
Vitamin D and Risk of Obesity-Related Cancers: Results from the SUN (‘Seguimiento Universidad de Navarra’) Project

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
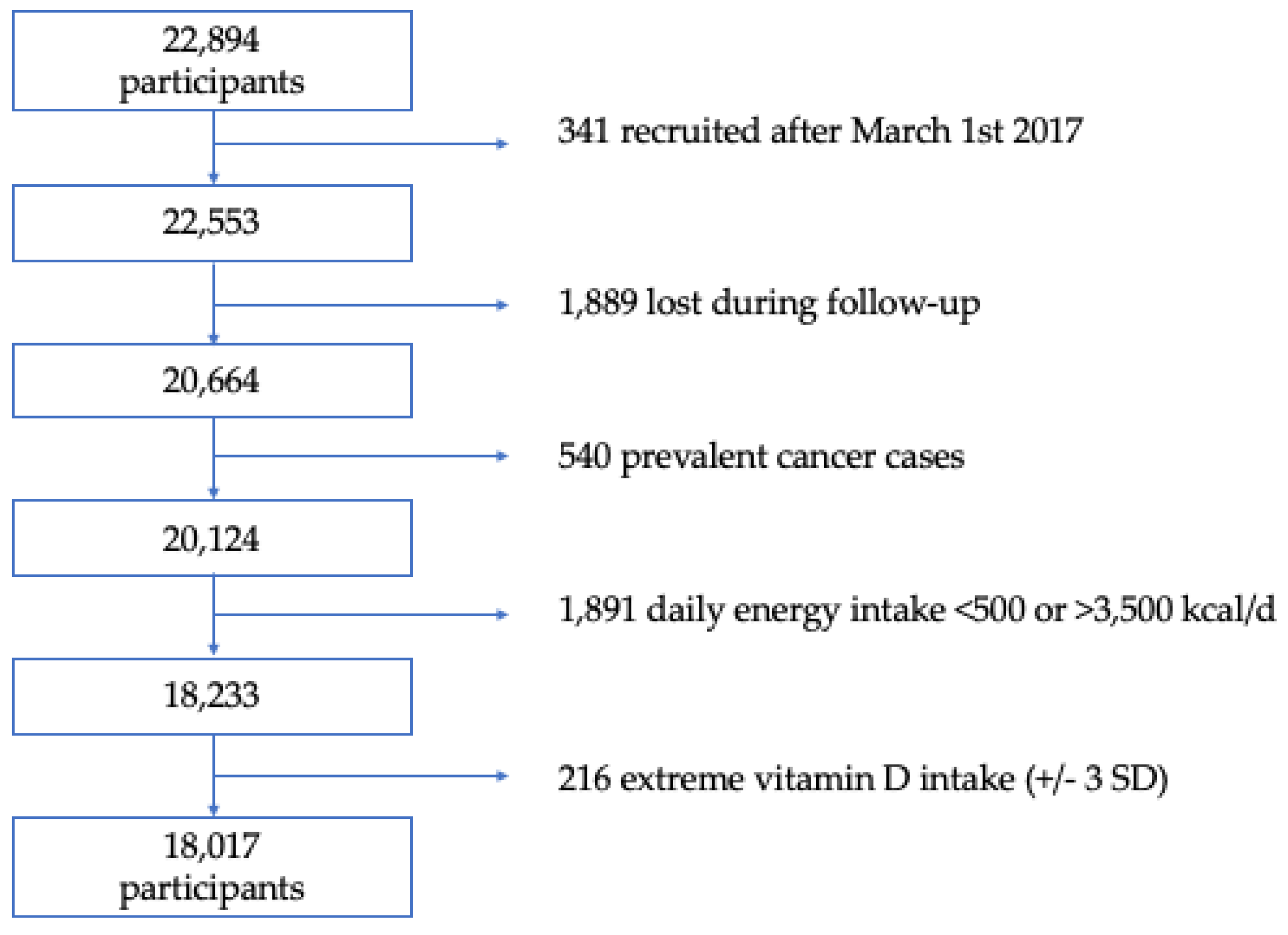
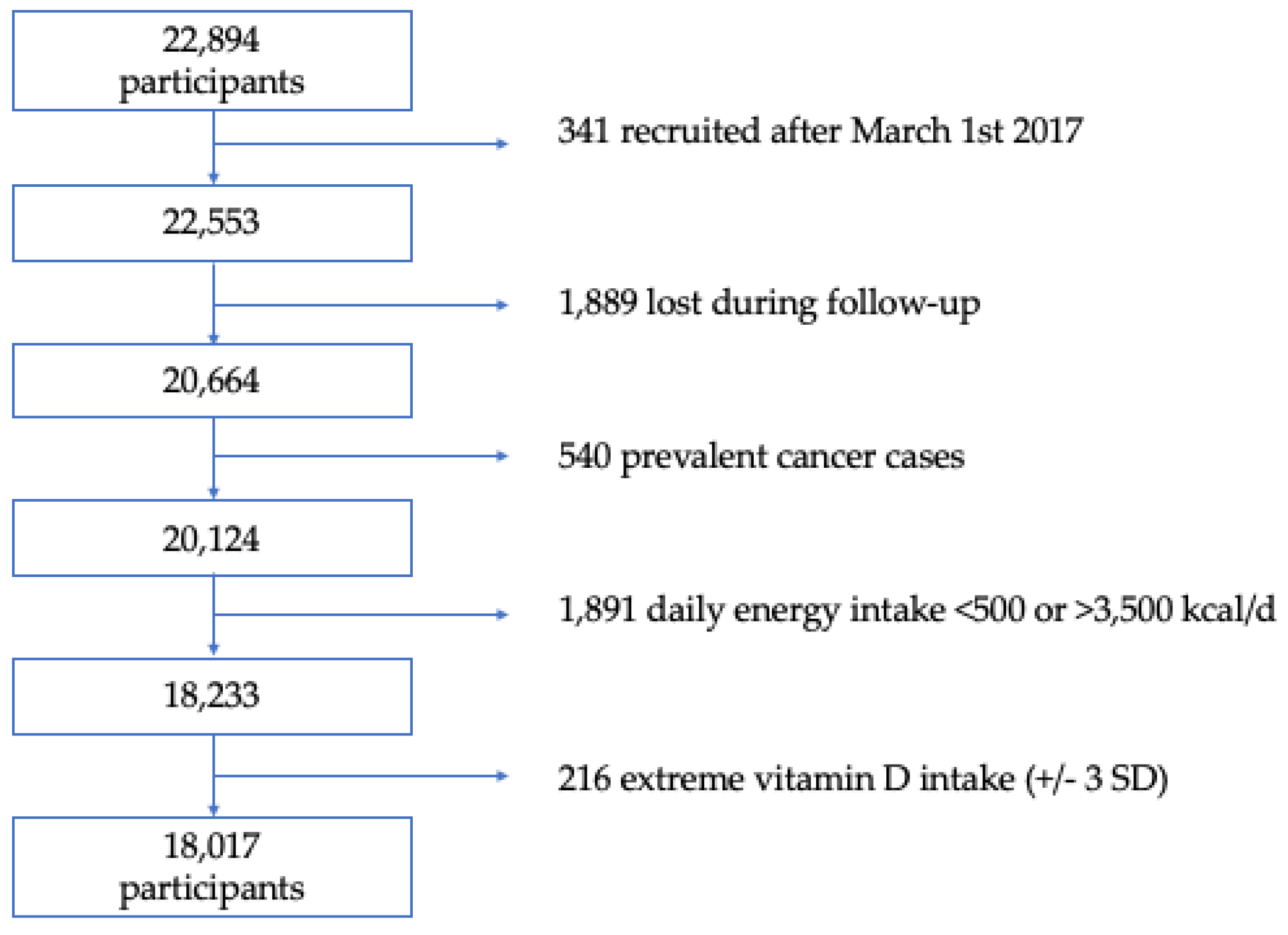
2.1. Study Population
2.2. Assessment of Vitamin D Intake
2.3. Ascertainment of Obesity-Related Cancer Cases
2.4. Covariate Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017, 16, 2627–2642. [Google Scholar]
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Vekic, J.; Zeljkovic, A.; Stefanovic, A.; Jelic-Ivanovic, Z.; Spasojevic-Kalimanovska, V. Obesity and dyslipidemia. Metabolism 2019, 92, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Polyzos, S.A.; Kountouras, J.; Mantzoros, C.S. Obesity and nonalcoholic fatty liver disease: From pathophysiology to therapeutics. Metabolism 2019, 92, 82–97. [Google Scholar] [CrossRef]
- Piché, M.E.; Tchernof, A.; Després, J.P. Obesity Phenotypes, Diabetes, and Cardiovascular Diseases. Circ. Res. 2020, 126, 1477–1500. [Google Scholar] [CrossRef] [PubMed]
- Seravalle, G.; Grassi, G. Obesity and hypertension. Pharmacol Res. 2017, 122, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Avgerinos, K.I.; Spyrou, N.; Mantzoros, C.S.; Dalamaga, M. Obesity and cancer risk: Emerging biological mechanisms and perspectives. Metabolism 2019, 92, 121–135. [Google Scholar] [CrossRef]
- Global Burden of Disease 2019 Cancer Collaboration. Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2022, 8, 420–444. [Google Scholar] [CrossRef]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K.; International Agency for Research on Cancer Handbook Working Group. Body Fatness and Cancer—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, B.D.; Goncalves, M.D.; Cantley, L.C. Obesity and Cancer Mechanisms: Cancer Metabolism. J. Clin. Oncol. 2016, 34, 4277–4283. [Google Scholar] [CrossRef] [Green Version]
- Zhang, A.M.Y.; Wellberg, E.A.; Kopp, J.L.; Johnson, J.D. Hyperinsulinemia in Obesity, Inflammation, and Cancer. Diabetes Metab. J. 2021, 45, 285–311. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. Office of Dietary Supplements. Vitamin D Fact Sheet for Consumers. Available online: https://ods.od.nih.gov/factsheets/VitaminD-Consumer/ (accessed on 12 June 2022).
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.S.; Bowles, S.; Evans, A.L. Vitamin D in obesity. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Oussaada, S.M.; van Galen, K.A.; Cooiman, M.I.; Kleinendorst, L.; Hazebroek, E.J.; van Haelst, M.M.; Ter Horst, K.W.; Serlie, M.J. The pathogenesis of obesity. Metabolism 2019, 92, 26–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estébanez, N.; Gómez-Acebo, I.; Palazuelos, C.; Llorca, J.; Dierssen-Sotos, T. Vitamin D exposure and Risk of Breast Cancer: A meta-analysis. Sci. Rep. 2018, 8, 9039. [Google Scholar] [CrossRef]
- Zhou, J.; Ge, X.; Fan, X.; Wang, J.; Miao, L.; Hang, D. Associations of vitamin D status with colorectal cancer risk and survival. Int. J. Cancer 2021, 149, 606–614. [Google Scholar] [CrossRef]
- Carlos, S.; De La Fuente-Arrillaga, C.; Bes-Rastrollo, M.; Razquin, C.; Rico-Campá, A.; Martínez-González, M.A.; Ruiz-Canela, M. Mediterranean Diet and Health Outcomes in the SUN Cohort. Nutrients 2018, 10, 439. [Google Scholar] [CrossRef] [Green Version]
- Willett, W.C. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- De la Fuente-Arrillaga, C.; Vázquez Ruiz, Z.; Bes-Rastrollo, M.; Sampson, L.; Martinez-González, M. Reproducibility of an FFQ validated in Spain. Public Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos (Food Composition Tables), 15th ed.; Pirámide: Madrid, Spain, 2011. [Google Scholar]
- Mataix-Verdú, J.; García-Diz, L.; Mañas, M.; Martínez-Victoria, E.; Llopis González, J. Tabla de Composición de Alimentos (Spanish Food Composition Tables), 4th ed.; Universidad de Granada Press: Granada, Spain, 2003. [Google Scholar]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.Á.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [Green Version]
- Bes-Rastrollo, M.; Valdivieso, J.R.P.; Sánchez-Villegas, A.; Alonso, Á.; Martínez-González, M.Á. Validación del peso e índice de masa corporal autodeclarados de los participantes de una cohorte de graduados universitarios (validation of self-reported weight and body mass index among participants of a cohort of university graduates). Rev. Esp. Obes. 2005, 3, 352–358. [Google Scholar]
- Martínez-González, M.A.; López-Fontana, C.; Varo, J.J.; Sánchez-Villegas, A.; Martinez, J.A. Validation of the Spanish version of the physical activity questionnaire used in the nurses’ health study and the health professionals’ follow-up study. Public Health Nutr. 2005, 8, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean dieat and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Bayona, R.; Gea, A.; Gardeazabal, I.; Romanos-Nanclares, A.; Martínez-González, M.A.; Bes-Rastrollo, M.; Santisteban, M.; Toledo, E. Binge drinking and risk of breast cancer: Results from the SUN (‘Seguimiento Universidad de Navarra’) Project. Nutrients 2020, 12, 731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scoccianti, C.; Cecchini, M.; Anderson, A.S.; Berrino, F.; Boutron-Ruault, M.C.; Espina, C.; Key, T.J.; Leitzmann, M.; Norath, T.; Powersi, H.; et al. European Code against Cancer 4th Edition: Alcohol drinking and cancer. Cancer Epidemiol. 2016, 45, 181–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Bank Group. Global Solar Atlas. Global horizontal irradiance (GHI) in Spain 1994–2015. 2020. Available online: https://globalsolaratlas.info (accessed on 1 February 2020).
- Gardeazabal, I.; Romanos-Nanclares, A.; Martínez-González, M.Á.; Sánchez-Bayona, R.; Vitelli-Storelli, F.; Gaforio, J.J.; Aramendía-Beitia, J.M.; Toledo, E. Total polyphenol intake and breast cancer risk in the Seguimiento Universidad de Navarra (SUN) cohort. Br. J. Nutr. 2019, 122, 542–551. [Google Scholar] [CrossRef]
- Romanos-Nanclares, A.; Sánchez-Quesada, C.; Gardeazábal, I.; Martínez-González, M.Á.; Gea, A.; Toledo, E. Phenolic acid subclasses, individual compounds, and breast cancer risk in a Mediterranean cohort: The SUN project. J. Acad. Nutr. Diet 2020, 120, 1002–1015.e5. [Google Scholar] [CrossRef]
- Sánchez-Quesada, C.; Romanos-Nanclares, A.; Navarro, A.M.; Gea, A.; Cervantes, S.; Martínez-González, M.; Toledo, E. Coffee consumption and breast cancer risk in the SUN project. Eur. J. Nutr. 2020, 59, 3461–3471. [Google Scholar] [CrossRef]
- Romanos-Nanclares, A.; Toledo, E.; Gardeazabal, I.; Jiménez-Moleón, J.J.; Martínez-González, M.A.; Gea, A. Sugar-sweetened beverage consumption and incidence of breast cancer: The Seguimiento Universidad de Navarra (SUN) project. Eur. J. Nutr. 2019, 58, 2875–2886. [Google Scholar] [CrossRef]
- Romanos-Nanclares, A.; Gea, A.; Martínez-González, M.Á; Zazpe, I.; Gardeazabal, I.; Fernández-Lazaro, C.I.; Toledo, E. Carbohydrate quality index and breast cancer risk in a Mediterranean cohort: The SUN project. Clin. Nutr. 2020, 40, 137–145. [Google Scholar] [CrossRef]
- Sánchez-Bayona, R.; Gardeazabal, I.; Romanos-Nanclares, A.; Fernandez-Lazaro, C.I.; Alvarez-Alvarez, I.; Ruiz-Canela, M.; Gea, A.; Martinez-Gonzalez, M.A.; Santisteban, M.; Toledo, E. Leisure-time physical activity, sedentary behavior, and risk of breast cancer: Results from the SUN (‘Seguimiento Universidad De Navarra’) project. Prev. Med. 2021, 148, 106535. [Google Scholar] [CrossRef]
- Shanmugalingam, T.; Crawley, D.; Bosco, C.; Melvin, J.; Rohrmann, S.; Chowdhury, S.; Holmberg, L.; Van Hemelrijck, M. Obesity and cancer: The role of vitamin D. BMC Cancer 2014, 14, 712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blum, M.; Dolnikowski, G.; Seyoum, E.; Harris, S.S.; Booth, S.L.; Peterson, J.; Saltzman, E.; Dawson-Hughes, B. Vitamin D(3) in fat tissue. Endocrine 2008, 33, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Kull, M.; Kallikorm, R.; Lember, M. Body mass index determines sunbathing habits: Implications on vitamin D levels. Intern. Med. J. 2009, 39, 256–258. [Google Scholar] [CrossRef] [PubMed]
- Gorham, E.D.; Garland, C.F.; Garland, F.C.; Grant, W.; Mohr, S.B.; Lipkin, M.; Newmark, H.L.; Giovannucci, E.; Wei, M.; Holick, M. Optimal vitamin D status for colorectal cancer prevention: A quantitative meta analysis. Am. J. Prev. Med 2007, 32, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Touvier, M.; Chan, D.S.; Lau, R.; Aune, D.; Vieira, R.; Greenwood, D.C.; Kampman, E.; Riboli, E.; Hercberg, S.; Norat, T. Meta-analyses of vitamin D intake, 25-hydroxyvitamin D status, vitamin D receptor polymorphisms, and colorectal cancer risk. Cancer Epidemiol. Biomark. Prev. 2011, 20, 1003–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, L.; Grandi, N.; Raum, E.; Haug, U.; Arndt, V.; Brenner, H. Meta-analysis: Longitudinal studies of serum vitamin D and colorectal cancer risk. Aliment. Pharm. 2009, 30, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Rossi, M.; McLaughlin, J.K.; Lagiou, P.; Bosetti, C.; Talamini, R.; Lipworth, L.; Giacosa, A.; Montella, M.; Franceschi, S.; Negri, E.; et al. Vitamin D intake and breast cancer risk: A case-control study in Italy. Ann. Oncol. 2009, 20, 374–378. [Google Scholar] [CrossRef]
- Abbas, S.; Linseisen, J.; Rohrmann, S.; Chang-Claude, J.; Peeters, P.H.; Engel, P.; Brustad, M.; Lund, E.; Skeie, G.; Olsen, A.; et al. Dietary intake of vitamin D and calcium and breast cancer risk in the European Prospective Investigation into Cancer and Nutrition. Nutr. Cancer 2013, 65, 178–187. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Lazaro, C.I.; Romanos-Nanclares, A.; Sánchez-Bayona, R.; Gea, A.; Sayon-Orea, C.; Martinez-Gonzalez, M.A.; Toledo, E. Dietary calcium, vitamin D, and breast cancer risk in women: Findings from the SUN cohort. Eur. J. Nutr. 2021, 60, 3783–3797. [Google Scholar] [CrossRef]
- Garland, C.F.; Garland, F.C. Do sunlight and vitamin D reduce the likelihood of colon cancer? Int. J. Epidemiol. 1980, 9, 227–231. [Google Scholar] [CrossRef]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Gordon, D.; Copeland, T.; D’Agostino, D.; et al. Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease. N. Engl. J. Med. 2019, 380, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Wactawski-Wende, J.; Kotchen, J.M.; Anderson, G.L.; Assaf, A.R.; Brunner, R.L.; O’Sullivan, M.J.; Margolis, K.L.; Ockene, J.K.; Phillips, L.; Pottern, L.; et al. Women’s Health Initiative, Calcium plus vitamin D supplementation and the risk of colorectal cancer. N. Engl. J. Med. 2006, 354, 684–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avenell, A.; MacLennan, G.S.; Jenkinson, D.J.; McPherson, G.C.; McDonald, A.M.; Pant, P.R.; Grant, A.M.; Campbell, M.K.; Anderson, F.H.; Cooper, C.; et al. Long-term follow-up for mortality and cancer in a randomized placebo-controlled trial of vitamin D3 and/or calcium (RECORD trial). J. Clin. Endocrinol. Metab. 2012, 97, 614–622. [Google Scholar] [CrossRef] [Green Version]
- Trivedi, D.P.; Doll, R.; Khaw, K.T. Effect of four monthly oral vitamin D3 (cholecalciferol) supplementation on fractures and mortality in men and women living in the community: Randomised double blind controlled trial. BMJ 2003, 326, 469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ong, J.S.; Dixon-Suen, S.C.; Han, X.; An, J.; Esophageal Cancer Consortium; 23 and Me Research Team; Liyanage, U.; Dusingize, J.C.; Schumacher, J.; Gockel, I.; et al. A comprehensive re-assessment of the association between vitamin D and cancer susceptibility using Mendelian randomization. Nat. Commun. 2021, 12, 246. [Google Scholar] [CrossRef] [PubMed]
- Vukic, M.; Neme, A.; Seuter, S.; Saksa, N.; de Mello, V.D.; Nurmi, T.; Uusitupa, M.; Tuomainen, T.P.; Virtanen, J.K.; Carlberg, C. Relevance of vitamin D receptor target genes for monitoring the vitamin D responsiveness of primary human cells. PLoS ONE 2015, 10, e0124339. [Google Scholar] [CrossRef] [Green Version]
- Seuter, S.; Virtanen, J.K.; Nurmi, T.; Pihlajamäki, J.P.; Mursu, J.; Voutilainen, S.; Tuomainen, T.-P.; Neme, A.; Carlberg, C. Molecularevaluation of vitamin D responsiveness of healthy young adults. J. Steroid. Biochem. Mol. Biol. 2017, 174, 314–321. [Google Scholar]
- Feldman, D.; Krishnan, A.V.; Swami, S.; Giovannucci, E.; Feldman, B.J. The role of vitamin D in reducing cancer risk and progression. Nat. Rev. Cancer 2014, 14, 342–357. [Google Scholar] [CrossRef]
- Charoenngam, N.; Holick, M.F. Immunologic Effects of Vitamin D on Human Health and Disease. Nutrients 2020, 12, 2097. [Google Scholar] [CrossRef]
- Gnagnarella, P.; Raimondi, S.; Aristarco, V.; Johansson, H.A.; Bellerba, F.; Corso, F.; Gandini, S. Vitamin D Receptor Polymorphisms and Cancer. Adv. Exp. Med. Biol. 2020, 1268, 53–114. [Google Scholar] [CrossRef]
- Cuevas-Sierra, A.; Ramos-Lopez, O.; Riezu-Boj, J.I.; Milagro, F.I.; Martinez, J.A. Diet, Gut Microbiota, and Obesity: Links with Host Genetics and Epigenetics and Potential Applications. Adv. Nutr. 2019, 10 (Suppl. 1), S17–S30. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Variable | Q1 | Q2 | Q3 | Q4 | p Value + |
|---|---|---|---|---|---|
| n | 4505 | 4504 | 4504 | 4504 | |
| Total vitamin D intake (µg/day) * | 2.7 (2.0–3.2) | 4.4 (4.0–4.7) | 5.8 (5.4–6.5) | 11.7 (11.0–12.5) | <0.001 |
| Age (years) | 35 (27–45) | 36 (27–46) | 35 (27–46) | 37 (28–49) | <0.001 |
| Sex (% women) | 62.1 | 59.3 | 58.4 | 59.6 | 0.003 |
| Body-mass index (kg/m2) | 22.8 (20.7–25.4) | 23.1 (20.9–25.6) | 23.1 (20.9–25.5) | 23.4 (21.0–25.9) | <0.001 |
| Height (cm) | 168 (162–174) | 168 (162–175) | 168 (162–175) | 168 (162–174) | 0.174 |
| Physical activity (METs-h/week) | 14.2 (4.2–27.5) | 14.8 (5.1–29.1) | 15.9 (5.7–29.8) | 18.9 (7.4–34.4) | <0.001 |
| Total energy intake (kcal/day) | 2517 (2048–2997) | 2362 (1976–2715) | 2041 (1682–2503) | 2358 (1975–2767) | <0.001 |
| Alcohol intake (g/day) | 2.6 (0.6–8.8) | 3.2 (0.9–8.8) | 3.1 (0.9–8.4) | 3.2 (0.9–9.0) | <0.001 |
| Sugar-sweetened beverages (servings/day) | 0.1 (0.0–0.4) | 0.1 (0.0–0.1) | 0.1 (0.0–0.1) | 0.1 (0.0–0.1) | <0.001 |
| Coffee (servings/day) | 1.0 (0.4–2.5) | 1.0 (0.4–2.5) | 1.0 (0.4–2.5) | 1.0 (0.4–2.5) | <0.001 |
| Adherence to Mediterranean Diet Score | 4 (3–5) | 4 (3–5) | 4 (3–5) | 5 (3–6) | <0.001 |
| Time of university education (years) | 5 (4–5) | 5 (4–5) | 5 (4–5) | 5 (4–5) | 0.047 |
| Smoking habit (%) | <0.001 | ||||
| Never | 47.6 | 48.7 | 50.6 | 47.7 | |
| Current | 23.8 | 22.6 | 21.5 | 20.2 | |
| Former | 28.6 | 28.7 | 27.9 | 32.1 | |
| Tobacco consumption (pack-years) | 0.5 (0.0–10.0) | 0.5 (0.0–10.0) | 0.0 (0.0–9.0) | 0.5 (0.0–11.0) | <0.001 |
| TV watching (h/day) | 1.5 (0.8–2.0) | 1.5 (0.8–2.0) | 1.4 (0.7–2.0) | 1.4 (0.8–2.0) | 0.101 |
| Solar irradiation (kWh/m2/day) | 4.0 (3.9–4.5) | 4.0 (3.7–4.6) | 4.1 (3.8–4.6) | 4.2 (3.7–4.7) | 0.192 |
| Sunlight exposure (h/year) | 1984 (1866–2816) | 1984 (1866–2822) | 1984 (1866–2887) | 2279 (1866–2887) | <0.001 |
| Family history (%) | |||||
| Breast cancer | 27.0 | 25.6 | 27.4 | 27.1 | 0.21 |
| Colorectal cancer | 14.6 | 14.6 | 15.1 | 16.3 | 0.09 |
| Obesity-Related Cancer Cases | Q1 | Q2 | Q3 | Q4 |
|---|---|---|---|---|
| Cases/person-years | 50/52657 | 57/52666 | 58/51328 | 60/50131 |
| Age adjusted | 1 (Ref.) | 1.14 (0.78–1.67) | 1.14 (0.78–1.67) | 1.01 (0.69–1.48) |
| Multivar. adjusted * | 1 (Ref.) | 1.19 (0.81–1.76) | 1.21 (0.82–1.79) | 1.06 (0.72–1.55) |
| Multivar. adjusted † | 1 (Ref.) | 1.19 (0.81–1.75) | 1.20 (0.81–1.78) | 1.02 (0.69–1.51) |
| Obesity-Related Cancer Cases | Q1 | Q2 | Q3 | Q4 |
|---|---|---|---|---|
| Cases/person-years | 48/52523 | 55/52640 | 59/51412 | 63/50205 |
| Age adjusted | 1 (Ref.) | 1.12 (0.76–1.66) | 1.19 (0.81–1.75) | 1.07 (0.73–1.56) |
| Multivar. adjusted * | 1 (Ref.) | 1.15 (0.78–1.71) | 1.27 (0.85–1.89) | 1.12 (0.76–1.65) |
| Multivar. adjusted † | 1 (Ref.) | 1.14 (0.77–1.69) | 1.25 (0.84–1.87) | 1.08 (0.73–1.61) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Bayona, R.; Bes-Rastrollo, M.; Fernández-Lázaro, C.I.; Bastyr, M.; Madariaga, A.; Pons, J.J.; Martínez-González, M.A.; Toledo, E. Vitamin D and Risk of Obesity-Related Cancers: Results from the SUN (‘Seguimiento Universidad de Navarra’) Project. Nutrients 2022, 14, 2561. https://doi.org/10.3390/nu14132561
Sánchez-Bayona R, Bes-Rastrollo M, Fernández-Lázaro CI, Bastyr M, Madariaga A, Pons JJ, Martínez-González MA, Toledo E. Vitamin D and Risk of Obesity-Related Cancers: Results from the SUN (‘Seguimiento Universidad de Navarra’) Project. Nutrients. 2022; 14(13):2561. https://doi.org/10.3390/nu14132561
Chicago/Turabian StyleSánchez-Bayona, Rodrigo, Maira Bes-Rastrollo, Cesar I. Fernández-Lázaro, Maite Bastyr, Ainhoa Madariaga, Juan J. Pons, Miguel A. Martínez-González, and Estefanía Toledo. 2022. "Vitamin D and Risk of Obesity-Related Cancers: Results from the SUN (‘Seguimiento Universidad de Navarra’) Project" Nutrients 14, no. 13: 2561. https://doi.org/10.3390/nu14132561
APA StyleSánchez-Bayona, R., Bes-Rastrollo, M., Fernández-Lázaro, C. I., Bastyr, M., Madariaga, A., Pons, J. J., Martínez-González, M. A., & Toledo, E. (2022). Vitamin D and Risk of Obesity-Related Cancers: Results from the SUN (‘Seguimiento Universidad de Navarra’) Project. Nutrients, 14(13), 2561. https://doi.org/10.3390/nu14132561