
Food Insecurity, Dietary Diversity, and Coping Strategies in Jordan during the COVID-19 Pandemic: A Cross-Sectional Study

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethical Approval
2.3. Survey Tool
2.4. Sample Size
2.5. Data Classification
2.6. Statistical Analysis
3. Results
3.1. Socio-Demographic Characteristics
3.2. Household Food Security Status
3.3. Determinants of Household Food Insecurity
3.4. Weekly Food Group Consumption
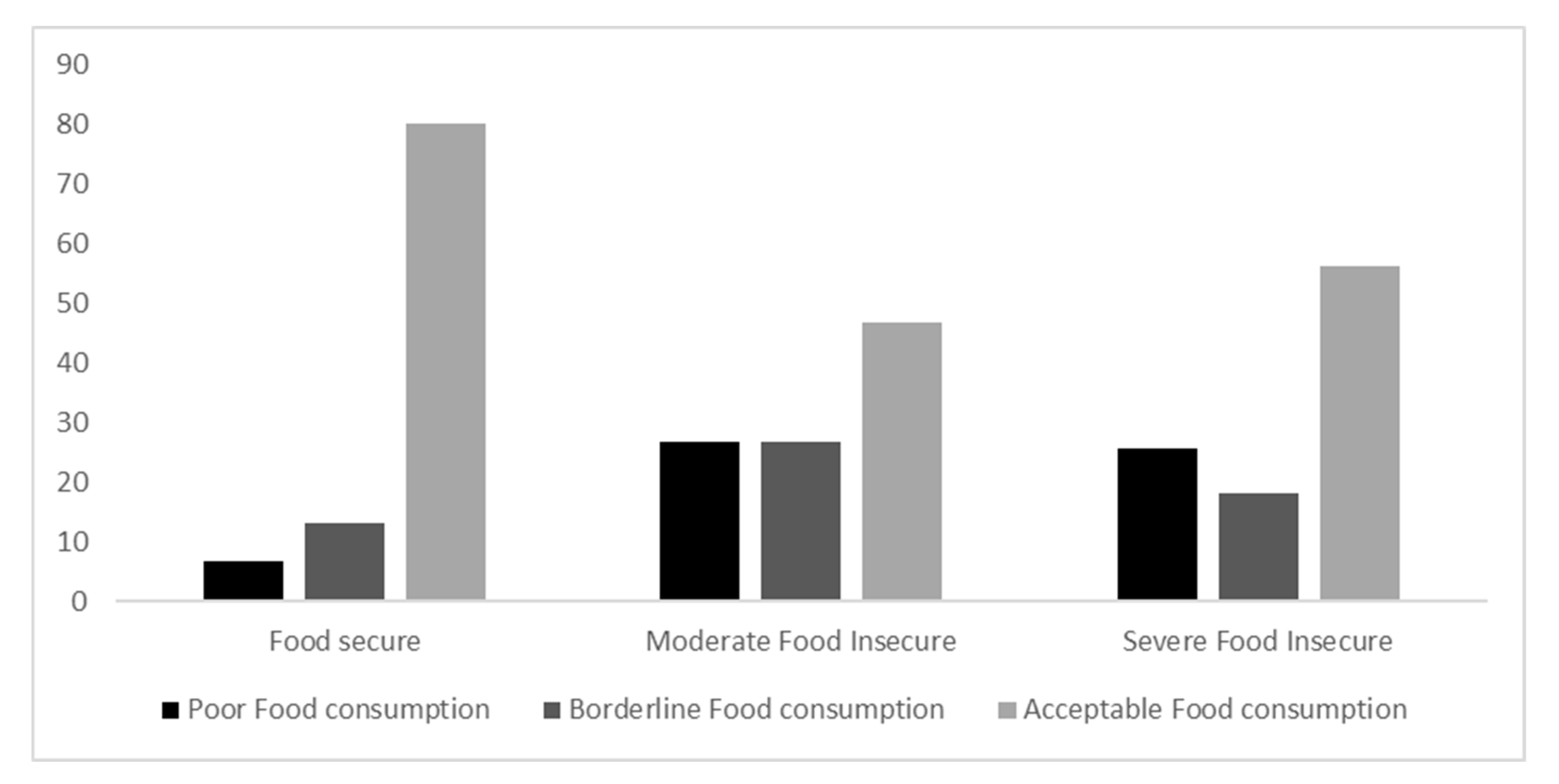
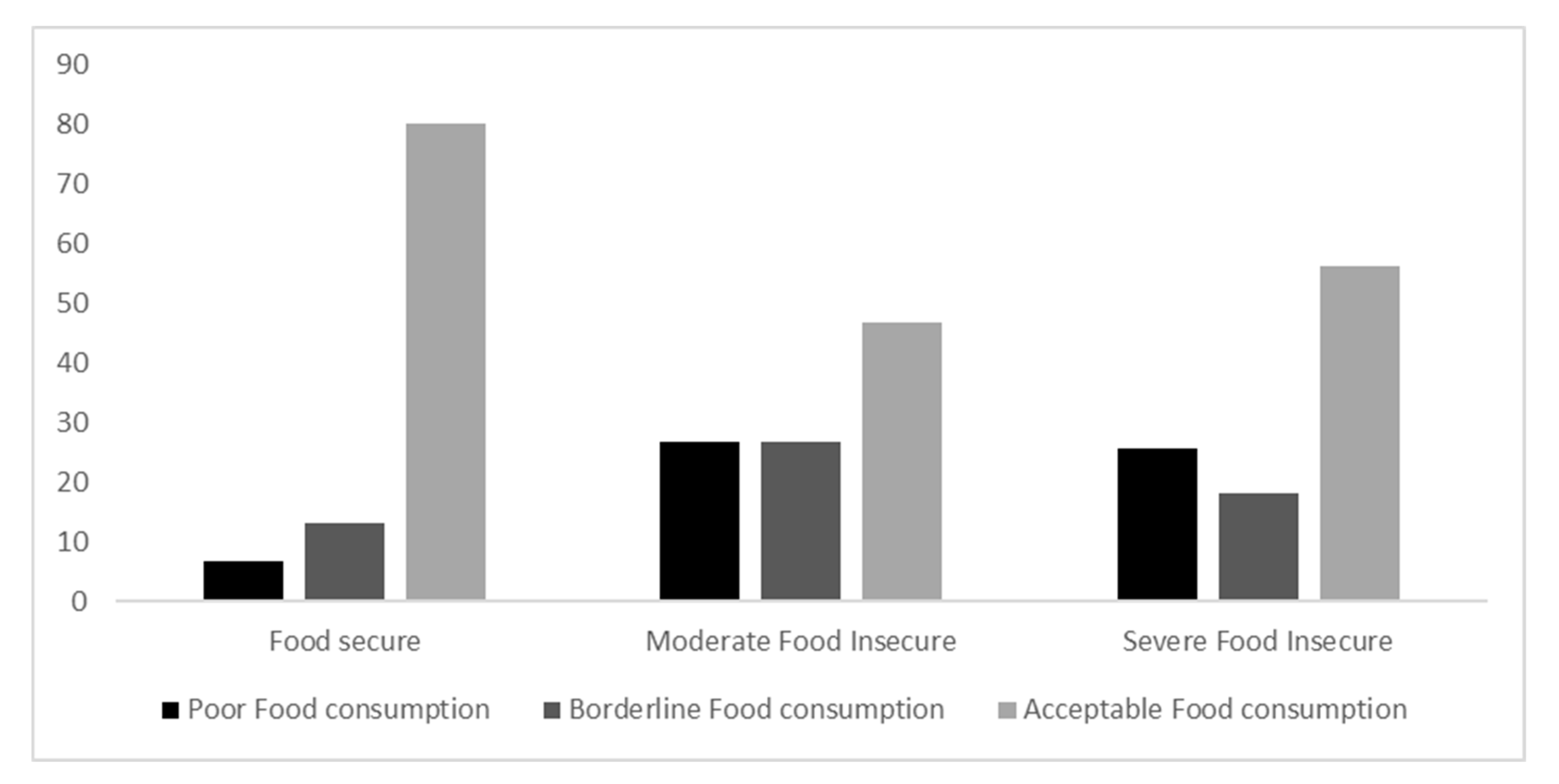
3.5. Food Consumption Scores
3.6. Food-Based Coping Strategies during the Last Week
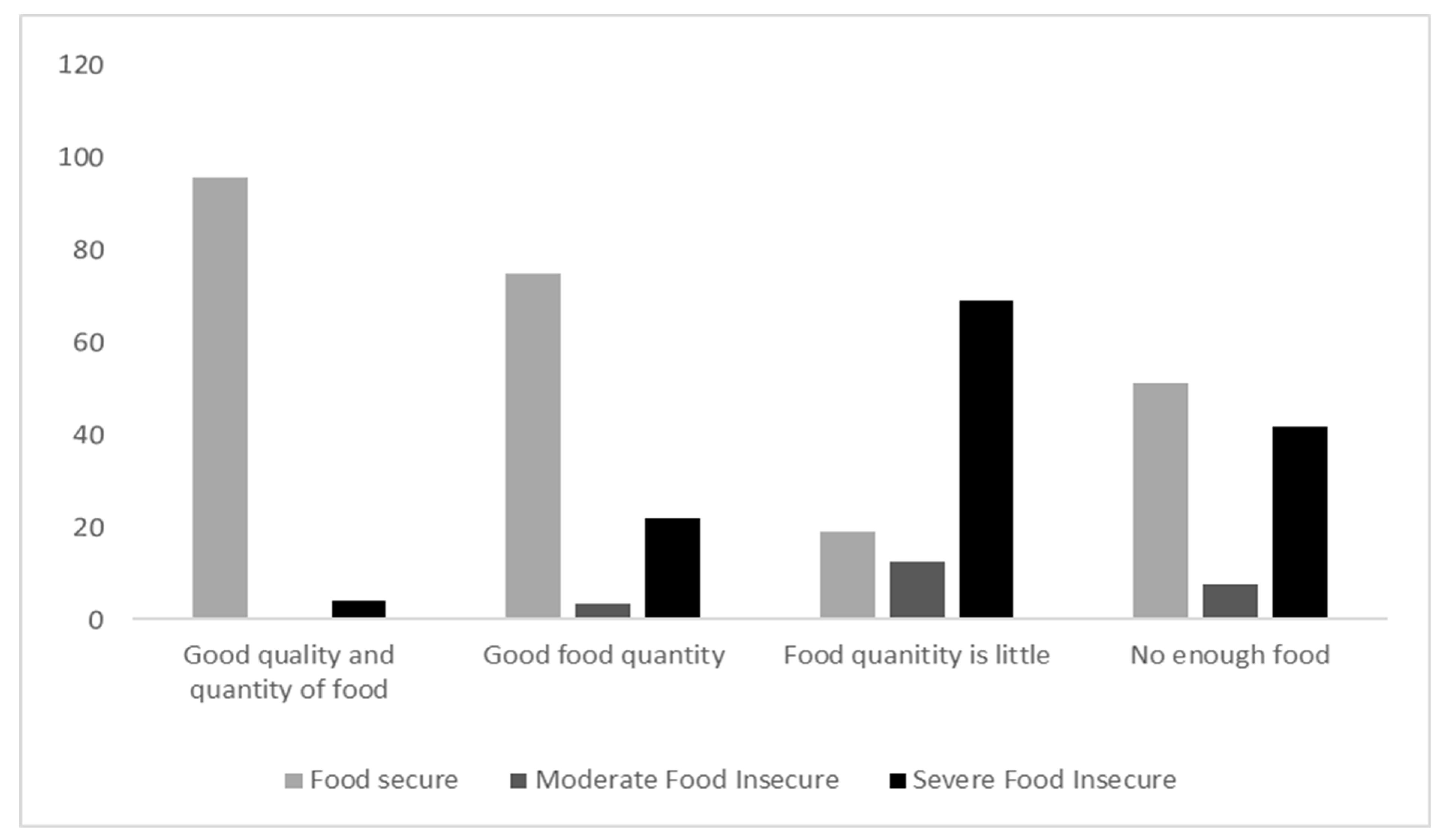
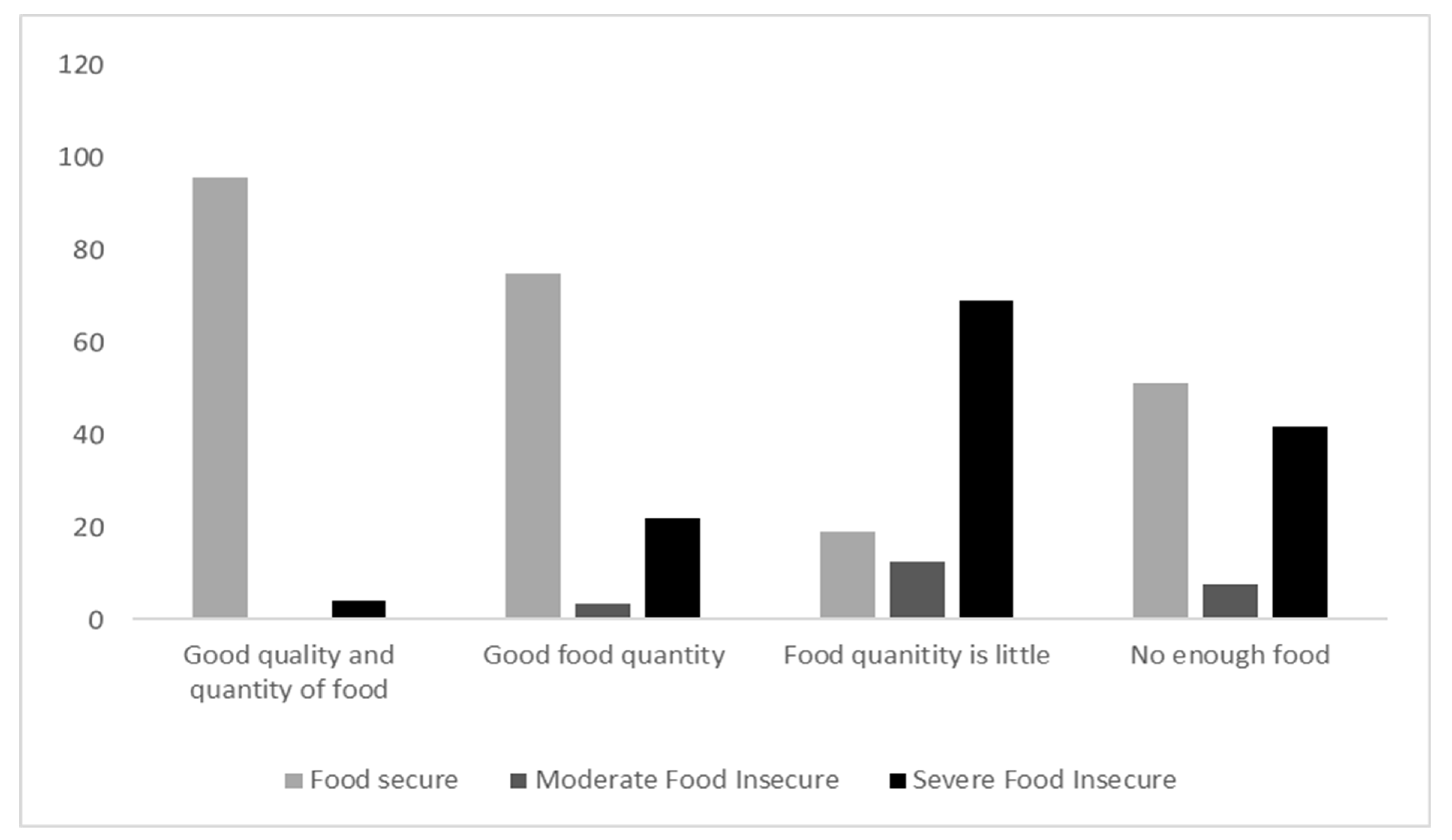
3.7. Food Quality and Quantity
4. Discussion
- Ensure the availability of food at the national, household, and individual levels, with the following sub-objectives:
- A
- Achievement of the maximum potential of local food production
- B
- Provision of a sufficient and stable supply of imported items
- C
- Improvement of regional collaboration and integration of the different aspects of food security
- D
- Reduction in food loss and waste, and enhanced food safety
- Optimize the utilization and stability of food, with the following sub-objectives:
- A
- Improvement of food quality for all people in Jordan
5. Study Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- CDC. Basics of COVID-19. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/your-health/about-covid-19/basics-covid-19.html (accessed on 10 March 2022).
- Fauci, A.S.; Lane, H.C.; Redfield, R.R. COVID-19—Navigating the Uncharted. N. Engl. J. Med. 2020, 382, 1268–1269. [Google Scholar] [CrossRef] [PubMed]
- Velavan, T.P.; Meyer, C.G. The COVID-19 epidemic. Trop. Med. Int. Health 2020, 25, 278–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 pathophysiology: A review. Clin. Immunol. 2020, 215, 108427. [Google Scholar] [CrossRef] [PubMed]
- WHO. Coronavirus Disease (COVID-19). 2022. Available online: https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed on 24 March 2022).
- WHO. WHO Coronavirus (COVID-19) Dashboard. 2022. Retrieved 2022, from World Health Organization. Available online: https://covid19.who.int/ (accessed on 24 March 2022).
- Jordanian Ministry of Health (JMOH). COVID-19 Awareness Information—Jordan. 2021. Available online: https://corona.moh.gov.jo/en (accessed on 23 March 2022).
- Al-Domi, H.; Al-Dalaeen, A.; Al-Rosan, S.; Batarseh, N.; Nawaiseh, H. Healthy Nutritional Behavior during COVID-19 lockdown: A cross-sectional study. Clin. Nutr. ESPEN 2021, 42, 132–137. [Google Scholar] [CrossRef]
- Al-Tammemi, A.B. The Battle Against COVID-19 in Jordan: An Early Overview of the Jordanian Experience. Front. Public Health 2020, 8, 188. [Google Scholar] [CrossRef]
- Al-Tammemi, A.B.; Akour, A.; Alfalah, L. Is it just about physical health? an online cross-sectional study exploring the psychological distress among university students in jordan in the midst of COVID-19 pandemic. Front. Psychol. 2020, 11, 562213. [Google Scholar] [CrossRef]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Kawohl, W.; Nordt, C. COVID-19, unemployment, and suicide. Lancet Psychiatry 2020, 7, 389–390. [Google Scholar] [CrossRef]
- Mardones, F.O.; Rich, K.M.; Boden, L.A.; Moreno-Switt, A.I.; Caipo, M.L.; Zimin-Veselkoff, N.; Alateeqi, A.M.; Baltenweck, I. The COVID-19 pandemic and global food security. Front. Vet. Sci. 2020, 7, 578508. [Google Scholar] [CrossRef]
- Petrosky-Nadeau, N.; Valletta, R.G. An unemployment crisis after the onset of COVID-19. FRBSF Econ. Lett. 2020, 12, 1–5. [Google Scholar]
- Pérez-Escamilla, R.; Segall-Corrêa, A.M. Food insecurity measurement and indicators. Rev. Nutr. 2008, 21, 15s–26s. [Google Scholar] [CrossRef]
- Gundersen, C.; Hake, M.; Dewey, A.; Engelhard, E. Food Insecurity during COVID-19. Appl. Econ. Perspect. Policy 2020, 43, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Food and Agricultural Organization (FAO). Hunger and Food Insecurity. 2021. Retrieved Nov, 2021. Available online: https://www.fao.org/hunger/en/ (accessed on 12 February 2022).
- Laborde, D.; Martin, W.; Swinnen, J.; Vos, R. COVID-19 risks to global food security. Science 2020, 369, 500–502. [Google Scholar] [CrossRef] [PubMed]
- Gundersen, C.; Ziliak, J.P. Food insecurity and health outcomes. Health Aff. 2015, 34, 1830–1839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Hara, S.; Toussaint, E.C. Food access in crisis: Food security and COVID-19. Ecol. Econ. 2021, 180, 106859. [Google Scholar] [CrossRef]
- Sahyoun, N.R.; Nord, M.; Sassine, A.J.; Seyfert, K.; Hwalla, N.; Ghattas, H. Development and validation of an Arab family food security scale. J. Nutr. 2014, 144, 751–757. [Google Scholar] [CrossRef] [Green Version]
- Food and Agricultural Organization (FAO). FIES Survey Modules. 2014. Available online: https://www.fao.org/3/BL404AR/bl404ar.pdf (accessed on 30 March 2022).
- Sheikomar, O.B.; Dean, W.; Ghattas, H.; Sahyoun, N.R. Validity of the food insecurity experience scale (FIES) for use in league of Arab states (LAS) and characteristics of food insecure individuals by the human development index (HDI). Curr. Dev. Nutr. 2021, 5, nzab017. [Google Scholar] [CrossRef]
- World Food Programme, Vulnerability Analysis and Mapping. Technical Guidance Sheet, Food Consumption and Analysis. Calculation and Use of the Food Consumption Score in Food Security Analysis. 2008. Available online: https://documents.wfp.org/stellent/groups/public/documents/manual_guide_proced/wfp197216.pdf (accessed on 10 January 2022).
- Elsahoryi, N.; Al-Sayyed, H.; Odeh, M.; McGrattan, A.; Hammad, F. Effect of COVID-19 on food security: A cross-sectional survey. Clin. Nutr. ESPEN 2020, 40, 171–178. [Google Scholar] [CrossRef]
- Mutisya, M.; Ngware, M.W.; Kabiru, C.W.; Kandala, N.-B. The effect of education on household food security in two informal urban settlements in Kenya: A longitudinal analysis. Food Secur. 2016, 8, 743–756. [Google Scholar] [CrossRef] [Green Version]
- De Muro, P.; Burchi, F. Education for Rural People: A Neglected Key to Food Security: Department of Economics-University Roma Tre. 2007. Available online: https://www.die-gdi.de/uploads/media/wp78romatre.pdf (accessed on 3 May 2022).
- Gebre, G.G. Determinants of food insecurity among households in Addis Ababa city, Ethiopia. Interdiscip. Descr. Complex Syst. INDECS 2012, 10, 159–173. [Google Scholar] [CrossRef]
- Bashir, M.K.; Schilizzi, S. Determinants of rural household food security: A comparative analysis of African and Asian studies. J. Sci. Food Agric. 2013, 93, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- De Muro, P.; Burchi, F. Education for Rural People and Food Security. A cross Country Analysis; Food and Agricultural Organization of the United Nations: Rome, Italy, 2007. [Google Scholar]
- Aboaba, K.O.; Fadiji, D.M.; Hussayn, J.A. Determinants of food security among rural households in Southwestern Nigeria: USDA food security questionnaire core module approach. J. Agribus. Rural. Dev. 2020, 2, 113–124. [Google Scholar] [CrossRef]
- Kumba, J.K. The Role of Household characteristics in determining food security in Kisii Central Sub-County, Kenya. Res. Humanit. Soc. Sci. 2015, 5, 186–193. [Google Scholar]
- CEIC Data. Jordan Avg Monthly Wage per Employee: Professionals. 2021. Available online: https://www.ceicdata.com/en/jordan/average-monthly-wage-per-employee/avg-monthly-wage-per-employee-professionals (accessed on 3 May 2022).
- Tabrizi, J.S.; Nikniaz, L.; Sadeghi-Bazargani, H.; Farahbakhsh, M.; Nikniaz, Z. Socio-demographic determinants of household food insecurity among Iranian: A population-based study from Northwest of Iran. Iran. J. Public Health 2018, 47, 893–900. [Google Scholar] [PubMed]
- Aidoo, R.; Mensah, J.O.; Tuffour, T. Determinants of household food security in the Sekyere-Afram plains district of Ghana. In Proceedings of the 1st Annual International Interdisciplinary Conference, AIIC 2013—Proceedings-514-521, Azores, Portugal, 24–26 April 2013. [Google Scholar]
- Muche, M.; Endalew, B.; Koricho, T. Determinants of household food security among southwest Ethiopia rural households. Food Sci. Technol. 2014, 2, 93–100. [Google Scholar] [CrossRef]
- Department of Statistics (DOS). Unemployment Rate during the Third Quarter of 2021. Available online: http://dosweb.dos.gov.jo/unemp-q3_2021/ (accessed on 15 February 2022).
- World Food Program (WFP). Jordan Food Security Update (Implications of COVID-19). from World Food Programme. 2020. Available online: https://docs.wfp.org/api/documents/WFP-0000122056/download/ (accessed on 5 March 2022).
- Loopstra, R.; Tarasuk, V. Severity of household food insecurity is sensitive to change in household income and employment status among low-income families. J. Nutr. 2013, 143, 1316–1323. [Google Scholar] [CrossRef]
- Mehran, F. Measurement of employment-related income: Concepts, data sources and a test of methods. WEGO Stat. Brief 2014, 13, 1–22. [Google Scholar]
- Ibukun, C.O.; Adebayo, A.A. Household food security and the COVID-19 pandemic in Nigeria. Afr. Dev. Rev. 2021, 33 (Suppl. 1), S75–S87. [Google Scholar] [CrossRef]
- Esturk, O.; Oren, M.N. Impact of household socio-economic factors on food security: Case of Adana. Pak. J. Nutr. 2014, 13, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Sekhampu, T.J. Association of food security and household demographics in a South African township. Int. J. Soc. Sci. Humanit. Stud. 2017, 9, 157–170. [Google Scholar]
- Nour, S.S.O.M.; Abdalla, E.M. The determinants of food security in Sudan: The case of Kassala state. World J. Sci. Technol. Sustain. Dev. 2021, 18, 285–302. [Google Scholar] [CrossRef]
- Ali, S.; Noor, T.; Alam, K.J. The Determinants of food security among households in Rangpur City, Bangladesh: A logistic regression approach. IOSR J. Econ. Financ. 2016, 7, 51–56. [Google Scholar] [CrossRef]
- Tantu, A.T.; Gamebo, T.D.; Sheno, B.K.; Kabalo, M.Y. Household food insecurity and associated factors among households in Wolaita Sodo town, 2015. Agric. Food Secur. 2017, 6, 19. [Google Scholar] [CrossRef] [Green Version]
- Kirkpatrick, S.I.; Tarasuk, V. Adequacy of food spending is related to housing expenditures among lower-income Canadian households. Public Health Nutr. 2007, 10, 1464–1473. [Google Scholar] [CrossRef] [Green Version]
- El-Qudah, J.M. Food consumption patterns and prevalence of obesity in an adult population in Amman, Jordan. Aust. J. Basic. Appl. Sci. 2008, 2, 1165–1171. [Google Scholar]
- Cheikh Ismail, L.; Osaili, T.M.; Mohamad, M.N.; Al Marzouqi, A.; Jarrar, A.H.; Zampelas, A.; Habib-Mourad, C.; Abu Jamous, D.O.; Ali, H.I.; Al Sabbah, H.; et al. Assessment of eating habits and lifestyle during the coronavirus 2019 pandemic in the Middle East and North Africa region: A cross-sectional study. Br. J. Nutr. 2021, 126, 757–766. [Google Scholar] [CrossRef]
- Cheikh Ismail, L.; Osaili, T.M.; Mohamad, M.N.; Al Marzouqi, A.; Jarrar, A.H.; Abu Jamous, D.O.; Magriplis, E.; Ali, H.I.; Al Sabbah, H.; Hasan, H.; et al. Eating habits and lifestyle during COVID-19 lockdown in the United Arab Emirates: A cross-sectional study. Nutrients 2020, 12, 3314. [Google Scholar] [CrossRef]
- Yilmaz, H.Ö.; Aslan, R.; Unal, C. Effect of the COVID-19 pandemic on eating habits and food purchasing behaviors of university students. Kesmas 2020, 15, 154–159. [Google Scholar]
- Scarmozzino, F.; Visioli, F. COVID-19 and the subsequent lockdown modified dietary habits of almost half the population in an Italian sample. Foods 2020, 9, 675. [Google Scholar] [CrossRef]
- Bhol, A.; Sanwalka, N.; Kapasi, T.A.; Piplodwala, S.Z.; Ansari, L.M.A.; Katawala, F.M.; Bhandary, T.A. Changes in snacking patterns during COVID-19 lockdown in adults from Mumbai City, India. Curr. Res. Nutr. Food Sci. J. 2021, 9, 970–979. [Google Scholar] [CrossRef]
- Alfawaz, H.; Amer, O.E.; Aljumah, A.A.; Aldisi, D.A.; Enani, M.A.; Aljohani, N.J.; Alotaibi, N.H.; Alshingetti, N.; Alomar, S.Y.; Khattak, M.N.K.; et al. Effects of home quarantine during COVID-19 lockdown on physical activity and dietary habits of adults in Saudi Arabia. Sci. Rep. 2021, 11, 5904. [Google Scholar] [CrossRef] [PubMed]
- Alamri, E.S. Effects of COVID-19 home confinement on eating behavior: A review. J. Public Health Res. 2021, 10, 2088. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 home confinement on eating behaviour and physical activity: Results of the ECLB-COVID19 international online survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef] [PubMed]
- Coulthard, H.; Sharps, M.; Cunliffe, L.; van den Tol, A. Eating in the lockdown during the COVID 19 pandemic; self-reported changes in eating behaviour, and associations with BMI, eating style, coping and health anxiety. Appetite 2021, 161, 105082. [Google Scholar] [CrossRef]
- Mumena, W. Impact of COVID-19 Curfew on eating habits, eating frequency, and weight according to food security status in Saudi Arabia: A retrospective study. Prog. Nutr. 2021, 22, e2020075. [Google Scholar]
- Hoteit, M.; Mortada, H.; Al-Jawaldeh, A.; Ibrahim, C.; Mansour, R. COVID-19 home isolation and food consumption patterns: Investigating the correlates of poor dietary diversity in Lebanon: A cross-sectional study. F1000Research 2022, 11, 110. [Google Scholar] [CrossRef]
- Jafri, A.; Mathe, N.; Aglago, E.K.; Konyole, S.O.; Ouedraogo, M.; Audain, K.; Zongo, U.; Laar, A.K.; Johnson, J.; Sanou, D. Food availability, accessibility and dietary practices during the COVID-19 pandemic: A multi-country survey. Public Health Nutr. 2021, 24, 1798–1805. [Google Scholar] [CrossRef]
- Tsegaye, A.T.; Tariku, A.; Worku, A.G.; Abebe, S.M.; Yitayal, M.; Awoke, T.; Alemu, K.; Biks, G.A. Reducing amount and frequency of meal as a major coping strategy for food insecurity. Arch. Public Health 2018, 76, 56. [Google Scholar] [CrossRef] [Green Version]
- Niles, M.T.; Bertmann, F.; Belarmino, E.H.; Wentworth, T.; Biehl, E.; Neff, R. The Early Food Insecurity Impacts of COVID-19. Nutrients 2020, 12, 2096. [Google Scholar] [CrossRef]
- World Food Program (WFP). The state of Food Security in Jordan (2013–2014). 2016. Available online: https://www.wfp.org/publications/jordan-state-food-security-2013-2014-analytical-report-february-2016 (accessed on 30 April 2022).
- Department of Statistics (DOS). The State of Food Security in Jordan 2010/2011. 2012. Available online: https://data2.unhcr.org/en/documents/download/39420 (accessed on 1 May 2022).
- Bawadi, H.A.; Tayyem, R.F.; Dwairy, A.N.; Al-Akour, N. Prevalence of Food Insecurity among women in Northern Jordan. J. Health Popul. Nutr. 2012, 30, 49–55. [Google Scholar] [CrossRef] [Green Version]
- World Food Program (WFP). Jordan Food Security Survey in the Poverty Pockets. 2008. Available online: http://documents.wfp.org/stellent/groups/public/documents/ena/wfp204530.pdf (accessed on 1 May 2022).
- Bawadi, H.; Saeed, D.; Tayyem, R. Food Insecurity Among Children in Northern Jordan: Prevalence, Socio-Economic Determinants, and Impact on School Performance. Curr. Nutr. Food Sci. 2015, 11, 204–208. [Google Scholar] [CrossRef]
- Doocy, S.; Sirois, A.; Anderson, J.; Tileva, M.; Biermann, E.; Storey, J.D.; Burnham, G. Food security and humanitarian assistance among displaced Iraqi populations in Jordan and Syria. Soc. Sci. Med. 2011, 72, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Krafft, C.; Sieverding, M.; Salemi, C.; Keo, C. Syrian Refugees in Jordan: Demographics, Livelihoods, Education, and Health. Economic Research Forum 2018. Available online: https://erf.org.eg/publications/syrian-refugees-in-jordan-demographics-livelihoods-education-and-health/ (accessed on 3 May 2022).
- Tayyem, R.F. Prevalence of Food Insecurity among Palestinian Refugees in Jordan: RHSC Working Paper Series. J. Agric. Res. Econ. 2010, 31, 14–26. [Google Scholar]
- World Food Program (WFP). Jordan—Comprehensive Food Security and Vulnerability Assessment, 2018. 2019. Available online: https://www.wfp.org/publications/wfp-jordan-comprehensive-food-security-and-vulnerability-assessment-2018 (accessed on 3 May 2022).

{kind=link}
{kind=link}
| Food Group | Food Items (Examples) | Weight |
|---|---|---|
| Main staples | Bread, rice, macaroni, cereals | 2 |
| Pulses | Broad beans, beans, chickpeas | 3 |
| Vegetables | All types of vegetables | 1 |
| Fruits | All types of vegetables | 1 |
| Meat/Fish | Beef, lamb, poultry, eggs, fish, organ meat | 4 |
| Milk | Milk, yogurt, cheese, labneh | 4 |
| Sugar | Sugar, sugar product, honey | 0.5 |
| Oil | Vegetable oils, butter, ghee | 0.5 |
| Condiments | Spices | 0 |
| Variables | Total | Food Security Status | p-Value | |||
|---|---|---|---|---|---|---|
| Food-Secure 622 (84.1) | Moderate Food Insecurity 15 (2.0) | Severe Food Insecurity 103 (13.9) | ||||
| Gender | Male | 160 (21.6) | 133 (83.1) | 3 (1.9) | 24 (15.0) | 0.898 |
| Female | 580 (78.4) | 489 (84.3) | 12 (2.1) | 79 (13.6) | ||
| Age | 18–49 years | 686 (92.7) | 576 (84.0) | 12 (1.7) | 98 (14.3) | 0.106 |
| 50 years and more | 54 (7.3) | 46 (85.2) | 3 (5.6) | 5 (9.3) | ||
| Educational level | Secondary school or less | 68 (9.2) | 43 (63.2) | 1 (1.5) | 24 (35.3) | <0.001 |
| Diploma or bachelor | 502 (67.8) | 421 (83.9) | 14 (2.8) | 67 (13.3) | ||
| Postgraduate | 170 (23.0) | 158 (92.9) | 0 (0.0) | 12 (7.1) | ||
| Marital status | Single | 407 (55.0) | 360 (88.5) | 4 (1.0) | 43 (10.6) | 0.001 |
| Married | 315 (42.6) | 251 (79.7) | 10 (3.2) | 54 (17.1) | ||
| Divorced or widowed | 18 (2.4) | 11 (61.1) | 1 (5.6) | 6 (33.3) | ||
| Number of children | None | 472 (63.8) | 416 (88.1) | 4 (0.8) | 52 (11.0) | 0.003 |
| Less than 3 | 109 (14.7) | 86 (78.9) | 4 (3.7) | 19 (17.4) | ||
| 3–5 children | 137 (18.5) | 103 (75.2) | 6 (4.4) | 28 (20.4) | ||
| More than 5 children | 22 (3.0) | 17 (77.3) | 1 (4.5) | 4 (18.2) | ||
| Residence | City | 632 (85.4) | 531 (84.0) | 15 (2.4) | 86 (13.6) | 0.239 |
| Village | 108 (14.6) | 91 (84.3) | 0 (0.0) | 17 (15.7) | ||
| Job of the head of the family | Employee at private sector | 268 (36.2) | 229 (85.4) | 4 (1.5) | 35 (13.1) | 0.624 |
| Employee at governmental sector | 195 (26.4) | 165 (84.6) | 4 (2.1) | 26 (13.3) | ||
| Free business | 159 (21.5) | 130 (81.8) | 6 (3.8) | 23 (14.5) | ||
| Unemployed | 118 (15.9) | 98 (83.1) | 1 (0.8) | 19 (16.1) | ||
| Number of employees working in the family | 0–1 person | 387 (52.3) | 312 (80.6) | 7 (1.8) | 68 (17.6) | 0.023 |
| 2–4 people | 334 (45.1) | 291 (87.1) | 8 (2.4) | 35 (10.5) | ||
| More than 4 | 19 (2.6) | 19 (100.0) | 0 (0.0) | 0 (0.0) | ||
| Type of residence | Own residence | 523 (70.7) | 460 (88.0) | 7 (1.3) | 56 (10.7) | <0.001 |
| Rented residence | 217 (29.3) | 162 (74.7) | 8 (3.7) | 47 (21.7) | ||
| Monthly income | Less than JOD 500 * | 218 (29.5) | 153 (70.2) | 6 (2.8) | 59 (27.1) | <0.001 |
| JOD 501–1000 | 334 (45.1) | 294 (88.0) | 6 (1.8) | 34 (10.2) | ||
| More than JOD 1000 | 188 (25.4) | 175 (93.1) | 3 (1.6) | 10 (5.3) | ||
| Number of family members | Less than 4 | 260 (35.1) | 218 (83.8) | 5 (3.3) | 37 (14.2) | 0.694 |
| 4–7 members | 388 (52.4) | 331 (85.3) | 7 (1.8) | 50 (12.9) | ||
| More than 7 | 92 (12.4) | 73 (79.3) | 3 (3.3) | 16 (17.4) | ||
| Availability of health insurance | Yes | 491 (66.4) | 426 (86.8) | 4 (0.8) | 61 (12.4) | 0.001 |
| No | 249 (33.6) | 196 (78.7) | 11 (4.4) | 42 (16.9) | ||
| Variables | Food Security Status | ||
|---|---|---|---|
| Moderate Food Insecurity | Severe Food Insecurity | ||
| Gender | Male | 0.919 (0.256–3.306) | 1.117 (0.681–1.833) |
| Female | Reference | Reference | |
| Age | 18–49 years | 0.319 (0.087–1.172) | 1.565 (0.607–4.037) |
| 50 years and more | Reference | Reference | |
| Educational level | Secondary school or less | ND | 7.349 (3.401–15.881) ** |
| Diploma or bachelor | ND | 2.095 (1.104–3.978) * | |
| Postgraduate | Reference | Reference | |
| Marital status | Single | 0.122 (0.013–1.185) | 0.219 (0.077–0.622) * |
| Married | 0.438 (0.051–3.734) | 0.394 (0.140–1.113) | |
| Divorced or widowed | Reference | Reference | |
| Number of children | None | 0.163 (0.017–1.542) | 0.531 (0.172–1.639) |
| Less than 3 | 0.791 (0.083–7.519) | 0.939 (0.284–3.109) | |
| 3–5 children | 0.990 (0.112–8.745) | 1.155 (0.360–3.710) | |
| More than 5 children | Reference | Reference | |
| Residence | City | ND | 0.867 (0.492–1.527) |
| Village | Reference | Reference | |
| The job of the head of the family | Employee at the private sector | 1.712 (0.189–15.511) | 0.788 (0.430–1.446) |
| Employee at governmental sector | 2.376 (0.262–21.560) | 0.813 (0.428–1.545) | |
| Free business | 4.523 (0.536–38.182) | 0.913 (0.471–1.769) | |
| Unemployed | Reference | Reference | |
| Type of residence | Own residence | 0.308 (0.110–0.863) * | 0.420 (0.274–0.643) ** |
| Rented residence | Reference | Reference | |
| Monthly income | Less than JOD 500 | 2.288 (0.563–9.302) | 6.748 (3.336–13.651) ** |
| JOD 501–1000 | 1.190 (0.294–4.820) | 2.024 (0.976–4.197) | |
| More than JOD 1000 | Reference | Reference | |
| Number of family members | Less than 4 | 0.558 (0.130–2.393) | 0.774 (0.407–1.474) |
| 4–7 members | 0.515 (0.130–2.037) | 0.689 (0.372–1.278) | |
| More than 7 | Reference | Reference | |
| Availability of health insurance | Yes | 0.167 (0.053–0.532) * | 0.668 (0.436–1.025) |
| No | Reference | Reference | |
| Variables | Total | Food Security Status | p-Value | |||
|---|---|---|---|---|---|---|
| Food-Secure | Moderate Food Insecurity | Severe Food Insecurity | ||||
| Number of meals per day (1 day before) | 2 meals or less | 465 (62.8) | 380 (81.7) | 14 (3.0) | 71 (15.3) | 0.015 |
| More than 2 meals | 275 (37.2) | 242 (88.0) | 1 (0.4) | 32 (11.6) | ||
| The actual number of meals as reported | As usual | 644 (87.0) | 554 (86.0) | 11 (1.7) | 79 (12.3) | <0.001 |
| Less than usual | 79 (10.7) | 52 (65.8) | 4 (5.1) | 23 (29.1) | ||
| More than usual | 17 (2.3) | 16 (94.1) | 0 (0.0) | 1 (5.9) | ||
| Food group consumption in the previous 7 days | ||||||
| Cereals | 3 days and fewer | 306 (41.4) | 240 (78.4) | 9 (2.9) | 57 (18.6) | 0.002 |
| 4 days and more | 434 (58.6) | 382 (88.0) | 6 (1.4) | 46 (10.6) | ||
| White tubers | 3 days and fewer | 654 (88.4) | 544 (83.2) | 14 (2.1) | 96 (14.7) | 0.201 |
| 4 days and more | 86 (11.6) | 78 (90.7) | 1 (1.2) | 7 (8.1) | ||
| Vegetables | 3 days and fewer | 431 (58.2) | 345 (80.0) | 12 (2.8) | 74 (17.2) | 0.002 |
| 4 days and more | 309 (41.8) | 277 (89.6) | 3 (1.0) | 29 (9.4) | ||
| Fruits | 3 days and fewer | 453 (61.2) | 354 (78.1) | 13 (2.9) | 86 (19.0) | <0.001 |
| 4 days and more | 287 (38.8) | 268 (93.4) | 2 (0.7) | 17 (5.9) | ||
| Eggs | 3 days and fewer | 591 (79.9) | 487 (82.4) | 15 (2.5) | 89 (15.1) | 0.024 |
| 4 days and more | 149 (20.1) | 135 (90.6) | 0 (0.0) | 14 (9.4) | ||
| Legumes and nuts | 3 days and fewer | 563 (76.1) | 458 (81.3) | 13 (2.3) | 92 (16.3) | 0.002 |
| 4 days and more | 177 (23.9) | 164 (92.7) | 2 (1.1) | 11 (6.2) | ||
| Milk and dairy products | 3 days and fewer | 473 (63.9) | 378 (79.9) | 13 (2.7) | 82 (17.3) | <0.001 |
| 4 days and more | 267 (36.1) | 244 (91.4) | 2 (0.7) | 21 (7.9) | ||
| Oil and fat | 3 days and fewer | 415 (56.1) | 330 (79.5) | 12 (2.9) | 73 (17.6) | 0.001 |
| 4 days and more | 325 (43.9) | 292 (89.8) | 3 (0.9) | 30 (9.2) | ||
| Sugar | 3 days and fewer | 434 (58.6) | 343 (79.0) | 13 (3.0) | 78 (18.0) | <0.001 |
| 4 days and more | 306 (41.4) | 279 (91.2) | 2 (0.7) | 25 (8.2) | ||
| Spices and condiments | 3 days and fewer | 341 (46.1) | 260 (76.2) | 12 (3.5) | 69 (20.2) | <0.001 |
| 4 days and more | 399 (53.9) | 362 (90.7) | 3 (0.8) | 34 (8.5) | ||
| Meat and poultry | 3 days and fewer | 369 (49.9) | 279 (75.6) | 10 (2.7) | 80 (21.7) | <0.001 |
| 4 days and more | 371 (50.1) | 343 (92.5) | 5 (1.3) | 23 (6.2) | ||
| Fish | 3 days and fewer | 706 (95.4) | 593 (84.0) | 14 (2.0) | 99 (14.0) | 0.873 |
| 4 days and more | 34 (4.6) | 29 (85.3) | 1 (2.9) | 4 (11.8) | ||
| Variables | Total | Food Security Status | p-Value | |||
|---|---|---|---|---|---|---|
| Food-Secure | Moderate Food Insecurity | Severe Food Insecurity | ||||
| Eating cheaper foods | 3 days and fewer | 718 (97.0) | 610 (85.0) | 15 (2.1) | 93 (13.0) | <0.001 |
| 4 days and more | 22 (3.0) | 12 (54.5) | 0 (0.0) | 10 (45.5) | ||
| Borrowing food | 3 days and fewer | 728 (98.4) | 614 (84.3) | 14 (1.9) | 100 (13.7) | 0.142 |
| 4 days and more | 12 (1.6) | 8 (66.7) | 1 (8.3) | 3 (25.0) | ||
| Eating less meals to spare food for children | 3 days and fewer | 718 (97.0) | 610 (85.0) | 13 (1.8) | 95 (13.2) | <0.001 |
| 4 days and more | 22 (3.0) | 12 (54.5) | 2 (9.1) | 8 (36.4) | ||
| Eating small amounts | 3 days and fewer | 717 (96.9) | 611 (85.2) | 12 (1.7) | 94 (13.1) | <0.001 |
| 4 days and more | 23 (3.1) | 11 (47.8) | 3 (13.0) | 9 (39.1) | ||
| Adults only eat less to spare food for children | 3 days and fewer | 715 (96.6) | 609 (85.2) | 14 (2.0) | 92 (12.9) | <0.001 |
| 4 days and more | 25 (3.4) | 13 (52.0) | 1 (4.0) | 103 (13.9) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olaimat, A.N.; Alshami, I.K.; Al Hourani, H.; Sarhan, W.; Al-Holy, M.; Abughoush, M.; Al-Awwad, N.J.; Hoteit, M.; Al-Jawaldeh, A. Food Insecurity, Dietary Diversity, and Coping Strategies in Jordan during the COVID-19 Pandemic: A Cross-Sectional Study. Nutrients 2022, 14, 2252. https://doi.org/10.3390/nu14112252
Olaimat AN, Alshami IK, Al Hourani H, Sarhan W, Al-Holy M, Abughoush M, Al-Awwad NJ, Hoteit M, Al-Jawaldeh A. Food Insecurity, Dietary Diversity, and Coping Strategies in Jordan during the COVID-19 Pandemic: A Cross-Sectional Study. Nutrients. 2022; 14(11):2252. https://doi.org/10.3390/nu14112252
Chicago/Turabian StyleOlaimat, Amin N., Islam K. Alshami, Huda Al Hourani, Wafaa Sarhan, Murad Al-Holy, Mahmoud Abughoush, Narmeen Jamal Al-Awwad, Maha Hoteit, and Ayoub Al-Jawaldeh. 2022. "Food Insecurity, Dietary Diversity, and Coping Strategies in Jordan during the COVID-19 Pandemic: A Cross-Sectional Study" Nutrients 14, no. 11: 2252. https://doi.org/10.3390/nu14112252
APA StyleOlaimat, A. N., Alshami, I. K., Al Hourani, H., Sarhan, W., Al-Holy, M., Abughoush, M., Al-Awwad, N. J., Hoteit, M., & Al-Jawaldeh, A. (2022). Food Insecurity, Dietary Diversity, and Coping Strategies in Jordan during the COVID-19 Pandemic: A Cross-Sectional Study. Nutrients, 14(11), 2252. https://doi.org/10.3390/nu14112252