
The Effect of a Product Placement Intervention on Pupil’s Food and Drink Purchases in Two Secondary Schools: An Exploratory Study


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Sample
2.2. Study Design
2.3. School Interventions
2.4. Data Collection
2.5. Ethics, Access to Data and Confidentiality
2.6. Main Outcome Measures
2.7. Data Manipulation and Statistical Analysis
3. Results
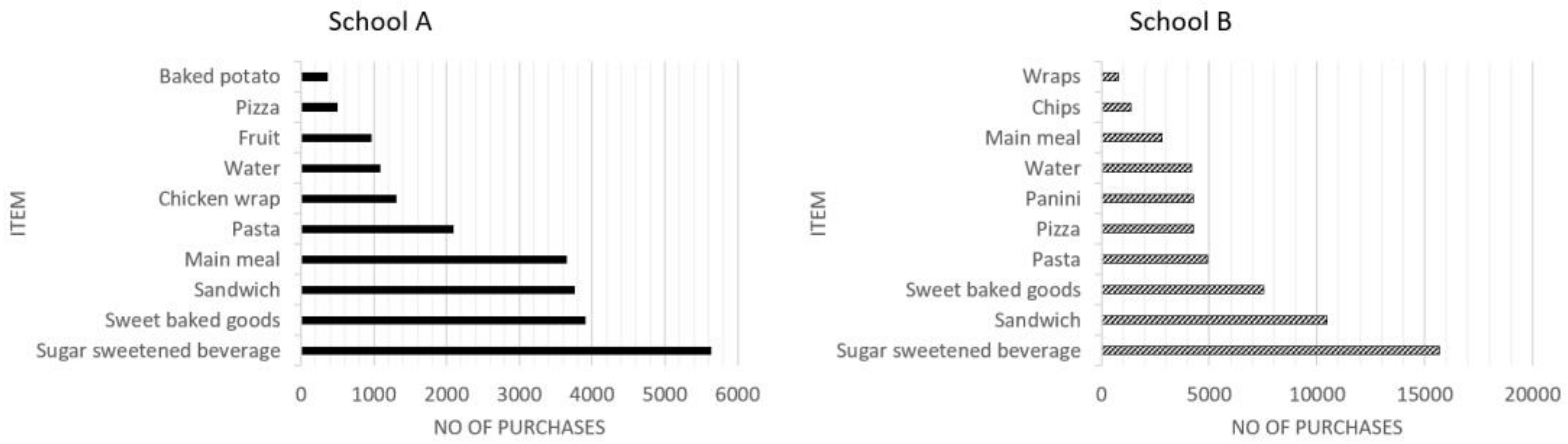
3.1. Total Sales of the Top Ten Pupil Purchases by School
3.2. Effect of the Intervention(s) on Pupil Purchasing by School
4. Discussion
4.1. Summary of Key Results
4.2. Relationship to Other Studies
4.3. Strengths and Limitations
4.4. Future Research and Implications for Policy and Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [Google Scholar] [CrossRef]
- Lascar, N.; Brown, J.; Pattison, H.; Barnett, A.H.; Bailey, C.J.; Bellary, S. Type 2 diabetes in adolescents and young adults. Lancet Diabetes Endocrinol 2018, 6, 69–80. [Google Scholar] [CrossRef] [Green Version]
- Holden, S.H.; Barnett, A.H.; Peters, J.R.; Jenkins-Jones, S.; Poole, C.D.; Morgan, C.L.; Currie, C.J. The incidence of type 2 diabetes in the United Kingdom from 1991 to 2010. Diabetes Obes. Metab. 2013, 15, 844–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Public Health England. NDNS: Results from Years 1 to 4 (combined): Results of the National Diet and Nutrition Survey (NDNS) Rolling Programme for 2008/2009 to 2011/2012. 2014. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/594361/NDNS_Y1_to_4_UK_report_full_text_revised_February_2017.pdf (accessed on 24 May 2022).
- Roberto, C.A.; Swinburn, B.; Hawkes, C.; Huang, T.T.-K.; Costa, S.A.; Ashe, M.; Zwicker, L.; Cawley, J.H.; Brownell, K.D. Patchy progress on obesity prevention: Emerging examples, entrenched barriers, and new thinking. Lancet 2015, 385, 2400–2409. [Google Scholar] [CrossRef]
- Nuffield Council on Bioethics. Public Health: Ethical Issues; Nuffield Council on Bioethics: London, UK, 2007. [Google Scholar]
- Brown, T.; Summerbell, C. Systematic review of school-based interventions that focus on changing dietary intake and physical activity levels to prevent childhood obesity: An update to the obesity guidance produced by the National Institute for Health and Clinical Excellence. Obes. Rev. 2019, 10, 110–141. [Google Scholar] [CrossRef] [Green Version]
- Hawkes, C.; Smith, T.G.; Jewell, J.; Wardle, J.; Hammond, R.A.; Friel, S.; Thow, A.M.; Kain, J. Smart food policies for obesity prevention. Lancet 2015, 385, 2410–2421. [Google Scholar] [CrossRef]
- Department for Education. Schools, Pupils and Their Characteristics: January 2016. 2016. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/552342/SFR20_2016_Main_Text.pdf (accessed on 4 February 2020).
- The Requirements for School Food Regulations 2014. Available online: http://www.legislation.gov.uk/uksi/2014/1603/pdfs/uksi_20141603_en.pdf (accessed on 25 July 2019).
- Spence, S.; Delve, J.; Stamp, E.; Matthews, J.N.S.; White, M.; Adamson, A.J. Did School Food and Nutrient-Based Standards in England Impact on 11–12Y Olds Nutrient Intake at Lunchtime and in Total Diet? Repeat Cross-Sectional Study. PLoS ONE 2014, 9, e112648. [Google Scholar] [CrossRef] [Green Version]
- Hollands, G.J.; Bignardi, G.; Johnston, M.; Kelly, M.P.; Ogilvie, D.; Petticrew, M.; Prestwich, A.; Shemilt, I.; Sutton, S.; Marteau, T.M. The TIPPME intervention typology for changing environments to change behaviour. Nat. Hum. Behav. 2017, 1, 1–9. [Google Scholar] [CrossRef]
- The Academy of Medical Sciences. Improving the Health of The Public by 2040: Optimising the Research Environment for a Healthier, Fairer Future. 2016. Available online: https://acmedsci.ac.uk/file-download/41399-5807581429f81.pdf (accessed on 24 May 2022).
- van Kleef, E.; Otten, K.; van Trijp, H.C.M. Healthy snacks at the checkout counter: A lab and field study on the impact of shelf arrangement and assortment structure on consumer choices. BMC Public Health 2012, 12, 1072. [Google Scholar] [CrossRef] [Green Version]
- Broers, V.J.V.; De Breucker, C.; Van den Broucke, S.; Luminet, O. A systematic review and meta-analysis of the effectiveness of nudging to increase fruit and vegetable choice. Eur. J. Public Health 2017, 27, 912–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vecchio, R.; Cavallo, C. Increasing healthy food choices through nudges: A systematic review. Food Qual. Prefer. 2019, 78, 103714. [Google Scholar] [CrossRef]
- Bucher, T.; Collins, C.; Rollo, M.E.; McCaffrey, T.; De Vlieger, N.; Van Der Bend, D.; Truby, H.; Perez-Cueto, F.J.A. Nudging consumers towards healthier choices: A systematic review of positional influences on food choice. Br. J. Nutr. 2016, 115, 2252–2263. [Google Scholar] [CrossRef] [PubMed]
- Ensaff, H.; Homer, M.; Sahota, P.; Braybrook, D.; Coan, S.; McLeod, H. Food Choice Architecture: An Intervention in a Secondary School and its Impact on Students’ Plant-based Food Choices. Nutrients 2015, 7, 4426. [Google Scholar] [CrossRef] [Green Version]
- Hanks, A.S.; Just, D.R.; Wansink, B. Smarter Lunchrooms Can Address New School Lunchroom Guidelines and Childhood Obesity. J. Pediatr. 2013, 162, 867–869. [Google Scholar] [CrossRef]
- Hanks, A.S.; Just, D.R.; Smith, L.E.; Wansink, B. Healthy convenience: Nudging students toward healthier choices in the lunchroom. J. Public Health 2012, 34, 370–376. [Google Scholar] [CrossRef] [Green Version]
- Quinn, E.L.; Johnson, D.B.; Podrabsky, M.; Saelens, B.E.; Bignell, W.; Krieger, J. Effects of a Behavioral Economics Intervention on Food Choice and Food Consumption in Middle-School and High-School Cafeterias. Prev. Chronic Dis. 2018, 15, E91. [Google Scholar] [CrossRef] [Green Version]
- Shepherd, R. Resistance to Changes in Diet. Proc. Nutr. Soc. 2002, 61, 267–272. [Google Scholar] [CrossRef]
- McSweeney, L.; Bradley, J.; Adamson, A.J.; Spence, S. The ‘Voice’ of Key Stakeholders in a School Food and Drink Intervention in Two Secondary Schools in NE England: Findings from a Feasibility Study. Nutrients 2019, 11, 2746. [Google Scholar] [CrossRef] [Green Version]
- Hussey, M.A.; Hughes, J.P. Design and analysis of stepped wedge cluster randomized trials. Contemp. Clin. Trials 2007, 28, 182–191. [Google Scholar] [CrossRef]
- Gustafson, A.; Hankins, S.; Jilcott, S. Measures of the consumer food store environment: A systematic review of the evidence 2000–2011. J. Community Health 2012, 37, 897–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvert, S.; Dempsey, R.C.; Povey, R. Delivering in-school interventions to improve dietary behaviours amongst 11- to 16-year-olds: A systematic review. Obes. Rev. 2019, 20, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Wills, W.; Backett-Milburn, K.; Gregory, S.; Lawton, J. The influence of the secondary school setting on the food practices of young teenagers from disadvantaged backgrounds in Scotland. Health Educ. Res. 2005, 20, 458–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Time Period | ||||
|---|---|---|---|---|
| School | T1 | T2 | T3 | T4 |
| School A | C * | I † | I | PI ‡ |
| School B | C | C | I | PI |
| T1 | |||
|---|---|---|---|
| T2 | No | Yes | |
| No | a * | b †,ǁ | |
| Yes | c ǂ,ǁ | d § | |
| School A (Total Number of Pupils n = 540) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 *&T2 † | T2&T3 ‡ | T3&T4 § | ||||||||||
| Item | D1 ǁ | D2 ¶ | OR (95% CI) | p-Value | D3 ** | D4 †† | OR (95% CI) | p-Value | D5 ‡‡ | D6 §§ | OR (95% CI) | p-Value |
| n | n | n | n | n | n | |||||||
| Water | 60 | 62 | 1.0 (0.7 to 1.4) | 0.9 | 66 | 76 | 0.9 (0.6 to 1.2) | 0.5 | 78 | 61 | 1.3 (0.9 to 1.8) | 0.2 |
| SSBs | 50 | 59 | 0.8 (0.6 to 1.3) | 0.4 | 61 | 73 | 0.8 (0.6 to 1.2) | 0.3 | 67 | 48 | 1.4 (0.9 to 2.1) | 0.09 |
| Zing | 85 | 9 | 9.4 (4.7 to 21.4) | <0.001 | 79 | 0 | 0 (21 to 0) | <0.001 | 0 | 0 | - | - |
| Yoghurt | 3 | 1 | 3 (0.2 to 157.5) | 0.6 | 1 | 1 | 1 (0.01 to 78.5) | 1.0 | 1 | 2 | 0.5 (0.0 to 9.6) | 1.0 |
| Sweet baked goods | 62 | 69 | 0.9 (0.6 to 1.3) | 0.5 | 71 | 68 | 1 (0.7 to 1.5) | 0.9 | 57 | 68 | 0.8 (0.6 to 1.2) | 0.4 |
| Fruit Pots | 0 | 81 | 0 (0 to 0.04) | <0.001 | 41 | 53 | 0.8 (0.5 to 1.2) | 0.3 | 81 | 6 | 13.5 (5.9 to 37.9) | <0.001 |
| Fruit | 48 | 26 | 1.8 (1.1 to 3.1) | 0.01 | 39 | 9 | 4.3 (2.1 to 10.2) | <0.001 | 12 | 47 | 0.3 (0.1 to 0.5) | <0.001 |
| School B (Total Number of Pupils n = 1194) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 *&T2 † | T2&T3 ‡ | T3&T4 § | ||||||||||
| Item | D1 ǁ | D2 ¶ | OR (95% CI) | p-Value | D3 ** | D4 †† | OR (95% CI) | p-Value | D5 ‡‡ | D6 §§ | OR (95% CI) | p-Value |
| n | n | n | n | n | n | |||||||
| Water | 130 | 146 | 0.9 (0.7 to 1.1) | 0.4 | 144 | 163 | 0.9 (0.7 to 1.1) | 0.3 | 193 | 98 | 2.0 (1.5 to 2.5) | <0.001 |
| SSBs | 123 | 150 | 0.8 (0.6 to 1.0) | 0.1 | 158 | 161 | 1.0 (0.8 to 1.2) | 0.9 | 180 | 79 | 2.3 (1.7 to 3.0) | <0.001 |
| Zing ¶¶ | - | - | - | - | - | - | - | - | - | - | - | - |
| Yoghurt | 2 | 8 | 0.3 (0.03 to 1.3) | 0.06 | 9 | 5 | 1.8 (0.5 to 6.8) | 0.3 | 5 | 4 | 1.3 (0.3 to 6.3) | 0.7 |
| Sweet baked goods | 175 | 131 | 1.3 (1.0 to 1.7) | 0.01 | 183 | 147 | 1.2 (1.0 to 1.6) | 0.05 | 161 | 122 | 1.3 (1.0 to 1.7) | 0.02 |
| Fruit Pots | 54 | 24 | 2.3 (1.4 to 3.8) | <0.001 | 30 | 34 | 0.9 (0.5 to 1.5) | 0.6 | 40 | 21 | 1.9 (1.1 to 3.4) | 0.01 |
| Fruit | 12 | 11 | 1.1 (0.4 to 2.7) | 0.8 | 12 | 22 | 0.5 (0.2 to 1.2) | 0.08 | 20 | 12 | 1.7 (0.8 to 3.7) | 0.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spence, S.; Matthews, J.N.S.; McSweeney, L.; Adamson, A.J.; Bradley, J. The Effect of a Product Placement Intervention on Pupil’s Food and Drink Purchases in Two Secondary Schools: An Exploratory Study. Nutrients 2022, 14, 2626. https://doi.org/10.3390/nu14132626
Spence S, Matthews JNS, McSweeney L, Adamson AJ, Bradley J. The Effect of a Product Placement Intervention on Pupil’s Food and Drink Purchases in Two Secondary Schools: An Exploratory Study. Nutrients. 2022; 14(13):2626. https://doi.org/10.3390/nu14132626
Chicago/Turabian StyleSpence, Suzanne, John N. S. Matthews, Lorraine McSweeney, Ashley J. Adamson, and Jennifer Bradley. 2022. "The Effect of a Product Placement Intervention on Pupil’s Food and Drink Purchases in Two Secondary Schools: An Exploratory Study" Nutrients 14, no. 13: 2626. https://doi.org/10.3390/nu14132626
APA StyleSpence, S., Matthews, J. N. S., McSweeney, L., Adamson, A. J., & Bradley, J. (2022). The Effect of a Product Placement Intervention on Pupil’s Food and Drink Purchases in Two Secondary Schools: An Exploratory Study. Nutrients, 14(13), 2626. https://doi.org/10.3390/nu14132626