m2) | Chokeberry extract (Agropharm, Pieńków, Poland) | 3 × 100 mg | 8 | No changes | fibrinogen↑ | [77] |
| n = 52 (31/21) | MetS (n = 38, age 42–65, BMI 31.1 kg/m2), healthy (n = 14, age 42–65, BMI 24.4 kg/m2) | Chokeberry extract (Agropharm, Pieńków, Poland) | 3 × 100 mg | 8 | Low-fat diet | platelet aggregation↔, fibrinolysis↔, clot preparation ↔ | [74] |
| n = 38 (24/14) | Mildly elevated BP: SBP 130–159 mmHg, DBP 85–99 mmHg (mean age 55.8, BMI < 35 kg/m2) without DM2 | Cold-pressed 100% chokeberry juice (KiantamaLtd, Finland) or convection oven-dried chokeberry powder (Finnish Berry Powders Ltd., Finland) | 300 mL of chokeberry juice or 3 g of dried chokeberry powder | 8 | No changes | CEPI-CT↔, CADP-CT↔, PLT↔ | [76] |
| n = 144 patients (74/70) | MetS according to the AHA guidelines (age 50–60, BMI 30.1–34.4 kg/m2) I. n = 42, fMetS II. n = 42, mMetS III. n = 32, fMetS-DM IV. n = 28, mMetS-DM | Standarized chokeberry extract (Alixir 400 PROTECT, Pharmanova, Belgrade, Serbia) | 30 mL (prior or during dinner) | 4 | No changes | fMetS, mMetS: PLT↔ fMetS-DM, mMetS-DM: PLT↑ | [71] |
3.7. Impact of Chokeberry on Liver Functions
| Number of Participants (n) (Women/Men) | Characteristics of the Group | Type of Chokeberry Product | Dose of Chokeberry Product per Day | Time of Intervention (Weeks) | Changes in Diet | Results | References |
|---|---|---|---|---|---|---|---|
| n = 23 (11/12) | High normal BP or grade I hypertension: SBP = 130–159 mmHg, DBP = 85–99 mmHg, no regular use of antihypertensive drugs was declared by 23 patients (mean age 47.5, BMI nd) | Organic chokeberry juice (Conimex Trade d.o.o., Belgrade, Serbia) | 200 mL | 4 | No changes | AST↔ ALT↔ | [79] |
| n = 38 (24/14) | Mildly elevated BP: SBP 130–159 mmHg, DBP: 85–99 mmHg (mean age 55.8 years, BMI < 35) without DM2 | Cold-pressed 100% chokeberry juice (Kiantama Ltd, Finland) or convection oven-dried chokeberry powder (Finnish Berry Powders Ltd., Finland) | 300 mL chokeberry juice or 3 g dried chokeberry powder | 8 | No changes | GGTP↔ | [76] |
| n= 22 (13/9) | overweight (n = 11, mean age 51.9, BMI 25–30 kg/m2), healthy (n = 11, mean age 41.4, BMI 18–25 kg/m2) | Chokeberry juice (Aronia Alive Agriculture Ltd.,Sofia, Bulgaria) | 150 mL (50 mL, three times daily before meals) | 12 | nd | ALT↔ AST↔ GGTP↓ | [104] |
| n = 144 (74/70) | MetS according to the AHA guidelines (age 50–60, BMI 30.1–34.4 kg/m2) I. n = 42, fMetS II. n = 42, mMetS III. n = 32, fMetS-DM IV. n = 28, mMetS-DM | standarized chokeberry extract (Alixir 400 PROTECT, Pharmanova, Belgrade, Serbia) | 30 mL (prior or during dinner) | 4 | No changes | fMetS: AST↓, ALT↓, dBIL↔ mMetS: AST↓, ALT↔, dBIL↔ fMetS-DM: AST↓, ALT↔, dBIL↑ mMetS-DM: AST↔, ALT↔, dBIL↑ | [71] |
3.8. Impact Chokeberry on Uric Acid and Creatinine Level
| Number of Participants (n) (Women/Men) | Characteristics of the Group | Type of Chokeberry Product | Dose of Chokeberry Product per Day | Time of Intervention (Weeks) | Changes in Diet | Results | References |
|---|---|---|---|---|---|---|---|
| n = 58 (0/58) | Mild hypocholesterolemia (TC > 200 mg/dL) without pharmacological treatment (mean age 54.1, BMI 27.7 kg/m2) | Organic chokebery juice (A. M. Lech Dzieciolowo, Poland) | 250 mL | 18 (12 weeks with drinking chokeberry juice) | No changes | uric acid↔ | [103] |
| n = 47 (32/15) | MetS (n = 25, age 42–65, BMI 31.05 kg/m2), healthy (n = 22, BMI 24.15 kg/m2) | Chokeberry extract (Agropharm, Poland) | 3 × 100 mg | 8 | No changes | uric acid↔ | [77] |
| n = 23 (11/12) | High normal BP or grade I hypertension: SBP = 130–159 mmHg, DBP = 85–99 mmHg, no regular use of antihypertensive drugs (mean age 47.5, BMI nd) | Organic chokeberry juice (Conimex Trade d.o.o., Belgrade, Serbia) | 200 mL | 4 | No changes | uric acid↔, urea↔, creatinine ↔ | [79] |
| n = 35 (23/12) | DM2 and oral antidiabetic drugs therapy for at least 6 months (mean age 56.3, BMI 28.8 kg/m2) | Chokeberry juice (Nutrica d.o.o., Belgrade, Serbia) | 150 mL (three times daily for 50 mL) | 12 | No changes | creatinine↓, urea↔, urine creatinine↔, microalbuminuria↔ | [100] |
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Navab, M.; Gharavi, N.; Watson, A.D. Inflammation and metabolic disorders. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Kopp, W. How Western Diet And Lifestyle Drive The Pandemic Of Obesity And Civilization Diseases. Diabetes, Metab. Syndr. Obes. Targets Ther. 2019, 12, 2221–2236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zorena, K.; Jachimowicz-Duda, O.; Ślęzak, D.; Robakowska, M.; Mrugacz, M. Adipokines and Obesity. Potential Link to Metabolic Disorders and Chronic Complications. Int. J. Mol. Sci. 2020, 21, 3570. [Google Scholar] [CrossRef]
- World Health Organization. Body Mass Index-BMI. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 3 April 2021).
- Ronti, T.; Lupattelli, G.; Mannarino, E. The endocrine function of adipose tissue: An update. Clin. Endocrinol. 2006, 64, 355–365. [Google Scholar] [CrossRef]
- Rani, V.; Deep, G.; Singh, R.K.; Palle, K.; Yadav, U.C.S. Oxidative stress and metabolic disorders: Pathogenesis and therapeutic strategies. Life Sci. 2016, 148, 183–193. [Google Scholar] [CrossRef]
- Reaven, G.M. Banting lecture 1988. Role of insulin resistance in human disease. Diabetes 1988, 37, 1595–1607. [Google Scholar] [CrossRef]
- Oda, E. Metabolic syndrome: Its history, mechanisms, and limitations. Acta Diabetol. 2012, 49, 89–95. [Google Scholar] [CrossRef]
- Grundy, S.M. Metabolic syndrome update. Trends Cardiovasc. Med. 2015, 26, 364–373. [Google Scholar] [CrossRef]
- International Diabetes Federation. The IDF Consensus Worldwide Definition of the Metabolic Syndrome. Available online: https://www.idf.org/e-library/consensus-statements/60-idfconsensus-worldwide-definitionof-the-metabolic-syndrome.html (accessed on 3 April 2022).
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [Green Version]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; National heart, lung, and blood institute; American heart association; World heart federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurka, M.J.; Filipp, S.L.; DeBoer, M.D. Geographical variation in the prevalence of obesity, metabolic syndrome, and diabetes among US adults. Nutr. Diabetes 2018, 8, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scuteri, A.; Laurent, S.; Cucca, F.; Cockcroft, J.; Cunha, P.; Rodríguez-Mañas, L.; Raso, F.U.M.; Muiesan, M.L.; Ryliškytė, L.; Rietzschel, E.; et al. Metabolic syndrome across Europe: Different clusters of risk factors. Eur. J. Prev. Cardiol. 2015, 22, 486–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zujko, M.E.; Waśkiewicz, A.; Witkowska, A.M.; Szcześniewska, D.; Zdrojewski, T.; Kozakiewicz, K.; Drygas, W. Dietary Total Antioxidant Capacity and Dietary Polyphenol Intake and Prevalence of Metabolic Syndrome in Polish Adults: A Nationwide Study. Oxidative Med. Cell. Longev. 2018, 2018, 7487816. [Google Scholar] [CrossRef]
- Gregório, B.M.; De Souza, D.B.; Nascimento, F.A.D.M.; Matta, L.; Fernandes-Santos, C. The Potential Role of Antioxidants in Metabolic Syndrome. Curr. Pharm. Des. 2016, 22, 859–869. [Google Scholar] [CrossRef]
- Soory, M. Relevance of nutritional antioxidants in metabolic syndrome, ageing and cancer: Potential for therapeutic targeting. Infect. Disord. Drug Targets 2009, 9, 400–414. [Google Scholar] [CrossRef]
- Tolić, M.-T.; Jurčević, I.L.; Krbavčić, I.P.; Marković, K.; Vahčić, N. Phenolic Content, Antioxidant Capacity and Quality of Chokeberry (Aronia melanocarpa) Products. Food Technol. Biotechnol. 2015, 53, 171–179. [Google Scholar] [CrossRef]
- Jakobek, L.; Šeruga, M.; Krivak, P. The influence of interactions among phenolic compounds on the antiradical activity of chokeberries (Aronia melanocarpa). Int. J. Food Sci. Nutr. 2011, 62, 345–352. [Google Scholar] [CrossRef]
- Rop, O.; Mlcek, J.; Jurikova, T.; Valsikova, M.; Sochor, J.; Reznicek, V.; Kramarova, D. Phenolic content, antioxidant capacity, radical oxygen species scavenging and lipid peroxidation inhibiting activities of extracts of five black chokeberry (Aronia melanocarpa (Michx.) Elliot) cultivars. J. Med. Plant Res. 2010, 4, 2431–2437. [Google Scholar] [CrossRef]
- Jeon, Y.-D.; Kang, S.-H.; Moon, K.-H.; Lee, J.-H.; Kim, D.-G.; Kim, W.; Kim, J.-S.; Ahn, B.-Y.; Jin, J.-S. The Effect of Aronia Berry on Type 1 Diabetes In Vivo and In Vitro. J. Med. Food 2018, 21, 244–253. [Google Scholar] [CrossRef]
- Takahashi, A.; Shimizu, H.; Okazaki, Y.; Sakaguchi, H.; Taira, T.; Suzuki, T.; Chiji, H. Anthocyanin-rich Phytochemicals from Aronia Fruits Inhibit Visceral Fat Accumulation and Hyperglycemia in High-fat Diet-induced Dietary Obese Rats. J. Oleo Sci. 2015, 64, 1243–1250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valcheva-Kuzmanova, S.; Kuzmanov, K.; Tancheva, S.; Belcheva, A. Hypoglycemic effects of Aronia melanocarpa fruit juice in streptozotocin-induced diabetic rats. Methods Find. Exp. Clin. Pharmacol. 2007, 29, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Kong, Y.; Yan, T.; Tong, Y.; Deng, H.; Tan, C.; Wan, M.; Wang, M.; Meng, X.; Wang, Y. Gut Microbiota Modulation by Polyphenols from Aronia melanocarpa of LPS-Induced Liver Diseases in Rats. J. Agric. Food Chem. 2021, 69, 3312–3325. [Google Scholar] [CrossRef] [PubMed]
- Kondeva-Burdina, M.; Valcheva-Kuzmanova, S.; Markova, T.; Mitcheva, M.; Belcheva, A. Effects of aronia melanocarpa fruit juice on isolated rat hepatocytes. Pharmacogn. Mag. 2015, 11, 592–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H.; Liu, Y.; Kim, H.-S.; Shin, J.-H. Chokeberry attenuates the expression of genes related to de novo lipogenesis in the hepatocytes of mice with nonalcoholic fatty liver disease. Nutr. Res. 2016, 36, 57–64. [Google Scholar] [CrossRef]
- Valcheva-Kuzmanova, S.; Borisova, P.; Galunska, B.; Krasnaliev, I.; Belcheva, A. Hepatoprotective effect of the natural fruit juice from Aronia melanocarpa on carbon tetrachloride-induced acute liver damage in rats. Exp. Toxicol. Pathol. 2004, 56, 195–201. [Google Scholar] [CrossRef]
- Piotrowska-Kempisty, H.; Nowicki, M.; Jodynis-Liebert, J.; Kurpik, M.; Ewertowska, M.; Adamska, T.; Oszmiański, J.; Kujawska, M. Assessment of Hepatoprotective Effect of Chokeberry Juice in Rats Treated Chronically with Carbon Tetrachloride. Molecules 2020, 25, 1268. [Google Scholar] [CrossRef] [Green Version]
- Bhaswant, M.; Shafie, S.R.; Mathai, M.L.; Mouatt, P.; Brown, L. Anthocyanins in chokeberry and purple maize attenuate diet-induced metabolic syndrome in rats. Nutrition 2017, 41, 24–31. [Google Scholar] [CrossRef]
- Ciocoiu, M.; Badescu, L.; Miron, A.; Badescu, M. The Involvement of a Polyphenol-Rich Extract of Black Chokeberry in Oxidative Stress on Experimental Arterial Hypertension. Evid.-Based Complement. Altern. Med. 2013, 2013, 912769. [Google Scholar] [CrossRef]
- Banihani, S.; Swedan, S.; Alguraan, Z. Pomegranate and type 2 diabetes. Nutr. Res. 2013, 33, 341–348. [Google Scholar] [CrossRef]
- Lim, S.-M.; Lee, H.S.; Jung, J.I.; Kim, S.M.; Kim, N.Y.; Seo, T.S.; Bae, J.-S.; Kim, E.J. Cyanidin-3-O-Galactoside-Enriched Aronia melanocarpa Extract Attenuates Weight Gain and Adipogenic Pathways in High-Fat Diet-Induced Obese C57BL/6 Mice. Nutrients 2019, 11, 1190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daskalova, E.; Delchev, S.; Peeva, Y.; Vladimirova-Kitova, L.; Kratchanova, M.; Kratchanov, C.; Denev, P. Antiatherogenic and Cardioprotective Effects of Black Chokeberry (Aronia melanocarpa) Juice in Aging Rats. Evid.-Based Complement. Altern. Med. 2015, 2015, 717439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valcheva-Kuzmanova, S.; Kuzmanov, K.; Mihova, V.; Krasnaliev, I.; Borisova, P.; Belcheva, A. Antihyperlipidemic Effect of Aronia melanocarpa Fruit Juice in Rats Fed a High-Cholesterol Diet. Plant Foods Hum. Nutr. 2007, 62, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Liu, X.; Zheng, Y.; Liu, W.; Ding, C. Aronia melanocarpa polysaccharide ameliorates inflammation and aging in mice by modulating the AMPK/SIRT1/NF-κB signaling pathway and gut microbiota. Sci. Rep. 2021, 11, 20558. [Google Scholar] [CrossRef] [PubMed]
- Shatoor, A.S.; Al Humayed, S. The Protective Effect of Crataegus aronia Against High-Fat Diet-Induced Vascular Inflammation in Rats Entails Inhibition of the NLRP-3 Inflammasome Pathway. Cardiovasc. Toxicol. 2020, 20, 82–99. [Google Scholar] [CrossRef]
- Yu, S.-Y.; Kim, M.-B.; Park, Y.-K.; Bae, M.; Kang, H.; Hu, S.; Pham, T.X.; Carpenter, R.; Lee, J.; Lee, O.-H.; et al. Anthocyanin-Rich Aronia Berry Extract Mitigates High-Fat and High-Sucrose Diet-Induced Adipose Tissue Inflammation by Inhibiting Nuclear Factor-κB Activation. J. Med. Food 2021, 24, 586–594. [Google Scholar] [CrossRef]
- Kang, S.-H.; Jeon, Y.-D.; Moon, K.-H.; Lee, J.-H.; Kim, D.-G.; Kim, W.; Myung, H.; Kim, J.-S.; Kim, H.-J.; Bang, K.-S.; et al. Aronia Berry Extract Ameliorates the Severity of Dextran Sodium Sulfate-Induced Ulcerative Colitis in Mice. J. Med. Food 2017, 20, 667–675. [Google Scholar] [CrossRef]
- Valcheva-Kuzmanova, S.; Kuzmanov, A.; Kuzmanova, V.; Tzaneva, M. Aronia melanocarpa fruit juice ameliorates the symptoms of inflammatory bowel disease in TNBS-induced colitis in rats. Food Chem. Toxicol. 2018, 113, 33–39. [Google Scholar] [CrossRef]
- Pei, R.; Liu, J.; Martin, D.A.; Valdez, J.C.; Jeffety, J.; Barrett-Wilt, G.A.; Liu, Z.; Bolling, B.W. Aronia Berry Supplementation Mitigates Inflammation in T Cell Transfer-Induced Colitis by Decreasing Oxidative Stress. Nutrients 2019, 11, 1316. [Google Scholar] [CrossRef] [Green Version]
- Tomić, M.; Ignjatović, Đ.; Tovilović-Kovačević, G.; Krstić-Milošević, D.; Ranković, S.; Popović, T.; Glibetić, M. Reduction of anxiety-like and depression-like behaviors in rats after one month of drinking Aronia melanocarpa berry juice. Food Funct. 2016, 7, 3111–3120. [Google Scholar] [CrossRef]
- Wei, J.; Zhang, G.; Zhang, X.; Xu, D.; Gao, J.; Fan, J.; Zhou, Z. Anthocyanins from Black Chokeberry (Aroniamelanocarpa Elliot) Delayed Aging-Related Degenerative Changes of Brain. J. Agric. Food Chem. 2017, 65, 5973–5984. [Google Scholar] [CrossRef] [PubMed]
- Wen, H.; Cui, H.; Tian, H.; Zhang, X.; Ma, L.; Ramassamy, C.; Li, J. Isolation of Neuroprotective Anthocyanins from Black Chokeberry (Aronia melanocarpa) against Amyloid-β-Induced Cognitive Impairment. Foods 2020, 10, 63. [Google Scholar] [CrossRef] [PubMed]
- Daskalova, E.; Delchev, S.; Topolov, M.; Dimitrova, S.; Uzunova, Y.; Valcheva-Kuzmanova, S.; Kratchanova, M.; Vladimirova-Kitova, L.; Denev, P. Aronia melanocarpa (Michx.) Elliot fruit juice reveals neuroprotective effect and improves cognitive and locomotor functions of aged rats. Food Chem. Toxicol. 2019, 132, 110674. [Google Scholar] [CrossRef]
- Gajić, D.; Saksida, T.; Koprivica, I.; Šenerović, L.; Morić, I.; Šavikin, K.; Menković, N.; Pejnović, N.; Stojanović, I. Immunomodulatory activity and protective effects of chokeberry fruit extract on Listeria monocytogenes infection in mice. Food Funct. 2020, 11, 7793–7803. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kim, J.I.; Lee, I.; Lee, S.; Hwang, M.-W.; Bae, J.-Y.; Heo, J.; Kim, D.; Han, S.-Z.; Park, M.-S. Aronia melanocarpa and its components demonstrate antiviral activity against influenza viruses. Biochem. Biophys. Res. Commun. 2013, 440, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, J.; Hires, C.; Baker, C.; Keenan, L.; Bush, M. Daily supplementation with aronia melanocarpa (chokeberry) reduces blood pressure and cholesterol: A meta analysis of controlled clinical trials. J. Diet. Suppl. 2020, 18, 517–530. [Google Scholar] [CrossRef]
- Rahmani, J.; Clark, C.; Varkaneh, H.K.; Lakiang, T.; Vasanthan, L.T.; Onyeche, V.; Mousavi, S.M.; Zhang, Y. The effect of Aronia consumption on lipid profile, blood pressure, and biomarkers of inflammation: A systematic review and meta-analysis of randomized controlled trials. Phytother. Res. 2019, 33, 1981–1990. [Google Scholar] [CrossRef]
- Zheng, W.; Wang, S.Y. Oxygen Radical Absorbing Capacity of Phenolics in Blueberries, Cranberries, Chokeberries, and Lingonberries. J. Agric. Food Chem. 2003, 51, 502–509. [Google Scholar] [CrossRef]
- Sidor, A.; Gramza-Michałowska, A. Black Chokeberry Aronia melanocarpa L.—A Qualitative Composition, Phenolic Profile and Antioxidant Potential. Molecules 2019, 24, 3710. [Google Scholar] [CrossRef] [Green Version]
- King, E.S.; Bolling, B.W.; Kiritsakis, A.K.; Kiritsakis, K.A.; Tsitsipas, C.K. Composition, polyphenol bioavailability, and health benefits of aronia berry: A review. J. Food Bioact. 2020, 11, 13–30. [Google Scholar] [CrossRef]
- Trenka, M.; Nawirska-Olszańska, A.; Oziembłowski, M. Analysis of Selected Properties of Fruits of Black Chokeberry (Aronia melanocarpa L.) from Organic and Conventional Cultivation. Appl. Sci. 2020, 10, 9096. [Google Scholar] [CrossRef]
- Zielińska, A.; Siudem, P.; Paradowska, K.; Gralec, M.; Kaźmierski, S.; Wawer, I. Aronia melanocarpa Fruits as a Rich Dietary Source of Chlorogenic Acids and Anthocyanins: 1H-NMR, HPLC-DAD, and Chemometric Studies. Molecules 2020, 25, 3234. [Google Scholar] [CrossRef] [PubMed]
- Putta, S.; Yarla, N.S.; Kumar, E.K.; Lakkappa, D.B.; Kamal, M.A.; Scotti, L.; Scotti, M.T.; Ashraf, G.; Rao, B.S.B.; Kumari, S.; et al. Preventive and Therapeutic Potentials of Anthocyanins in Diabetes and Associated Complications. Curr. Med. Chem. 2019, 25, 5347–5371. [Google Scholar] [CrossRef] [PubMed]
- Oszmiański, J.; Lachowicz, S. Effect of the Production of Dried Fruits and Juice from Chokeberry (Aronia melanocarpa L.) on the Content and Antioxidative Activity of Bioactive Compounds. Molecules 2016, 21, 1098. [Google Scholar] [CrossRef]
- Guo, H.; Xia, M. Chapter 12—Anthocyanins and Diabetes Regulation. In Polyphenols: Mechanisms of Action in Human Health and Disease, 2nd ed.; Watson, R.R., Preedy, V.R., Zibadi, S., Eds.; Academic Press: Cambridge, MA, USA, 2018. [Google Scholar]
- Cindrić, I.J.; Zeiner, M.; Mihajlov-Konanov, D.; Stingeder, G. Inorganic Macro- and Micronutrients in “Superberries” Black Chokeberries (Aronia melanocarpa) and Related Teas. Int. J. Environ. Res. Public Health 2017, 14, 539. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Werner, M.; Winterhalter, P.; Esatbeyoglu, T. Phenolic Composition, Radical Scavenging Activity and an Approach for Authentication of Aronia melanocarpa Berries, Juice, and Pomace. J. Food Sci. 2019, 84, 1791–1798. [Google Scholar] [CrossRef]
- Romani, A.; Vignolini, P.; Ieri, F.; Heimler, D. Polyphenols and Volatile Compounds in Commercial Chokeberry (Aronia melanocarpa) Products. Nat. Prod. Commun. 2016, 11, 99–102. [Google Scholar] [CrossRef] [Green Version]
- Bolling, B.W.; Taheri, R.; Pei, R.; Kranz, S.; Yu, M.; Durocher, S.N.; Brand, M.H. Harvest date affects aronia juice polyphenols, sugars, and antioxidant activity, but not anthocyanin stability. Food Chem. 2015, 187, 189–196. [Google Scholar] [CrossRef]
- Wilkes, K.; Howard, L.R.; Brownmiller, C.; Prior, R.L. Changes in Chokeberry (Aronia melanocarpa L.) Polyphenols during Juice Processing and Storage. J. Agric. Food Chem. 2014, 62, 4018–4025. [Google Scholar] [CrossRef]
- Hwang, E.-S.; Thi, N.D. Effects of Different Growing Regions on Quality Characteristics, Bioactive Compound Contents, and Antioxidant Activity of Aronia (Aronia melanocarpa) in Korea. Prev. Nutr. Food Sci. 2016, 21, 255–262. [Google Scholar] [CrossRef] [Green Version]
- Casadei, K.; Kiel, J. Anthropometric Measurement. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Cetin, D.; Lessig, B.A.; Nasr, E. Comprehensive Evaluation for Obesity: Beyond Body Mass Index. J. Osteopat. Med. 2016, 116, 376–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Moustaid-Moussa, N.; Chen, L.; Mo, H.; Shastri, A.; Su, R.; Bapat, P.; Kwun, I.; Shen, C.-L. Novel insights of dietary polyphenols and obesity. J. Nutr. Biochem. 2014, 25, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akhlaghi, M.; Ghobadi, S.; Hosseini, M.M.; Gholami, Z.; Mohammadian, F. Flavanols are potential anti-obesity agents, a systematic review and meta-analysis of controlled clinical trials. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 675–690. [Google Scholar] [CrossRef] [PubMed]
- Prior, R.L.; Wu, X.; Gu, L.; Hager, T.J.; Hager, A.; Howard, L.R. Whole Berries versus Berry Anthocyanins: Interactions with Dietary Fat Levels in the C57BL/6J Mouse Model of Obesity. J. Agric. Food Chem. 2008, 56, 647–653. [Google Scholar] [CrossRef]
- Kim, N.-Y.; Thomas, S.S.; Hwang, D.-I.; Lee, J.-H.; Kim, K.-A.; Cha, Y.-S. Anti-Obesity Effects of Morus alba L. and Aronia melanocarpa in a High-Fat Diet-Induced Obese C57BL/6J Mouse Model. Foods 2021, 10, 1914. [Google Scholar] [CrossRef]
- Kowalska, K.; Olejnik, A.; Szwajgier, D.; Olkowicz, M. Inhibitory activity of chokeberry, bilberry, raspberry and cranberry polyphenol-rich extract towards adipogenesis and oxidative stress in differentiated 3T3-L1 adipose cells. PLoS ONE 2017, 12, e0188583. [Google Scholar] [CrossRef] [Green Version]
- Tasic, N.; Jakovljevic, V.L.J.; Mitrovic, M.; Djindjic, B.; Tasic, D.; Dragisic, D.; Citakovic, Z.; Kovacevic, Z.; Radoman, K.; Zivkovic, V.; et al. Black chokeberry Aronia melanocarpa extract reduces blood pressure, glycemia and lipid profile in patients with metabolic syndrome: A prospective controlled trial. Mol. Cell. Biochem. 2021, 476, 2663–2673. [Google Scholar] [CrossRef]
- Kardum, N.; Petrović-Oggiano, G.; Takic, M.; Glibetić, N.; Zec, M.; Debeljak-Martacic, J.; Konić-Ristić, A. Effects of Glucomannan-Enriched, Aronia Juice-Based Supplement on Cellular Antioxidant Enzymes and Membrane Lipid Status in Subjects with Abdominal Obesity. Sci. World J. 2014, 2014, 869250. [Google Scholar] [CrossRef] [Green Version]
- Pokimica, B.; García-Conesa, M.-T.; Zec, M.; Debeljak-Martačić, J.; Ranković, S.; Vidović, N.; Petrović-Oggiano, G.; Konić-Ristić, A.; Glibetić, M. Chokeberry Juice Containing Polyphenols Does Not Affect Cholesterol or Blood Pressure but Modifies the Composition of Plasma Phospholipids Fatty Acids in Individuals at Cardiovascular Risk. Nutrients 2019, 11, 850. [Google Scholar] [CrossRef] [Green Version]
- Sikora, J.; Broncel, M.; Markowicz, M.; Chałubiński, M.; Wojdan, K.; Mikiciuk-Olasik, E. Short-term supplementation with Aronia melanocarpa extract improves platelet aggregation, clotting, and fibrinolysis in patients with metabolic syndrome. Eur. J. Nutr. 2012, 51, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Sikora, J.; Broncel, M.; Mikiciuk-Olasik, E. Aronia melanocarpa ElliotReduces the Activity of Angiotensin I-Converting Enzyme—In Vitro and Ex Vivo Studies. Oxidative Med. Cell. Longev. 2014, 2014, 739721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loo, B.-M.; Erlund, I.; Koli, R.; Puukka, P.; Hellström, J.; Wähälä, K.; Mattila, P.; Jula, A. Consumption of chokeberry (Aronia mitschurinii) products modestly lowered blood pressure and reduced low-grade inflammation in patients with mildly elevated blood pressure. Nutr. Res. 2016, 36, 1222–1230. [Google Scholar] [CrossRef] [PubMed]
- Broncel, M.; Kozirog, M.; Duchnowicz, P.; Koter-Michalak, M.; Sikora, J.; Chojnowska-Jezierska, J. Aronia melanocarpa extract reduces blood pressure, serum endothelin, lipid, and oxidative stress marker levels in patients with metabolic syndrome. Med. Sci. Monit. 2010, 16, CR28-34. [Google Scholar]
- Naruszewicz, M.; Łaniewska, I.; Millo, B.; Dłużniewski, M. Combination therapy of statin with flavonoids rich extract from chokeberry fruits enhanced reduction in cardiovascular risk markers in patients after myocardial infraction (MI). Atherosclerosis 2007, 194, e179–e184. [Google Scholar] [CrossRef]
- Kardum, N.; Milovanović, B.; Šavikin, K.; Zdunić, G.; Mutavdžin, S.; Gligorijević, T.; Spasić, S. Beneficial Effects of Polyphenol-Rich Chokeberry Juice Consumption on Blood Pressure Level and Lipid Status in Hypertensive Subjects. J. Med. Food 2015, 18, 1231–1238. [Google Scholar] [CrossRef]
- Kardum, N.; Ristić, A.K.; Šavikin, K.; Spasić, S.; Stefanović, A.; Ivanišević, J.; Miljković, M. Effects of Polyphenol-Rich Chokeberry Juice on Antioxidant/Pro-Oxidant Status in Healthy Subjects. J. Med. Food 2014, 17, 869–874. [Google Scholar] [CrossRef]
- Jebur, A.B.; Mokhamer, M.H.; El-Demerdash, F.M. A Review on Oxidative Stress and Role of Antioxidants in Diabetes Mellitus. Austin Endocrinol. Diabetes Case Rep. 2016, 1, 1006. [Google Scholar]
- Aryaeian, N.; Sedehi, S.K.; Arablou, T. Polyphenols and their effects on diabetes management: A review. Med. J. Islam. Repub. Iran 2017, 31, 886–892. [Google Scholar] [CrossRef] [Green Version]
- Guasch-Ferré, M.; Merino, J.; Sun, Q.; Fitó, M.; Salas-Salvadó, J. Dietary Polyphenols, Mediterranean Diet, Prediabetes, and Type 2 Diabetes: A Narrative Review of the Evidence. Oxid. Med. Cell. Longev. 2017, 2017, 6723931. [Google Scholar] [CrossRef]
- Schulze, C.; Bangert, A.; Kottra, G.; Geillinger, K.E.; Schwanck, B.; Vollert, H.; Blaschek, W.; Daniel, H. Inhibition of the intestinal sodium-coupled glucose transporter 1 (SGLT1) by extracts and polyphenols from apple reduces postprandial blood glucose levels in mice and humans. Mol. Nutr. Food Res. 2014, 58, 1795–1808. [Google Scholar] [CrossRef]
- Papuc, C.; Goran, G.V.; Predescu, C.N.; Tudoreanu, L.; Ștefan, G. Plant polyphenols mechanisms of action on insulin resistance and against the loss of pancreatic beta cells. Crit. Rev. Food Sci. Nutr. 2022, 62, 325–352. [Google Scholar] [CrossRef] [PubMed]
- Williamson, G.; Sheedy, K. Effects of Polyphenols on Insulin Resistance. Nutrients 2020, 12, 3135. [Google Scholar] [CrossRef] [PubMed]
- Toupchian, O.; Abdollahi, S.; Salehi-Abargouei, A.; Heshmati, J.; Clark, C.C.T.; Sheikhha, M.H.; Fallahzadeh, H.; Mozaffari-Khosravi, H. The effects of resveratrol supplementation on PPARα, p16, p53, p21 gene expressions, and sCD163/sTWEAK ratio in patients with type 2 diabetes mellitus: A double-blind controlled randomized trial. Phytother. Res. 2021, 35, 3205–3213. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Ling, W.; Yang, Y.; Chen, Y.; Tian, Z.; Du, Z.; Chen, J.; Xie, Y.; Liu, Z.; Yang, L. Role of Purified Anthocyanins in Improving Cardiometabolic Risk Factors in Chinese Men and Women with Prediabetes or Early Untreated Diabetes—A Randomized Controlled Trial. Nutrients 2017, 9, 1104. [Google Scholar] [CrossRef] [Green Version]
- Li, D.; Zhang, Y.; Liu, Y.; Sun, R.; Xia, M. Purified Anthocyanin Supplementation Reduces Dyslipidemia, Enhances Antioxidant Capacity, and Prevents Insulin Resistance in Diabetic Patients. J. Nutr. 2015, 145, 742–748. [Google Scholar] [CrossRef]
- Shehzad, A.; Iqbal, W.; Shehzad, O.; Lee, Y.S. Adiponectin: Regulation of its production and its role in human diseases. Hormones 2012, 11, 8–20. [Google Scholar] [CrossRef]
- Nigro, E.; Scudiero, O.; Monaco, M.L.; Palmieri, A.; Mazzarella, G.; Costagliola, C.; Bianco, A.; Daniele, A. New Insight into Adiponectin Role in Obesity and Obesity-Related Diseases. BioMed. Res. Int. 2014, 2014, 658913. [Google Scholar] [CrossRef]
- Rugină, D.; Diaconeasa, Z.; Coman, C.; Bunea, A.; Socaciu, C.; Pintea, A. Chokeberry Anthocyanin Extract as Pancreaticβ-Cell Protectors in Two Models of Induced Oxidative Stress. Oxidative Med. Cell. Longev. 2015, 2015, 429075. [Google Scholar] [CrossRef] [Green Version]
- Yamane, T.; Kozuka, M.; Konda, D.; Nakano, Y.; Nakagaki, T.; Ohkubo, I.; Ariga, H. Improvement of blood glucose levels and obesity in mice given aronia juice by inhibition of dipeptidyl peptidase IV and α-glucosidase. J. Nutr. Biochem. 2016, 31, 106–112. [Google Scholar] [CrossRef]
- Bräunlich, M.; Slimestad, R.; Wangensteen, H.; Brede, C.; Malterud, K.E.; Barsett, H. Extracts, Anthocyanins and Procyanidins from Aronia melanocarpa as Radical Scavengers and Enzyme Inhibitors. Nutrients 2013, 5, 663–678. [Google Scholar] [CrossRef] [Green Version]
- DE, S.; Banerjee, S.; Kumar, S.A.; Paira, P. Critical Role of Dipeptidyl Peptidase IV: A Therapeutic Target for Diabetes and Cancer. Mini-Rev. Med. Chem. 2019, 19, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Deacon, C.F.; Lebovitz, H.E. Comparative review of dipeptidyl peptidase-4 inhibitors and sulphonylureas. Diabetes Obes. Metab. 2016, 18, 333–347. [Google Scholar] [CrossRef] [Green Version]
- Kozuka, M.; Yamane, T.; Nakano, Y.; Nakagaki, T.; Ohkubo, I.; Ariga, H. Identification and characterization of a dipeptidyl peptidase IV inhibitor from aronia juice. Biochem. Biophys. Res. Commun. 2015, 465, 433–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Worsztynowicz, P.; Napierała, M.; Białas, W.; Grajek, W.; Olkowicz, M. Pancreatic α-amylase and lipase inhibitory activity of polyphenolic compounds present in the extract of black chokeberry (Aronia melanocarpa L.). Process Biochem. 2014, 49, 1457–1463. [Google Scholar] [CrossRef]
- Mu, J.; Xin, G.; Zhang, B.; Wang, Y.; Ning, C.; Meng, X. Beneficial effects of Aronia melanocarpa berry extract on hepatic insulin resistance in type 2 diabetes mellitus rats. J. Food Sci. 2020, 85, 1307–1318. [Google Scholar] [CrossRef] [PubMed]
- Milutinović, M.; Radovanović, R.V.; Šavikin, K.; Radenković, S.; Arvandi, M.; Pešić, M.; Kostić, M.; Miladinović, B.; Branković, S.; Kitić, D. Chokeberry juice supplementation in type 2 diabetic patients—Impact on health status. J. Appl. Biomed. 2019, 17, 218–224. [Google Scholar] [CrossRef]
- Nathan, D.M.; Turgeon, H.; Regan, S. Relationship between glycated haemoglobin levels and mean glucose levels over time. Diabetologia 2007, 50, 2239–2244. [Google Scholar] [CrossRef] [Green Version]
- Lancrajan, I. Aronia Melanocarpa, a Potential Therapeutic Agent. Studia Universitatis “Vasile Goldiş”. Ser. Ştiinţele Vieţii 2012, 22, 389–394. [Google Scholar]
- Skoczyńska, A.; Jedrychowska, I.; Poręba, R.; Affelska-Jercha, A.; Turczyn, B.; Wojakowska, A.; Andrzejak, R. Influence of chokeberry juice on arterial blood pressure and lipid parameters in men with mild hypercholesterolemia. Pharmacol. Rep. 2007, 59, 177–182. [Google Scholar]
- Gancheva, S.; Ivanova, I.; Atanassova, A.; Gancheva-Tomova, D.; Eftimov, M.; Moneva, K.; Zhelyazkova-Savova, M.; Valcheva-Kuzmanova, S. Effects of Aronia melanocarpa fruit juice on oxidative stress, energy homeostasis, and liver function in overweight and healthy-weight individuals. Scr. Sci. Med. 2021, 53, 39–46. [Google Scholar] [CrossRef]
- Yamane, T.; Kozuka, M.; Wada-Yoneta, M.; Sakamoto, T.; Nakagaki, T.; Nakano, Y.; Ohkubo, I. Aronia juice suppresses the elevation of postprandial blood glucose levels in adult healthy Japanese. Clin. Nutr. Exp. 2017, 12, 20–26. [Google Scholar] [CrossRef] [Green Version]
- Petrovic, S.; Arsic, A.; Glibetic, M.; Cikiriz, N.; Jakovljevic, V.; Vucic, V. The effects of polyphenol-rich chokeberry juice on fatty acid profiles and lipid peroxidation of active handball players: Results from a randomized, double-blind, placebo-controlled study. Can. J. Physiol. Pharmacol. 2016, 94, 1058–1063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kardum, N.; Takić, M.; Šavikin, K.; Zec, M.; Zdunić, G.; Spasić, S.; Konić-Ristić, A. Effects of polyphenol-rich chokeberry juice on cellular antioxidant enzymes and membrane lipid status in healthy women. J. Funct. Foods 2014, 9, 89–97. [Google Scholar] [CrossRef]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- Kjeldsen, S.E. Hypertension and cardiovascular risk: General aspects. Pharmacol. Res. 2018, 129, 95–99. [Google Scholar] [CrossRef]
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef]
- Ozemek, C.; Laddu, D.R.; Arena, R.; Lavie, C.J. The role of diet for prevention and management of hypertension. Curr. Opin. Cardiol. 2018, 33, 388–393. [Google Scholar] [CrossRef]
- Galleano, M.; Pechanova, O.; Fraga, C.G. Hypertension, Nitric Oxide, Oxidants, and Dietary Plant Polyphenols. Curr. Pharm. Biotechnol. 2010, 11, 837–848. [Google Scholar] [CrossRef]
- Godos, J.; Vitale, M.; Micek, A.; Ray, S.; Martini, D.; Del Rio, D.; Riccardi, G.; Galvano, F.; Grosso, G. Dietary Polyphenol Intake, Blood Pressure, and Hypertension: A Systematic Review and Meta-Analysis of Observational Studies. Antioxidants 2019, 8, 152. [Google Scholar] [CrossRef] [Green Version]
- Hügel, H.M.; Jackson, N.; May, B.; Zhang, A.L.; Xue, C.C. Polyphenol protection and treatment of hypertension. Phytomedicine 2016, 23, 220–231. [Google Scholar] [CrossRef]
- Vendrame, S.; Klimis-Zacas, D. Potential Factors Influencing the Effects of Anthocyanins on Blood Pressure Regulation in Humans: A Review. Nutrients 2019, 11, 1431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavlovic, A.N.; Brcanović, J.M.; Veljković, J.N.; Mitic, S.S.; Tošić, S.; Kaličanin, B.M.; Kostic, D.A.; Ðorđević, M.S.; Velimirović, D.S. Characterization of commercially available products of aronia according to their metal content. Fruits 2015, 70, 385–393. [Google Scholar] [CrossRef] [Green Version]
- Tjelle, T.E.; Holtung, L.; Bøhn, S.K.; Aaby, K.; Thoresen, M.; Wiik, S.; Paur, I.; Karlsen, A.S.; Retterstøl, K.; Iversen, P.O.; et al. Polyphenol-rich juices reduce blood pressure measures in a randomised controlled trial in high normal and hypertensive volunteers. Br. J. Nutr. 2015, 114, 1054–1063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahles, S.; Stevens, Y.R.; Joris, P.J.; Vauzour, D.; Adam, J.; De Groot, E.; Plat, J. The Effect of Long-Term Aronia melanocarpa Extract Supplementation on Cognitive Performance, Mood, and Vascular Function: A Randomized Controlled Trial in Healthy, Middle-Aged Individuals. Nutrients 2020, 12, 2475. [Google Scholar] [CrossRef]
- Masuyer, G.; Yates, C.J.; Sturrock, E.D.; Acharya, K.R. Angiotensin-I converting enzyme (ACE): Structure, biological roles, and molecular basis for chloride ion dependence. Biol. Chem. 2014, 395, 1135–1149. [Google Scholar] [CrossRef]
- Piepho, R.W. Overview of the angiotensin-converting-enzyme inhibitors. Am. J. Health Syst. Pharm. 2000, 57 (Suppl. 1), S3–S7. [Google Scholar] [CrossRef]
- Shihoya, W.; Nishizawa, T.; Okuta, A.; Tani, K.; Dohmae, N.; Fujiyoshi, W.S.A.O.K.T.Y.; Nureki, W.S.T.N.O.; Doi, T. Activation mechanism of endothelin ETB receptor by endothelin-1. Nature 2016, 537, 363–368. [Google Scholar] [CrossRef]
- Khimji, A.-K.; Rockey, D.C. Endothelin—Biology and disease. Cell. Signal. 2010, 22, 1615–1625. [Google Scholar] [CrossRef]
- Mannu, G.S.; Zaman, M.J.; Gupta, A.; Rehman, H.U.; Myint, P.K. Evidence of Lifestyle Modification in the Management of Hypercholesterolemia. Curr. Cardiol. Rev. 2013, 9, 2–14. [Google Scholar] [CrossRef] [Green Version]
- Sonestedt, E.; Hellstrand, S.; Drake, I.; Schulz, C.-A.; Ericson, U.; Hlebowicz, J.; Persson, M.M.; Gullberg, B.; Hedblad, B.; Engström, G.; et al. Diet Quality and Change in Blood Lipids during 16 Years of Follow-up and Their Interaction with Genetic Risk for Dyslipidemia. Nutrients 2016, 8, 274. [Google Scholar] [CrossRef] [Green Version]
- Orozco-Beltran, D.; Gil-Guillen, V.F.; Redon, J.; Martin-Moreno, J.M.; Pallares-Carratala, V.; Navarro-Perez, J.; Valls-Roca, F.; Sanchis-Domenech, C.; Fernandez-Gimenez, A.; Perez-Navarro, A.; et al. Correction: Lipid profile, cardiovascular disease and mortality in a Mediterranean high-risk population: The ESCARVAL-RISK study. PLoS ONE 2018, 13, e0205047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchholz, T.; Melzig, M.F. Polyphenolic Compounds as Pancreatic Lipase Inhibitors. Planta Med. 2015, 81, 771–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bialecka-Florjanczyk, E.; Fabiszewska, A.U.; Krzyczkowska, J.; Kurylowicz, A. Synthetic and Natural Lipase Inhibitors. Mini-Reviews Med. Chem. 2018, 18, 672–683. [Google Scholar] [CrossRef] [PubMed]
- Shishikura, Y.; Khokhar, A.S.; Murray, B.S. Effects of Tea Polyphenols on Emulsification of Olive Oil in a Small Intestine Model System. J. Agric. Food Chem. 2006, 54, 1906–1913. [Google Scholar] [CrossRef]
- Tung, W.-C.; Rizzo, B.; Dabbagh, Y.; Saraswat, S.; Romanczyk, M.; Codorniu-Hernández, E.; Rebollido-Rios, R.; Needs, P.W.; Kroon, P.A.; Rakotomanomana, N.; et al. Polyphenols bind to low density lipoprotein at biologically relevant concentrations that are protective for heart disease. Arch. Biochem. Biophys. 2020, 694, 108589. [Google Scholar] [CrossRef]
- Guo, H.; Liu, G.; Zhong, R.; Wang, Y.; Wang, D.; Xia, M. Cyanidin-3-O-β-glucoside regulates fatty acid metabolism via an AMP-activated protein kinase-dependent signaling pathway in human HepG2 cells. Lipids Health Dis. 2012, 11, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahdavi, A.; Bagherniya, M.; Fakheran, O.; Reiner, Ž.; Xu, S.; Sahebkar, A. Medicinal plants and bioactive natural compounds as inhibitors of HMG-CoA reductase: A literature review. BioFactors 2020, 46, 906–926. [Google Scholar] [CrossRef]
- Towler, M.C.; Hardie, G. AMP-Activated Protein Kinase in Metabolic Control and Insulin Signaling. Circ. Res. 2007, 100, 328–341. [Google Scholar] [CrossRef] [PubMed]
- Lorrain, B.; Dangles, O.; Genot, C.; Dufour, C. Chemical Modeling of Heme-Induced Lipid Oxidation in Gastric Conditions and Inhibition by Dietary Polyphenols. J. Agric. Food Chem. 2010, 58, 676–683. [Google Scholar] [CrossRef]
- Lorrain, B.; Dangles, O.; Loonis, M.; Armand, M.; Dufour, C. Dietary Iron-Initiated Lipid Oxidation and Its Inhibition by Polyphenols in Gastric Conditions. J. Agric. Food Chem. 2012, 60, 9074–9081. [Google Scholar] [CrossRef]
- Kim, B.; Park, Y.; Wegner, C.J.; Bolling, B.W.; Lee, J. Polyphenol-rich black chokeberry (Aronia melanocarpa) extract regulates the expression of genes critical for intestinal cholesterol flux in Caco-2 cells. J. Nutr. Biochem. 2013, 24, 1564–1570. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Ku, C.S.; Pham, T.X.; Park, Y.; Martin, D.A.; Xie, L.; Taheri, R.; Lee, J.; Bolling, B. Aronia melanocarpa (chokeberry) polyphenol–rich extract improves antioxidant function and reduces total plasma cholesterol in apolipoprotein E knockout mice. Nutr. Res. 2013, 33, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Duchnowicz, P.; Ziobro, A.; Rapacka, E.; Koter-Michalak, M.; Bukowska, B. Changes in Cholinesterase Activity in Blood of Adolescent with Metabolic Syndrome after Supplementation with Extract from Aronia melanocarpa. BioMed. Res. Int. 2018, 2018, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Škovierová, H.; Vidomanová, E.; Mahmood, S.; Sopková, J.; Drgová, A.; Červeňová, T.; Halašová, E.; Lehotský, J. The Molecular and Cellular Effect of Homocysteine Metabolism Imbalance on Human Health. Int. J. Mol. Sci. 2016, 17, 1733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lei, X.; Zeng, G.; Zhang, Y.; Li, Q.; Zhang, J.; Bai, Z.; Yang, K. Association between homocysteine level and the risk of diabetic retinopathy: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2018, 10, 61. [Google Scholar] [CrossRef]
- Agoston-Coldea, L.; Mocan, T.; Gatfosse, M.; Lupu, S.; Dumitrascu, D.L. Plasma homocysteine and the severity of heart failure in patients with previous myocardial infarction. Cardiol. J. 2011, 18, 55–62. [Google Scholar]
- Yeh, J.-K.; Chen, C.-C.; Hsieh, M.-J.; Tsai, M.-L.; Yang, C.-H.; Chen, D.-Y.; Chang, S.-H.; Wang, C.-Y.; Lee, C.-H.; Hsieh, I.-C. Impact of Homocysteine Level on Long-term Cardiovascular Outcomes in Patients after Coronary Artery Stenting. J. Atheroscler. Thromb. 2017, 24, 696–705. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Hu, F.B.; Manson, J.E. Marine Omega-3 Supplementation and Cardiovascular Disease: An Updated Meta-Analysis of 13 Randomized Controlled Trials Involving 127 477 Participants. J. Am. Heart Assoc. 2019, 8, e013543. [Google Scholar] [CrossRef]
- Kaneva, A.M.; Potolitsyna, N.N.; Bojko, E.R.; Odland, J. The Apolipoprotein B/Apolipoprotein A-I Ratio as a Potential Marker of Plasma Atherogenicity. Dis. Markers 2015, 2015, 591454. [Google Scholar] [CrossRef] [Green Version]
- Xie, L.; Vance, T.; Kim, B.; Gil Lee, S.G.; Caceres, C.; Wang, Y.; Hubert, P.A.; Lee, J.-Y.; Chun, O.K.; Bolling, B.W. Aronia berry polyphenol consumption reduces plasma total and low-density lipoprotein cholesterol in former smokers without lowering biomarkers of inflammation and oxidative stress: A randomized controlled trial. Nutr. Res. 2016, 37, 67–77. [Google Scholar] [CrossRef]
- Nowak, D.; Grąbczewska, Z.; Gośliński, M.; Obońska, K.; Dąbrowska, A.; Kubica, J. Effect of chokeberry juice consumption on antioxidant capacity, lipids profile and endothelial function in healthy people: A pilot study. Czech J. Food Sci. 2016, 34, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Di Gioia, M.; Zanoni, I. Dooming Phagocyte Responses: Inflammatory Effects of Endogenous Oxidized Phospholipids. Front. Endocrinol. 2021, 12, 626842. [Google Scholar] [CrossRef]
- Yavuzer, H.; Yavuzer, S.; Cengiz, M.; Erman, H.; Doventas, A.; Balci, H.; Erdincler, D.S.; Uzun, H. Biomarkers of lipid peroxidation related to hypertension in aging. Hypertens. Res. 2016, 39, 342–348. [Google Scholar] [CrossRef]
- Duchnowicz, P.; Nowicka, A.; Koter-Michalak, M.; Broncel, M. In vivo influence of extract from Aronia melanocarpa on the erythrocyte membranes in patients with hypercholesterolemia. Med. Sci. Monit. 2012, 18, CR569–CR574. [Google Scholar] [CrossRef] [Green Version]
- Pilaczynska-Szczesniak, L.; Skarpanska-Steinborn, A.; Deskur, E.; Basta, P.; Horoszkiewicz-Hassan, M. The Influence of Chokeberry Juice Supplementation on the Reduction of Oxidative Stress Resulting from an Incremental Rowing Ergometer Exercise. Int. J. Sport Nutr. Exerc. Metab. 2005, 15, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Stojković, L.; Zec, M.; Zivkovic, M.; Bundalo, M.; Bošković, M.; Glibetić, M.; Stankovic, A. Polyphenol-Rich Aronia melanocarpa Juice Consumption Affects LINE-1 DNA Methylation in Peripheral Blood Leukocytes in Dyslipidemic Women. Front. Nutr. 2021, 8, 689055. [Google Scholar] [CrossRef] [PubMed]
- Pearce, M.S.; McConnell, J.C.; Potter, C.; Barrett, L.M.; Parker, L.; Mathers, J.C.; Relton, C.L. Global LINE-1 DNA methylation is associated with blood glycaemic and lipid profiles. Int. J. Epidemiol. 2012, 41, 210–217. [Google Scholar] [CrossRef] [Green Version]
- Martín-Núñez, G.M.; Rubio-Martín, E.; Cabrera-Mulero, R.; Rojo-Martínez, G.; Olveira, G.; Valdés, S.; Soriguer, F.; Castaño, L.; Morcillo, S. Type 2 diabetes mellitus in relation to global LINE-1 DNA methylation in peripheral blood: A cohort study. Epigenetics 2014, 9, 1322–1328. [Google Scholar] [CrossRef] [Green Version]
- Cash, H.L.; McGarvey, S.T.; Houseman, E.A.; Marsit, C.J.; Hawley, N.L.; Lambert-Messerlian, G.M.; Viali, S.; Tuitele, J.; Kelsey, K.T. Cardiovascular disease risk factors and DNA methylation at theLINE-1repeat region in peripheral blood from Samoan Islanders. Epigenetics 2011, 6, 1257–1264. [Google Scholar] [CrossRef] [Green Version]
- Pan, M.-H.; Lai, C.-S.; Wu, J.-C.; Ho, C.-T. Epigenetic and Disease Targets by Polyphenols. Curr. Pharm. Des. 2013, 19, 6156–6185. [Google Scholar] [CrossRef]
- Liu, G.; Bin, P.; Wang, T.; Ren, W.; Zhong, J.; Liang, J.; Hu, C.-A.A.; Zeng, Z.; Yin, Y. DNA Methylation and the Potential Role of Methyl-Containing Nutrients in Cardiovascular Diseases. Oxidative Med. Cell. Longev. 2017, 2017, 1670815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, W.; Larbi, A. Immunity and Inflammation: From Jekyll to Hyde. Exp. Gerontol. 2018, 107, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Kotas, M.E.; Medzhitov, R. Homeostasis, Inflammation, and Disease Susceptibility. Cell 2015, 160, 816–827. [Google Scholar] [CrossRef] [Green Version]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic inflammation in the etiology of disease across the life span. Nat. Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Xian, X.; Wang, Z.; Bi, Y.; Chen, Q.; Han, X.; Tang, D.; Chen, R. Research Progress on the Relationship between Atherosclerosis and Inflammation. Biomolecules 2018, 8, 80. [Google Scholar] [CrossRef] [Green Version]
- Golia, E.; Limongelli, G.; Natale, F.; Fimiani, F.; Maddaloni, V.; Pariggiano, I.; Bianchi, R.; Crisci, M.; D’Acierno, L.; Giordano, R.; et al. Inflammation and Cardiovascular Disease: From Pathogenesis to Therapeutic Target. Curr. Atheroscler. Rep. 2014, 16, 435. [Google Scholar] [CrossRef]
- Lontchi-Yimagou, E.; Sobngwi, E.; Matsha, T.E.; Kengne, A.P. Diabetes Mellitus and Inflammation. Curr. Diabetes Rep. 2013, 13, 435–444. [Google Scholar] [CrossRef]
- Koyama, Y.; Brenner, D.A. Liver inflammation and fibrosis. J. Clin. Investig. 2017, 127, 55–64. [Google Scholar] [CrossRef]
- Kimura, T.; Isaka, Y.; Yoshimori, T. Autophagy and kidney inflammation. Autophagy 2017, 13, 997–1003. [Google Scholar] [CrossRef]
- Stephenson, J.; Nutma, E.; Van Der Valk, P.; Amor, S. Inflammation in CNS neurodegenerative diseases. Immunology 2018, 154, 204–219. [Google Scholar] [CrossRef] [Green Version]
- Banerjee, S.; Biehl, A.; Gadina, M.; Hasni, S.; Schwartz, D. JAK–STAT Signaling as a Target for Inflammatory and Autoimmune Diseases: Current and Future Prospects. Drugs 2017, 77, 521–546. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Deng, H.; Cui, H.; Fang, J.; Zuo, Z.; Deng, J.; Li, Y.; Wang, X.; Zhao, L. Inflammatory responses and inflammation-associated diseases in organs. Oncotarget 2018, 9, 7204–7218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arulselvan, P.; Fard, M.T.; Tan, W.S.; Gothai, S.; Fakurazi, S.; Norhaizan, M.E.; Kumar, S.S. Role of Antioxidants and Natural Products in Inflammation. Oxid. Med. Cell. Longev. 2016, 2016, 5276130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menzel, A.; Samouda, H.; Dohet, F.; Loap, S.; Ellulu, M.S.; Bohn, T. Common and Novel Markers for Measuring Inflammation and Oxidative Stress Ex Vivo in Research and Clinical Practice—Which to Use Regarding Disease Outcomes? Antioxidants 2021, 10, 414. [Google Scholar] [CrossRef] [PubMed]
- Appel, K.; Meiser, P.; Millán, E.; Collado, J.A.; Rose, T.; Gras, C.C.; Carle, R.; Muñoz, E. Chokeberry (Aronia melanocarpa (Michx.) Elliot) concentrate inhibits NF-κB and synergizes with selenium to inhibit the release of pro-inflammatory mediators in macrophages. Fitoterapia 2015, 105, 73–82. [Google Scholar] [CrossRef]
- Iwashima, T.; Kudome, Y.; Kishimoto, Y.; Saita, E.; Tanaka, M.; Taguchi, C.; Hirakawa, S.; Mitani, N.; Kondo, K.; Iida, K. Aronia berry extract inhibits TNF-α-induced vascular endothelial inflammation through the regulation of STAT3. Food Nutr. Res. 2019, 63. [Google Scholar] [CrossRef] [Green Version]
- Ailuno, G.; Zuccari, G.; Baldassari, S.; Lai, F.; Caviglioli, G. Anti-Vascular Cell Adhesion Molecule-1 Nanosystems: A Promising Strategy Against Inflammatory Based Diseases. J. Nanosci. Nanotechnol. 2021, 21, 2793–2807. [Google Scholar] [CrossRef]
- Witkowska, A.M.; Borawska, M.H. Soluble intercellular adhesion molecule-1 (sICAM-1): An overview. Eur. Cytokine Netw. 2004, 15, 91–98. [Google Scholar]
- Lin, J.; Kakkar, V.; Lu, X. Impact of MCP -1 in Atherosclerosis. Curr. Pharm. Des. 2014, 20, 4580–4588. [Google Scholar] [CrossRef]
- Wiesner, P.; Tafelmeier, M.; Chittka, D.; Choi, S.-H.; Zhang, L.; Byun, Y.S.; Almazan, F.; Yang, X.; Iqbal, N.; Chowdhury, P.; et al. MCP-1 binds to oxidized LDL and is carried by lipoprotein(a) in human plasma. J. Lipid Res. 2013, 54, 1877–1883. [Google Scholar] [CrossRef] [Green Version]
- Milne, G.L.; Musiek, E.S.; Morrow, J.D. F2-Isoprostanes as markers of oxidative stress in vivo: An overview. Biomarkers 2005, 10 (Suppl. 1), 10–23. [Google Scholar] [CrossRef] [PubMed]
- Proudfoot, J.M.; Murrey, M.W.; McLean, S.; Greenland, E.L.; Barden, A.E.; Croft, K.D.; Galano, J.-M.; Durand, T.A.; Mori, T.; Pixley, F.J. F2-isoprostanes affect macrophage migration and CSF-1 signalling. Free Radic. Biol. Med. 2018, 126, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Milosavljevic, I.; Jakovljevic, V.; Petrovic, D.; Draginic, N.; Jeremic, J.; Mitrovic, M.; Zivkovic, V.; Srejovic, I.; Stojic, V.; Bolevich, S.; et al. Standardized Aronia melanocarpa extract regulates redox status in patients receiving hemodialysis with anemia. Mol. Cell. Biochem. 2021, 476, 4167–4175. [Google Scholar] [CrossRef] [PubMed]
- Serafini, M.; Peluso, I. Functional Foods for Health: The Interrelated Antioxidant and Anti-Inflammatory Role of Fruits, Vegetables, Herbs, Spices and Cocoa in Humans. Curr. Pharm. Des. 2016, 22, 6701–6715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.-Q.; Zhou, J.-C.; Wu, Y.-Y.; Ren, F.-Z.; Lei, X.G. Role of glutathione peroxidase 1 in glucose and lipid metabolism-related diseases. Free Radic. Biol. Med. 2018, 127, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Lubos, E.; Loscalzo, J.; Handy, D.E. Glutathione Peroxidase-1 in Health and Disease: From Molecular Mechanisms to Therapeutic Opportunities. Antioxid. Redox Signal. 2011, 15, 1957–1997. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.H.; Batist, G. Glutathione and glutathione analogues; Therapeutic potentials. Biochim. Biophys. Acta 2013, 1830, 3350–3353. [Google Scholar] [CrossRef]
- Loeffen, R.; Spronk, H.M.H.; Cate, H.T. The impact of blood coagulability on atherosclerosis and cardiovascular disease. J. Thromb. Haemost. 2012, 10, 1207–1216. [Google Scholar] [CrossRef]
- Seegers, W.H. Blood Clotting Enzymology; Academic Press: London, UK, 1967; pp. 1–21. [Google Scholar]
- Vita, J.A. Polyphenols and cardiovascular disease: Effects on endothelial and platelet function. Am. J. Clin. Nutr. 2005, 81, 292S–297S. [Google Scholar] [CrossRef]
- Bijak, M.; Bobrowski, M.; Borowiecka, M.; Podsędek, A.; Golański, J.; Nowak, P. Anticoagulant effect of polyphenols-rich extracts from black chokeberry and grape seeds. Fitoterapia 2011, 82, 811–817. [Google Scholar] [CrossRef]
- Malinowska, J.; Babicz, K.; Olas, B.; Stochmal, A.; Oleszek, W. Aronia melanocarpa extract suppresses the biotoxicity of homocysteine and its metabolite on the hemostatic activity of fibrinogen and plasma. Nutrition 2012, 28, 793–798. [Google Scholar] [CrossRef] [PubMed]
- Sikora, J.; Markowicz-Piasecka, M.; Broncel, M.; Mikiciuk-Olasik, E. Extract of Aronia melanocarpa-modified hemostasis: In vitro studies. Eur. J. Nutr. 2014, 53, 1493–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevanović, V.; Pantović, A.; Krga, I.; Zeković, M.; Šarac, I.; Glibetić, M.; Vidović, N. Aronia juice consumption prior to half-marathon race can acutely affect platelet activation in recreational runners. Appl. Physiol. Nutr. Metab. 2020, 45, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Arias, I.M.; Alter, H.J.; Boyer, J.L.; Cohen, D.E.; Shafritz, D.A.; Thorgeirsson, S.S.; Wolkoff, A.W. The Liver: Biology and Pathobiology, 6th ed.; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2020. [Google Scholar]
- Mansouri, A.; Gattolliat, C.-H.; Asselah, T. Mitochondrial Dysfunction and Signaling in Chronic Liver Diseases. Gastroenterology 2018, 155, 629–647. [Google Scholar] [CrossRef] [Green Version]
- Ceriotti, F.; Henny, J.; Queraltó, J.; Ziyu, S.; Özarda, Y.; Chen, B.; Boyd, J.C.; Panteghini, M. Common reference intervals for aspartate aminotransferase (AST), alanine aminotransferase (ALT) and γ-glutamyl transferase (GGT) in serum: Results from an IFCC multicenter study. Clin. Chem. Lab. Med. 2010, 48, 1593–1601. [Google Scholar] [CrossRef]
- Li, S.; Tan, H.-Y.; Wang, N.; Zhang, Z.-J.; Lao, L.; Wong, C.-W.; Feng, Y. The Role of Oxidative Stress and Antioxidants in Liver Diseases. Int. J. Mol. Sci. 2015, 16, 26087–26124. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Tan, H.Y.; Wang, N.; Cheung, F.; Hong, M.; Feng, Y. The Potential and Action Mechanism of Polyphenols in the Treatment of Liver Diseases. Oxid. Med. Cell. Longev. 2018, 2018, 8394818. [Google Scholar] [CrossRef] [Green Version]
- Mężyńska, M.; Brzóska, M.M.; Rogalska, J.; Piłat-Marcinkiewicz, B. Extract from Aronia melanocarpa L. Berries Prevents Cadmium-Induced Oxidative Stress in the Liver: A Study in A Rat Model of Low-Level and Moderate Lifetime Human Exposure to this Toxic Metal. Nutrients 2018, 11, 21. [Google Scholar] [CrossRef] [Green Version]
- Park, C.-H.; Kim, J.-H.; Lee, E.B.; Hur, W.; Kwon, O.-J.; Park, H.-J.; Yoon, S.K. Aronia melanocarpa Extract Ameliorates Hepatic Lipid Metabolism through PPARγ2 Downregulation. PLoS ONE 2017, 12, e0169685. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Gao, J.; Yu, W.; Hao, R.; Fan, J.; Wei, J. The effects and mechanism of Aronia melanocarpa Elliot anthocyanins on hepatic fibrosis. J. Funct. Foods 2020, 68, 103897. [Google Scholar] [CrossRef]
- Kozłowska, M.; Brzóska, M.M.; Rogalska, J.; Galicka, A. The Impact of a Polyphenol-Rich Extract from the Berries of Aronia melanocarpa L. on Collagen Metabolism in the Liver: A Study in an In Vivo Model of Human Environmental Exposure to Cadmium. Nutrients 2020, 12, 2766. [Google Scholar] [CrossRef] [PubMed]
- Glantzounis, G.K.; Tsimoyiannis, E.C.; Kappas, A.M.; Galaris, D.A. Uric Acid and Oxidative Stress. Curr. Pharm. Des. 2005, 11, 4145–4151. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.H.; Gladden, J.D.; Ahmed, M.; Ahmed, A.; Filippatos, G. Relation of serum uric acid to cardiovascular disease. Int. J. Cardiol. 2016, 213, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, A.; Kaze, A.D.; McMullan, C.J.; Isakova, T.; Waikar, S.S. Uric Acid and the Risks of Kidney Failure and Death in Individuals With CKD. Am. J. Kidney Dis. 2018, 71, 362–370. [Google Scholar] [CrossRef]
- Yanai, H.; Adachi, H.; Hakoshima, M.; Katsuyama, H. Molecular Biological and Clinical Understanding of the Pathophysiology and Treatments of Hyperuricemia and Its Association with Metabolic Syndrome, Cardiovascular Diseases and Chronic Kidney Disease. Int. J. Mol. Sci. 2021, 22, 9221. [Google Scholar] [CrossRef]
- Wang, J.; Qin, T.; Chen, J.; Li, Y.; Wang, L.; Huang, H.; Li, J. Hyperuricemia and Risk of Incident Hypertension: A Systematic Review and Meta-Analysis of Observational Studies. PLoS ONE 2014, 9, e114259. [Google Scholar] [CrossRef] [Green Version]
- Lv, Q.; Meng, X.-F.; He, F.-F.; Chen, S.; Su, H.; Xiong, J.; Gao, P.; Tian, X.-J.; Liu, J.-S.; Zhu, Z.-H.; et al. High Serum Uric Acid and Increased Risk of Type 2 Diabetes: A Systemic Review and Meta-Analysis of Prospective Cohort Studies. PLoS ONE 2013, 8, e56864. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Yang, H.; Chen, Y.; Wang, J.; Xu, L.; Miao, M.; Xu, C. Association between serum uric acid levels and dyslipidemia in Chinese adults: A cross-sectional study and further meta-analysis. Medicine 2020, 99, e19088. [Google Scholar] [CrossRef]
- Sautin, Y.Y.; Johnson, R.J. Uric Acid: The Oxidant-Antioxidant Paradox. Nucleosides Nucleotides Nucleic Acids 2008, 27, 608–619. [Google Scholar] [CrossRef] [Green Version]
- Lippi, G.; Montagnana, M.; Franchini, M.; Favaloro, E.J.; Targher, G. The paradoxical relationship between serum uric acid and cardiovascular disease. Clin. Chim. Acta 2008, 392, 1–7. [Google Scholar] [CrossRef]
- Li, L.; Li, J.; Xu, H.; Zhu, F.; Li, Z.; Lu, H.; Zhang, J.; Yang, Z.; Liu, Y. The Protective Effect of Anthocyanins Extracted from Aronia Melanocarpa Berry in Renal Ischemia-Reperfusion Injury in Mice. Mediat. Inflamm. 2021, 2021, 7372893. [Google Scholar] [CrossRef] [PubMed]
- Delanaye, P.; Cavalier, E.; Pottel, H. Serum Creatinine: Not So Simple! Nephron 2017, 136, 302–308. [Google Scholar] [CrossRef]
- Khosla, N.; Sarafidis, P.A.; Bakris, G.L. Microalbuminuria. Clin. Lab. Med. 2006, 26, 635–653. [Google Scholar] [CrossRef] [PubMed]
- Savarese, G.; Dei Cas, A.; Rosano, G.; D’Amore, C.; Musella, F.; Mosca, S.; Reiner, M.F.; Marchioli, R.; Trimarco, B.; Perrone-Filardi, P. Reduction of albumin urinary excretion is associated with reduced cardiovascular events in hypertensive and/or diabetic patients. A meta-regression analysis of 32 randomized trials. Int. J. Cardiol. 2014, 172, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Hong, Z.; Jiang, Y.; Liu, P.; Zhang, L. Association of microalbuminuria and adverse outcomes in hypertensive patients: A meta-analysis. Int. Urol. Nephrol. 2021, 53, 2311–2319. [Google Scholar] [CrossRef]
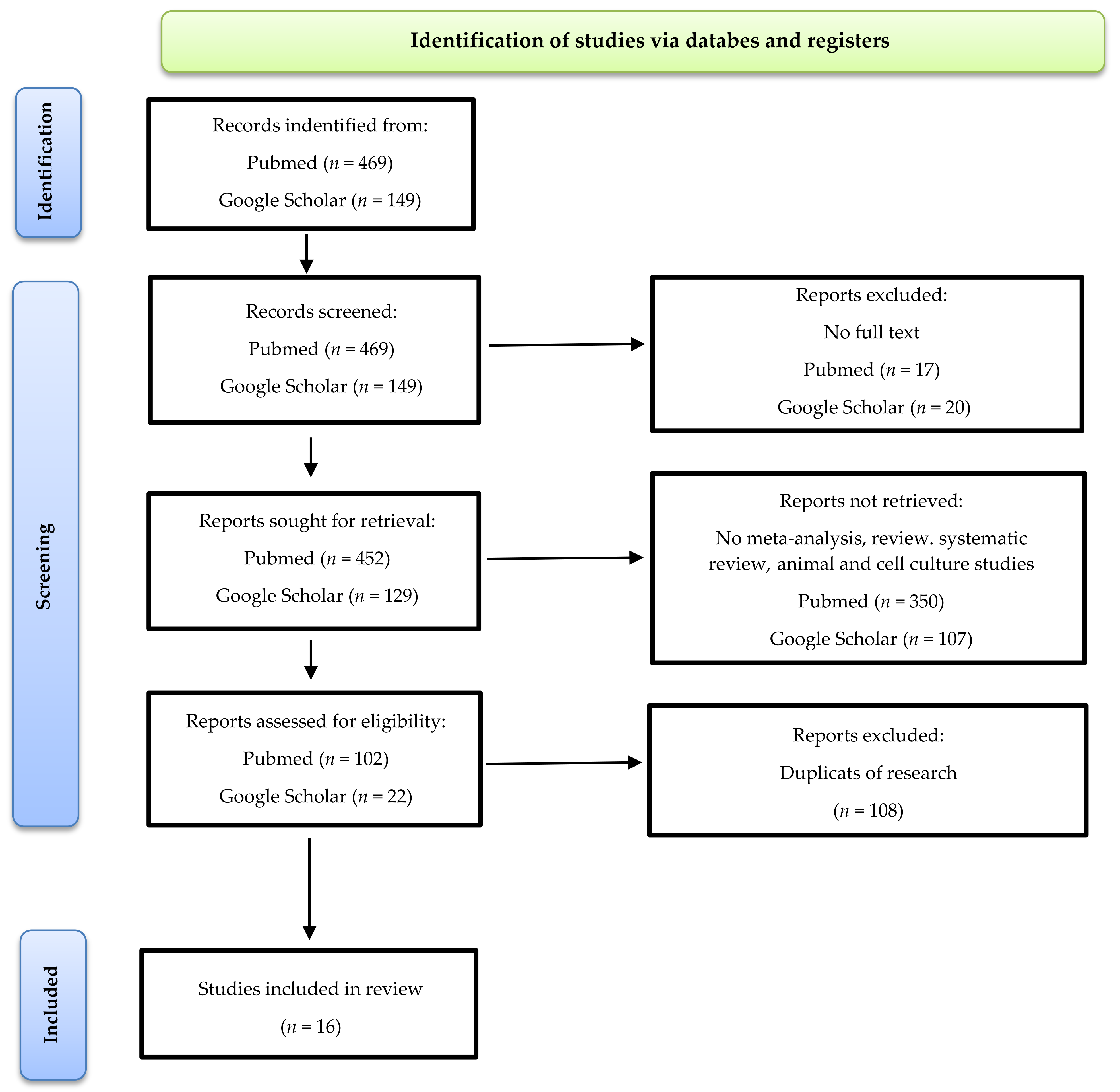
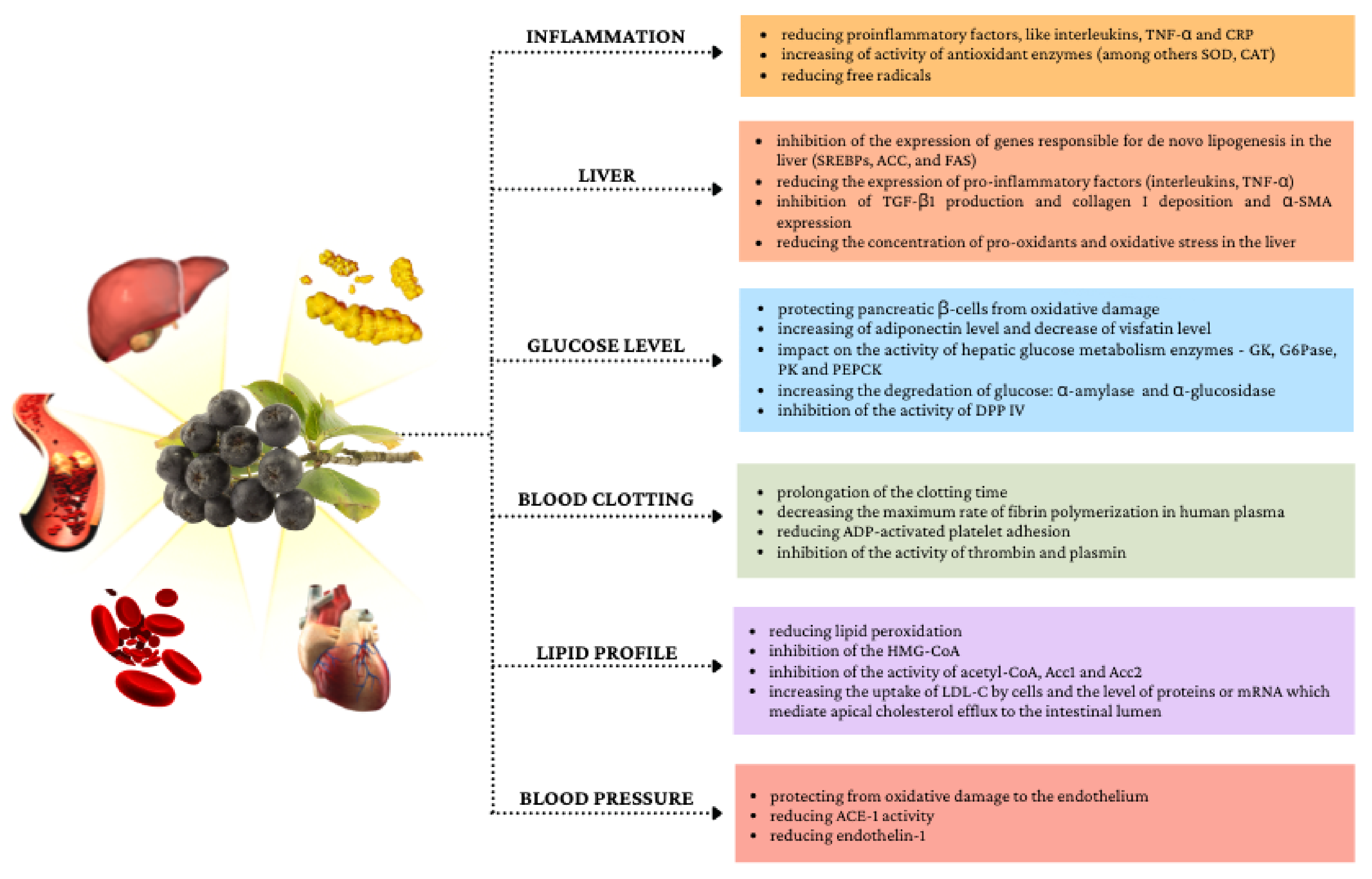
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olechno, E.; Puścion-Jakubik, A.; Zujko, M.E. Chokeberry (A. melanocarpa (Michx.) Elliott)—A Natural Product for Metabolic Disorders? Nutrients 2022, 14, 2688. https://doi.org/10.3390/nu14132688
Olechno E, Puścion-Jakubik A, Zujko ME. Chokeberry (A. melanocarpa (Michx.) Elliott)—A Natural Product for Metabolic Disorders? Nutrients. 2022; 14(13):2688. https://doi.org/10.3390/nu14132688
Chicago/Turabian StyleOlechno, Ewa, Anna Puścion-Jakubik, and Małgorzata Elżbieta Zujko. 2022. "Chokeberry (A. melanocarpa (Michx.) Elliott)—A Natural Product for Metabolic Disorders?" Nutrients 14, no. 13: 2688. https://doi.org/10.3390/nu14132688
APA StyleOlechno, E., Puścion-Jakubik, A., & Zujko, M. E. (2022). Chokeberry (A. melanocarpa (Michx.) Elliott)—A Natural Product for Metabolic Disorders? Nutrients, 14(13), 2688. https://doi.org/10.3390/nu14132688