
Evaluating the Efficacy of Probiotics in IBS Treatment Using a Systematic Review of Clinical Trials and Multi-Criteria Decision Analysis



Abstract
:1. Introduction
2. Materials and Methods
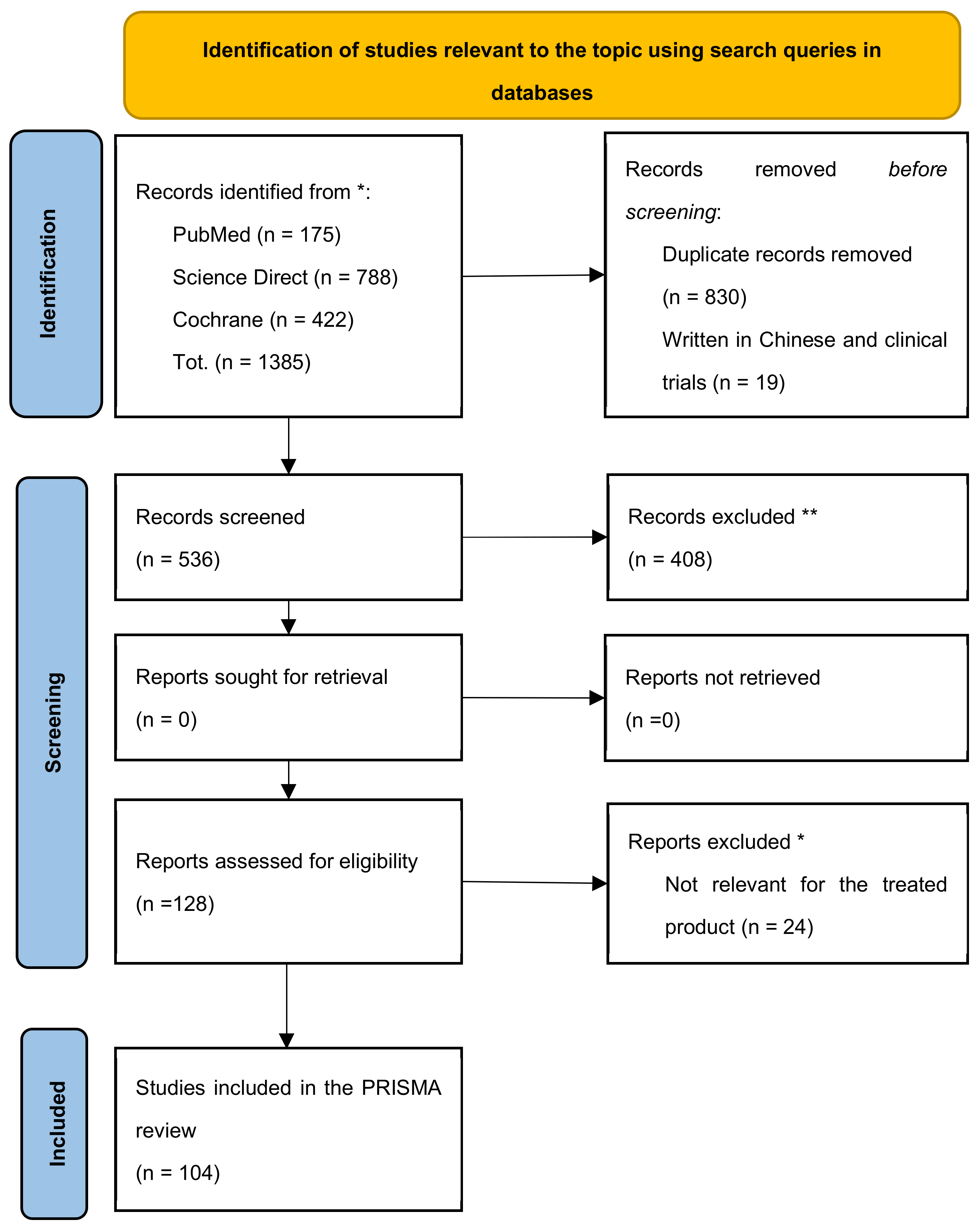
2.1. PRISMA Method
Identification of Studies Using Databases and Registries
- -
- Year: year of publication, between 2011 and 2021.
- -
- Title: title of the article.
- -
- First author: first author’s name and primary affiliation.
- -
- Country: country and continent where the study was conducted.
- -
- Journal: peer-review journal of publication, with related impact factor.
- -
- Product: probiotic, prebiotic, and symbiotic under investigation by the clinical trial.
- -
- Type of composition: type of composition of each product and their possible combined formulation (probiotic, prebiotic, symbiotic, probiotic mix, prebiotic mix, and symbiotic mix).
- -
- Composition: bacterial strain i.e., name(s) of the probiotic(s) and prebiotic(s).
2.2. Multi-Criteria Decision Making Analysis—MCDA
- -
- -
- Bifidobacterium animalis subsp. lactis, Lactobacillus acidophilus [37] (nr. 1)
- -
Limits of the Study
3. Results
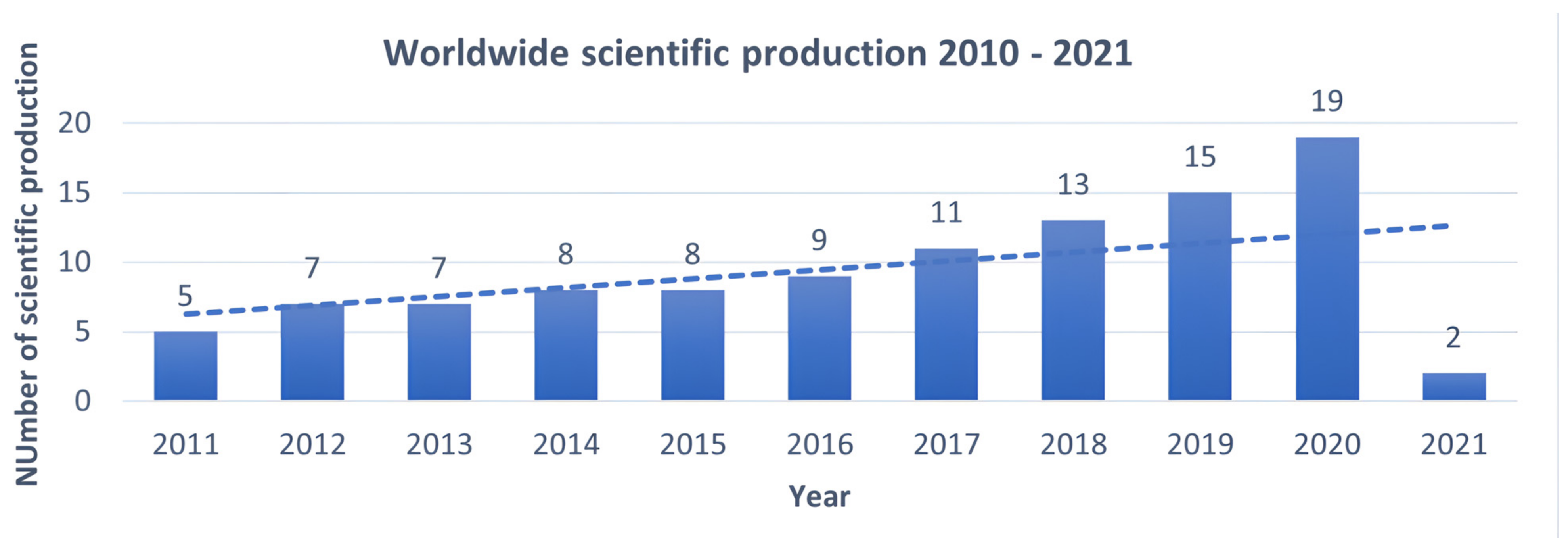
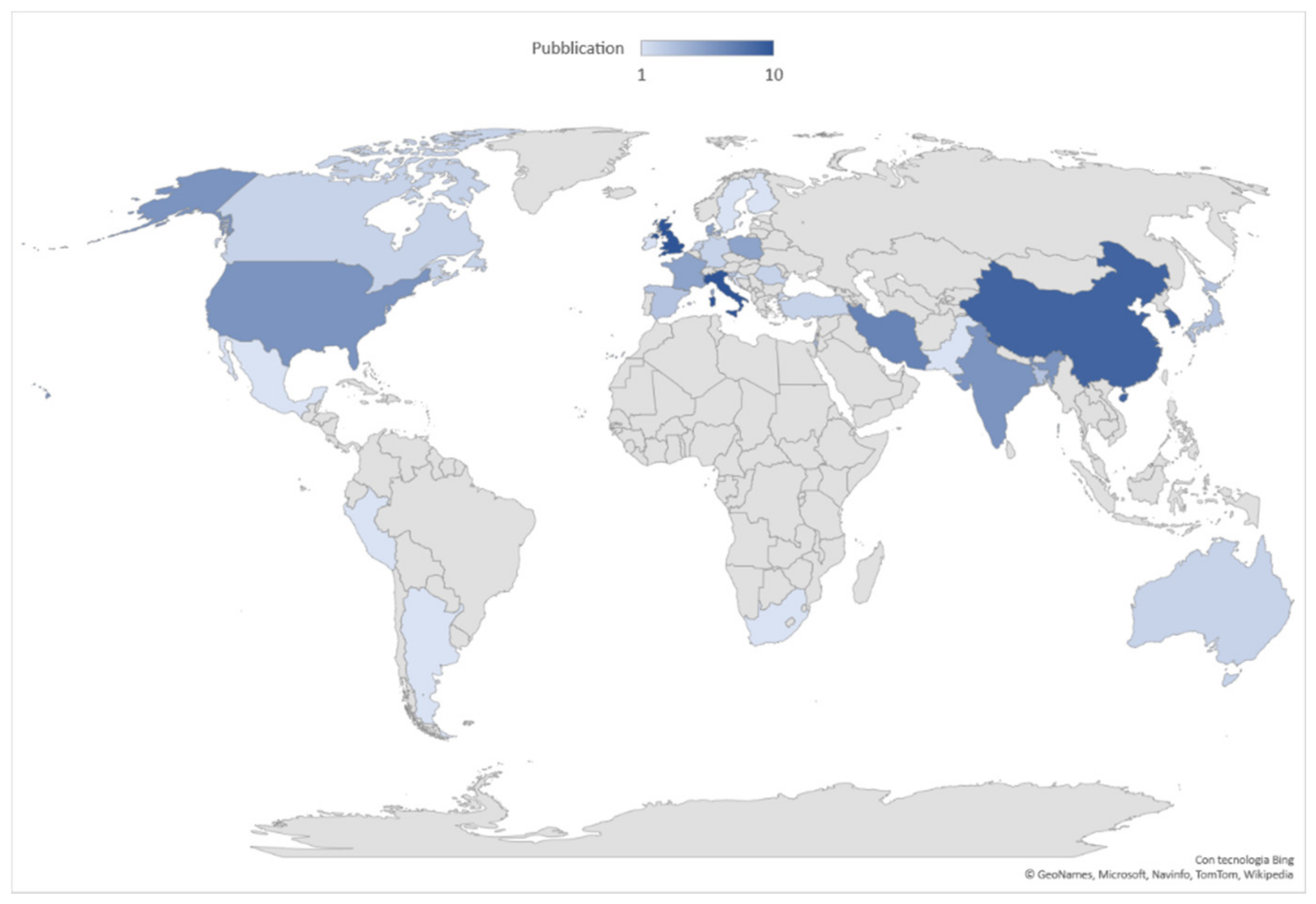
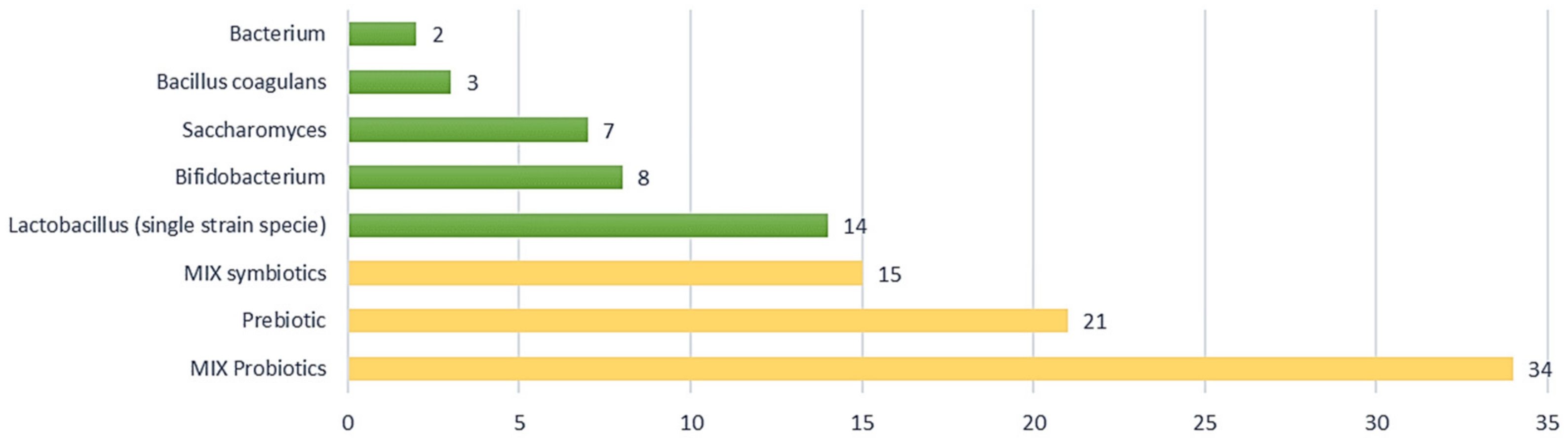
3.1. PRISMA Results
- -
- probiotic, tested individually and combined forms of different strains;
- -
- prebiotic, tested individually and combined form of different strains;
- -
- symbiotic, testing the effect of combined forms of probiotics with prebiotics.
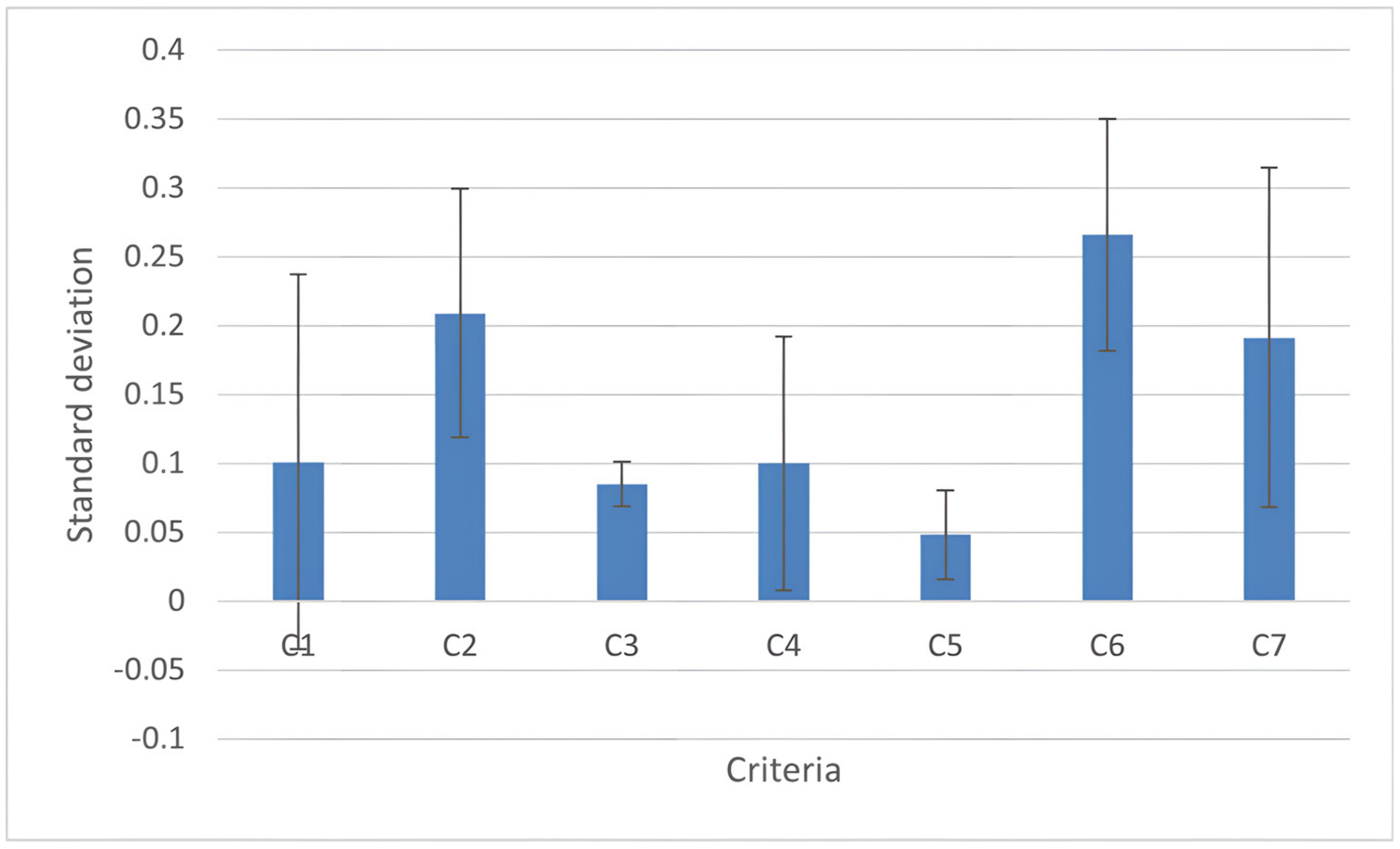
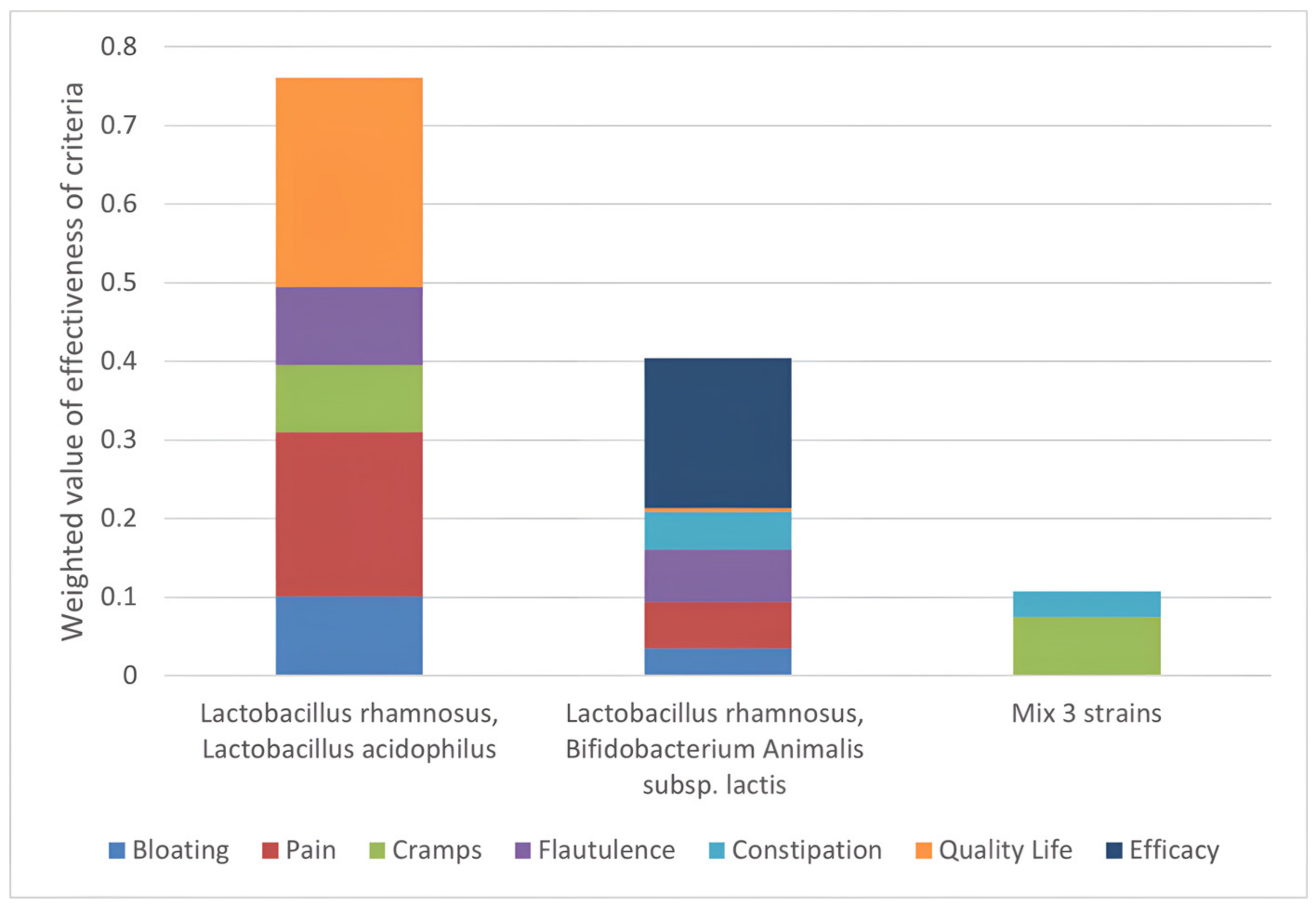
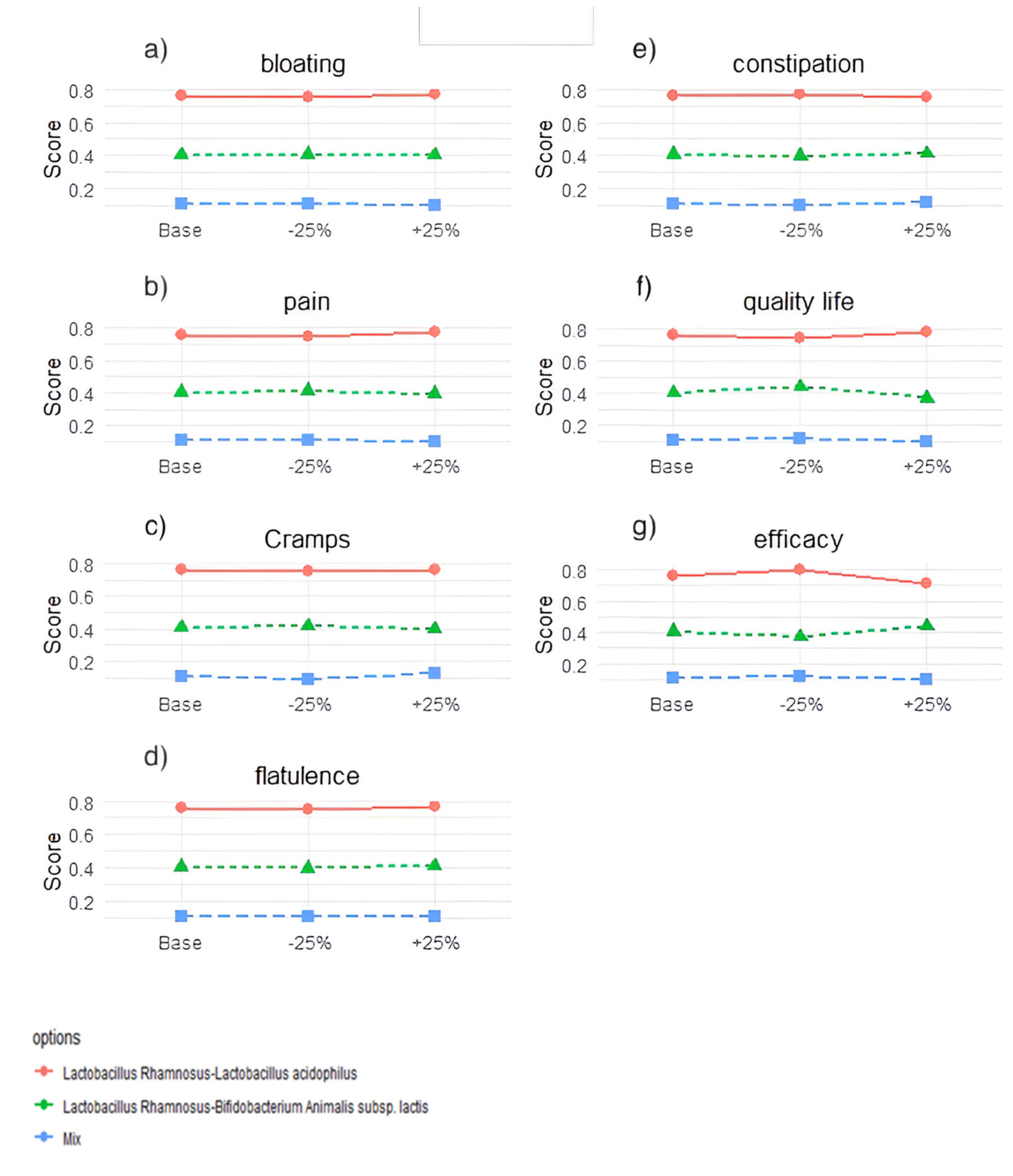
3.2. MCDA Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Toscano, M.; De Grandi, R.; Pastorelli, L.; Vecchi, M.; Drago, L. A consumer’s guide for probiotics: 10 golden rules for a correct use. Dig. Liver Dis. 2017, 49, 1177–1184. [Google Scholar] [CrossRef]
- Giorgi, P.L. Probiotici. Recenti Progress. Med. 2009, 100, 40–47. [Google Scholar]
- Ford, A.C.; Lacy, B.E.; Talley, N.J. Irritable Bowel Syndrome. N. Engl. J. Med. 2017, 376, 2566–2578. [Google Scholar] [CrossRef] [Green Version]
- Szałwińska, P.; Włodarczyk, J.; Spinelli, A.; Fichna, J.; Włodarczyk, M. IBS-Symptoms in IBD Patients-Manifestation of Concomitant or Different Entities. J. Clin. Med. 2020, 10, 31. [Google Scholar] [CrossRef]
- Staudacher, H.M.; Whelan, K. Altered gastrointestinal microbiota in irritable bowel syndrome and its modification by diet: Probiotics, prebiotics and the low FODMAP diet. Proc. Nutr. Soc. 2016, 75, 306–318. [Google Scholar] [CrossRef]
- Gibson, G.R.; Beatty, E.R.; Wang, X.; Cummings, J.H. Selective stimulation of bifidobacteria in the human colon by oligofructose and inulin. Gastroenterology 1995, 108, 975–982. [Google Scholar] [CrossRef]
- Ahmed, S.; Raza, K.A. Irritable Bowel Syndrome: Clinical Review. World Fam. Med. J. Middle East J. Fam. Med. 2020, 18, 106–114. [Google Scholar] [CrossRef]
- Chong, P.P.; Chin, V.K.; Looi, C.Y.; Wong, W.F.; Madhavan, P.; Yong, V.C. The Microbiome and Irritable Bowel Syndrome-A Review on the Pathophysiology, Current Research and Future Therapy. Front. Microbiol. 2019, 10, 1136. [Google Scholar] [CrossRef] [Green Version]
- Holvoet, T.; Joossens, M.; Vázquez-Castellanos, J.F.; Christiaens, E.; Heyerick, L.; Boelens, J.; Verhasselt, B.; van Vlierberghe, H.; De Vos, M.; Raes, J.; et al. Fecal Microbiota Transplantation Reduces Symptoms in Some Patients With Irritable Bowel Syndrome With Predominant Abdominal Bloating: Short- and Long-term Results From a Placebo-Controlled Randomized Trial. Gastroenterology 2021, 160, 145–157.e8. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, L.; Guo, C.; Mu, D.; Feng, B.; Zuo, X.; Li, Y. Effects of probiotic type, dose and treatment duration on irritable bowel syndrome diagnosed by Rome III criteria: A meta-analysis. BMC Gastroenterol. 2016, 16, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, D.; Longgui, N.; Guoqiang, X. Efficacy of different probiotic protocols in irritable bowel syndrome: A network meta-analysis. Medicine 2019, 98, e16068. [Google Scholar] [CrossRef]
- Didari, T.; Mozaffari, S.; Nikfar, S.; Abdollahi, M. Effectiveness of probiotics in irritable bowel syndrome: Updated systematic review with meta-analysis. World J. Gastroenterol. 2015, 21, 3072–3084. [Google Scholar] [CrossRef]
- Ferreira, A.I.; Garrido, M.; Castro-Poças, F. Irritable Bowel Syndrome: News from an Old Disorder. GE Port. J. Gastroenterol. 2020, 27, 255–268. [Google Scholar] [CrossRef]
- Radovanovic-Dinic, B.; Tesic-Rajkovic, S.; Grgov, S.; Petrovic, G.; Zivkovic, V. Irritable bowel syndrome-From etiopathogenesis to therapy. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czechoslov. 2018, 162, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1–e34. [Google Scholar] [CrossRef]
- Gatto, F.; Daniotti, S.; Re, I. Driving green investments by measuring innovation impacts. Multi-Criteria Decision Analysis for regional bioeconomy growth. Sustainability 2021, 13, 11709. [Google Scholar] [CrossRef]
- Wahlster, P.; Goetghebeur, M.; Kriza, C.; Niederländer, C.; Kolominsky-Rabas, P. Balancing costs and benefits at different stages of medical innovation: A systematic review of Multi-criteria decision analysis (MCDA). BMC Health Serv. Res. 2015, 15, 262. [Google Scholar] [CrossRef] [Green Version]
- Polisena, J.; Clifford, T.; Elshaug, A.; Mitton, C.; Russell, E.; Skidmore, B. Case studies that illustrate disinvestment and resource allocation decision-making processes in health care: A systematic review. Int. J. Technol. Assess. Health Care 2013, 29, 174–184. [Google Scholar] [CrossRef] [PubMed]
- Adunlin, G.; Diaby, V.; Montero, A.J.; Xiao, H. Multicriteria decision analysis in oncology. Health Expect. 2015, 18, 1812–1826. [Google Scholar] [CrossRef] [PubMed]
- Dehe, B.; Bamford, D. Development, test and comparison of two Multiple Criteria Decision Analysis (MCDA) models: A case of healthcare infrastructure location. Expert Syst. Appl. 2015, 42, 6717–6727. [Google Scholar] [CrossRef] [Green Version]
- Rutten-van Mölken, M.; Leijten, F.; Hoedemakers, M.; Tsiachristas, A.; Verbeek, N.; Karimi, M.; Bal, R.; de Bont, A.; Islam, K.; Askildsen, J.E.; et al. Strengthening the evidence-base of integrated care for people with multi-morbidity in Europe using Multi-Criteria Decision Analysis (MCDA). BMC Health Serv. Res. 2018, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tervonen, T.; van Valkenhoef, G.; Buskens, E.; Hillege, H.L.; Postmus, D. A stochastic multicriteria model for evidence-based decision making in drug benefit-risk analysis. Stat. Med. 2011, 30, 1419–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunes, L.C.; Pinheiro, P.R.; Pequeno, T.C.; Pinheiro, M.C.D. Toward an Application to Psychological Disorders Diagnosis. In Advances in Experimental Medicine and Biology; Springer: New York, NY, USA, 2011; p. 8. [Google Scholar]
- Danner, M.; Gerber-Grote, A. Analytic Hierarchy Process. In Patient Involvement in Health Technology Assessment; Adis: Singapore, 2017; pp. 135–147. ISBN 978-981-10-4067-2. [Google Scholar]
- Glaize, A.; Duenas, A.; Di Martinelly, C.; Fagnot, I. Healthcare decision-making applications using multicriteria decision analysis: A scoping review. J. Multi-Criteria Decis. Anal. 2019, 26, 62–83. [Google Scholar] [CrossRef] [Green Version]
- Borroni, M.; Pozzi, C.M.; Daniotti, S.; Gatto, F.; Re, I. Multi-criteria decision-making approach for nutraceuticals greener applications: The Cynara cardunculus case study. Sustainability 2021, 13, 3483. [Google Scholar] [CrossRef]
- Gatto, F.; Re, I. Circular bioeconomy business models to overcome the valley of death. A systematic statistical analysis of studies and projects in emerging bio-based technologies and trends linked to the sme instrument support. Sustainability 2021, 13, 1–37. [Google Scholar] [CrossRef]
- Daniotti, S.; Re, I. Marine Biotechnology: Challenges and Development Market Trends for the Enhancement of Biotic Resources in Industrial Pharmaceutical and Food Applications. A Statistical Analysis of Scientific Literature and Business Models. Mar. Drugs 2021, 19, 61. [Google Scholar] [CrossRef]
- Department for Communities and Local Government of London. Multi-Criteria Analysis: A Manual; Communities and Local Government: New York, NY, USA, 2009; ISBN 978-1-4098-1023-0. [Google Scholar]
- Bigaret, S.; Hodgett, R.E.; Meyer, P.; Mironova, T.; Olteanu, A.L. Supporting the multi-criteria decision aiding process: R and the MCDA package. Euro J. Decis. Processes 2017, 5, 169–194. [Google Scholar] [CrossRef] [Green Version]
- Aragon, T.; Dalnoki-Veress, F.; Shiu, K. Deriving Criteria Weights for Health Decision Making: A Brief Tutorial. UC Berkeley Cent Infect. Dis. Emerg. Readiness 2017. Available online: https://escholarship.org/content/qt52755837/qt52755837.pdf?t=ox8spw (accessed on 6 June 2022).
- Preston, K.; Krumian, R.; Hattner, J.; de Montigny, D.; Stewart, M.; Gaddam, S. Lactobacillus acidophilus CL1285, Lactobacillus casei LBC80R and Lactobacillus rhamnosus CLR2 improve quality-of-life and IBS symptoms: A double-blind, randomised, placebo-controlled study. Benef. Microbes 2018, 9, 697–706. [Google Scholar] [CrossRef]
- Hod, K.; Sperber, A.D.; Ron, Y.; Boaz, M.; Dickman, R.; Berliner, S.; Halpern, Z.; Maharshak, N.; Dekel, R. A double-blind, placebo-controlled study to assess the effect of a probiotic mixture on symptoms and inflammatory markers in women with diarrhea-predominant IBS. Neurogastroenterol. Motil. Off. J. Eur. Gastrointest. Motil. Soc. 2017, 29, e13037. [Google Scholar] [CrossRef] [PubMed]
- Sisson, G.; Ayis, S.; Sherwood, R.A.; Bjarnason, I. Randomised clinical trial: A liquid multi-strain probiotic vs. placebo in the irritable bowel syndrome–A 12 week double-blind study. Aliment. Pharmacol. Ther. 2014, 40, 51–62. [Google Scholar] [CrossRef] [Green Version]
- Hod, K.; Dekel, R.; Aviv Cohen, N.; Sperber, A.; Ron, Y.; Boaz, M.; Berliner, S.; Maharshak, N. The effect of a multispecies probiotic on microbiota composition in a clinical trial of patients with diarrhea-predominant irritable bowel syndrome. Neurogastroenterol. Motil. Off. J. Eur. Gastrointest. Motil. Soc. 2018, 30, e13456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ship, N.; Mallais, C.; Carrière, S. 509 Burden of IBS-Diarrhea Symptoms Tracked With Daily Journals for 12 Weeks in a Randomized, Double-Blind, Placebo-Controlled Study of Lactobacillus AcidophilusCL1285, L. Casei LBC80R and L. Rhamnosus CLR2. Off. J. Am. Coll. Gastroenterol. ACG 2019, 114, S296. [Google Scholar] [CrossRef]
- Mezzasalma, V.; Manfrini, E.; Ferri, E.; Sandionigi, A.; La Ferla, B.; Schiano, I.; Michelotti, A.; Nobile, V.; Labra, M.; Di Gennaro, P. A Randomized, Double-Blind, Placebo-Controlled Trial: The Efficacy of Multispecies Probiotic Supplementation in Alleviating Symptoms of Irritable Bowel Syndrome Associated with Constipation. Biomed. Res. Int. 2016, 2016, 4740907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, J.S.; Sohn, W.; Lee, O.Y.; Lee, S.P.; Lee, K.N.; Jun, D.W.; Lee, H.L.; Yoon, B.C.; Choi, H.S.; Chung, W.-S.; et al. Effect of multispecies probiotics on irritable bowel syndrome: A randomized, double-blind, placebo-controlled trial. J. Gastroenterol. Hepatol. 2014, 29, 52–59. [Google Scholar] [CrossRef]
- Ki Cha, B.; Mun Jung, S.; Hwan Choi, C.; Song, I.-D.; Woong Lee, H.; Joon Kim, H.; Hyuk, J.; Kyung Chang, S.; Kim, K.; Chung, W.-S.; et al. The effect of a multispecies probiotic mixture on the symptoms and fecal microbiota in diarrhea-dominant irritable bowel syndrome: A randomized, double-blind, placebo-controlled trial. J. Clin. Gastroenterol. 2012, 46, 220–227. [Google Scholar] [CrossRef]
- Ludidi, S.; Jonkers, D.M.; Koning, C.J.; Kruimel, J.W.; Mulder, L.; van der Vaart, I.B.; Conchillo, J.M.; Masclee, A.A.M. Randomized clinical trial on the effect of a multispecies probiotic on visceroperception in hypersensitive IBS patients. Neurogastroenterol. Motil. Off. J. Eur. Gastrointest. Motil. Soc. 2014, 26, 705–714. [Google Scholar] [CrossRef] [Green Version]
- FDA Guidance for Industry: Irritable Bowel Syndrome-Clinical Evaluation of Drugs for Treatment; Docket No. FDA-2012-D-0146; 2012; pp. 32124–32125. Available online: https://www.federalregister.gov/documents/2012/05/31/2012-13143/guidance-for-industry-on-irritable-bowel-syndrome-clinical-evaluation-of-drugs-for-treatment (accessed on 6 June 2022).
- Delgado, D.A.; Lambert, B.S.; Boutris, N.; McCulloch, P.C.; Robbins, A.B.; Moreno, M.R.; Harris, J.D. Validation of Digital Visual Analog Scale Pain Scoring With a Traditional Paper-based Visual Analog Scale in Adults. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2018, 2, e088. [Google Scholar] [CrossRef]
- Castrogiovanni, P.; Goracci, A.; Martinucci, M.; Scalcione, U.; Bossini, L. Questionnaire for the Assessment of Quality of Life in Healthy Subjects (VQV-ss): Elaboration of a new instrument for the assessment of quality of life in the general population. J. Psychopathol. 2004, 4. Available online: https://www.jpsychopathol.it/article/questionario-per-la-valutazione-della-qualita-della-vita-nei-soggetti-sani-vqv-ss-elaborazione-di-un-nuovo-strumento-per-lassessment-della-qualita-della-vita-nella-popolazione-generale/ (accessed on 6 June 2022).
- Goepel, K.D. Implementing the Analytic Hierarchy Process as a Standard Method for Multi-Criteria Decision Making In Corporate Enterprises–A New AHP Excel Template with Multiple Inputs. In Proceedings of the International Symposium on the Analytic Hierarchy Process; Creative Decisions Foundation Kuala Lumpur: Kuala Lumpur, Malaysia, 2013. [Google Scholar] [CrossRef] [Green Version]
- Banna, G.L.; Torino, F.; Marletta, F.; Santagati, M.; Salemi, R.; Cannarozzo, E.; Falzone, L.; Ferraù, F.; Libra, M. Lactobacillus rhamnosus GG: An overview to explore the rationale of its use in cancer. Front. Pharmacol. 2017, 8, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Sapkota, A. Lactobacillus acidophilus-An Overview. 2021. Available online: https://microbenotes.com/lactobacillus-acidophilus/ (accessed on 16 February 2022).
- van Kessel, L.; Teunissen, D.; Lagro-Janssen, T. Sex-gender differences in the effectiveness of treatment of irritable bowel syndrome: A systematic review. Int. J. Gen. Med. 2021, 14, 867–884. [Google Scholar] [CrossRef]
- Kim, Y.S.; Kim, N. Sex-gender differences in irritable bowel syndrome. J. Neurogastroenterol. Motil. 2018, 24, 544–558. [Google Scholar] [CrossRef] [Green Version]
- Villani, A.; Lemire, M.; Fortin, G.; Louis, E.; Mark, S.; Collette, C.; Baba, N.; Libioulle, C.; Belaiche, J.; Bitton, A.; et al. The microgenderome revealed: Sex differences in bidirectional interactions between the microbiota, hormones, immunity and disease susceptibility. Semin. Immunopathol. 2018, 41, 265–275. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Query | Science Direct | PubMed | Cochrane |
|---|---|---|---|
| IBS clinical trials probiotics | 236 | 76 | 148 |
| Clinical trials probiotics IBS | 236 | 76 | 186 |
| IBS clinical trials prebiotics | 111 | 10 | 33 |
| Clinical trials prebiotics IBS | 111 | 10 | 41 |
| Prebiotics probiotics IBS clinical trials | 94 | 3 | 14 |
| Criterium | Criterium Title | Measurement | Score Type | Evaluation Type |
|---|---|---|---|---|
| C1 | Bloating | % Value of the improvement | VAS (0–10) | Maximization |
| C2 | Pain | % Value of the improvement | VAS (0–10) | Maximization |
| C3 | Cramps | % Value of the improvement | VAS (0–10) | Maximization |
| C4 | Flatulence | % Value of the improvement | VAS (0–10) | Maximization |
| C5 | Constipation | % Value of the improvement | VAS (0–10) | Maximization |
| C6 | Quality Life | % Value of the improvement | Q-score (100–300) | Maximization |
| C7 | Efficacy | Number of trials resulting not effective | Yes/No | Minimized |
| IBS Probiotic Combinations | Lactobacillus acidophilus | Lactobacillus rhamnosus | Bifidobacterium animalis subsp. lactis |
|---|---|---|---|
| Lactobacillus acidophilus | 11 | 7 | 5 |
| Lactobacillus rhamnosus | 7 | 9 | 6 |
| Bifidobacterium animalis subsp. lactis | 5 | 6 | 10 |
| Bloating | pain | Cramps | Flatulence | Constipation | Quality Life | Efficacy | |
|---|---|---|---|---|---|---|---|
| L. rhamnosus-L.acidophilus | 45 | 48 | 38 | 38 | 11 | 73 | 1 |
| L.rhamnosus-B.animalis subsp. lactis | 30 | 30 | 30 | 30 | 30 | 22 | 0 |
| Mix 3 species | 22 | 23 | 37 | 14 | 24 | 21 | 1 |
| Bloating | Pain | Cramps | Flatulence | Constipation | Quality Life | Efficacy | |
|---|---|---|---|---|---|---|---|
| L.rhamnosus-L.acidophilus | 1 | 1 | 1 | 1 | 0 | 1 | 0 |
| L.rhamnosus-B.animalis subsp. lactis | 0.34 | 0.28 | 0 | 0.67 | 1 | 0.02 | 1 |
| Mix 3 species | 0 | 0 | 0.86 | 0 | 0.68 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceccherini, C.; Daniotti, S.; Bearzi, C.; Re, I. Evaluating the Efficacy of Probiotics in IBS Treatment Using a Systematic Review of Clinical Trials and Multi-Criteria Decision Analysis. Nutrients 2022, 14, 2689. https://doi.org/10.3390/nu14132689
Ceccherini C, Daniotti S, Bearzi C, Re I. Evaluating the Efficacy of Probiotics in IBS Treatment Using a Systematic Review of Clinical Trials and Multi-Criteria Decision Analysis. Nutrients. 2022; 14(13):2689. https://doi.org/10.3390/nu14132689
Chicago/Turabian StyleCeccherini, Cecilia, Sara Daniotti, Claudia Bearzi, and Ilaria Re. 2022. "Evaluating the Efficacy of Probiotics in IBS Treatment Using a Systematic Review of Clinical Trials and Multi-Criteria Decision Analysis" Nutrients 14, no. 13: 2689. https://doi.org/10.3390/nu14132689
APA StyleCeccherini, C., Daniotti, S., Bearzi, C., & Re, I. (2022). Evaluating the Efficacy of Probiotics in IBS Treatment Using a Systematic Review of Clinical Trials and Multi-Criteria Decision Analysis. Nutrients, 14(13), 2689. https://doi.org/10.3390/nu14132689