
Vitamin D Metabolite Ratio in Pregnant Women with Low Blood Vitamin D Concentrations Is Associated with Neonatal Anthropometric Data

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Measurement of Vitamin D Metabolites
2.3. Covariate and Birth Outcome Data
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
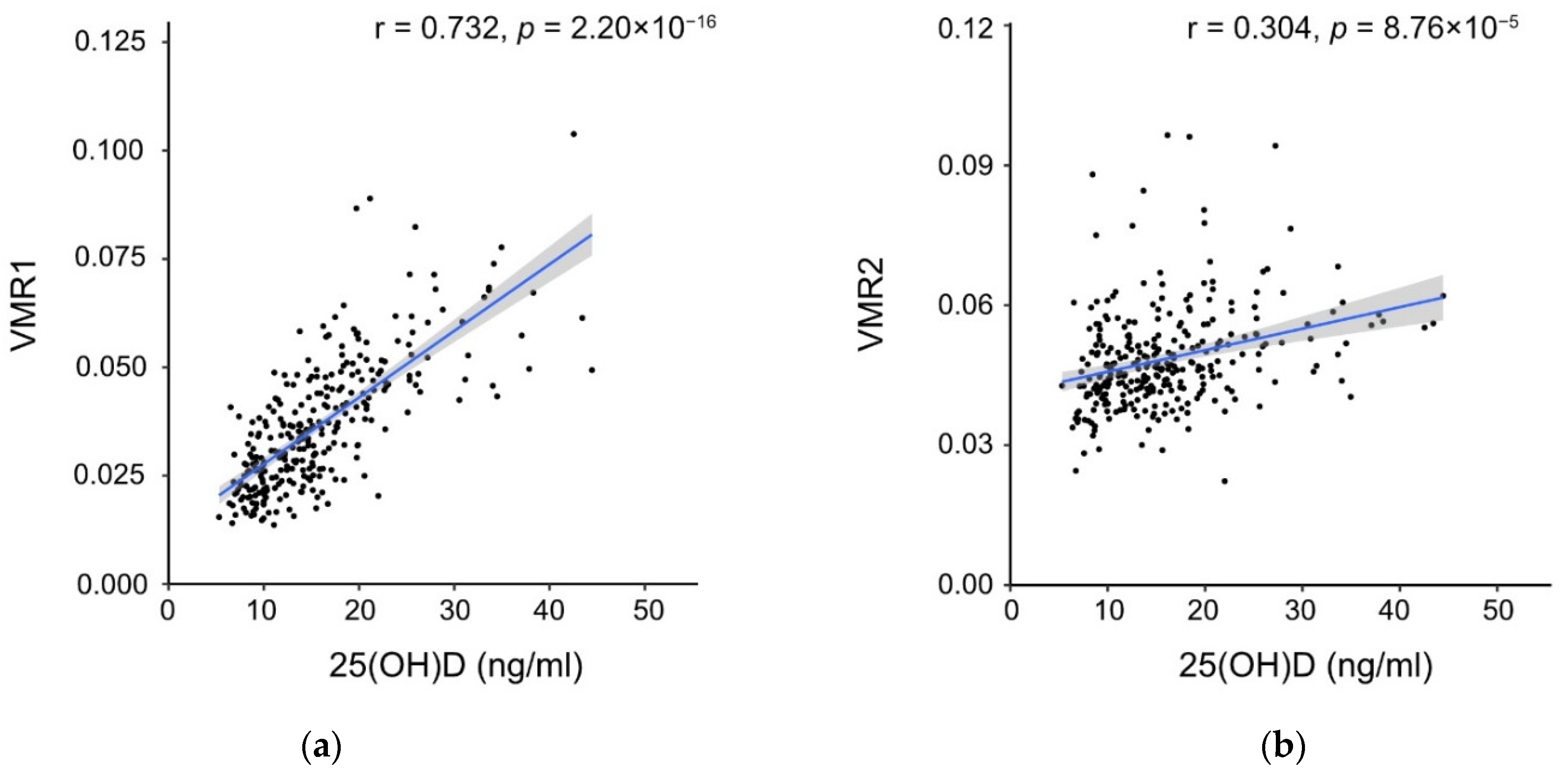
3.2. Vitamin D Metabolite Concentrations
3.3. Factors including VMR and Neonatal Anthropometric Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brooks, A.A.; Johnson, M.R.; Steer, P.J.; Pawson, M.E.; Abdalla, H.I. Birth weight: Nature or nurture? Early Hum. Dev. 1995, 42, 29–35. [Google Scholar] [CrossRef]
- Magnus, P.; Gjessing, H.K.; Skrondal, A.; Skjaerven, R. Paternal contribution to birth weight. J. Epidemiol. Community Health 2001, 55, 873–877. [Google Scholar] [CrossRef]
- Lunde, A.; Melve, K.K.; Gjessing, H.K.; Skjaerven, R.; Irgens, L.M. Genetic and environmental influences on birth weight, birth length, head circumference, and gestational age by use of population-based parent-offspring data. Am. J. Epidemiol. 2007, 165, 734–741. [Google Scholar] [CrossRef]
- Clausson, B.; Lichtenstein, P.; Cnattingius, S. Genetic influence on birthweight and gestational length determined by studies in offspring of twins. BJOG 2000, 107, 375–381. [Google Scholar] [CrossRef]
- Katz, J.; Lee, A.C.; Kozuki, N.; Lawn, J.E.; Cousens, S.; Blencowe, H.; Ezzati, M.; Bhutta, Z.A.; Marchant, T.; Willey, B.A.; et al. Mortality risk in preterm and small-for-gestational-age infants in low-income and middle-income countries: A pooled country analysis. Lancet 2013, 382, 417–425. [Google Scholar] [CrossRef]
- Mericq, V.; Martinez-Aguayo, A.; Uauy, R.; Iniguez, G.; Van der Steen, M.; Hokken-Koelega, A. Long-term metabolic risk among children born premature or small for gestational age. Nat. Rev. Endocrinol. 2017, 13, 50–62. [Google Scholar] [CrossRef]
- Pariente, G.; Sheiner, E.; Kessous, R.; Michael, S.; Shoham-Vardi, I. Association between delivery of a small-for-gestational-age neonate and long-term maternal cardiovascular morbidity. Int. J. Gynaecol. Obs. 2013, 123, 68–71. [Google Scholar] [CrossRef]
- Savchev, S.; Sanz-Cortes, M.; Cruz-Martinez, R.; Arranz, A.; Botet, F.; Gratacos, E.; Figueras, F. Neurodevelopmental outcome of full-term small-for-gestational-age infants with normal placental function. Ultrasound Obs. Gynecol. 2013, 42, 201–206. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Vital Statistics of Japan 1980–2010. Available online: https://www.mhlw.go.jp/english/database/db-hw/FY2010/live_births.html (accessed on 26 March 2021).
- Gernand, A.D.; Simhan, H.N.; Klebanoff, M.A.; Bodnar, L.M. Maternal serum 25-hydroxyvitamin D and measures of newborn and placental weight in a U.S. multicenter cohort study. J. Clin. Endocrinol. Metab. 2013, 98, 398–404. [Google Scholar] [CrossRef]
- Morales, E.; Rodriguez, A.; Valvi, D.; Iniguez, C.; Esplugues, A.; Vioque, J.; Marina, L.S.; Jimenez, A.; Espada, M.; Dehli, C.R.; et al. Deficit of vitamin D in pregnancy and growth and overweight in the offspring. Int. J. Obes. 2015, 39, 61–68. [Google Scholar] [CrossRef]
- Rodriguez, A.; Garcia-Esteban, R.; Basterretxea, M.; Lertxundi, A.; Rodriguez-Bernal, C.; Iniguez, C.; Rodriguez-Dehli, C.; Tardon, A.; Espada, M.; Sunyer, J.; et al. Associations of maternal circulating 25-hydroxyvitamin D3 concentration with pregnancy and birth outcomes. BJOG 2015, 122, 1695–1704. [Google Scholar] [CrossRef]
- Boyle, V.T.; Thorstensen, E.B.; Mourath, D.; Jones, M.B.; McCowan, L.M.; Kenny, L.C.; Baker, P.N. The relationship between 25-hydroxyvitamin D concentration in early pregnancy and pregnancy outcomes in a large, prospective cohort. Br. J. Nutr. 2016, 116, 1409–1415. [Google Scholar] [CrossRef]
- Miliku, K.; Vinkhuyzen, A.; Blanken, L.M.; McGrath, J.J.; Eyles, D.W.; Burne, T.H.; Hofman, A.; Tiemeier, H.; Steegers, E.A.; Gaillard, R.; et al. Maternal vitamin D concentrations during pregnancy, fetal growth patterns, and risks of adverse birth outcomes. Am. J. Clin. Nutr. 2016, 103, 1514–1522. [Google Scholar] [CrossRef]
- Hauta-Alus, H.H.; Viljakainen, H.T.; Holmlund-Suila, E.M.; Enlund-Cerullo, M.; Rosendahl, J.; Valkama, S.M.; Helve, O.M.; Hytinantti, T.K.; Makitie, O.M.; Andersson, S. Maternal vitamin D status, gestational diabetes and infant birth size. BMC Pregnancy Childbirth 2017, 17, 420. [Google Scholar] [CrossRef]
- Francis, E.C.; Hinkle, S.N.; Song, Y.; Rawal, S.; Donnelly, S.R.; Zhu, Y.; Chen, L.; Zhang, C. Longitudinal Maternal Vitamin D Status during Pregnancy Is Associated with Neonatal Anthropometric Measures. Nutrients 2018, 10, 1631. [Google Scholar] [CrossRef]
- Wen, J.; Kang, C.; Wang, J.; Cui, X.; Hong, Q.; Wang, X.; Zhu, L.; Xu, P.; Fu, Z.; You, L.; et al. Association of maternal serum 25-hydroxyvitamin D concentrations in second and third trimester with risk of macrosomia. Sci. Rep. 2018, 8, 6169. [Google Scholar] [CrossRef]
- Boghossian, N.S.; Koo, W.; Liu, A.; Mumford, S.L.; Tsai, M.Y.; Yeung, E.H. Longitudinal measures of maternal vitamin D and neonatal body composition. Eur. J. Clin. Nutr. 2019, 73, 424–431. [Google Scholar] [CrossRef]
- Thompson, W.D.; Tyrrell, J.; Borges, M.C.; Beaumont, R.N.; Knight, B.A.; Wood, A.R.; Ring, S.M.; Hattersley, A.T.; Freathy, R.M.; Lawlor, D.A. Association of maternal circulating 25(OH)D and calcium with birth weight: A mendelian randomisation analysis. PLoS Med. 2019, 16, e1002828. [Google Scholar] [CrossRef]
- WHO Scientific Group on the Prevention and Management of Osteoporosis. Prevention and Management of Osteoporosis: Report of a WHO Scientific Group; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Ginde, A.A.; Liu, M.C.; Camargo, C.A., Jr. Demographic differences and trends of vitamin D insufficiency in the US population, 1988–2004. Arch. Intern. Med. 2009, 169, 626–632. [Google Scholar] [CrossRef]
- Gutierrez, O.M.; Farwell, W.R.; Kermah, D.; Taylor, E.N. Racial differences in the relationship between vitamin D, bone mineral density, and parathyroid hormone in the National Health and Nutrition Examination Survey. Osteoporos. Int. 2011, 22, 1745–1753. [Google Scholar] [CrossRef]
- Mitchell, D.M.; Henao, M.P.; Finkelstein, J.S.; Burnett-Bowie, S.A. Prevalence and predictors of vitamin D deficiency in healthy adults. Endocr. Pract. 2012, 18, 914–923. [Google Scholar] [CrossRef]
- Bischoff-Ferrari, H.A.; Dietrich, T.; Orav, E.J.; Dawson-Hughes, B. Positive association between 25-hydroxy vitamin D levels and bone mineral density: A population-based study of younger and older adults. Am. J. Med. 2004, 116, 634–639. [Google Scholar] [CrossRef]
- Cauley, J.A.; Lui, L.Y.; Ensrud, K.E.; Zmuda, J.M.; Stone, K.L.; Hochberg, M.C.; Cummings, S.R. Bone mineral density and the risk of incident nonspinal fractures in black and white women. JAMA 2005, 293, 2102–2108. [Google Scholar] [CrossRef]
- Hannan, M.T.; Litman, H.J.; Araujo, A.B.; McLennan, C.E.; McLean, R.R.; McKinlay, J.B.; Chen, T.C.; Holick, M.F. Serum 25-hydroxyvitamin D and bone mineral density in a racially and ethnically diverse group of men. J. Clin. Endocrinol. Metab. 2008, 93, 40–46. [Google Scholar] [CrossRef]
- Cauley, J.A.; Danielson, M.E.; Boudreau, R.; Barbour, K.E.; Horwitz, M.J.; Bauer, D.C.; Ensrud, K.E.; Manson, J.E.; Wactawski-Wende, J.; Shikany, J.M.; et al. Serum 25-hydroxyvitamin D and clinical fracture risk in a multiethnic cohort of women: The Women’s Health Initiative (WHI). J. Bone Min. Res. 2011, 26, 2378–2388. [Google Scholar] [CrossRef]
- Ginsberg, C.; Katz, R.; de Boer, I.H.; Kestenbaum, B.R.; Chonchol, M.; Shlipak, M.G.; Sarnak, M.J.; Hoofnagle, A.N.; Rifkin, D.E.; Garimella, P.S.; et al. The 24,25 to 25-hydroxyvitamin D ratio and fracture risk in older adults: The cardiovascular health study. Bone 2018, 107, 124–130. [Google Scholar] [CrossRef]
- Shah, I.; Petroczi, A.; Naughton, D.P. Exploring the role of vitamin D in type 1 diabetes, rheumatoid arthritis, and Alzheimer disease: New insights from accurate analysis of 10 forms. J. Clin. Endocrinol. Metab. 2014, 99, 808–816. [Google Scholar] [CrossRef]
- Karras, S.N.; Shah, I.; Petroczi, A.; Goulis, D.G.; Bili, H.; Papadopoulou, F.; Harizopoulou, V.; Tarlatzis, B.C.; Naughton, D.P. An observational study reveals that neonatal vitamin D is primarily determined by maternal contributions: Implications of a new assay on the roles of vitamin D forms. Nutr. J. 2013, 12, 77. [Google Scholar] [CrossRef]
- Ahmed, L.H.M.; Butler, A.E.; Dargham, S.R.; Latif, A.; Chidiac, O.M.; Atkin, S.L.; Abi Khalil, C. Vitamin D3 metabolite ratio as an indicator of vitamin D status and its association with diabetes complications. BMC Endocr. Disord. 2020, 20, 161. [Google Scholar] [CrossRef]
- Kanatani, K.T.; Nakayama, T.; Adachi, Y.; Hamazaki, K.; Onishi, K.; Konishi, Y.; Kawanishi, Y.; Go, T.; Sato, K.; Kurozawa, Y.; et al. High frequency of vitamin D deficiency in current pregnant Japanese women associated with UV avoidance and hypo-vitamin D diet. PLoS ONE 2019, 14, e0213264. [Google Scholar] [CrossRef]
- Kanatani, K.T.; Adachi, Y.; Hamazaki, K.; Onishi, K.; Go, T.; Hirabayashi, K.; Watanabe, M.; Sato, K.; Kurozawa, Y.; Inadera, H.; et al. Association between vitamin D deficiency and allergic symptom in pregnant women. PLoS ONE 2019, 14, e0214797. [Google Scholar] [CrossRef]
- Kawamoto, T.; Nitta, H.; Murata, K.; Toda, E.; Tsukamoto, N.; Hasegawa, M.; Yamagata, Z.; Kayama, F.; Kishi, R.; Ohya, Y.; et al. Rationale and study design of the Japan environment and children’s study (JECS). BMC Public Health 2014, 14, 25. [Google Scholar] [CrossRef]
- Satoh, M.; Ishige, T.; Ogawa, S.; Nishimura, M.; Matsushita, K.; Higashi, T.; Nomura, F. Development and validation of the simultaneous measurement of four vitamin D metabolites in serum by LC-MS/MS for clinical laboratory applications. Anal. Bioanal. Chem. 2016, 408, 7617–7627. [Google Scholar] [CrossRef]
- Phinney, K.W.; Bedner, M.; Tai, S.S.; Vamathevan, V.V.; Sander, L.C.; Sharpless, K.E.; Wise, S.A.; Yen, J.H.; Schleicher, R.L.; Chaudhary-Webb, M.; et al. Development and certification of a standard reference material for vitamin D metabolites in human serum. Anal. Chem. 2012, 84, 956–962. [Google Scholar] [CrossRef]
- Yamamoto, M.; Sakurai, K.; Eguchi, A.; Yamazaki, S.; Nakayama, S.F.; Isobe, T.; Takeuchi, A.; Sato, T.; Hata, A.; Mori, C.; et al. Association between blood manganese level during pregnancy and birth size: The Japan environment and children’s study (JECS). Environ. Res. 2019, 172, 117–126. [Google Scholar] [CrossRef]
- Kobayashi, S.; Kishi, R.; Saijo, Y.; Ito, Y.; Oba, K.; Araki, A.; Miyashita, C.; Itoh, S.; Minatoya, M.; Yamazaki, K.; et al. Association of blood mercury levels during pregnancy with infant birth size by blood selenium levels in the Japan Environment and Children’s Study: A prospective birth cohort. Environ. Int. 2019, 125, 418–429. [Google Scholar] [CrossRef]
- Farrant, H.J.; Krishnaveni, G.V.; Hill, J.C.; Boucher, B.J.; Fisher, D.J.; Noonan, K.; Osmond, C.; Veena, S.R.; Fall, C.H. Vitamin D insufficiency is common in Indian mothers but is not associated with gestational diabetes or variation in newborn size. Eur. J. Clin. Nutr. 2009, 63, 646–652. [Google Scholar] [CrossRef]
- Prentice, A.; Jarjou, L.M.; Goldberg, G.R.; Bennett, J.; Cole, T.J.; Schoenmakers, I. Maternal plasma 25-hydroxyvitamin D concentration and birthweight, growth and bone mineral accretion of Gambian infants. Acta Paediatr. 2009, 98, 1360–1362. [Google Scholar] [CrossRef]
- Ginsberg, C.; Hoofnagle, A.N.; Katz, R.; Hughes-Austin, J.; Miller, L.M.; Becker, J.O.; Kritchevsky, S.B.; Shlipak, M.G.; Sarnak, M.J.; Ix, J.H. The Vitamin D Metabolite Ratio Is Associated With Changes in Bone Density and Fracture Risk in Older Adults. J. Bone Min. Res. 2021, 36, 2343–2350. [Google Scholar] [CrossRef]
- Armbrecht, H.J.; Hodam, T.L.; Boltz, M.A.; Partridge, N.C.; Brown, A.J.; Kumar, V.B. Induction of the vitamin D 24-hydroxylase (CYP24) by 1,25-dihydroxyvitamin D3 is regulated by parathyroid hormone in UMR106 osteoblastic cells. Endocrinology 1998, 139, 3375–3381. [Google Scholar] [CrossRef]
- Perwad, F.; Azam, N.; Zhang, M.Y.; Yamashita, T.; Tenenhouse, H.S.; Portale, A.A. Dietary and serum phosphorus regulate fibroblast growth factor 23 expression and 1,25-dihydroxyvitamin D metabolism in mice. Endocrinology 2005, 146, 5358–5364. [Google Scholar] [CrossRef]
- Allgrove, J.; Adami, S.; Manning, R.M.; O’Riordan, J.L. Cytochemical bioassay of parathyroid hormone in maternal and cord blood. Arch. Dis. Child. 1985, 60, 110–115. [Google Scholar] [CrossRef]
- Papantoniou, N.E.; Papapetrou, P.D.; Antsaklis, A.J.; Kontoleon, P.E.; Mesogitis, S.A.; Aravantinos, D. Circulating levels of immunoreactive parathyroid hormone-related protein and intact parathyroid hormone in human fetuses and newborns. Eur. J. Endocrinol. 1996, 134, 437–442. [Google Scholar] [CrossRef]
- Takaiwa, M.; Aya, K.; Miyai, T.; Hasegawa, K.; Yokoyama, M.; Kondo, Y.; Kodani, N.; Seino, Y.; Tanaka, H.; Morishima, T. Fibroblast growth factor 23 concentrations in healthy term infants during the early postpartum period. Bone 2010, 47, 256–262. [Google Scholar] [CrossRef][Green Version]
- Singh, R.J.; Taylor, R.L.; Reddy, G.S.; Grebe, S.K. C-3 epimers can account for a significant proportion of total circulating 25-hydroxyvitamin D in infants, complicating accurate measurement and interpretation of vitamin D status. J. Clin. Endocrinol. Metab. 2006, 91, 3055–3061. [Google Scholar] [CrossRef]
- Schleicher, R.L.; Encisco, S.E.; Chaudhary-Webb, M.; Paliakov, E.; McCoy, L.F.; Pfeiffer, C.M. Isotope dilution ultra performance liquid chromatography-tandem mass spectrometry method for simultaneous measurement of 25-hydroxyvitamin D2, 25-hydroxyvitamin D3 and 3-epi-25-hydroxyvitamin D3 in human serum. Clin. Chim. Acta 2011, 412, 1594–1599. [Google Scholar] [CrossRef]
- van den Ouweland, J.M.; Beijers, A.M.; van Daal, H.; Elisen, M.G.; Steen, G.; Wielders, J.P. Evaluation of 3-epi-25-hydroxyvitamin D3 cross-reactivity in the Roche Elecsys Vitamin D Total protein binding assay. Clin. Chem. Lab. Med. 2014, 52, 373–380. [Google Scholar] [CrossRef]
- Butler, A.E.; Dargham, S.R.; Latif, A.; Mokhtar, H.R.; Robay, A.; Chidiac, O.M.; Jayyousi, A.; Al Suwaidi, J.; Crystal, R.G.; Abi Khalil, C.; et al. Association of vitamin D3 and its metabolites in patients with and without type 2 diabetes and their relationship to diabetes complications. Adv. Chronic. Dis. 2020, 11, 2040622320924159. [Google Scholar] [CrossRef]
- Yetley, E.A.; Pfeiffer, C.M.; Schleicher, R.L.; Phinney, K.W.; Lacher, D.A.; Christakos, S.; Eckfeldt, J.H.; Fleet, J.C.; Howard, G.; Hoofnagle, A.N.; et al. NHANES monitoring of serum 25-hydroxyvitamin D: A roundtable summary. J. Nutr. 2010, 140, 2030S–2045S. [Google Scholar] [CrossRef]
- Tuckey, R.C.; Cheng, C.Y.S.; Slominski, A.T. The serum vitamin D metabolome: What we know and what is still to discover. J. Steroid Biochem. Mol. Biol. 2019, 186, 4–21. [Google Scholar] [CrossRef]
- Kamao, M.; Tatematsu, S.; Hatakeyama, S.; Sakaki, T.; Sawada, N.; Inouye, K.; Ozono, K.; Kubodera, N.; Reddy, G.S.; Okano, T. C-3 epimerization of vitamin D3 metabolites and further metabolism of C-3 epimers: 25-hydroxyvitamin D3 is metabolized to 3-epi-25-hydroxyvitamin D3 and subsequently metabolized through C-1alpha or C-24 hydroxylation. J. Biol. Chem. 2004, 279, 15897–15907. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | All (N = 297) | ||
|---|---|---|---|
| N | % | ||
| Age at delivery (years), mean (SD) | 31.3 (4.8) | ||
| <25 | 24 | 8.1 | |
| 25–<30 | 85 | 28.6 | |
| 30–<35 | 108 | 36.4 | |
| 35≤ | 80 | 26.9 | |
| Education (years) | |||
| <10 | 8 | 2.7 | |
| 10–<13 | 199 | 67.0 | |
| 13–<17 | 88 | 29.6 | |
| 17≤ | 2 | 0.7 | |
| Parity | |||
| 0 | 107 | 36.0 | |
| 1≤ | 190 | 64.0 | |
| BMI before pregnancy (kg/m2), mean (SD) | 21.5 (3.3) | ||
| <18.5 | 43 | 14.5 | |
| 18.5–<25 | 221 | 74.4 | |
| 25≤ | 33 | 11.1 | |
| Annual household income (million Japanese Yen) | |||
| <2 | 15 | 5.1 | |
| 2–<4 | 97 | 32.7 | |
| 4–<6 | 107 | 36.0 | |
| 6–<8 | 48 | 16.2 | |
| 8–<10 | 19 | 6.4 | |
| 10≤ | 11 | 3.7 | |
| Smoking habits | |||
| Never | 159 | 53.5 | |
| Quit before pregnancy | 93 | 31.3 | |
| Smoking early pregnancy | 45 | 15.2 | |
| Alcohol consumption | |||
| Never | 111 | 37.4 | |
| Quit before pregnancy | 57 | 19.2 | |
| Drink early pregnancy | 129 | 43.4 | |
| Pregnancy-induced hypertension | 9 | 3.0 | |
| Gestational diabetes mellitus | 10 | 3.4 | |
| Diabetes Mellitus | 10 | 3.4 | |
| Vitamin D insufficiency (25(OH)D < 20 ng/mL) | 253 | 85.2 | |
| All (N = 297) | |||
|---|---|---|---|
| N | % | ||
| Sex | |||
| Male | 145 | 48.3 | |
| Female | 152 | 50.7 | |
| Mode of delivery | |||
| Vaginal | 233 | 77.7 | |
| Cesarian | 64 | 21.3 | |
| Birth weight (g), mean (SD) | 3028.5 (416.0) | ||
| Birth length(cm), mean (SD) | 48.6 (2.1) | ||
| Birth head circumference(cm), mean (SD) | 33.2 (1.4) | ||
| Birth chest circumference(cm), mean (SD) | 31.7 (1.7) | ||
| Gestational week, mean (SD) | 39.2 (1.5) |
| Mean | SD | Minimum | 25 Percentiles | Median | 75 Percentiles | Maximum | |
|---|---|---|---|---|---|---|---|
| 25(OH)D (ng/mL) | 15.82 | 7.10 | 5.31 | 10.31 | 14.63 | 19.27 | 44.45 |
| 25(OH)D2(ng/mL) | 0.51 | 0.52 | 0.14 | 0.34 | 0.43 | 0.56 | 8.18 |
| 25(OH)D3 (ng/mL) | 15.31 | 7.09 | 4.97 | 9.89 | 13.82 | 18.42 | 44.05 |
| 24,25(OH)2D3 (ng/mL) | 0.66 | 0.56 | 0.08 | 0.27 | 0.46 | 0.85 | 4.42 |
| 3-epi-25(OH)D3 (ng/mL) | 0.79 | 046 | 0.17 | 0.48 | 0.66 | 0.96 | 2.76 |
| VMR1 (×10−2) | 3.66 | 1.50 | 1.37 | 2.49 | 3.46 | 4.59 | 10.38 |
| VMR2 (×10−2) | 4.84 | 1.08 | 2.22 | 4.20 | 4.67 | 5.34 | 9.65 |
| Birth Weight (g) | ||||||||
| Model | 25(OH)D | 25(OH)D2 | 25(OH)D3 | 24,25(OH)2D3 | 3-epi-25(OH)D3 | VMR1 | VMR2 | |
| Unadjusted | β | 0.28 | 66.08 | −0.08 | −8.63 | −49.42 | −155.80 | −5907.30 |
| (95% CI) | (−6.44, 6.99) | (−25.49, 157.65) | (−6.80, 6.65) | (−93.07, 75.82) | (−153.68, 54.85) | (−3357.23, 3045.53) | (−10,285.77, −1528.86) | |
| p-value | 0.936 | 0.157 | 0.982 | 0.841 | 0.352 | 0.924 | 0.008 | |
| Adjusted | β | −0.21 | 34.21 | −0.39 | −3.81 | −46.58 | −113.99 | −4937.35 |
| (95% CI) | (−5.61, 5.20) | (−39.89, 108.31) | (−5.80, 5.02) | (−71.79, 64.17) | (−130.41, 37.26) | (−2693.21, 2465.23) | (−8455.06, −1419.64) | |
| p-value | 0.940 | 0.364 | 0.888 | 0.912 | 0.275 | 0.931 | 0.006 | |
| Birth length (cm) | ||||||||
| Model | 25(OH)D | 25(OH)D2 | 25(OH)D3 | 24,25(OH)2D3 | 3-epi-25(OH)D3 | VMR1 | VMR2 | |
| Unadjusted | β | 0.01 | 0.24 | 0.01 | 0.09 | −0.11 | 3.63 | −23.24 |
| (95% CI) | (−0.03, 0.04) | (−0.23, 0.70) | (−0.03, 0.04) | (−0.34, 0.52) | (−153.68, 54.85) | (−12.71, 19.97) | (−45.71, −0.78) | |
| p-value | 0.621 | 0.321 | 0.672 | 0.681 | 0.697 | 0.662 | 0.043 | |
| Adjusted | β | 0.00 | 0.04 | 0.00 | 0.09 | −0.13 | 3.87 | −19.48 |
| (95% CI) | (−0.02, 0.03) | (−0.34, 0.42) | (−0.02, 0.03) | (−0.26, 0.43) | (−0.56, 0.29) | (−9.18, 16.92) | (−37.39, −1.58) | |
| p-value | 0.808 | 0.834 | 0.820 | 0.614 | 0.533 | 0.560 | 0.033 | |
| Birth head circumference (cm) | ||||||||
| Model | 25(OH)D | 25(OH)D2 | 25(OH)D3 | 24,25(OH)2D3 | 3-epi-25(OH)D3 | VMR1 | VMR2 | |
| Unadjusted | β | −0.01 | 0.13 | −0.01 | −0.07 | −0.29 | −3.38 | −20.66 |
| (95% CI) | (−0.03, 0.01) | (−0.17, 0.44) | (−0.03, 0.01) | (−0.35, 0.21) | (−0.63, 0.06) | (−13.97, 7.21) | (−35.14, −6.19) | |
| p-value | 0.369 | 0.395 | 0.335 | 0.614 | 0.100 | 0.530 | 0.005 | |
| Adjusted | β | −0.01 | 0.05 | −0.01 | −0.05 | −0.27 | −2.64 | −18.75 |
| (95% CI) | (−0.03, 0.01) | (−0.25, 0.34) | (−0.03, 0.01) | (−0.32, 0.22) | (−0.60, 0.06) | (−12.86, 7.58) | (−32.71, −4.79) | |
| p-value | 0.348 | 0.742 | 0.335 | 0.724 | 0.109 | 0.612 | 0.009 | |
| Birth chest circumference (cm) | ||||||||
| Model | 25(OH)D | 25(OH)D2 | 25(OH)D3 | 24,25(OH)2D3 | 3-epi-25(OH)D3 | VMR1 | VMR2 | |
| Unadjusted | β | 0.00 | 0.36 | −0.01 | −0.11 | −0.30 | −4.23 | −26.55 |
| (95% CI) | (−0.03, 0.02) | (−0.01, 0.73) | (−0.03, 0.02) | (−0.46, 0.23) | (−0.73, 0.12) | (−17.31, 8.85) | (−44.41, −8.69) | |
| p-value | 0.749 | 0.060 | 0.647 | 0.513 | 0.164 | 0.525 | 0.004 | |
| Adjusted | β | −0.01 | 0.22 | −0.01 | −0.10 | −0.30 | −4.21 | −23.66 |
| (95% CI) | (−0.03, 0.02) | (−0.10, 0.53) | (−0.03, 0.01) | (−0.38, 0.19) | (−0.66, 0.05) | (−15.08, 6.66) | (−38.44, −8.87) | |
| p-value | 0.563 | 0.174 | 0.498 | 0.502 | 0.090 | 0.445 | 0.002 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takatani, T.; Kunii, Y.; Satoh, M.; Eguchi, A.; Yamamoto, M.; Sakurai, K.; Takatani, R.; Nomura, F.; Shimojo, N.; Mori, C. Vitamin D Metabolite Ratio in Pregnant Women with Low Blood Vitamin D Concentrations Is Associated with Neonatal Anthropometric Data. Nutrients 2022, 14, 2201. https://doi.org/10.3390/nu14112201
Takatani T, Kunii Y, Satoh M, Eguchi A, Yamamoto M, Sakurai K, Takatani R, Nomura F, Shimojo N, Mori C. Vitamin D Metabolite Ratio in Pregnant Women with Low Blood Vitamin D Concentrations Is Associated with Neonatal Anthropometric Data. Nutrients. 2022; 14(11):2201. https://doi.org/10.3390/nu14112201
Chicago/Turabian StyleTakatani, Tomozumi, Yuzuka Kunii, Mamoru Satoh, Akifumi Eguchi, Midori Yamamoto, Kenichi Sakurai, Rieko Takatani, Fumio Nomura, Naoki Shimojo, and Chisato Mori. 2022. "Vitamin D Metabolite Ratio in Pregnant Women with Low Blood Vitamin D Concentrations Is Associated with Neonatal Anthropometric Data" Nutrients 14, no. 11: 2201. https://doi.org/10.3390/nu14112201
APA StyleTakatani, T., Kunii, Y., Satoh, M., Eguchi, A., Yamamoto, M., Sakurai, K., Takatani, R., Nomura, F., Shimojo, N., & Mori, C. (2022). Vitamin D Metabolite Ratio in Pregnant Women with Low Blood Vitamin D Concentrations Is Associated with Neonatal Anthropometric Data. Nutrients, 14(11), 2201. https://doi.org/10.3390/nu14112201