
Patterns and Predictors of Breast Milk Feeding from Birth to Age 4 Months among Primiparous African American Mother–Infant Dyads

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Procedures
2.3. Measures
2.3.1. Sociodemographic Characteristics
2.3.2. Psychosocial Characteristics
2.3.3. Assessment of Infant Feeding Practices
2.4. Statistical Analyses
3. Results
3.1. Sociodemographic Characteristics
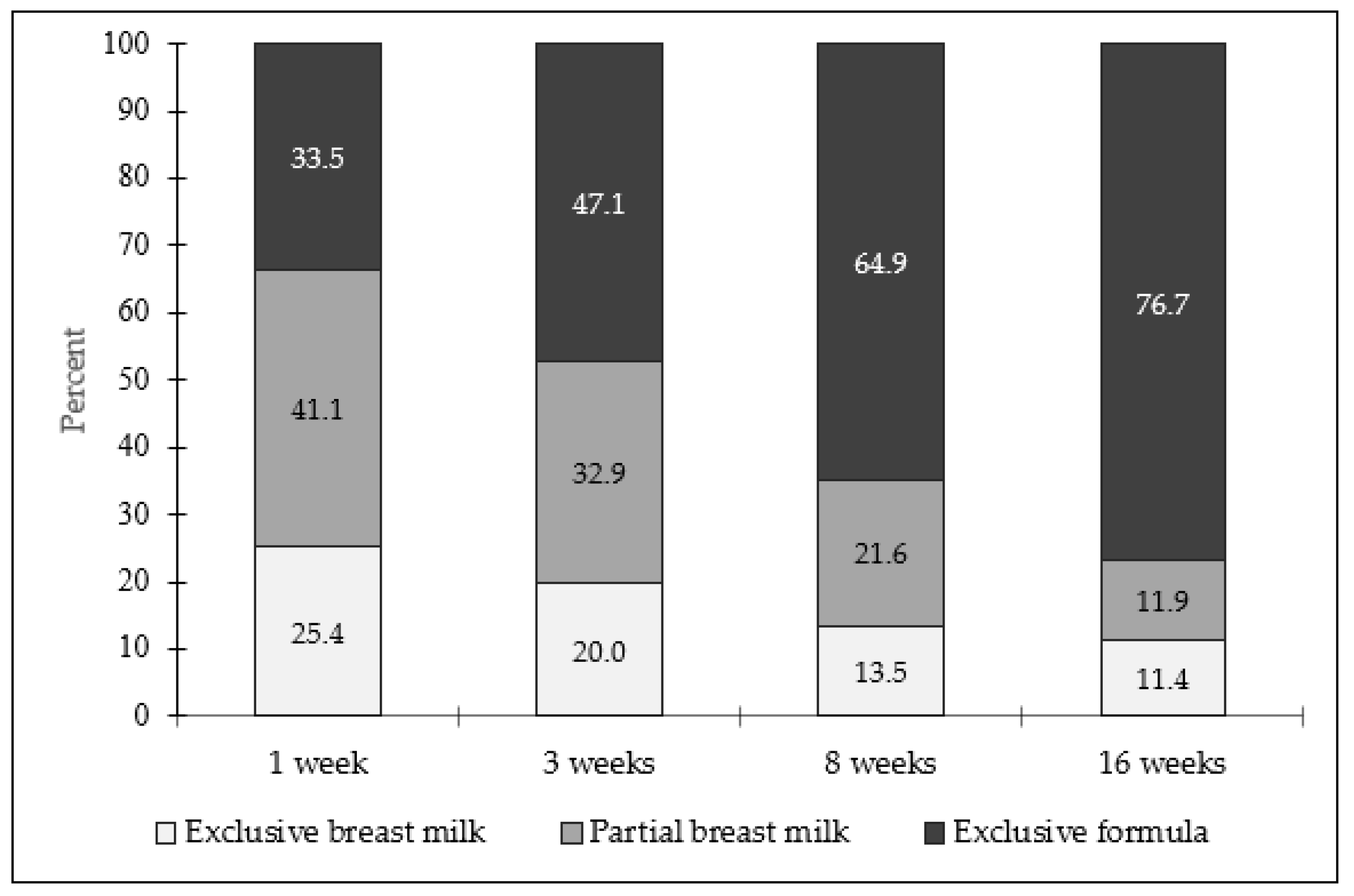
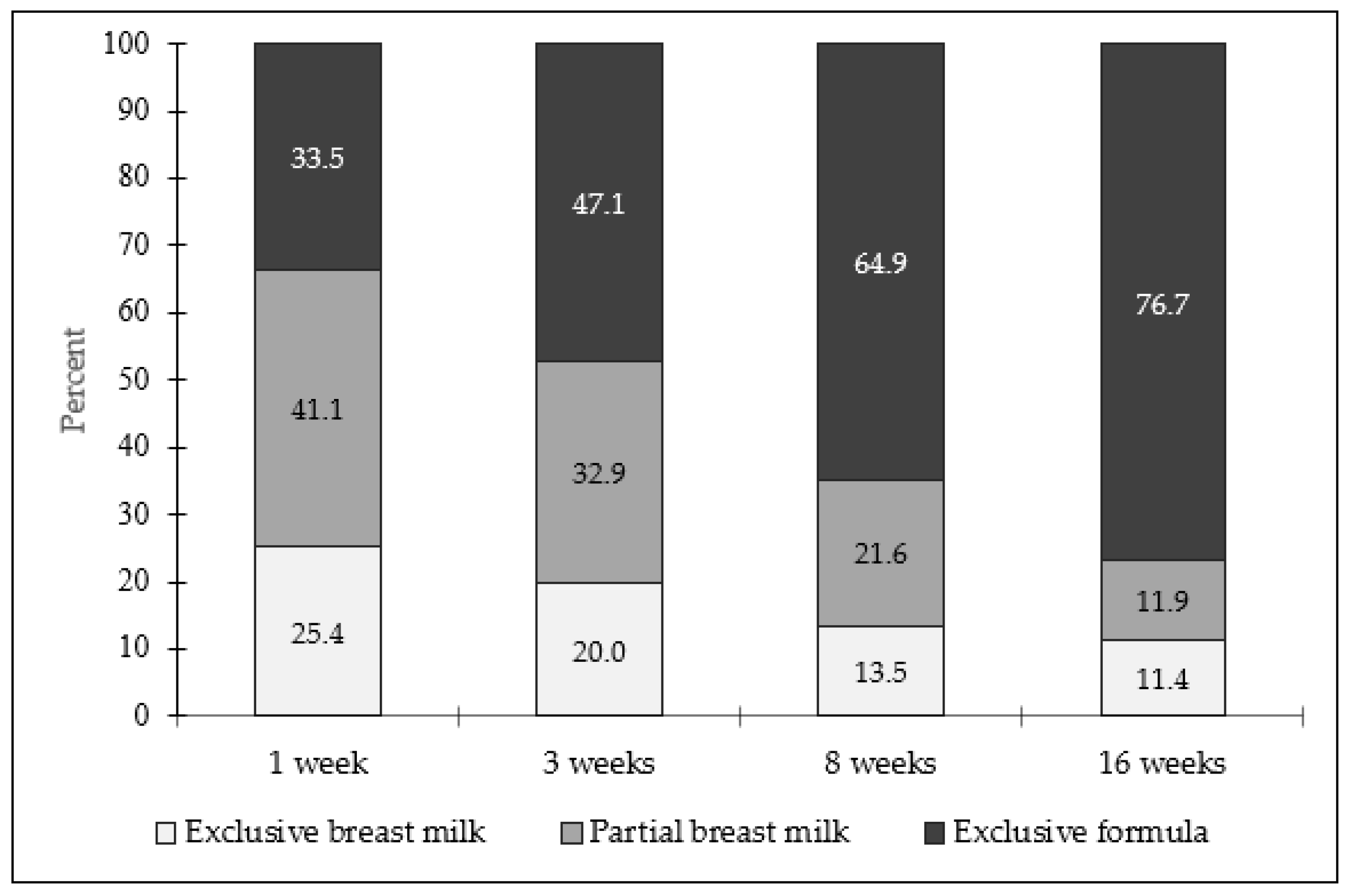
3.2. Infant Feeding Practices
3.3. Associations between Sociodemographic and Psychosocial Characteristics and Any Breast Milk Feeding by Infant Age 1 Week
3.4. Associations between Sociodemographic and Psychosocial Characteristics and Cessation of Any Breast Milk Feeding by Infant Ages 3, 8, and 16 Weeks
3.5. Bottle-Feeding Practices
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025, 9th Edition. December 2020. Available online: https://www.dietaryguidelines.gov (accessed on 3 November 2021).
- American Academy of Pediatrics Committee on Nutrition. Pediatric Nutrition, 8th ed.; Kleinman, R.E., Greer, F.R., Eds.; American Academy of Pediatrics: Itasca, IL, USA, 2019. [Google Scholar] [CrossRef]
- Chowdhury, R.; Sinha, B.; Sankar, M.J.; Taneja, S.; Bhandari, N.; Rollins, N.; Bahl, R.; Martines, J. Breastfeeding and maternal health outcomes: A systematic review and meta-analysis. Acta Paediatr. Int. J. Paediatr. 2015, 104, 96–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, B.; Jin, K.; Ding, D. Breastfeeding and maternal cardiovascular risk factors and outcomes: A systematic review. PLoS ONE 2017, 12, e0187923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ip, S.; Chung, M.; Raman, G.; Chew, P.; Magula, N.; DeVine, D.; Trikalinos, T.; Lau, J. Breastfeeding and maternal and infant health outcomes in developed countries. Evid. Rep. Technol. Assess. 2007, 153, 1–186. [Google Scholar]
- Anstey, E.H.; Macgowan, C.A.; Allen, J.A. Five-year progress update on the Surgeon General’s Call to Action to Support Breastfeeding, 2011. J. Women’s Health 2017, 25, 768–776. [Google Scholar] [CrossRef] [Green Version]
- Dieterich, C.M.; Felice, J.P.; O’Sullivan, E.; Rasmussen, K.M. Breastfeeding and health outcomes for the mother-infant dyad. Pediatr. Clin. N. Am. 2013, 60, 31–48. [Google Scholar] [CrossRef] [Green Version]
- Louis-Jacques, A.; Deubel, T.F.; Taylor, M.; Stuebe, A.M. Racial and ethnic disparities in U.S. breastfeeding and implications for maternal and child health outcomes. Semin. Perinatol. 2017, 41, 299–307. [Google Scholar] [CrossRef] [Green Version]
- Beauregard, J.L.; Hamner, H.C.; Chen, J.; Avila-Rodriguez, W.; Elam-Evans, L.D.; Perrine, C.G. Racial disparities in breastfeeding initiation and duration among U.S. infants born in 2015. Morb. Mortal. Wkly. Rep. 2019, 68, 745–748. [Google Scholar] [CrossRef]
- Li, R.; Perrine, C.G.; Anstey, E.H.; Chen, J.; MacGowan, C.A.; Elam-Evans, L.D. Breastfeeding trends by race/ethnicity among US children born from 2009 to 2015. JAMA Pediatr. 2019, 173, e193319. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Breastfeeding Among US Children Born 2011–2018, CDC National Immunization Survey. Available online: https://www.cdc.gov/breastfeeding/data/nis_data/results.html (accessed on 19 November 2021).
- Odar Stough, C.; Khalsa, A.S.; Nabors, L.A.; Merianos, A.L.; Peugh, J. Predictors of exclusive breastfeeding for 6 months in a national sample of US children. Am. J. Health Promot. 2019, 33, 48–56. [Google Scholar] [CrossRef]
- Jones, J.R.; Kogan, M.D.; Singh, G.K.; Dee, D.L.; Grummer-Strawn, L.M. Factors associated with exclusive breastfeeding in the United States. Pediatrics 2011, 128, 1117–1125. [Google Scholar] [CrossRef] [Green Version]
- Haga, S.M.; Lisøy, C.; Drozd, F.; Valla, L.; Slinning, K. A population-based study of the relationship between perinatal depressive symptoms and breastfeeding: A cross-lagged panel study. Arch. Women’s. Ment. Health 2018, 21, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Ogbuanu, C.; Glover, S.; Probst, J.; Liu, J.; Hussey, J. The effect of maternity leave length and time of return to work on breastfeeding. Pediatrics 2011, 127, e1414–e1427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, K.M.; Power, M.L.; Queenan, J.T.; Schulkin, J. Racial and ethnic disparities in breastfeeding. Breastfeed. Med. 2015, 10, 186–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimacali, D.; Marmol, C.; Fortune, J.; Rodriguez, J.; Pc, C.; Baker, H. Barriers and promoters to initiating and sustaining breastfeeding among African American women. Int. Public Health J. 2018, 10, 431–444. [Google Scholar]
- Lavner, J.A.; Stansfield, B.K.; Beach, S.R.H.; Brody, G.H.; Birch, L.L. Sleep SAAF: A responsive parenting intervention to prevent excessive weight gain and obesity among African American infants. BMC Pediatr. 2019, 19, 224. [Google Scholar] [CrossRef]
- Paul, I.M.; Williams, J.S.; Anzman-Frasca, S.; Beiler, J.S.; Makova, K.D.; Marini, M.E.; Hess, L.B.; Rzucidlo, S.E.; Verdiglione, N.; Mindell, J.A.; et al. The Intervention Nurses Start Infants Growing on Healthy Trajectories (INSIGHT) study. BMC Pediatr. 2014, 14, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Onis, M.; Garza, C.; Victora, C.G.; Onyango, A.W.; Frongillo, E.A.; Martines, J. The WHO Multicentre Growth Reference Study: Planning, study design, and methodology. Food Nutr. Bull. 2004, 25, 15–26. [Google Scholar] [CrossRef] [Green Version]
- Hager, E.R.; Quigg, A.M.; Black, M.M.; Coleman, S.M.; Heeren, T.; Rose-Jacobs, R.; Cook, J.T.; de Cuba, S.A.E.; Casey, P.H.; Chilton, M.; et al. Development and validity of a 2-item screen to identify families at risk for food insecurity. Pediatrics 2010, 126, e26–e32. [Google Scholar] [CrossRef] [Green Version]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Funk, J.L.; Rogge, R.D. Testing the ruler with item response theory: Increasing precision of measurement for relationship satisfaction with the Couples Satisfaction Index. J. Fam. Psychol. 2007, 21, 572–583. [Google Scholar] [CrossRef]
- Russel, D.; Cutrona, C. The provisions of social relationships and adaptation to stress. In Proceedings of the Annual Meeting of the American Psychological Association, Anaheim, CA, USA, 20–22 January 1984. [Google Scholar]
- Landrine, H.; Klonoff, E. The schedule of racist events: A measure of racial discrimination and a study of its negative physical and mental health consequences. J. Black Psychol. 1993, 22, 144–168. [Google Scholar] [CrossRef]
- Stifter, C.A.; Anzman-Frasca, S.; Birch, L.L.; Voegtline, K. Parent use of food to soothe infant/toddler distress and child weight status. An exploratory study. Appetite 2011, 57, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Bibbins-Domingo, K. Primary care interventions to support breastfeeding US preventive services task force recommendation statement. JAMA 2016, 316, 1688–1693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SAS Software, Version 9.4 of the SAS System for Windows; SAS Institute Inc.: Cary, NC, USA, 2015.
- Anstey, E.H.; Chen, J.; Elam-Evans, L.D.; Perrine, C.G. Racial and geographic differences in breastfeeding—United States, 2011–2015. MMWR. Morb. Mortal. Wkly. Rep. 2017, 66, 723–727. [Google Scholar] [CrossRef]
- Petit, M.; Smart, D.A.; Sattler, V.; Wood, N.K. Examination of factors that contribute to breastfeeding disparities and inequities for Black women in the US. J. Nutr. Educ. Behav. 2021, 53, 977–986. [Google Scholar] [CrossRef]
- Kramer, M.; Kakuma, R. Optimal duration of exclusive breastfeeding. Cochrane Database Syst. Rev. 2012, 8, CD003517. [Google Scholar] [CrossRef]
- Yeung, H.; Leff, M.; Rhee, K.E. Effect of exclusive breastfeeding among overweight and obese mothers on infant weight-for-length percentile at 1 year. Breastfeed. Med. 2017, 12, 39–47. [Google Scholar] [CrossRef]
- Orr, S.K.; Dachner, N.; Frank, L.; Tarasuk, V. Relation between household food insecurity and breastfeeding in Canada. Can. Med. Assoc. J. 2018, 190, E312–E319. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, V.; Prell, M.; Cheng, X. The Economic Impacts of Breastfeeding: A Focus on USDA’s Special Supplemental Nutrition Program for Women, Infants, and Children (WIC); United States Department of Agriculture: Washington, DC, USA, 2019. [Google Scholar]
- Li, K.; Wen, M.; Reynolds, M.; Zhang, Q. WIC participation and breastfeeding after the 2009 WIC revision: A propensity score approach. Int. J. Environ. Res. Public Health 2019, 16, 2645. [Google Scholar] [CrossRef] [Green Version]
- Davis, C.; Villalobos, A.V.K.; Turner, M.M.; Long, S.; Lapinski, M.K. Racism and resistance: A qualitative study of bias as a barrier to breastfeeding. Breastfeed. Med. 2021, 16, 471–480. [Google Scholar] [CrossRef]
- Scott, K.A.; Britton, L.; McLemore, M.R. The ethics of perinatal care for Black women: Dismantling the structural racism in “mother blame” narratives. J. Perinat. Neonatal Nurs. 2019, 33, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Appleton, J.; Russell, C.G.; Laws, R.; Fowler, C.; Campbell, K.; Denney-Wilson, E. Infant formula feeding practices associated with rapid weight gain: A systematic review. Matern. Child Nutr. 2018, 14, e12602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savage, J.S.; Hohman, E.E.; Marini, M.E.; Shelly, A.; Paul, I.M.; Birch, L.L. INSIGHT responsive parenting intervention and infant feeding practices: Randomized clinical trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devane-Johnson, S.; Woods Giscombe, C.; Williams, R.; Fogel, C.; Thoyre, S. A qualitative stude of social, cultural, and historial influences on African American womens’ infant feeding practices. J. Perinat. Educ. 2017, 27, 71–85. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic | n | |
|---|---|---|
| Mother | ||
| Age (years), mean (SD) | 185 | 22.9 (4.6) |
| Race, African American/Black, n (%) | 185 | 185 (100.0) |
| Prepregnancy BMI, mean (SD) | 184 | 28.3 (8.4) |
| Romantic relationship status, n (%) | 185 | |
| Single | 71 (38.4) | |
| Married, living together | 22 (11.9) | |
| Married, but not living together | 1 (0.5) | |
| Living together | 58 (31.4) | |
| Involved, but not living together | 33 (17.8) | |
| Working prepregnancy, n (%) | 185 | |
| Full-time | 64 (34.6) | |
| Part-time | 29 (15.7) | |
| Student | 9 (4.9) | |
| Unemployed | 80 (43.2) | |
| Other | 3 (1.6) | |
| Currently working outside the home, n (%) | 185 | |
| 1 week | 0 (0.0) | |
| 3 weeks | 19 (10.3) | |
| 8 weeks | 74 (40.0) | |
| 16 weeks | 103 (55.7) | |
| Annual household income, n (%) | 184 | |
| <$10,000 | 41 (22.8) | |
| $10,000–24,999 | 23 (12.5) | |
| $25,000–49,999 | 26 (14.3) | |
| $50,000 or more | 16 (8.7) | |
| Don’t know | 72 (39.1) | |
| Refuse to answer | 6 (3.3) | |
| Education, n (%) | 185 | |
| Some high school | 22 (11.9) | |
| High school graduate | 91 (49.1) | |
| Some college or technical school | 48 (26.0) | |
| College graduate or graduate degree | 24 (13.0) | |
| Number in household, mean (SD) | 139 | 2.0 (1.5) |
| Federal Nutrition Assistance, n (%) | ||
| SNAP participant | 179 | 84 (46.9) |
| WIC participant | 182 | 139 (76.4) |
| Food insecurity, n (%) | 80 (43.2) | |
| Depressive symptoms, mean (SD) | 184 | 0.64 (0.45) |
| Romantic relationship satisfaction, mean (SD) | 114 | 16.1 (2.8) |
| Social provision, mean (SD) | 185 | |
| Reliable alliance | 3.4 (0.53) | |
| Guidance | 3.1 (0.56) | |
| Racial discrimination, mean (SD) | 185 | 1.4 (0.58) |
| Infant | ||
| Male, n (%) | 185 | 89 (48.1) |
| Gestational age (weeks), mean (SD) | 185 | 39.1 (1.1) |
| Weight (kg) at enrollment, mean (SD) | 185 | 6.0 (0.35) |
| Length (cm) at enrollment, mean (SD) | 185 | 48.7 (1.7) |
| WFLz at enrollment, mean (SD) | 182 | −0.34 (0.96) |
| 1 Week | ||
|---|---|---|
| Characteristics a | OR | 95% CI |
| Sociodemographic | ||
| Age (years) | 1.08 | 1.00–1.16 |
| Prepregnancy BMI | 1.09 * | 1.04–1.15 |
| In a romantic relationship b | 1.53 | 0.82–2.86 |
| Worked outside the home prepregnancy c | 2.25 * | 1.21–4.18 |
| Number in household | 1.01 | 0.77–1.29 |
| SNAP participation | 0.55 | 0.30–1.04 |
| WIC participation | 0.21 * | 0.08–0.56 |
| Food insecurity | 2.49 * | 1.29–4.77 |
| Infant WFLz at enrollment | 0.75 | 0.54–1.05 |
| Psychosocial | ||
| Depressive symptoms | 1.17 | 0.58–2.33 |
| Relationship satisfaction | 1.00 | 0.87–1.16 |
| Social provision | ||
| Reliable alliance | 1.07 | 0.61–1.89 |
| Guidance | 1.30 | 0.74–2.28 |
| Racial discrimination | 1.16 | 0.67–2.00 |
| 3 Weeks | 8 Weeks | 16 Weeks | ||||
|---|---|---|---|---|---|---|
| Characteristics a | OR | 95% CI | OR | 95% CI | OR | 95% CI |
| Sociodemographic | ||||||
| Age (years) | 0.90 | 0.81–1.00 | 0.93 | 0.87–1.00 | 0.92 * | 0.85–0.98 |
| Prepregnancy BMI | 0.97 | 0.92–1.03 | 0.95 * | 0.91–0.99 | 1.01 | 0.96–1.05 |
| In a romantic relationship b | 0.67 | 0.28–1.63 | 1.15 | 0.55–2.42 | 1.16 | 0.54–2.52 |
| Currently working outside the home c | ||||||
| 3 weeks | 1.03 | 0.25–5.20 | ||||
| 8 weeks | 1.04 | 0.50–2.15 | ||||
| 16 weeks | 1.13 | 0.53–2.35 | ||||
| Number in household | 1.30 | 0.96–1.75 | 1.07 | 0.82–1.39 | 1.40 | 0.99–1.95 |
| SNAP participation | 2.86 * | 1.13–5.21 | 2.33 * | 1.11–4.91 | 2.06 | 0.93–4.57 |
| WIC participation | 1.64 | 0.60–4.49 | 2.38 * | 1.07–5.27 | 2.16 | 0.98–4.76 |
| Food insecurity | 1.20 | 0.50–2.84 | 0.66 | 0.32–1.33 | 1.27 | 0.61–2.67 |
| Infant WFLz at enrollment | 1.31 | 0.80–2.13 | 1.31 | 0.88–1.95 | 0.98 | 0.65–1.47 |
| Psychosocial | ||||||
| Depressive symptoms | 1.74 | 0.74–4.10 | 0.59 | 0.25–1.22 | 0.58 | 0.27–1.27 |
| Relationship satisfaction | 1.05 | 0.85–1.31 | 1.04 | 0.89–1.22 | 0.95 | 0.80–1.14 |
| Social provision | ||||||
| Reliable alliance | 1.18 | 0.37–1.90 | 1.25 | 0.63–2.45 | 1.15 | 0.57–2.33 |
| Guidance | 1.05 | 0.42–2.63 | 0.79 | 0.37–1.66 | 1.23 | 0.64–2.36 |
| Racial discrimination | 2.14 * | 1.10–4.17 | 1.31 | 0.71–2.42 | 0.89 | 0.40–1.94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moore, A.M.; Smith, J.J.; Stansfield, B.K.; Savage, J.S.; Lavner, J.A. Patterns and Predictors of Breast Milk Feeding from Birth to Age 4 Months among Primiparous African American Mother–Infant Dyads. Nutrients 2022, 14, 2350. https://doi.org/10.3390/nu14112350
Moore AM, Smith JJ, Stansfield BK, Savage JS, Lavner JA. Patterns and Predictors of Breast Milk Feeding from Birth to Age 4 Months among Primiparous African American Mother–Infant Dyads. Nutrients. 2022; 14(11):2350. https://doi.org/10.3390/nu14112350
Chicago/Turabian StyleMoore, Amy M., Jessica J. Smith, Brian K. Stansfield, Jennifer S. Savage, and Justin A. Lavner. 2022. "Patterns and Predictors of Breast Milk Feeding from Birth to Age 4 Months among Primiparous African American Mother–Infant Dyads" Nutrients 14, no. 11: 2350. https://doi.org/10.3390/nu14112350
APA StyleMoore, A. M., Smith, J. J., Stansfield, B. K., Savage, J. S., & Lavner, J. A. (2022). Patterns and Predictors of Breast Milk Feeding from Birth to Age 4 Months among Primiparous African American Mother–Infant Dyads. Nutrients, 14(11), 2350. https://doi.org/10.3390/nu14112350