
Impact of a Farm-to-School Nutrition and Gardening Intervention for Native American Families from the FRESH Study: A Randomized Wait-List Controlled Trial

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
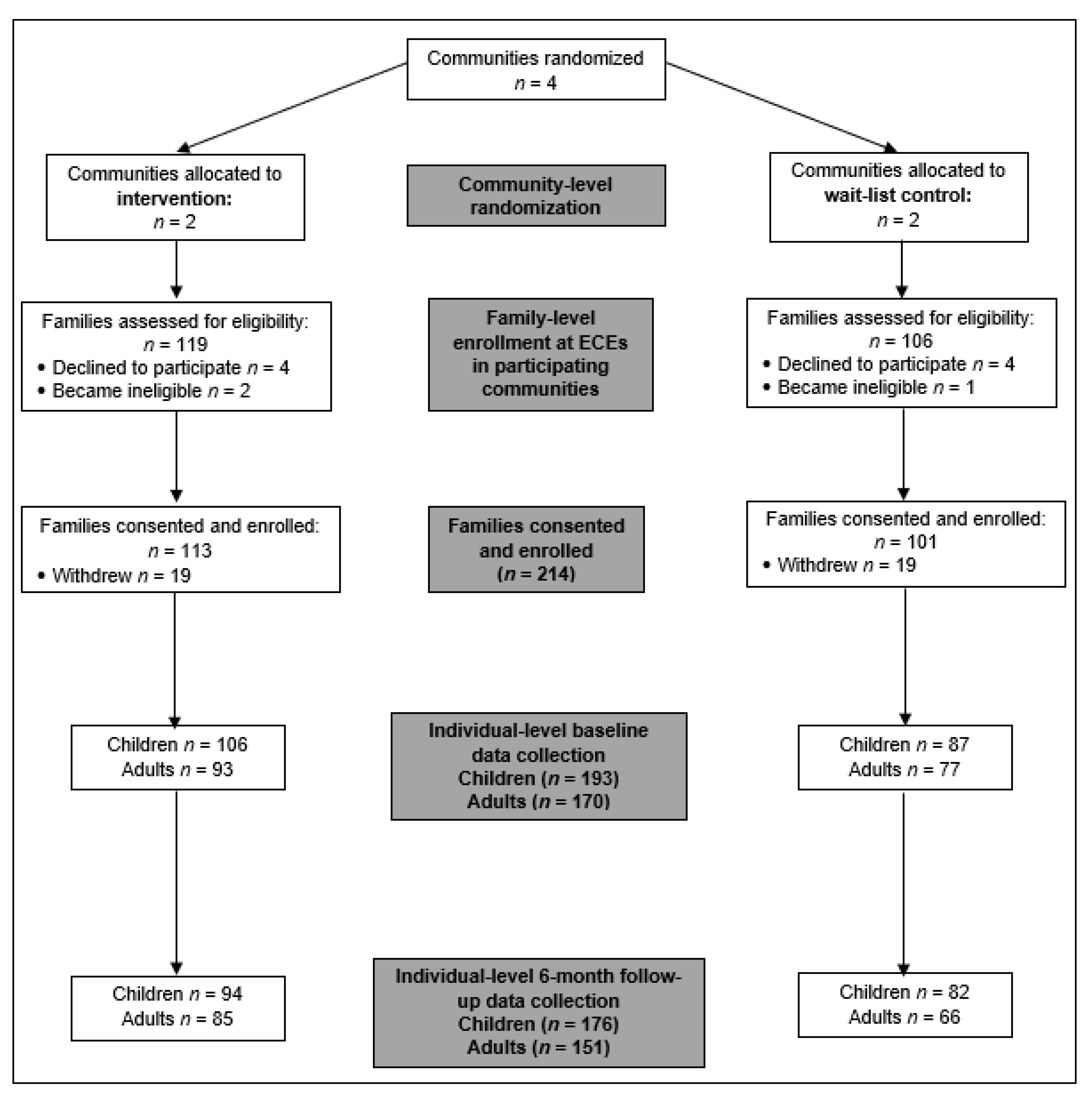
2.1. Trial Design
2.2. Participant Recruitment
2.3. FRESH Intervention Description
2.3.1. Farm-to-School Nutrition and Gardening Curriculum
2.3.2. Parent Curriculum
2.3.3. Menu Modifications
2.4. Trainings
2.5. Process Evaluations
2.6. Data Collection and Measures
2.6.1. Demographics
2.6.2. Dietary Intake
2.6.3. Biometrics and Health Status
2.6.4. Food Insecurity
2.7. Statistical Analyses
3. Results
3.1. Demographics
3.2. Child Outcomes
3.2.1. Dietary Intake
3.2.2. Health Outcomes
3.3. Adult Outcomes
3.3.1. Dietary Intake
3.3.2. Health Outcomes
3.3.3. Food Insecurity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jacobs-Wingo, J.L.; Espey, D.K.; Groom, A.V.; Phillips, L.E.; Haverkamp, D.S.; Sandte, L. Causes and disparities in death rates among urban American Indian and Alaska Native populations, 1999–2009. Am. J. Public Health 2016, 106, 906–914. [Google Scholar] [CrossRef]
- Blackwell, D.; Villarroal, M. Tables of Summary Health Statistics for U.S. Adults: 2016 National Health Interview Survey; National Center for Health Statistics: Hyattsville, MD, USA, 2018. [Google Scholar]
- Pan, L.; Freedman, D.S.; Park, S.; Galuska, D.A.; Potter, A.; Blanck, H.M. Changes in obesity among US children aged 2 through 4 years enrolled in WIC during 2010–2016. JAMA 2019, 321, 2364–2366. [Google Scholar] [CrossRef]
- Sanlier, N.; Ulusoy, H.G.; Kocabaş, S.; Çelik, B.; Göbel, P.; Yilmaz, S. Mediterranean Diet Adherence among Preschoolers and its Association with Parents’ Beliefs, Attitudes, and Practices. Ecol. Food Nutr. 2021, 60, 225–243. [Google Scholar] [CrossRef]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors influencing children’s eating behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef]
- Liu, J.; Rehm, C.D.; Onopa, J.; Mozaffarian, D. Trends in diet quality among youth in the United States, 1999–2016. JAMA 2020, 323, 1161–1174. [Google Scholar] [CrossRef]
- Watts, V.; Rockett, H.; Baer, H.; Leppert, J.; Colditz, G. Assessing diet quality in a population of low-income pregnant women: A comparison between Native Americans and whites. Matern. Child Health J. 2007, 11, 127–136. [Google Scholar] [CrossRef]
- Ferranti, E.P.; Hartman, T.J.; Elliott, A.J.; Mitchell, D.C.; Angal, J.; Nickleach, D.; Bellissimo, M.; Breslow, R. Peer Reviewed: Diet Quality of Pregnant American Indian Women in the Northern Plains. Prev. Chron. Dis. 2019, 16, E53. [Google Scholar]
- Byker Shanks, C.; Ahmed, S.; Dupuis, V.; Tryon, M.; Running Crane, M.; Houghtaling, B.; Garvin, T. Dietary quality varies among adults on the Flathead nation of the confederated Salish and Kootenai tribes in Montana. J. Community Health 2020, 45, 388–399. [Google Scholar] [CrossRef]
- Cullen, K.W.; Chen, T.-A. The contribution of the USDA school breakfast and lunch program meals to student daily dietary intake. Prev. Med. Rep. 2017, 5, 82–85. [Google Scholar] [CrossRef]
- Matwiejczyk, L.; Mehta, K.; Scott, J.; Tonkin, E.; Coveney, J. Characteristics of effective interventions promoting healthy eating for pre-schoolers in childcare settings: An umbrella review. Nutrients 2018, 10, 293. [Google Scholar] [CrossRef]
- Wetherill, M.S.; Bourque, E.E.; Taniguchi, T.; Love, C.V.; Sisk, M.; Jernigan, V.B.B. Development of a Tribally-led Gardening Curriculum for Indigenous Preschool Children: The FRESH Study. J. Nutr. Educ. Behav. 2021, 53, 991–995. [Google Scholar] [CrossRef] [PubMed]
- Natale, R.A.; Messiah, S.E.; Asfour, L.S.; Uhlhorn, S.B.; Englebert, N.E.; Arheart, K.L. Obesity prevention program in childcare centers: Two-year follow-up. Am. J. Health Promot. 2017, 31, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Jernigan, V.B.B.; Taniguchi, T.; Haslam, A.; Williams, M.B.; Maudrie, T.L.; Nikolaus, C.J.; Wetherill, M.S.; Jacob, T.; Love, C.V.; Sisson, S. Design and Methods of a Participatory Healthy Eating Intervention for Indigenous Children: The FRESH Study. Front. Public Health 2022, 10, 790008. [Google Scholar] [CrossRef] [PubMed]
- Langellotto, G.A.; Gupta, A. Gardening increases vegetable consumption in school-aged children: A meta-analytical synthesis. HortTechnology 2012, 22, 430–445. [Google Scholar] [CrossRef]
- Kos, M.; Jerman, J. Preschool children learning about the origin of food, on local farms and in the preschool garden. Nutr. Food Sci. 2012, 42, 324–331. [Google Scholar] [CrossRef]
- Savoie-Roskos, M.R.; Wengreen, H.; Durward, C. Increasing fruit and vegetable intake among children and youth through gardening-based interventions: A systematic review. J. Acad. Nutr. Diet. 2017, 117, 240–250. [Google Scholar] [CrossRef]
- Triador, L.; Farmer, A.; Maximova, K.; Willows, N.; Kootenay, J. A school gardening and healthy snack program increased Aboriginal First Nations children’s preferences toward vegetables and fruit. J. Nutr. Educ. Behav. 2015, 47, 176–180. [Google Scholar] [CrossRef]
- Wallerstein, N.B.; Duran, B. Using community-based participatory research to address health disparities. Health Promot. Pract. 2006, 7, 312–323. [Google Scholar] [CrossRef]
- Kalich, K.; Bauer, D.; McPartlin, D. Early Sprouts: Cultivating Healthy Food Choices in Young Children; Redleaf Press: St. Paul, MN, USA, 2009. [Google Scholar]
- Namenek Brouwer, R.J.; Benjamin Neelon, S.E. Watch Me Grow: A garden-based pilot intervention to increase vegetable and fruit intake in preschoolers. BMC Public Health 2013, 13, 363. [Google Scholar] [CrossRef]
- Los Angeles County Department of Public Health. Healthy Parenting Workshops. 2015. Available online: http://www.choosehealthla.com/wp-content/uploads/2016/09/PDF-6-Healthy-Parenting-Workshops-2nd-Edition-English-Toolkit.pdf (accessed on 15 January 2016).
- Bell-Sheeter, A. Institute of First Nations Development: Food Sovereignty Assessment Tool, 2nd ed.; First Nations Development Institute: Longmont, CO, USA, 2014. [Google Scholar]
- Grassroots International. Food for thought and Action 2008. Available online: https://grassrootsonline.org/what-we-do/publications-and-resources/educational-resources/food-thought-action/ (accessed on 1 May 2018).
- Haslam, A.; Love, C.; Taniguchi, T.; Williams, M.B.; Wetherill, M.S.; Sisson, S.; Weedn, A.E.; Jacob, T.; Jernigan, V.B.B. Development and Implementation of a Hybrid Online and In-Person Food Sovereignty and Nutrition Education Curriculum for Native American Parents: The FRESH Study. Health Educ. Behav. 2022. [Google Scholar] [CrossRef]
- Sisson, S.B.; Sleet, K.; Rickman, R.; Love, C.; Williams, M.; Jernigan, V.B.B. Impact of the 2017 Child and Adult Care Food Program Meal Pattern Requirement Change on Menu Quality in Tribal Early Care Environments: The Food Resource Equity and Sustainability for Health Study. Curr. Dev. Nutr. 2019, 4, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Sisson, S.B.; Sleet, K.; Rickman, R.; Love, C.; Williams, M.; Jernigan, V.B.B. The development of child and adult care food program best-practice menu and training for Native American Head Start programs: The FRESH study. Prev. Med. Rep. 2019, 14, 100880. [Google Scholar] [CrossRef] [PubMed]
- Sleet, K.; Sisson, S.B.; Dev, D.A.; Love, C.; Williams, M.B.; Hoffman, L.A.; Jernigan, V.B.B. The impact of responsive feeding practice training on teacher feeding behaviors in tribal early care and education: The food resource equity and sustainability for health (FRESH) study. Curr. Dev. Nutr. 2020, 4, 23–32. [Google Scholar] [CrossRef]
- Taniguchi, T.E.; Salvatore, A.L.; Williams, M.B.; Love, C.V.; Noonan, C.J.; Cannady, T.K.; Standridge, J.; Fox, J.; Spiegel, J.; Owens, J.; et al. Process Evaluation Tool Development and Fidelity of Healthy Retail Interventions in American Indian Tribally Owned Convenience Stores: The Tribal Health Resilience in Vulnerable Environments (THRIVE) Study. Curr. Dev. Nutr. 2020, 4, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Gittelsohn, J.; Suratkar, H.J.; Sacher, S.; Rajan, R.; Rasooly, I.R.; Bednarek, E.; Sharma, S.; Anliker, J.A.A. Process evaluation of Baltimore Healthy Stores: A pilot health intervention program with supermarkets and corner stores in Baltimore City. Health Promot. Pract. 2010, 11, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Bollella, M.; Boccia, L.; Nicklas, T.; Lefkowitz, K.; Pittman, B.; Zang, E.; Williams, C. Assessing dietary intake in preschool children: The healthy start project-New York. Nutr. Res. 1999, 19, 37–48. [Google Scholar] [CrossRef]
- Farfan-Ramirez, L.; Diemoz, L.; Gong, E.J.; Lagura, M.A. Curriculum intervention in preschool children: Nutrition Matters! J. Nutr. Educ. Behav. 2011, 43, S162–S165. [Google Scholar] [CrossRef]
- Wetherill, M.S.; Williams, M.B.; Reese, J.; Taniguchi, T.; Sisson, S.B.; Malek-Lasater, A.D.; Love, C.V.; Jernigan, V.B.B. Methods for Assessing Willingness to Try and Vegetable Consumption among Children in Indigenous Early Childcare Settings: The FRESH Study. Nutrients 2022, 14, 58. [Google Scholar] [CrossRef]
- Automated Self-Administered 24-Hour (ASA24) Dietary Assessment Tool Version 2016. Available online: https://asa24.nci.nih.gov/ (accessed on 15 February 2020).
- Murphy, S.P.; Kaiser, L.L.; Townsend, M.S.; Allen, L.H. Evaluation of validity of items for a food behavior checklist. J. Am. Diet. Assoc. 2001, 101, 751–761. [Google Scholar] [CrossRef]
- Townsend, M.S.; Kaiser, L.L.; Allen, L.H.; Joy, A.B.; Murphy, S.P. Selecting items for a food behavior checklist for a limited-resource audience. J. Nutr. Educ. Behav. 2003, 35, 69–82. [Google Scholar] [CrossRef]
- Poskitt, E. Defining childhood obesity: The relative body mass index (BMI). Acta Paediatr. 1995, 84, 961–963. [Google Scholar] [CrossRef] [PubMed]
- Agriculture UDo: US Adult Food Security Survey Module: Three-Stage Design, with Screeners; US Department of Agriculture, Economic Research Service: Washington, DC, USA, 2012.
- SAS Institute Inc. SAS 9.4 Statements: Reference; SAS Institute Inc.: Cary, NC, USA, 2013. [Google Scholar]
- Davis, J.N.; Pérez, A.; Asigbee, F.M.; Landry, M.J.; Vandyousefi, S.; Ghaddar, R.; Hoover, A.; Jeans, M.; Nikah, K.; Fischer, B. School-based gardening, cooking and nutrition intervention increased vegetable intake but did not reduce BMI: Texas sprouts-a cluster randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Bacardi-Gascon, M.; Perez-Morales, M.E.; Jimenez-Cruz, A. A six month randomized school intervention and an 18-month follow-up intervention to prevent childhood obesity in Mexican elementary schools. Nutr. Hosp. 2012, 27, 755–762. [Google Scholar] [PubMed]
- Epstein, L.H.; Gordy, C.C.; Raynor, H.A.; Beddome, M.; Kilanowski, C.K.; Paluch, R. Increasing fruit and vegetable intake and decreasing fat and sugar intake in families at risk for childhood obesity. Obes Res. 2001, 9, 171–178. [Google Scholar] [CrossRef]
- Hart, C.N.; Jelalian, E.; Raynor, H.A.; Mehlenbeck, R.; Lloyd-Richardson, E.E.; Kaplan, J.; Flynn-O’Brien, K.; Wing, R.R. Early patterns of food intake in an adolescent weight loss trial as predictors of BMI change. Eat Behav. 2010, 11, 217–222. [Google Scholar] [CrossRef][Green Version]
- Scherr, R.E.; Linnell, J.D.; Dharmar, M.; Beccarelli, L.M.; Bergman, J.J.; Briggs, M.; Brian, K.M.; Feenstra, G.; Hillhouse, J.C.; Keen, C.L.; et al. A Multicomponent, School-Based Intervention, the Shaping Healthy Choices Program, Improves Nutrition-Related Outcomes. J. Nutr. Educ. Behav. 2017, 49, 368–379. [Google Scholar] [CrossRef]
- Izumi, B.T.; Eckhardt, C.L.; Hallman, J.A.; Herro, K.; Barberis, D.A. Harvest for healthy kids pilot study: Associations between exposure to a farm-to-preschool intervention and willingness to try and liking of target fruits and vegetables among low-income children in head start. J. Acad. Nutr. Diet. 2015, 115, 2003–2201. [Google Scholar] [CrossRef]
- Buller, D.B.; Woodall, W.G.; Zimmerman, D.E.; Slater, M.D.; Heimendinger, J.; Waters, E.; Hines, J.M.; Starling, R.; Hau, B.; Burris-Woodall, P.; et al. Randomized Trial on the 5 a Day, the Rio Grande Way Website, A Web-based Program to Improve Fruit and Vegetable Consumption in Rural Communities. J. Health Commun. 2008, 13, 230–249. [Google Scholar] [CrossRef]
- Caton, S.J.; Ahern, S.M.; Remy, E.; Nicklaus, S.; Blundell, P.; Hetherington, M.M. Repetition counts: Repeated exposure increases intake of a novel vegetable in UK pre-school children compared to flavour-flavour and flavour-nutrient learning. Br. J. Nutr. 2013, 109, 2089–2097. [Google Scholar] [CrossRef]
- Anzman-Frasca, S.; Savage, J.S.; Marini, M.E.; Fisher, J.O.; Birch, L.L. Repeated exposure and associative conditioning promote preschool children’s liking of vegetables. Appetite 2012, 58, 543–553. [Google Scholar] [CrossRef]
- Remy, E.; Issanchou, S.; Chabanet, C.; Nicklaus, S. Repeated Exposure of Infants at Complementary Feeding to a Vegetable Purée Increases Acceptance as Effectively as Flavor-Flavor Learning and More Effectively Than Flavor-Nutrient Learning. J. Nutr. 2013, 143, 1194–1200. [Google Scholar] [CrossRef] [PubMed]
- de Wild, V.W.; de Graaf, C.; Jager, G. Effectiveness of flavour nutrient learning and mere exposure as mechanisms to increase toddler’s intake and preference for green vegetables. Appetite 2013, 64, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Fildes, A.; van Jaarsveld, C.H.M.; Wardle, J.; Cooke, L. Parent-Administered Exposure to Increase Children’s Vegetable Acceptance: A Randomized Controlled Trial. J. Acad. Nutr. Diet. 2014, 114, 881–888. [Google Scholar] [CrossRef] [PubMed]
- Hausner, H.; Olsen, A.; Møller, P. Mere exposure and flavour–flavour learning increase 2–3 year-old children’s acceptance of a novel vegetable. Appetite 2012, 58, 1152–1159. [Google Scholar] [CrossRef] [PubMed]
- Lakkakula, A.; Geaghan, J.; Zanovec, M.; Pierce, S.; Tuuri, G. Repeated taste exposure increases liking for vegetables by low-income elementary school children. Appetite 2010, 55, 226–231. [Google Scholar] [CrossRef]
- Maier, A.; Chabanet, C.; Schaal, B.; Issanchou, S.; Leathwood, P. Effects of repeated exposure on acceptance of initially disliked vegetables in 7-month old infants. Food Qual. Prefer. 2007, 18, 1023–1032. [Google Scholar] [CrossRef]
- Wardle, J.; Cooke, L.J.; Gibson, E.L.; Sapochnik, M.; Sheiham, A.; Lawson, M. Increasing children’s acceptance of vegetables; a randomized trial of parent-led exposure. Appetite 2003, 40, 155–162. [Google Scholar] [CrossRef]
- Sinley, R.C.; Albrecht, J.A. Application of the IMB Model to the reported intake of fruits and vegetables of Native American Children. J. Health Disparities Res. Pract. 2018, 11, 2. [Google Scholar]


{kind=link}
| Child Demographics | ||||
|---|---|---|---|---|
| Overall n = 193 | Intervention n = 106 | Control n = 87 | p-Value 3 | |
| Age, n (%) | 0.001 | |||
| 3 | 42 (21.8) | 18 (17.0) | 24 (27.6) | |
| 4 | 97 (50.3) | 54 (50.9) | 43 (49.4) | |
| 5 | 41 (21.2) | 21 (19.8) | 20 (23.0) | |
| 6 or older | 13 (6.7) | 13 (12.3) | 0 (0.0) | |
| Gender, n (%) | 0.38 | |||
| Male | 87 (45.1) | 51 (48.1) | 36 (41.4) | |
| Female | 106 (54.9) | 55 (51.9) | 51 (58.6) | |
| Race/ethnicity 1, n (%) | ||||
| Native American or Alaska Native | 140 (72.5) | 85 (80.2) | 55 (63.2) | 0.01 |
| White/Caucasian | 81 (42.0) | 29 (27.4) | 52 (59.8) | <0.001 |
| Asian or Pacific Islander | 3 (1.6) | 2 (1.9) | 1 (1.1) | 1.0 |
| Black or African American | 6 (3.1) | 2 (1.9) | 4 (4.6) | 0.41 |
| Hispanic/Latino | 14 (7.3) | 9 (8.5) | 5 (5.7) | 0.58 |
| Adult Demographics | ||||
| Overall n = 170 | Intervention n = 93 | Control n = 77 | p-Value 4 | |
| Age, mean (SD) | 33.2 (7.1) | 34.0 (7.3) | 32.2 (6.8) | 0.11 |
| Gender, n (%) | 0.64 | |||
| Male | 14 (8.2) | 9 (9.7) | 5 (6.5) | |
| Female | 156 (91.8) | 84 (90.3) | 72 (93.5) | |
| Race/ethnicity 1, n (%) | ||||
| Native American or Alaska Native | 96 (56.5) | 62 (66.7) | 34 (44.2) | 0.005 |
| White/Caucasian | 88 (51.8) | 36 (38.7) | 52 (67.5) | <0.001 |
| Asian or Pacific Islander | 2 (1.2) | 1 (1.1) | 1 (1.3) | 1.00 |
| Black or African American | 3 (1.8) | 1 (1.1) | 2 (2.6) | 0.87 |
| Hispanic/Latino | 6 (3.5) | 3 (3.2) | 3 (3.9) | 1.00 |
| Married or living with partner, n (%) | 118 (69.4) | 65 (69.9) | 53 (68.8) | 1.00 |
| Receive public assistance 2, n (%) | 60 (35.3) | 27 (29.0) | 33 (42.9) | 0.09 |
| Children < 18 years living in household, n (%) | 2.8 (1.4) | 2.8 (1.4) | 2.7 (1.4) | 0.65 |
| Annual household income, n (%) | <0.001 | |||
| Less than $20,000 | 50 (29.8) | 24 (25.8) | 26 (34.7) | |
| $20,000–$50,000 | 71 (42.3) | 31 (33.3) | 40 (53.3) | |
| More than $50,000 | 47 (28.0) | 38 (40.9) | 9 (12.0) | |
| Education, n (%) | 0.02 | |||
| High school degree or less/GED | 77 (45.3) | 37 (39.8) | 40 (51.9) | |
| Some college or technical school | 52 (30.6) | 26 (28.0) | 26 (33.8) | |
| College degree or higher | 41 (24.1) | 30 (32.3) | 11 (14.3) | |
| Work full-time, n (%) | 90 (56.2) | 60 (64.6) | 37 (48.2) | 0.04 |
| Relationship to child participant, n (%) | 0.25 | |||
| Parent or step-parent | 157 (92.4) | 83 (88.3) | 75 (94.9) | |
| Grandparent | 10 (5.9) | 8 (8.5) | 3 (3.8) | |
| Aunt or Uncle | 1 (0.6) | 0 (0.0) | 1 (1.3) | |
| Other | 2 (1.2) | 2 (2.1) | 0 (0.0) | |
| Variable | Intervention n = 94 | Control n = 82 | p-Value 2 | ||
|---|---|---|---|---|---|
| Baseline | Follow-Up | Baseline | Follow-Up | ||
| Dietary Intake | |||||
| Plate Waste, mean ± SD | |||||
| Tomatoes | 5.6 ± 8.4 | 6.7 ± 8.9 | 4.4 ± 7.5 | 5.4 ± 9.6 | 0.94 |
| Carrots | 13.4 ± 12.8 | 11.5 ± 11.8 | 11.5 ± 12.8 | 10.2 ± 12.0 | 0.76 |
| Spinach | 1.4 ±1.8 | 1.9 ± 2.4 | 1.4 ± 2.0 | 1.9 ± 2.6 | 0.91 |
| Squash | −0.09 ± 3.2 | 1.3 ± 4.8 | 0.3 ± 3.8 | −0.8 ± 2.4 | 0.0007 |
| Beans | 1.4 ± 2.7 | 3.2 ± 5.3 | 1.2 ± 3.2 | 0.7 ± 2.0 | 0.0002 |
| Peppers | 2.4 ± 5.0 | 4.9 ± 8.0 | 1.3 ± 3.8 | 2.6 ± 6.9 | 0.28 |
| Willingness to Try | |||||
| Tomatoes | 2.7 ± 1.8 | 2.8 ± 1.9 | 2.1 ± 1.7 | 2.3 ± 1.8 | 0.01 |
| Carrots | 4.0 ± 1.6 | 4.0 ± 1.6 | 3.7 ± 1.8 | 3.7 ± 1.8 | 0.50 |
| Spinach | 3.3 ± 1.9 | 3.4 ± 1.9 | 2.3 ± 1.8 | 3.1 ± 2.0 | 0.94 |
| Squash | 2.0 ± 1.6 | 2.0 ± 1.5 | 1.9 ± 1.4 | 1.9 ± 1.4 | 0.94 |
| Beans | 2.4 ± 1.8 | 2.7 ± 1.9 | 2.0 ± 1.5 | 1.9 ± 1.5 | 0.049 |
| Peppers | 2.5 ± 1.8 | 3.1 ± 1.8 | 2.0 ± 1.4 | 2.3 ± 1.8 | 0.91 |
| Health Outcomes | |||||
| BMI (kg/m2), n (%) | 0.31 3 | ||||
| Underweight | 1 (1.1) | 0 (0.0) | 0 (0.0) | 2 (2.6) | |
| Healthy weight | 63 (67.0) | 55 (61.8) | 51 (65.4) | 44 (56.4) | |
| Overweight | 18 (19.1) | 20 (22.5) | 10 (12.8) | 13 (16.7) | |
| Obese | 12 (12.8) | 14 (15.7) | 17 (21.8) | 19 (24.4) | |
| Health status 1, n (%) | 0.35 3 | ||||
| Excellent | 35 (39.8) | 39 (47.0) | 36 (49.3) | 40 (56.3) | |
| Very good | 38 (43.2) | 33 (39.8) | 31 (42.5) | 24 (33.8) | |
| Good | 13 (14.8) | 10 (12.0) | 5 (6.8) | 6 (8.5) | |
| Fair | 2 (2.3) | 1 (1.2) | 1 (1.4) | 1 (1.4) | |
| Poor | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Variable | Intervention n = 93 | Control n = 77 | p-Value 1 | ||
|---|---|---|---|---|---|
| Baseline | Follow-Up | Baseline | Follow-Up | ||
| Dietary Intake | |||||
| F/V Behavior Checklist, mean ± SD (n = 152) | |||||
| Fruit and vegetable intake (cups per day) | 2.2 ± 0.99 | 2.6 ± 1.10 | 2.3 ± 1.12 | 2.3 ± 1.11 | 0.07 |
| Dietary recall, mean ± SD (n = 167) | |||||
| Total energy (kcal) | 1699.9 ± 764.3 | 1480.1 ± 708.7 3 | 1839.4 ± 767.2 | 1676.9 ± 732.1 | 0.14 |
| Total fat (g) | 68.5 ± 35.4 | 61.2 ± 37.3 | 68.5 ± 37.9 | 66.2 ± 31.6 | 0.38 |
| Total added sugar (g) | 17.5 ± 16.8 | 13.5 ± 13.4 3 | 25.0 ± 20.0 | 15.5 ± 14.2 3 | 0.79 |
| Total fruits (cup eq.) | 0.5 ± 1.0 | 0.4 ± 0.6 | 0.4 ± 0.8 | 0.5 ± 0.8 | 0.14 |
| Total vegetables (cup eq.) | 1.3 ± 1.0 | 1.3 ± 1.2 | 1.2 ± 1.0 | 1.3 ± 0.9 | 0.88 |
| Health Outcomes | |||||
| BMI (kg/m2), n (%) | 0.90 | ||||
| Underweight | 1 (1.1) | 1 (1.3) | 0 (0.0) | 0 (0.0) | |
| Healthy weight | 20 (21.7) | 18 (24.3) | 20 (23.5) | 16 (24.6) | |
| Overweight | 21 (22.8) | 17 (23.0) | 20 (23.5) | 14 (21.5) | |
| Obese | 50 (54.4) | 38 (51.4) | 45 (53.0) | 35 (53.8) | |
| Systolic blood pressure, mean ± SD (n = 152) | 126.5 ± 16.6 | 123.6 ± 18.6 | 120.7 ± 14.4 | 122.3 ± 14.6 | 0.14 |
| Health status, n (%) | 0.69 | ||||
| Excellent | 4 (4.5) | 3 (3.6) | 5 (6.8) | 6 (8.5) | |
| Very good | 30 (34.1) | 24 (28.9) | 24 (32.9) | 21 (29.6) | |
| Good | 40 (45.5) | 43 (51.8) | 32 (43.8) | 31 (43.7) | |
| Fair | 12 (13.6) | 11 (13.3) | 11 (15.1) | 10 (14.1) | |
| Poor | 2 (2.3) | 2 (2.3) | 1 (1.4) | 1 (1.4) | |
| Food Insecurity | |||||
| Household food security, n (%) | 0.63 2 | ||||
| High | 46 (49.5) | 54 (58.1) | 36 (46.8) | 48 (62.3) | |
| Marginal | 19 (20.4) | 21 (22.6) | 12 (15.6) | 12 (15.6) | |
| Low | 23 (24.7) | 17 (18.3) | 27 (35.1) | 18 (23.4) | |
| Very low | 6 (6.5) | 2 (2.2) | 5 (6.5) | 2 (2.6) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taniguchi, T.; Haslam, A.; Sun, W.; Sisk, M.; Hayman, J.; Jernigan, V.B.B. Impact of a Farm-to-School Nutrition and Gardening Intervention for Native American Families from the FRESH Study: A Randomized Wait-List Controlled Trial. Nutrients 2022, 14, 2601. https://doi.org/10.3390/nu14132601
Taniguchi T, Haslam A, Sun W, Sisk M, Hayman J, Jernigan VBB. Impact of a Farm-to-School Nutrition and Gardening Intervention for Native American Families from the FRESH Study: A Randomized Wait-List Controlled Trial. Nutrients. 2022; 14(13):2601. https://doi.org/10.3390/nu14132601
Chicago/Turabian StyleTaniguchi, Tori, Alyson Haslam, Wenjie Sun, Margaret Sisk, Jann Hayman, and Valarie Blue Bird Jernigan. 2022. "Impact of a Farm-to-School Nutrition and Gardening Intervention for Native American Families from the FRESH Study: A Randomized Wait-List Controlled Trial" Nutrients 14, no. 13: 2601. https://doi.org/10.3390/nu14132601
APA StyleTaniguchi, T., Haslam, A., Sun, W., Sisk, M., Hayman, J., & Jernigan, V. B. B. (2022). Impact of a Farm-to-School Nutrition and Gardening Intervention for Native American Families from the FRESH Study: A Randomized Wait-List Controlled Trial. Nutrients, 14(13), 2601. https://doi.org/10.3390/nu14132601